
Abstract
Background
Cerebrospinal fluid (CSF) spectrophotometry is well-established in the UK for measuring CSF bilirubin and oxyhaemoglobin to aid in the diagnosis of subarachnoid haemorrhage. Although it is known that some antibiotics and large amounts of oxyhaemoglobin interfere in the spectrophotometric analysis of CSF bilirubin, there is little published evidence about the impact of such interferences.
Methods
Experimental samples were distributed to participants in the UK National External Quality Assessment Service (NEQAS) for Immunology, Immunochemistry and Allergy EQA programme for CSF haem pigments. Distribution 244 consisted of a pair of matched samples but with sample 244-2 containing an increased amount of oxyhaemoglobin compared to sample 244-1. Distribution 251 consisted of a pair of matched samples but with sample 251-2 containing additional doxycycline at a concentration of 0.5 µg/mL compared to sample 251-1. Participants analysed the samples spectrophotometrically and absorbance values were returned to UK NEQAS.
Results
The net bilirubin absorbance (NBA) was significantly reduced in the presence of both interferants; adding 0.6% oxyhaemoglobin decreased the NBA by a mean of 55.9% and adding 0.5 µg/mL doxycycline decreased the NBA by a mean of 14.3%. Wilcoxon signed rank tests showed the NBA was significantly different for sample 2 compared to sample 1 for both distributions.
Conclusions
Increased amounts of oxyhaemoglobin and the presence of doxycycline can both negatively interfere with NBA. The interference is subtle and difficult to detect but has the potential to change a true positive result to a false negative, highlighting a significant limitation of the CSF spectrophotometry technique.
Background
Subarachnoid haemorrhage (SAH) is defined as bleeding into the subarachnoid space surrounding the brain and is most commonly caused by rupture of an intracranial aneurysm. 1 SAH typically presents with a sudden, severe headache that peaks within 1 to 5 min and lasts for more than an hour. 2 SAH is a neurological emergency and causes substantial morbidity and mortality. Cumulative case fatality rates after SAH are 25–30% on day one with 12% of all aneurysmal SAH patients dying before receiving medical attention. 3
The hyperdense appearance of blood in the subarachnoid space on a non-contrast computed tomography (CT) scan of the head is the primary diagnostic test for SAH. 1 Modern, third-generation scanners will detect cases with 100% sensitivity and specificity if performed within 6 h of symptom onset and interpreted by an experienced radiologist. 4 However, the sensitivity drops to 85.7% if the CT scan is performed greater than 6 h after the onset of symptoms. 4
In late presenting or CT-negative cases where clinical suspicion of SAH remains high, a second-line diagnostic test may be required. This can be done by biochemical analysis of cerebrospinal fluid (CSF) for the pigments oxyhaemoglobin and bilirubin. When blood enters the subarachnoid space, red blood cells undergo lysis and phagocytosis. Oxyhaemoglobin is released which is then enzymatically converted into bilirubin. 5 Detection of these pigments in CSF can aid in the diagnosis of SAH. Patients whose CT head scans and/or CSF analysis are suggestive of SAH will typically proceed to angiography to help identify the pathology and anatomy relating to the bleed and to plan the best options for treatment. 1
The phrase “xanthochromia” is used to describe increased bilirubin in CSF which may result in a yellow discolouration of the normally clear and colourless CSF. Historically, visual inspection alone was used to assess xanthochromia. However, this method has been widely refuted 6 and there are now well-established guidelines for the assessment of oxyhaemoglobin and bilirubin in CSF by spectrophotometry. 5 This method involves scanning the CSF between 350 and 600 nm, drawing a predicted baseline which forms a tangent to the scan between 350 and 400 nm and again between 430 and 530 nm and then measuring the net oxyhaemoglobin absorbance (NOA) above the baseline at approximately 415 nm and the net bilirubin absorbance (NBA) above the baseline at 476 nm5.
Unlike oxyhaemoglobin, which may form in vivo or in vitro, CSF bilirubin can only form in vivo as it is dependent on enzymes present in macrophages and other cells of the leptomeninges. 7 Therefore, an increased CSF bilirubin is a key finding in the investigation of SAH. An NBA >0.007 AU is considered diagnostically supportive of SAH although there may be some caveats to this if the CSF total protein or serum bilirubin is also raised. 5 In some circumstances, an adjusted NBA can be calculated to attempt to compensate for an increased serum bilirubin. 5 When xanthochromia is assessed spectrophotometrically after a negative or non-diagnostic CT head, the assay has a sensitivity of 100% and specificity of 95.2% for SAH. 8
The publication of the Revised National Guidelines for Analysis of CSF for Bilirubin in Suspected SAH 5 greatly improved laboratory performance when assessing xanthochromia by providing details of an evidence-based method, promoting best practice for sample handling and offering guidance for interpretation. 9 However, there are limitations to spectrophotometry as a method. Assessment of a raised CSF bilirubin is dependent on absorbance above a baseline at a single wavelength, so other substances that absorb in the region of 350 to 600 nm, if not removed by centrifugation, can potentially interfere by impacting on the predicted baseline. As an example of this phenomenon, studies have demonstrated that CSF samples stored long term will show an increasing absorbance at 380 nm over time that impacts on the assessment of NBA. 10
The guidelines for spectrophotometry state that oxyhaemoglobin may interfere with the detection of bilirubin and is a confounding element in interpretation. They advise that if the NOA is greater than 0.1 AU then the NBA will be underestimated, and the guidelines provide a suitable interpretative comment for this scenario. 5 The evidence for using a cut-off of 0.1 AU in this situation appears limited, based on an unpublished experiment analysing samples with increasing bilirubin and oxyhaemoglobin concentrations, and supported clinically by evidence from 29 patients with NBA ≤0.007 AU who had angiography. In 2 of these 29 cases, an aneurysm was identified despite the low NBA and in one of these the NOA was >0.1 AU.
There are also recent publications that have highlighted potential interference in spectrophotometry by the antibiotics tetracycline, doxycycline and metronidazole.11,12 All 3 of these antibiotics have absorption spectra in the range of interest when investigating xanthochromia. Doxycycline has an absorbance maxima between 350 and 375 nm, 13 tetracycline has an absorbance maxima at 357 nm, 14 and metronidazole has an absorbance maxima at 340 nm. 15
We decided to further investigate the impact of these endogenous and exogenous interfering substances using the UK NEQAS for Immunology, Immunochemistry & Allergy (IIA) external quality assurance programme for CSF haem pigments. With this scheme a pair of samples of artificial CSF matrix are distributed to participants for the analysis of bilirubin and oxyhaemoglobin. This provides the opportunity for a wide-scale study of the impact of increased amounts of oxyhaemoglobin and the presence of antibiotics on spectrophotometric assessment of CSF bilirubin.
Method
Preparation of samples
In August 2024 and February 2025, distributions 244 and 251, respectively, UK NEQAS prepared specific samples as part of the CSF haem pigments scheme to investigate the limitations of spectrophotometry for the analysis of xanthochromia. The samples used in these distributions were prepared as normal using an artificial matrix to replicate the characteristics of CSF and spiked with varying quantities of a bilirubin product (Beckman) and oxyhaemoglobin (fresh human blood). Approximately 300 mL of each sample was prepared to allow distribution of 0.5 mL to each of the 212 participants.
Constituents of experimental samples distributed by UK NEQAS and summary of results received from participants.
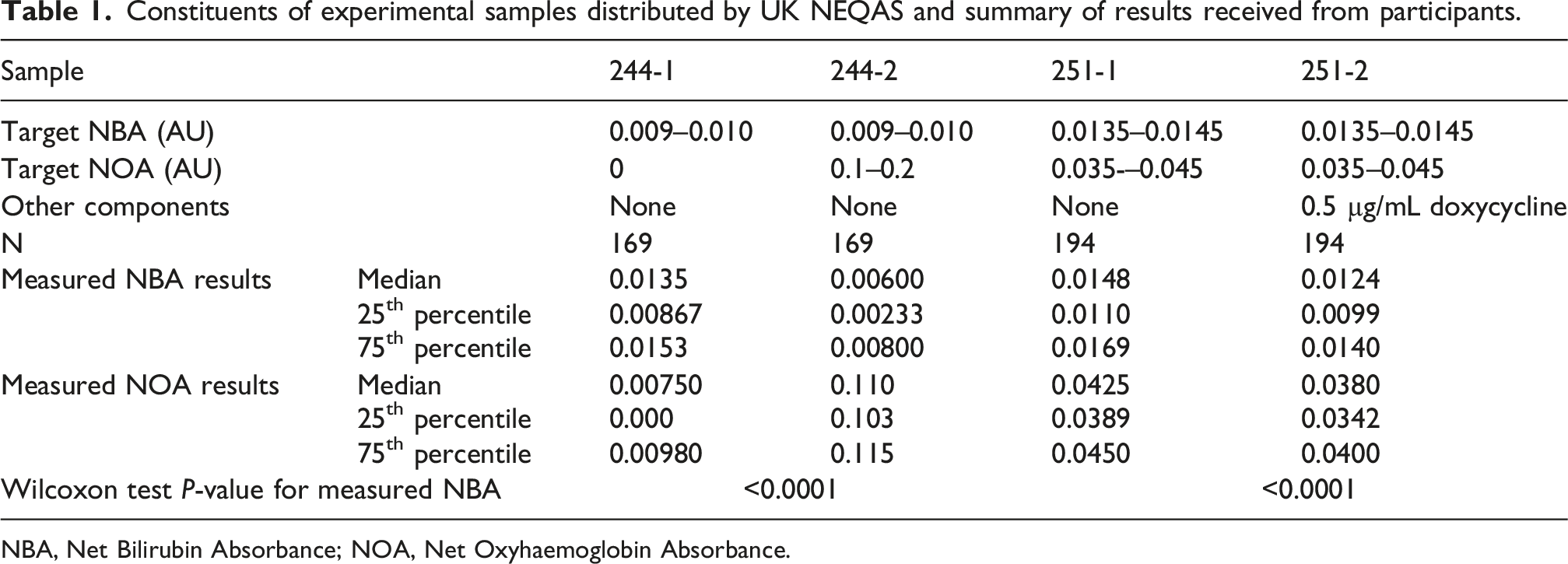
NBA, Net Bilirubin Absorbance; NOA, Net Oxyhaemoglobin Absorbance.
For distribution 251, paired samples were designed to assess the impact of the presence of doxycycline in the sample on the measurement of NBA. Sample 251-1 was spiked with bilirubin, to give a target NBA of 0.0135-0.0145 AU, and oxyhaemoglobin, to give a target NOA of 0.035-0.045 AU. Sample 251-2 was spiked with the same concentrations of bilirubin and oxyhaemoglobin but also had added doxycycline (Table 1).
5 mg of doxycycline monohydrate (Merck) was dissolved in 980 µL of water and 20 µL 1 mol/L hydrochloric acid (Merck) to give a solution of 5 mg/mL. This was then further diluted in phosphate buffered saline (Merck) to give an intermediate solution of 100 µg/mL which was spiked into sample 251-2 to give a final concentration of 0.5 µg/mL.
Data collection and analysis
Participants returned their NBA and NOA results for distributions 244 and 251 as per normal practice. If a complete set of 4 results was not received from a participant, these sets were excluded.
The data for each distribution was collated separately. Statistical analysis including histogram plots and two-sided Wilcoxon signed rank tests was carried out using Analyse-it software for Microsoft Excel. A P-value <.05 was considered significant.
Results
Distribution 244 – Impact of increasing oxyhaemoglobin on NBA analysis
169 complete sets of NBA and NOA results were included in the data analysis (43 registered participants did not return a complete set of results so were not included). For sample 244-1, the median measured NOA was 0.0075 AU and the median measured NBA was 0.0135 AU. For sample 244-2, which contained the same amount of spiked bilirubin as 244-1 but an increased amount of spiked oxyhaemoglobin, the median NOA was 0.11 AU and the median NBA was 0.006 AU (Table 1). An example spectrophotometric scan of these samples demonstrates an oxyhaemoglobin peak at 418 nm in sample 244-2 that is absent in sample 244-1 (Figure 1). Example spectrophotometric scans of sample 244-1 without oxyhaemoglobin and sample 244-2 with oxyhaemoglobin. The dashed line represents the baselines above which the NOA and NBA were measured. In this example, 244-1 had a measured NOA of 0.01 and an NBA of 0.009. Sample 244-2 had an NOA of 0.10 and an NBA of 0.000.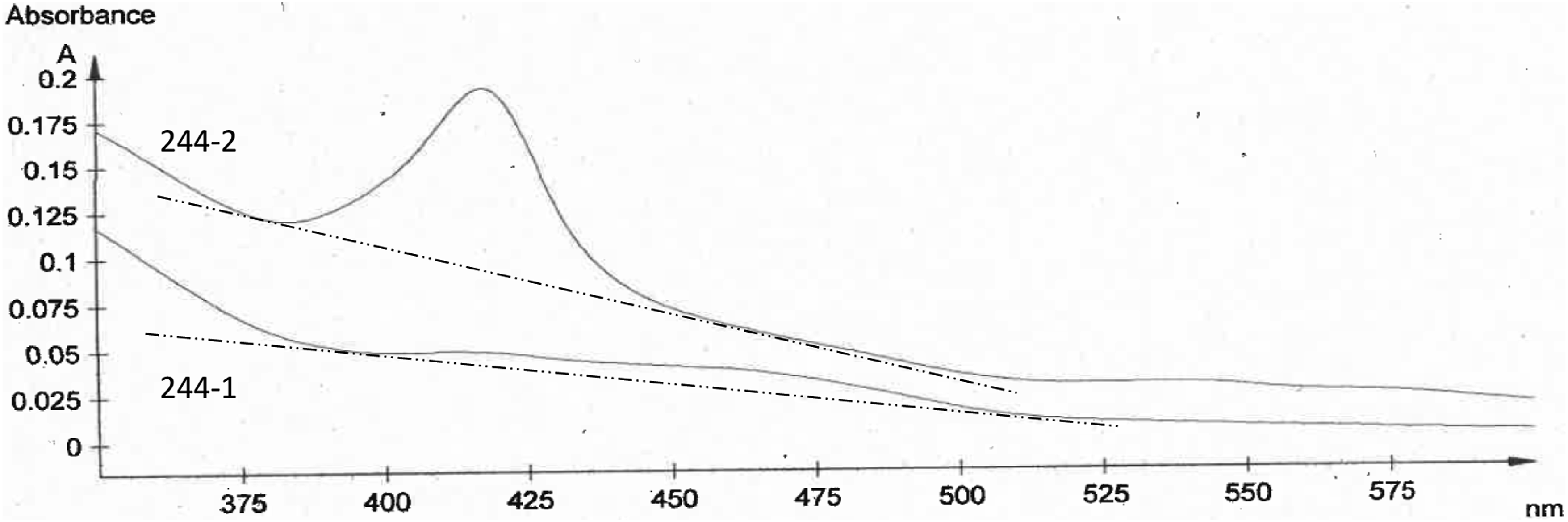
Histograms displaying the spread of results show the NOA to be lower in sample 244-1 than 244-2 as expected from the spiked values (Figure 2 (A) and (B)). Despite the same spike amount of bilirubin in both 244-1 and 244-2, a shift in NBA to lower values is seen when comparing the histogram for 244-2 to 244-1 (Figure 2 (C) and (D)). Comparison of the spread of NOA and NBA results from participants for distribution 244: (A) 244-1 NOA, (B) 244-2 NOA, (C) 244-1 NBA and (D) 244-2 NBA.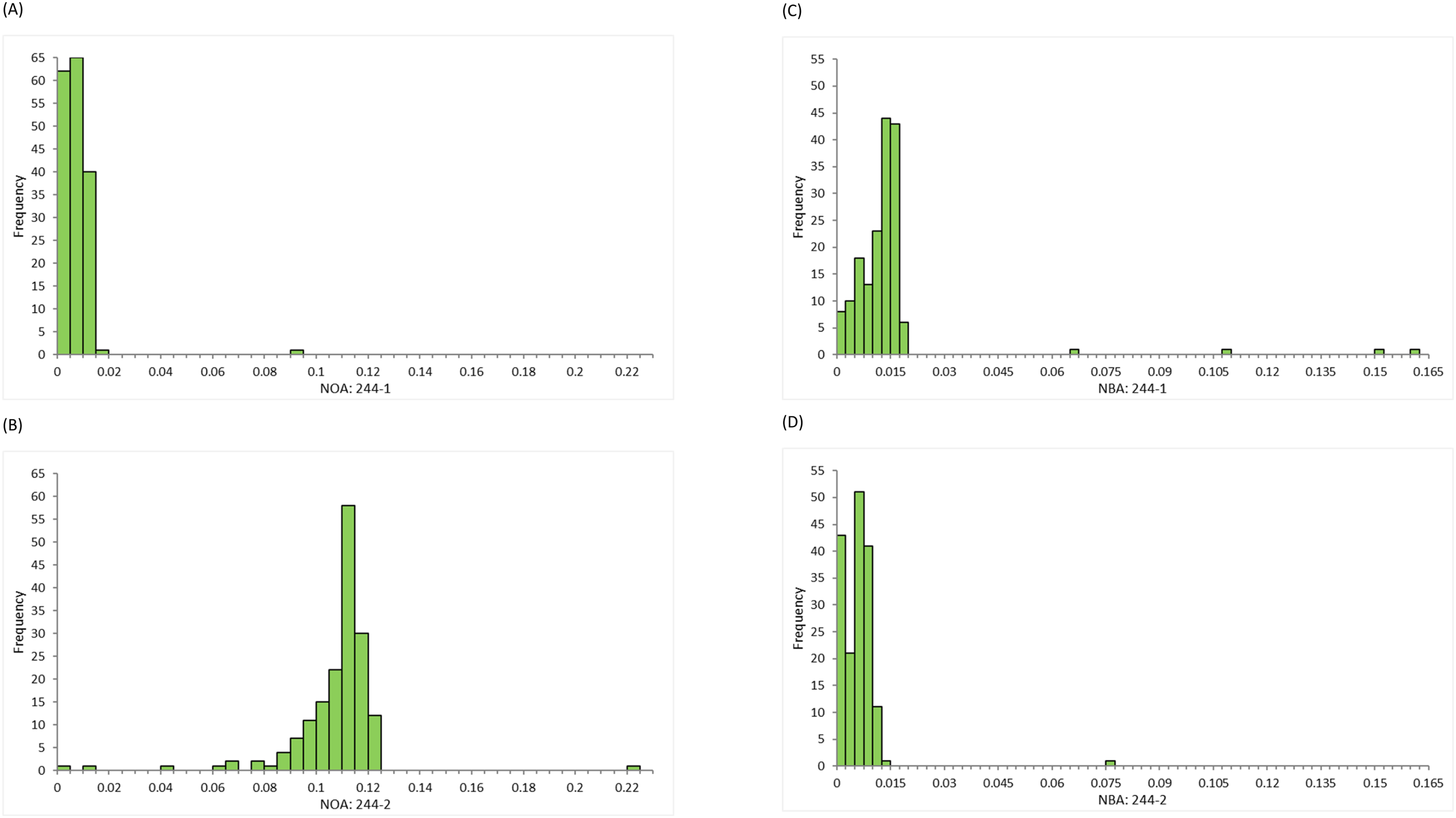
Of the 169 sets of data, 157 (93%) had a lower NBA for sample 244-2 than for 244-1. The mean absolute difference when comparing 244-2 NBA to 244-1 NBA was −0.0085 AU and the mean percentage difference was −55.9%. A Wilcoxon signed rank test confirmed that the 244-2 NBA values were significantly different than the 244-1 NBA values with p < .0001.
Distribution 251 – Impact of doxycycline on NBA analysis
194 complete sets of NBA and NOA results were included in the data analysis (18 registered participants did not return a complete set of results so were not included). For sample 251-1, the median measured NOA was 0.0425 AU and the median measured NBA was 0.0148 AU. For sample 251-2, the median measured NOA was 0.0380 AU and the median measured NBA was 0.0124 AU (Table 1). Histograms of the results demonstrate a shift in both NOA and NBA to lower values when comparing sample 251-1, without doxycycline, to 251-2, with doxycycline (Figure 3). Comparison of the spread of NOA and NBA results from participants for distribution 251: (A) 251-1 NOA, (B) 251-2 NOA, (C) 251-1 NBA and (D) 251-2 NBA.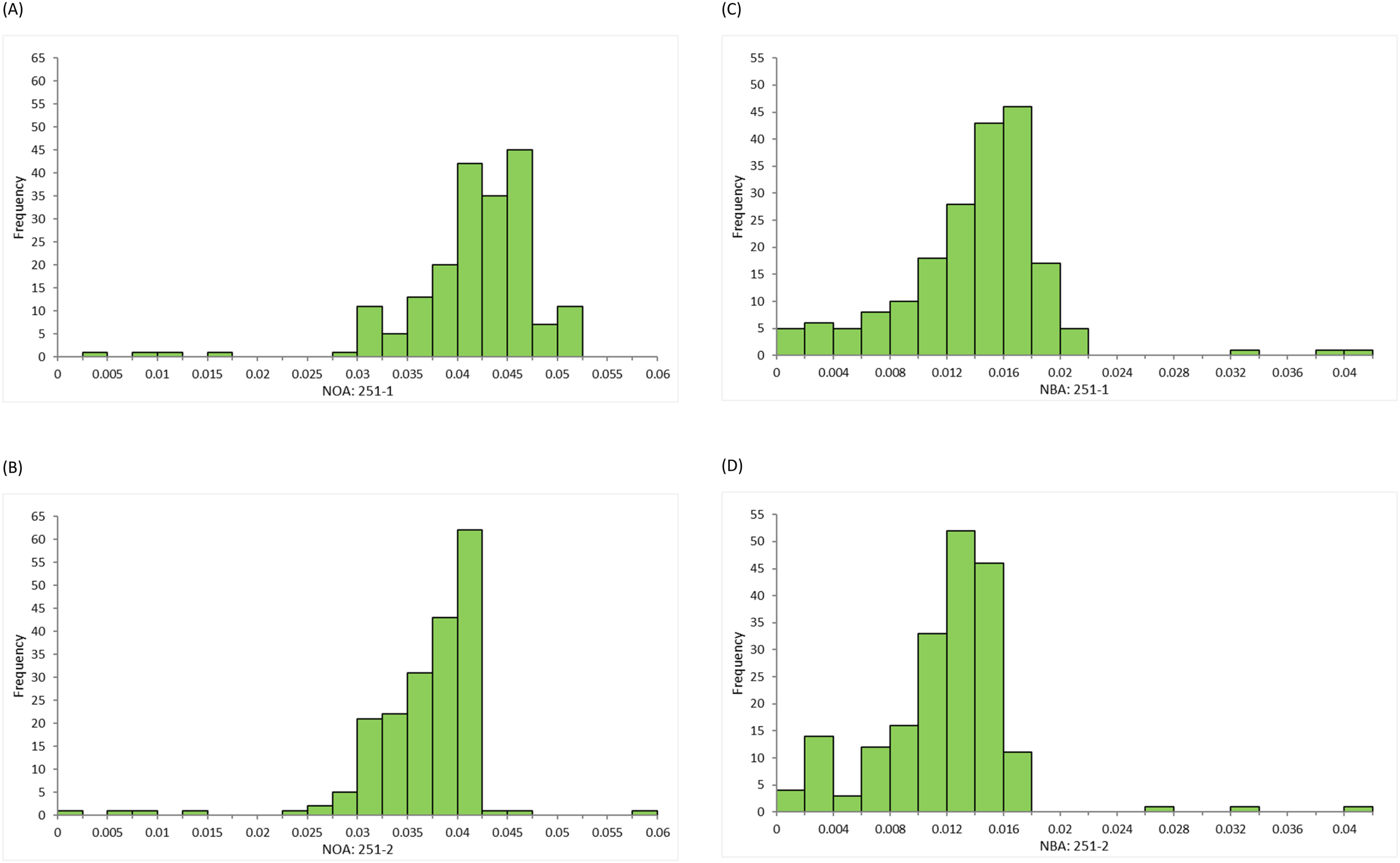
An example spectrophotometric scan of these samples shows sample 251-2 with doxycycline has an increased absorbance between 350 nm and 400 nm compared to sample 251-1 without doxycycline (Figure 4). No participants commented on the possible presence of an interfering substance. Example spectrophotometric scans of sample 251-1 without doxycycline and sample 251-2 with doxycycline. The dashed line represents the baselines above which the NOA and NBA were measured. In this example, 251-1 had a measured NOA of 0.05 and an NBA of 0.016. Sample 251-2 had an NOA of 0.04 and an NBA of 0.014.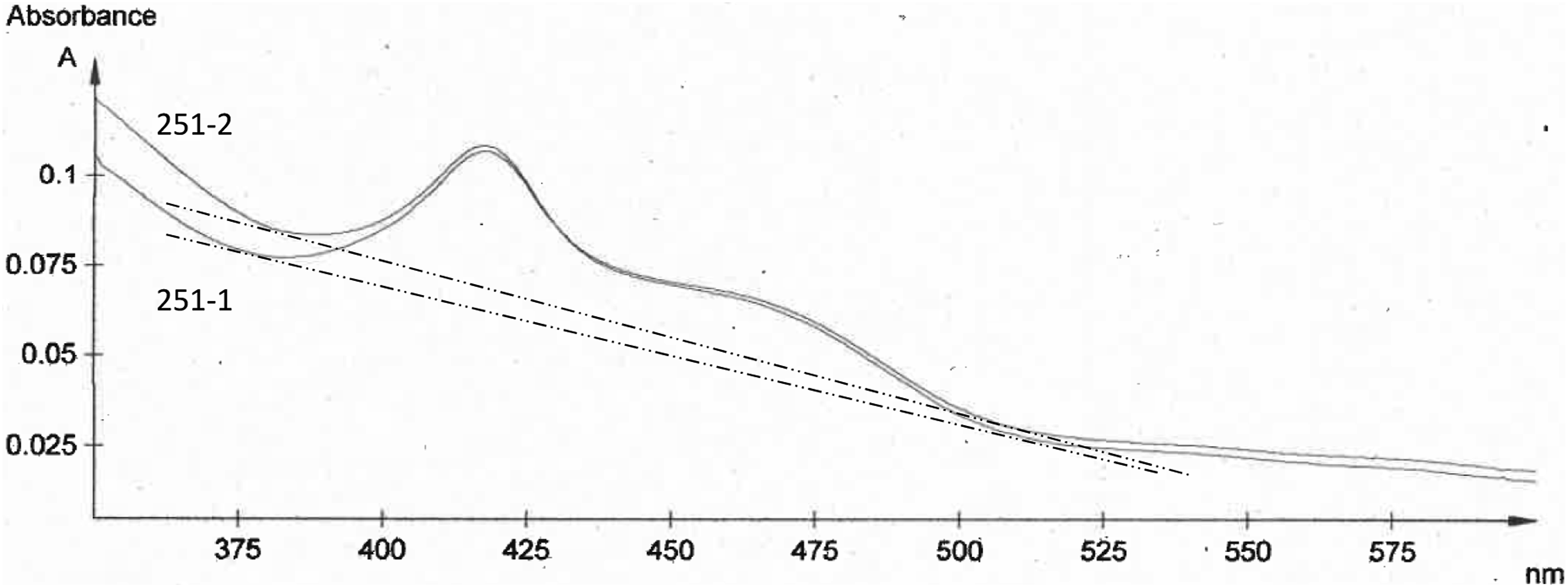
Of the 194 sets of data, 175 (90%) had a lower NBA for sample 251-2 than for 251-1. The mean absolute difference when comparing 251-2 NBA to 251-1 NBA was −0.0022 AU and the mean percentage difference was −14.3%. A Wilcoxon signed rank test confirmed that the 251-2 NBA values were significantly different than the 251-1 NBA values with p < .0001.
Discussion
We have demonstrated that measured NBA can be significantly reduced by the addition of substances that absorb at wavelengths in the region of 350–400 nm. These interfering substances may be endogenous, for example, oxyhaemoglobin, or exogenous, for example, doxycycline. The increased absorption between 350 nm and 400 nm can steepen the slope of the baseline drawn, thus decreasing the measured NBA above the baseline at 476 nm.
We found that adding 0.6% oxyhaemoglobin to a sample decreased the NBA by a mean of 55.9% and adding 0.5 µg/mL doxycycline decreased the NBA by a mean of 14.3%. The clinical significance of such a decrease will depend on the starting concentration of bilirubin in the CSF. In cases with a markedly raised bilirubin, the presence of an interfering substance may not affect interpretation if the underestimated NBA remains >0.007 AU. However, in cases where the actual NBA is only moderately raised above the 0.007 AU cut-off, any underestimation could have a significant impact, turning a “positive” result into a “negative” result for xanthochromia.
The Revised National Guidelines for Analysis of CSF for Bilirubin in Suspected SAH do make provision for the potential interference of oxyhaemoglobin in NBA analysis. If the NBA is ≤0.007 AU and the NOA is >0.1 AU, the guidelines recommend reporting the result as “Oxyhaemoglobin is present in sufficient concentration to impair the ability to detect bilirubin. SAH not excluded” 5 which is supported by our findings. However, given the significant decrease in NBA we found when the NOA was approximately 0.11 AU, further work is needed to investigate the impact of a wider range of oxyhaemoglobin concentrations.
Similarly for doxycycline, we only assessed the impact of one concentration, 0.5 µg/mL. Previous publications confirm that this was an appropriate physiological and pharmacological concentration to test, as patients being treated with oral doxycycline therapy were found to have CSF concentrations in the range of 0.4–1.9 µg/mL. 11 We found that, despite having a potentially significant impact on the measured NBA, doxycycline of concentration 0.5 µg/mL only subtly affects the slope of the scan, making it very difficult for a user to identify when doxycycline may be present. Higher concentrations can have a more obvious impact on the scan, making it impossible for a baseline to be drawn. 11 Similar to oxyhaemoglobin, further work is required to investigate the variable impact of a wider range of doxycycline concentrations.
It is difficult to predict the scale of the potential issue. Oxyhaemoglobin is produced during physiological processes following SAH, and the concentration will vary depending on the initial blood load and the timeframe between the bleed and lumbar puncture (LP). Although the CSF bilirubin peak can be greater than the oxyhaemoglobin peak in the second week after a bleed, 5 it is unfeasible to delay an LP, so oxyhaemoglobin in the CSF sample cannot be avoided.
The amount of oxyhaemoglobin in the sample will also be higher if peripheral blood is introduced into the CSF at the sampling site during a traumatic tap. The frequency of traumatic LPs is estimated to be between 10 and 30%, although this varies depending on the setting and how a traumatic LP is defined. 16 Oxyhaemoglobin release from red blood cells introduced to the sample during a traumatic tap can be minimised by not transporting the sample in a pneumatic tube system and by centrifuging the CSF sample promptly after collection. 5
Doxycycline is an antibiotic given orally for various bacterial infections including respiratory, skin, sexually transmitted and tick-borne diseases. 17 Prescribing patterns of doxycycline are variable, although a downward trend in response to antibiotic resistance was recently published. 18 A previous publication identified 6 out of 404 CSF spectrophotometric scans (1.5%) that were majorly affected by doxycycline interference. 12 However, this may be an underestimation of the potential impact as our work suggests that the presence of doxycycline in CSF can subtly influence the measured NBA without rendering the scan uninterpretable.
There are a number of limitations to our study. Some participants did not return complete sets of results so were not included in data analysis. Due to the large volume of testing material required for distribution to all participants in the EQA scheme, an artificial matrix was used rather than organic CSF. We were also unable to control for the storage of samples after receipt in participant laboratories nor the testing techniques used by individual departments although advice in these aspects is readily available. If samples were not analysed promptly on receipt, this could have been a contributing factor to a falsely low NBA. However, raw data from UK NEQAS suggests both samples are typically analysed on the same day by participants (data not shown) and we do not think that these limitations detract from the overriding message of our work; endogenous and exogenous substances in a CSF sample that absorb in the region of 350–400 nm can negatively interfere in NBA measurement.
Given the difficulties identified here with spectrophotometry as a method for the detection of xanthochromia, it is important that ways to improve the current method or potential alternative methods that would be less impacted by interference are considered. Some publications have suggested using alternative wavelengths in spectrophotometry to minimise interference and improve accuracy,19,20 but this approach could increase the complexity of spectrophotometry interpretation in the routine clinical laboratory.
Measuring an alternative analyte such as ferritin21–24 has also been considered. Ferritin is synthesised in the central nervous system following an intracranial bleed in response to the iron released from haemoglobin degradation. 23 The production of ferritin takes time however, and the measurement of CSF ferritin may be most suited to late presenting cases.24,25 CSF ferritin also has too low a specificity to function as a stand-alone test 23 but can potentially be used in combination with spectrophotometry. This may be of particular relevance to cases where spectrophotometry is compromised by possible interference.
Adapting automated serum bilirubin methods to measure the lower concentrations found in CSF has also been investigated.26–29 This approach could have the advantage of providing a robust and straightforward screen, but further work is required to understand the discrepancies between cut-offs for bilirubin absorbance and concentration for defining SAH that have been identified. 30 As the spectrophotometric method promoted by the Revised National Guidelines 5 is well-established in the UK and has proven clinical utility, 31 none of these alternative approaches have yet been widely adopted.
Until an alternative, interference free, approach for the assessment of CSF xanthochromia has been extensively validated, routine clinical laboratories have few options. CSF spectrophotometric scans with gross interference, where it is impossible to draw a baseline, are easily identified and should be reported as containing an interfering substance making the sample uninterpretable for xanthochromia. This is unsatisfactory for all concerned. CSF spectrophotometric scans with subtle interference are difficult to identify, but laboratories should be cautious about reporting negative CSF xanthochromia results if the NBA is close to 0.007 AU. In these cases, consideration should be given to the angle of the baseline drawn and whether there is increased absorbance in the region of 350–400 that may be falsely lowering the NBA. It may be prudent to identify which antibiotics the patient has been prescribed, and a cautionary comment could be added to the report.
In conclusion, we have shown that oxyhaemoglobin and doxycycline can reduce NBA when assessing CSF by spectrophotometry in the investigation of SAH. The interference is subtle and may not be immediately apparent yet can have a meaningful impact. Users need to be vigilant for potential interfering substances increasing absorbance between 350 and 400 nm, particularly in cases where the NBA is close to the significant cut-off of 0.007 AU.
Footnotes
Acknowledgements
Thank you to the teams at UK NEQAS for Immunology, Immunochemistry and Allergy and The Neuroscience Laboratories at The Walton Centre for their support with this project.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Not applicable.
Contributorship
All authors were involved in the project concept. The project was designed by KB, MS and DP. Data analysis and manuscript preparation were completed by KB. All authors reviewed and approved the final manuscript.
Guarantor
Katherine Birch.