
Abstract
A case involving the incidental diagnosis of multiple myeloma (MM) due to interference in the 25-hydroxy-vitamin D (25(OH) vitamin D) immunoassay is presented. The patient, under the care of rheumatology and receiving treatment with alendronic acid and vitamin D supplements, was referred to endocrinology for investigation of acromegaly. Acromegaly was subsequently ruled out; however, during the investigations, consistently elevated levels of 25(OH) vitamin D were noted, raising suspicion of vitamin D resistance syndrome. The laboratory and endocrinology teams engaged in discussions, and following the cessation of medication, repeated analyses for 25(OH) vitamin D and a single analysis of 1,25-dihydroxy-vitamin D levels were requested, yielding high and normal results, respectively. The laboratory conducted a three-step interference investigation, ultimately identifying a high molecular weight molecule responsible for the initially elevated 25(OH) vitamin D levels. Due to the clinical presentation of back pain, a proteinogram was requested, revealing a monoclonal band of 36 g/L. Subsequent free light chain analysis indicated an elevated ratio. With three risk factors identified, this was classified as an established MM and urgently referred to haematology for correct management. Laboratory assay interferences have the potential to disrupt the accurate diagnostic workup of patients. Collaborative discussions between laboratory and clinical teams regarding such cases aid in directing the diagnostic pathway appropriately, facilitating prompt and proper diagnosis and management.
Introduction
Paraproteins are monoclonal immunoglobulins produced in haematological disorders such as multiple myeloma (MM), myeloma of uncertain significance (MGUS), Waldenström’s macroglobulinemia, and amyloidosis. These conditions may present with incidental laboratory findings, such as elevated total protein levels due to the excessive production of immunoglobulins, or more specific abnormalities linked to the CRAB criteria (hypercalcemia, renal impairment, anaemia, and bone lesions), which are commonly associated with MM. 1
Vitamin D plays a crucial role in regulating bone metabolism and calcium homeostasis. In routine clinical practice, anti-osteoporosis drugs such as alendronic acid are combined with vitamin D and/or calcium supplementation to improve their efficacy on bone density increase.2,3
25-hydroxyvitamin D [25(OH) vitamin D)] represents the total vitamin D in the body. It is synthesized in the liver from vitamin D obtained through dietary sources or produced in the skin upon exposure to sunlight. This precursor is stable and circulates in the bloodstream until it is converted into its active form, 1,25-dihydroxyvitamin D [1,25(OH)2 vitamin D], primarily in the kidneys. Parathyroid hormone (PTH)
Testing for 25(OH) vitamin D levels is commonly used to assess an individual’s vitamin D status and determine if supplementation is necessary. Elevated levels of 25(OH) vitamin D may result from either excessive dosing leading to toxicity or from individual predisposition to increased absorption or altered metabolism. 1,25(OH)2 vitamin D toxicity can lead to hypercalcemia due to increased calcium absorption, which poses the primary concern. Another scenario involving abnormal Vitamin D levels is vitamin D resistance. High levels of 25(OH) vitamin D with normal to high PTH values are indicative of vitamin D resistance, assuming that dietary calcium and phosphate intake are adequate, and a differential diagnosis of hyperparathyroidism has been ruled out. Vitamin D resistance specifically refers to the body’s inability to respond to the active form of vitamin D, 1,25(OH)2 vitamin D. It is characterized by a failure of target tissues to respond to 1,25(OH)2 vitamin D, despite its presence, and is usually associated with severe rickets, hypocalcaemia, hypophosphatemia, elevated PTH and alkaline phosphatase (ALK) levels. This autosomal recessive disorder affects calcium and phosphate homeostasis and typically presents in childhood. The routinely measured form, 25(OH) vitamin D, is a precursor to 1,25(OH)2 vitamin D, and it circulates in the bloodstream as a stable marker of overall Vitamin D status. The conversion to 1,25(OH)2 vitamin D is regulated by calcium and PTH. Vitamin D resistance can impair calcium absorption in the intestine, calcium reabsorption in the kidneys, and bone mineralization, potentially contributing to the development of bone disorders such as osteoporosis. 4
The underlying mechanisms of vitamin D resistance are complex and can involve genetic factors as well as acquired conditions, such as chronic kidney disease, certain medications, or disorders affecting vitamin D metabolism. Additionally, abnormalities in vitamin D receptor (VDR) function or downstream signalling pathway may contribute to vitamin D resistance. Diagnosis involves measuring 25(OH) vitamin D, 1,25(OH)2 vitamin D, calcium, and PTH levels, as well as imaging studies to evaluate bone health.6,7
This report presents the case of a 48-year-old man with normal body mass index (BMI), referred to the endocrine department from the rheumatology department for investigation of acromegaly. The patient has been under observation for dorsal vertebral compression fractures and a rib fracture, undergoing antiresorptive therapy with alendronic acid and vitamin D for the past year.
Case report
The patient has been under intermittent follow-up with rheumatology for several years due to a history of kyphosis with chronic compression of the 7th thoracic vertebra (T7), without displacement of the posterior wall and without bone oedema, initially diagnosed through a bone scan. The patient has been receiving treatment with alendronic acid (71 mg per week) and vitamin D (1000 IU/day) since 2021. Additionally, the patient has a history of chronic alcohol consumption and drug abuse, which may interfere with bone metabolism, reducing calcium absorption and impairing bone formation, thereby contributing to decreased bone density. The patient has also experienced repeated injuries and fractures, primarily due to falls or accidents, which may further exacerbate bone weakening.
In January, the patient presented to the emergency department (ED) with back pain without trauma or apparent triggering cause and costal pain after cough effort. The patient underwent to Computerized Tomography (CT-Scan), MRI (Magnetic Resonance Imaging) and bone scintigraphy investigations, observing the known T7 wedging, new wedging on T8, T9 and T10 and a fracture on the 7th rib. Patient was discharged with corticosteroids and was recommended to continue normal therapy with alendronic acid and vitamin D.
Laboratory Results From Presentation at the Emergency Department in January 2022 to MM Diagnosis in November 2022 and Laboratory Results for Acromegaly Investigation.
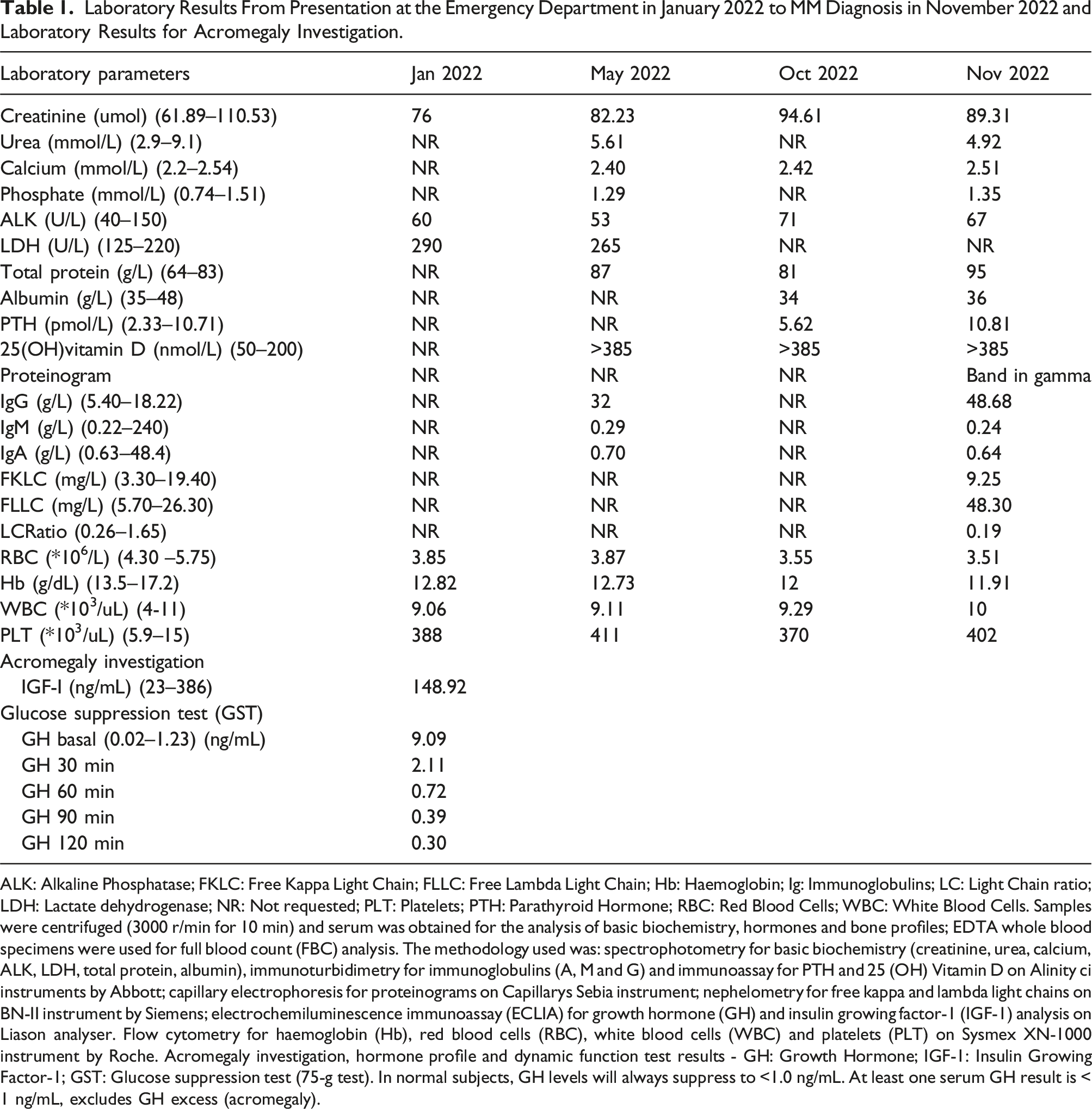
ALK: Alkaline Phosphatase; FKLC: Free Kappa Light Chain; FLLC: Free Lambda Light Chain; Hb: Haemoglobin; Ig: Immunoglobulins; LC: Light Chain ratio; LDH: Lactate dehydrogenase; NR: Not requested; PLT: Platelets; PTH: Parathyroid Hormone; RBC: Red Blood Cells; WBC: White Blood Cells. Samples were centrifuged (3000 r/min for 10 min) and serum was obtained for the analysis of basic biochemistry, hormones and bone profiles; EDTA whole blood specimens were used for full blood count (FBC) analysis. The methodology used was: spectrophotometry for basic biochemistry (creatinine, urea, calcium, ALK, LDH, total protein, albumin), immunoturbidimetry for immunoglobulins (A, M and G) and immunoassay for PTH and 25 (OH) Vitamin D on Alinity ci instruments by Abbott; capillary electrophoresis for proteinograms on Capillarys Sebia instrument; nephelometry for free kappa and lambda light chains on BN-II instrument by Siemens; electrochemiluminescence immunoassay (ECLIA) for growth hormone (GH) and insulin growing factor-1 (IGF-1) analysis on Liason analyser. Flow cytometry for haemoglobin (Hb), red blood cells (RBC), white blood cells (WBC) and platelets (PLT) on Sysmex XN-1000 instrument by Roche. Acromegaly investigation, hormone profile and dynamic function test results - GH: Growth Hormone; IGF-1: Insulin Growing Factor-1; GST: Glucose suppression test (75-g test). In normal subjects, GH levels will always suppress to <1.0 ng/mL. At least one serum GH result is < 1 ng/mL, excludes GH excess (acromegaly).
Throughout the year-long laboratory analysis (Table 1), abnormal toxic levels of 25 (OH) vitamin D (>385 nmol/L) were identified. Initially, the endocrine team had a suspicion of vitamin D resistance due to persistently elevated 25(OH) vitamin D levels and connected in some way with a potential acromegaly. However, true vitamin D resistance is characterized by resistance to the active form, 1,25(OH)2 vitamin D, along with biochemical markers such as hypocalcaemia, hypophosphatemia, elevated PTH, and ALK. These markers were not present in this patient. The subsequent analysis of 1,25(OH)2 vitamin D showed levels within the normal range, further ruling out true vitamin D resistance. The elevated 25(OH) vitamin D levels were more likely due to assay interference rather than resistance to the active form.
The clinical presentation did not align with the biochemical findings, so the laboratory initiated an investigation into potential interference with the 25(OH) vitamin D immunoassay through a three-step simultaneous process (Figure 1). Initially, a portion of the sample was dispatched to an alternative laboratory employing a different platform and immunoassay principle, specifically the Roche platform. Alinity i Vitamin D (Abbott) assay is based on a competitive chemiluminescence immunoassay analysis (CMIA), employing paramagnetic microparticles coated with rabbit IgG antibodies and an acridinium labelled conjugate,
8
while Elecsys Total Vitamin D, 25(OH) vitamin D, (Roche) assays principle is based on electrochemiluminescence binding competitive assay using a vitamin D binding protein (VDBP) labelled with ruthenium complex,
9
a pretreatment step and streptavidin coated microparticles. Result for vitamin D came back greater than 100 nmol/L from Roche assay. Investigation into potential interference: (1) Dilution studies and 25 (OH) Vitamin D analysis by Abbott immunoassay method (2) Vitamin D Total analysis by Roche method (3) Polyethylene glycol (PEG 6000) precipitation analysis.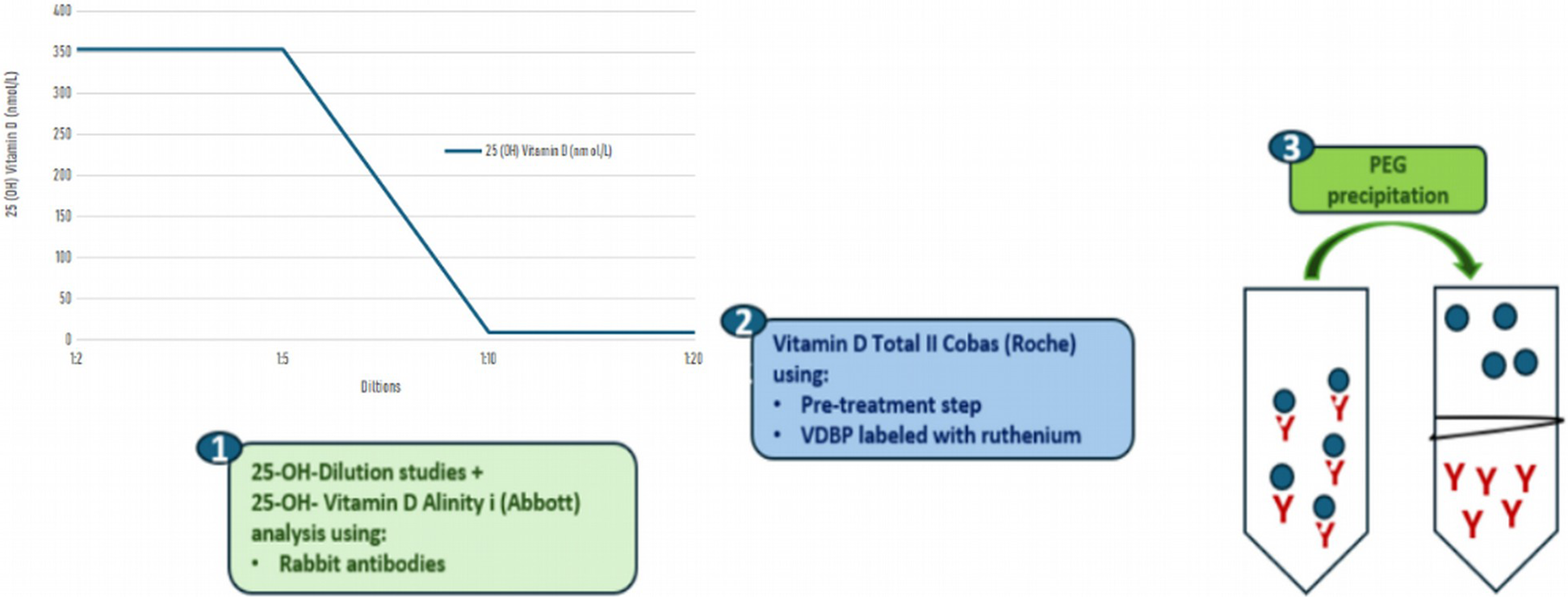
Secondly, a serial dilution study was conducted to address the potential issues of antigen excess. The serial dilutions began at 1:2 (automatic dilution), as recommended by the manufacturer, and were subsequently extended to further (manual) dilutions up to 1:20. Data for dilutions between 1:5 and 1:10 go from concentrations over the measuring range (>385 nmol/L) to concentrations below the lower limit of detection (LLOD <9 nmol/L). No further dilutions between 1:5 and 1:10 were carried out. The results observed exhibited a non-linear dilution pattern, which is a characteristic typically indicative of assay interference.
Lastly, precipitation with a 25% polyethylene glycol (PEG) 6000 solution was conducted to investigate potential interference stemming from macromolecules that could lead to falsely elevated levels detected in the immunoassay as 25(OH) vitamin D. The PEG precipitation test, known for its capability to eliminate immunoglobulins, is commonly utilized in the identification of pseudo hyperprolactinemia 10 induced by macroprolactin but can also effectively remove immunoglobulins in general. The samples were mixed with PEG at a 1:1 dilution ratio and incubated at room temperature for 10 min with gentle agitation. Following incubation, the suspension underwent centrifugation at 4000g for 10 min, after which the supernatant was subjected to repeat analysis using both methods. Result from this analysis was reported as under the LLOD.
The presence of a potentially high molecular weight molecule was identified, which was yielding falsely elevated results on the 25(OH) vitamin D immunoassay. Considering the patient’s clinical presentation, having been referred from rheumatology with bone symptoms and pain, a comprehensive electrophoresis analysis was conducted in conjunction with assessments of immunoglobulins and free light chains in serum, as recommended by the clinical team. The proteinogram revealed a distinct peak corresponding to a monoclonal band, identified as IgG Lambda through immunotyping (Figure 2). The patient was diagnosed of MM, based on three altered factors: the FLC ratio, a band concentration exceeding 30 g/L and bone lesions as described by the International Myeloma Working Group (IMWG). Trace of proteinogram. Monoclonal band corresponding to an IgG Lambda with concentration = 36 g/L.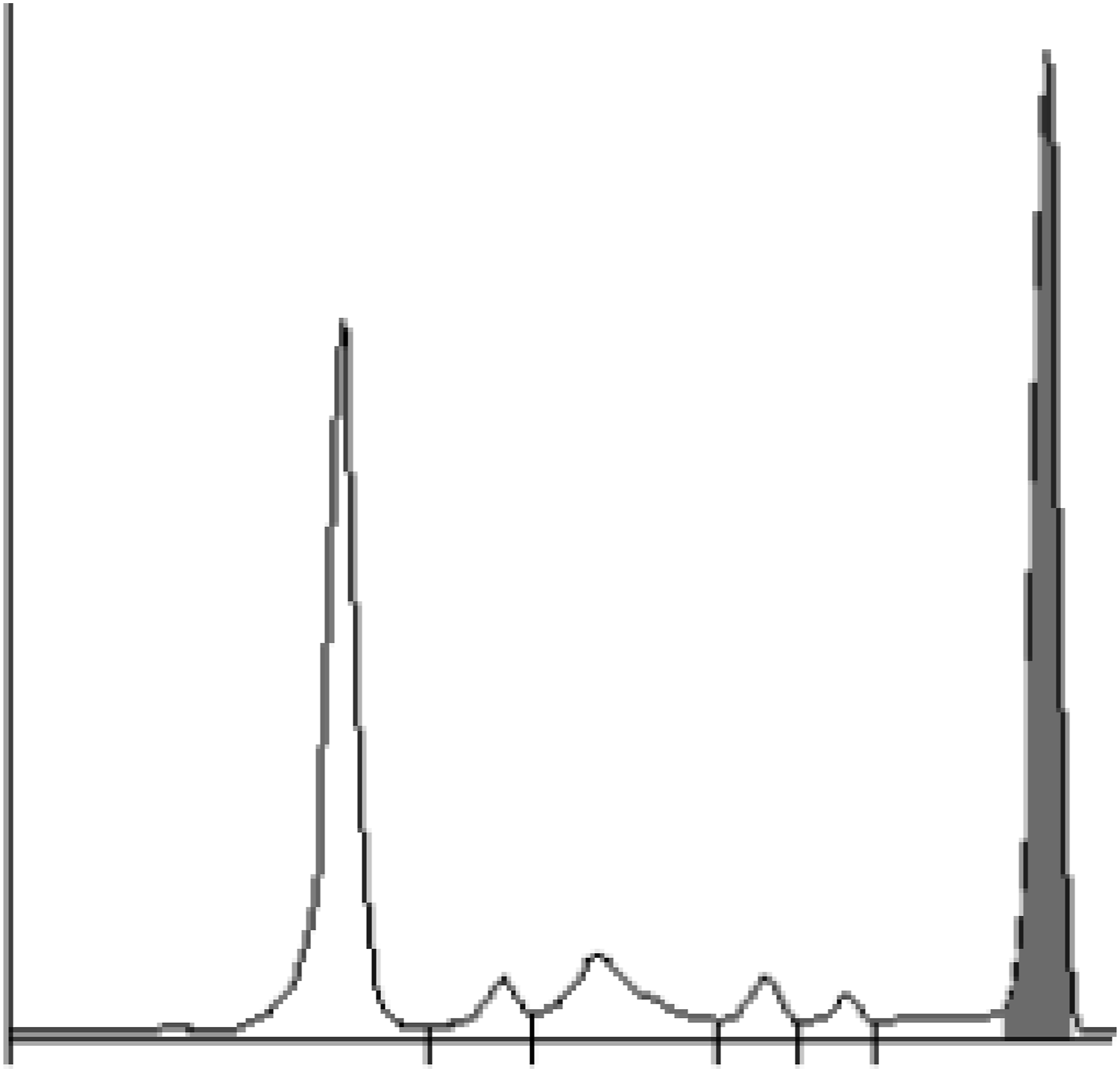
The patient was referred to haematology team and underwent for a bone marrow biopsy to characterize the type of myeloma by visual inspection, flow cytometry and FISH. Patient was diagnosed of IgG Lambda MM (aberrant phenotype, CD38+, CD19-, CD117+, CD27−, CD81−/+, CD56+) with 15% bone marrow infiltration and treated with a combination of Ledanidomide and Dexamethasone and monitored every month.
A critical observation in this case is that, following treatment and the normalization of IgG levels within the reference range, the patient’s vitamin D levels not only stabilized but were confirmed to be deficient. This finding strongly suggests that the initial elevated IgG or monoclonal protein had masked the true vitamin D deficiency. In April 2023, few months after specific MM treatment, a re-analysis of 25(OH) vitamin D was performed. At this point, total IgG levels had decreased from 50.4 g/L to 23 g/L, and the monoclonal band had reduced from 36 g/dL to 18 g/dL. The analysis revealed a significant vitamin D deficiency (14.4 nmol/L), which aligned with the clinical suspicion of deficiency noted in the patient’s history of osteoporosis, a condition that had previously been treated with vitamin D supplementation.
Discussion
This patient had been prescribed alendronic acid and vitamin D for few years by rheumatology specialists due to the underlying disease (kyphosis and osteoporosis). Suspicions arose regarding resistance to vitamin D in connection with the investigation of acromegaly and the presence of toxic levels of vitamin D. Resistance to vitamin D within the context of acromegaly is not extensively addressed in medical literature. Acromegaly is a disease caused by excessive production of GH, usually due to a tumour in the pituitary gland. This condition can affect bone metabolism and calcium balance in the body. Patients with acromegaly have been observed to have an increased prevalence of bone disorders such as osteoporosis and osteoarthritis.11,12 Acromegaly pathognomonic increased level of GH can act as an important regulator of renal vitamin D metabolism.13,14 For instance, IGF-1 can enhance the expression and activity of 1α-hydroxylase in the kidney, which increases levels of active vitamin D (1,25 (OH)2 D) and alters calcium-phosphate homeostasis. This may result in abnormal vitamin D metabolism in some cases. However, a direct causal relationship between acromegaly and vitamin D resistance has not been fully established.15,16
Elevated 25(OH) vitamin D levels, despite cessation of supplementation in October 2022, initially raised suspicion of vitamin D resistance. However, further investigation analysing 1,25(OH)2 vitamin D levels clarified the situation. Unlike 25(OH) vitamin D, which is a precursor, 1,25(OH)2 vitamin D represents the active form and was found to be within normal ranges, indicating the absence of vitamin D resistance. Measuring 1,25(OH)2 vitamin D can be pivotal in investigating resistance to vitamin D. This active form of vitamin D is regulated by the PTH and plays a crucial role in calcium homeostasis, bone metabolism, and immune function. In cases where resistance to vitamin D is suspected, assessing levels of 1,25(OH)2 vitamin D can provide valuable insights into the body’s response to vitamin D and the conversion of vitamin D into its active forms in target tissues.
To rule out interference, multiple techniques were employed, including PEG precipitation and dilution studies, which confirmed the presence of a high molecular weight molecule causing falsely elevated 25(OH) vitamin D readings. However, the reference method for accurate measurement is liquid chromatography-tandem mass spectrometry (LC-MS/MS) due to its superior specificity. 17 Unfortunately, this technology was not available at the medium-sized hospital where the patient was treated, nor in any of the nearby hospitals in the region. Immunoglobulin interference due to the patient’s underlying MM was identified as the source of the elevated results. Once the interference subsided, the 25(OH) vitamin D levels normalized, aligning with the patient’s true deficiency.
Interference from immunoglobulins is not addressed in the Abbott or Roche package insert. However, interference studies have been conducted with protein concentrations of up to 120 g/L, demonstrating a potential impact of up to a 4.4% variance in the concentration of 25(OH) vitamin D.
8
In this instance, while the protein concentration was moderately high in two
Several similar cases have been published in recent literature, but in most scenarios, there were other biochemical characteristics, such as an increased calcium or total protein concentration that pointed to interference caused by high concentration of immunoglobulins due to MM.18,19 The novelty of this case resides in the fact that the observed interference contributed to achieving an accurate diagnosis in a patient with a complex and ambiguous clinical presentation.
Footnotes
Acknowledgements
Clinical analysis staff and endocrinology service, Hospital Puerta del Mar.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
None declared.
Ethical statement
Guarantor
None declared.
Contributorship
NRR and AJR collect the data and wrote the first draft of the manuscript. CLT was involved in clinical care of the patient. All authors reviewed, contributed to and edited the manuscript and approved its final version.