
Abstract
Objectives: Police have long played a central role in the management of people experiencing mental illness. This study explored: (1) the frequency of contact between the police and people experiencing mental illness; (2) the way in which police officers’ knowledge and the sources of information used relates to various dispositions; (3) the signs, symptoms and behaviours that police officers consider are associated with mental illness; and (4) the challenges police face in this respect when performing their duties.
Method: A survey was completed by 3,534 police officers in Victoria, Australia. Canonical correlations were used to explore the ‘approach styles’ of police when responding to people with a mental illness. Thematic analyses, based on grounded theory, were utilized to examine and code open-ended responses.
Results/conclusions: Police reported that a considerable amount of their time each week was spent dealing with people they believed to be mentally ill. These encounters were reportedly associated with considerable practical difficulties for police, both in terms of knowing how to deal with people experiencing mental illness and how to best find appropriate supports for them. The most common results of their encounters were instigating a mental health apprehension, followed by arrest, but decision-making was influenced by the differential weight police placed on different sources of information received at the scene. Recommendations for police training, while based on practical wisdom, need to be multi-modal and should engage mental health experts in design and delivery.
Keywords
More than 40 years ago, Bittner highlighted the challenges faced by police officers in their encounters with people experiencing mental illness (Bittner, 1967). Since that time, changes in policy, practice and legislation have all contributed to a common perception that there is a scarcity of mental health resources. This argument has been used to explain, in part, why there is currently a high frequency of contact between the police and people experiencing mental illness (Bonovitz and Bonovitz, 1981; Menzies, 1987; Patch and Arrigo, 1999; Pogrebin and Poole, 1987; Teplin and Pruett, 1992). A high degree of contact between police officers and people experiencing mental illness is also supported by anecdotal reports of police officers (Wylie, 1990), the high prevalence of psychiatric symptoms among detainees in police cells (Ogloff et al., 2010) and, concomitantly, an increased rate of major mental illnesses found in prison populations as compared to estimated rates in the community (Butler and Allnutt, 2003; Fazel and Danesh, 2002; Ogloff, 2002).
The over-representation of mental illness in prisons has been attributed, in part, to the process by which police officers may arrest people experiencing mental illness due to an absence of appropriate mental health options (Holley and Arboleda-Florez, 1988; Lamb et al., 2002; Teplin and Pruett, 1992), although there are contradictory viewpoints on this (Bonovitz and Bonovtiz, 1981; Engel and Silver, 2001; Green, 1997). It might be that symptoms of mental illness have been ‘criminalised’, with mentally ill people being arrested for behaviours that are actually a direct consequence of their illness (e.g. bizarre behaviour and public order offences). What is clear from large-scale epidemiological data linkage studies is that individuals with severe mental illnesses have a disproportionately high offence, and particularly violent offence, rate compared to people without such diagnoses (e.g. Wallace et al., 2004). Regardless of whether the police play a role in any ‘criminalisation of the mentally ill’ (Lamb et al., 2002), when dealing with people experiencing mental illness in their work, police officers can and do have to make difficult decisions, often without the assistance of experts in mental health.
Encounters with people experiencing mental illness are now considered part and parcel of contemporary police practice; with recent police reforms emphasizing the need to go beyond what was traditionally the police’s core functions of catching and locking up the criminals, to a more global remit covering broader concepts of security, harm reduction and prevention (Stenning and Shearing, 2005). Against this social welfare doctrine to community policing, the police have three options open to them when faced with resolving an encounter: (1) arrest, if the person has committed a crime pursuant to the relevant criminal code in that jurisdiction; (2) detain and convey the person to a place of safety for a proper assessment of safety and risk, as set out in relevant mental health legislation; or (3) to use their discretionary powers. These ‘street-level decision-making’ processes, universal to police in all jurisdictions under the guidance of locally determined mental health legislation and criminal codes, are influenced by a number of practical and logistical factors. Of all of these options, it is their decision-making around the enactment of their discretionary powers that has been of most interest. Within this, the potential influence of the encounter being police- or citizen-initiated (Sanders and Young, 2005: 229) has received attention as these characteristically different encounters carry with them a whole range of, sometimes different, political and social expectations. These forces can be particularly problematic when the individual or group of ‘interest’ are socially marginalized and stigmatized (Kariminia et al., 2007) and, to an extent, demonized by the local community (Dinos et al., 2004; Hudson, 2006).
Quite apart from societal pressures, police are faced with the fundamental complication of their own ability to recognize signs, symptoms and behaviours associated with mental illness (Bayney and Ikkos, 2003; Finn and Stalans, 1997; Green, 1997; LaGrange, 2003). In Victoria, although police are not compelled or required to exercise clinical judgement in these situations under their powers in the Mental Health Act 1986 (Vic), their ‘duty of care’ in these encounters has recently been debated in Stuart v. Kirkland-Veenstra [2009] HCA 15. Scott (2010) argues on the grounds of what would be reasonably expected when encountering anyone in a vulnerable state, that police should in fact err on the side of caution and facilitate access to a proper assessment of safety and risk.
Different jurisdictions have taken individualized approaches to providing training on mental health awareness to police officers. One recent American study suggested the median time devoted to this training was 6.5 hours, but this varied widely and was commonly grouped with information about other vulnerable populations. Some developed and delivered the training totally in-house, while others either liaised with local mental health providers on content or developed and delivered part or all of the content (Hails and Borum, 2003). Whatever the case, Borum (2000) argues that the training is unlikely to be sufficient to fundamentally change the nature or outcome of the encounters. The lack of training in this regard has been attributed to the excessive (and fatal) use of force by police on people experiencing mental illness internationally (Fyfe, 2000). Indeed, issues around police training, policy and practice in Victoria have come under particular scrutiny over the last 20 or so years, following a number of reviews into the number of police shootings in the State and the over-representation of mental illness among the victims of these shootings (Dalton, 1998; Kesic et al., 2010). While training initiatives embarked upon have, at least temporarily, reinvigorated the focus on mental health awareness, and more recently moved away from classroom-based didactic teaching methods to a more realistic reflective and hands-on scenario-based training developed in collaboration with mental health specialists, these encounters account for a relatively unknown burden on police time.
The evidence regarding the frequency and nature of contacts between police and people experiencing mental illness is very limited, often amounting to little more than anecdote and conjecture. A recent small-scale study conducted in New South Wales suggested that approximately 10 per cent of police time was spent dealing with people experiencing mental illness (Fry et al., 2002), while a similar study conducted in New Zealand reported a comparable figure of 8.6 per cent (Dew and Badger, 1999). Apart from these two studies, very little empirical evidence is available. There is clearly a pressing need to gain a detailed understanding of the commonality and circumstances around these encounters. Such empirically derived evidence would provide a much needed starting point to help identify service gaps, inform the potential need for a clearer and more substantial focus in training on these issues, and act as a catalyst for commencing an informed dialogue about the need for broader health and justice reforms by recognizing the potentially significant role played by police at this interface. Against this background, the aims of this study were to explore: (1) the frequency of contact between the police and people experiencing mental illness; (2) the relationship between police officers’ knowledge and the sources of information they use when exercising their discretion; (3) the signs, symptoms and behaviours police officers believe are related to mental illness; and (4) the biggest challenges faced by police officers when dealing with people experiencing mental illness.
Method
Source population and recruitment
All operational police officers in the State of Victoria are required to attend Operational Safety and Tactics Training (OSTT) twice a year. All officers, up to and including the rank of Inspector attending OSTT during the data collection phase (January–June 2008) were eligible to participate. Officers were recruited from nine of the 13 training sites around the State, thereby allowing for a total potential sample of 7914 officers. The research was introduced by the OSTT training facilitator and questionnaire packs were handed out to all potential participants. Once participants had completed the questionnaires they were invited to post them in a sealed opaque box. Participation was voluntary; with potential participants instructed to post surveys, whether completed or left blank if they chose not to participate, in the box at the end of the session. The study received full ethical scrutiny and approval from the Monash Standing Committee on Ethics in Research Involving Humans and the Victoria Police Human Research Ethics Committee.
Questionnaire composition
A multi-component questionnaire was developed by the authors in consultation with senior police personnel and policy makers from Victoria Police. Specific sections sought to document the following: (1) the sources of information used to understand and identify whether someone had a mental illness, scored according to a 6-point Likert scale (1 = ‘not based at all/never’ to 6 = ‘strongly based/very often’); (2) the relative frequency of different outcomes resulting from their interactions with people experiencing mental illness (e.g. arrest, mental health apprehension, no further action or referral to another agency), according to a 6-point Likert scale (1 = ‘never’ to 6 = ‘very often’); (3) up to five, signs, symptoms or behaviours that they believed were useful in determining whether someone had a mental illness; (4) the biggest challenges they faced when attempting to resolve situations involving people experiencing mental illness; and (5) their attitudes toward mental illness using the Mental Health Attitude Survey for Police (MHASP; Clayfield, et al., 2009), again according to a 6-point Likert scale ranging from 1 = ‘strongly disagree’ to 6 = ‘strongly agree’. Minor amendments were made to the original MHASP scale to ensure cultural sensitivity and appropriateness; these werechecked for face validity by the multidisciplinary research team. Finally, social desirability was considered using the short 13-item version of the Marlowe Crowne Social Desirability Scale (Crowne and Marlowe, 1960; Reynolds, 1982).
Data manipulation and approach to analysis
Returned surveys were scanned and participants’ free text responses were recorded verbatim in a database which was later converted for use with SPSS (version 16, 2007). Descriptive statistics were used to explore the frequency of participants’ responses on the questions which utilized a Likert-type scale. A factor analysis was conducted on the responses to ‘sources of information used to determine if someone is mentally ill’ and ‘bases of knowledge regarding mental illnesses’; each being considered a ‘set of variables’. The relationship between these two sets were considered using canonical correlations (Tabachnick and Fidell, 2007: 567–606). Data gathered through free text responses to the open-ended questions were grouped, considered and interpreted using thematic analysis, based on the grounded theory framework described by Strauss and Corbin (Strauss and Corbin, 1998: 12). A random subset of 15 per cent of completed questionnaires were selected for these purposes to gain an in-depth understanding of the how the thoughts and experiences of police officers can be explained by the narratives on common signs, symptoms and behaviours they ascribe to mental illness. The latter sampling method was adopted to allow for a manageable data set and for the emergence of thematic saturation across the diversity of police experiences.
Results
Demographic data
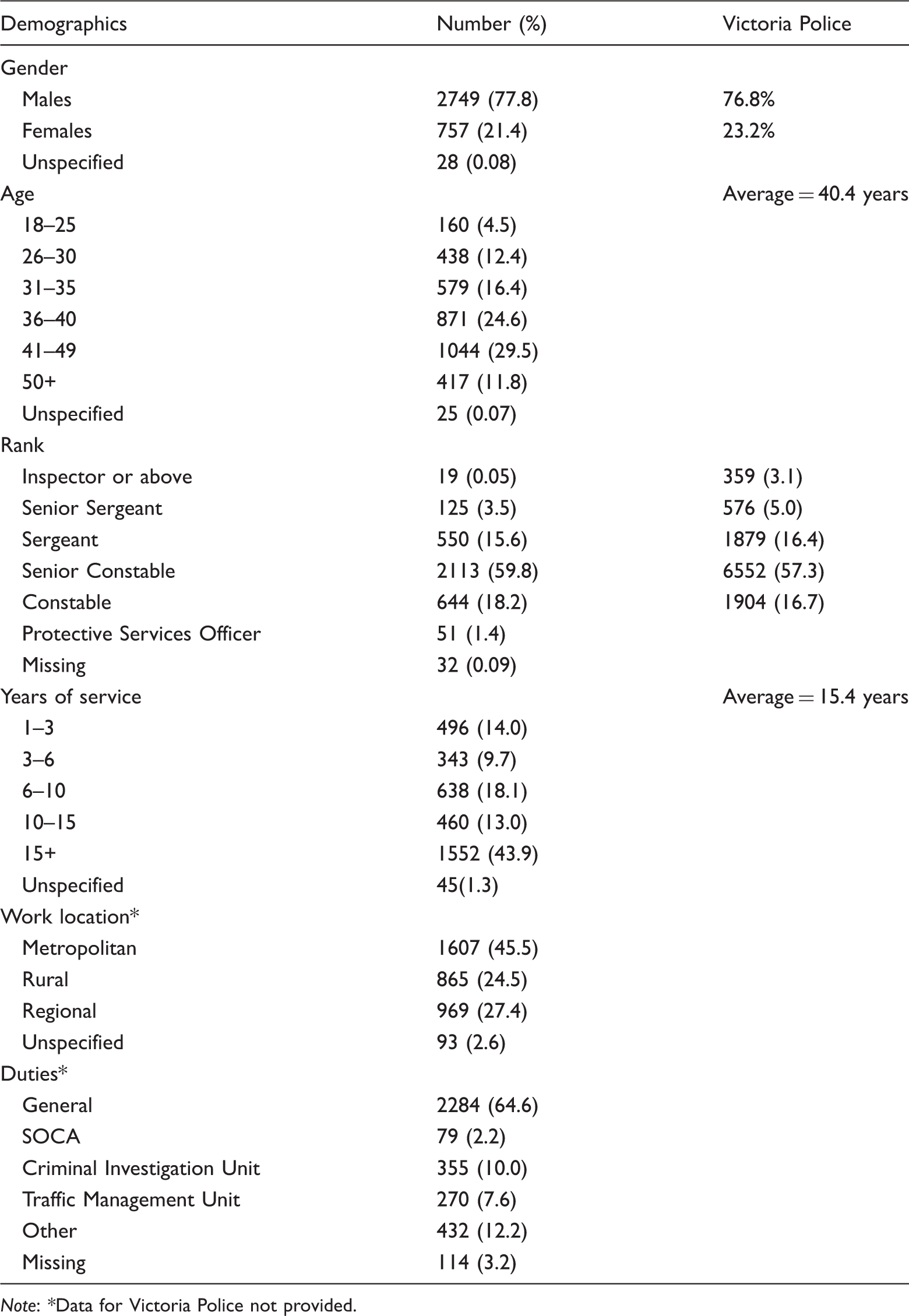
Note: *Data for Victoria Police not provided.
1. Frequency of contacts between the police and mentally ill people
Participants estimated that approximately 20 per cent of people with whom they have contact in any week are mentally ill. This figure did not differ depending on whether the people were offenders, suspects, victims, vulnerable/at risk people, or people in need of assistance. Just under half (48.2%; n = 1,705) reported that they had contact with someone who appeared to be mentally ill 1–2 times per week, 26.1 per cent (n = 923) reported 3–5 times, 10.1 per cent (n = 356) reported ‘never’, 9.2 per cent (n = 324) reported 6–10 times, 3.5 per cent (n = 125) reported ‘10 or more times’ a week.
2. Police identification of mental illness
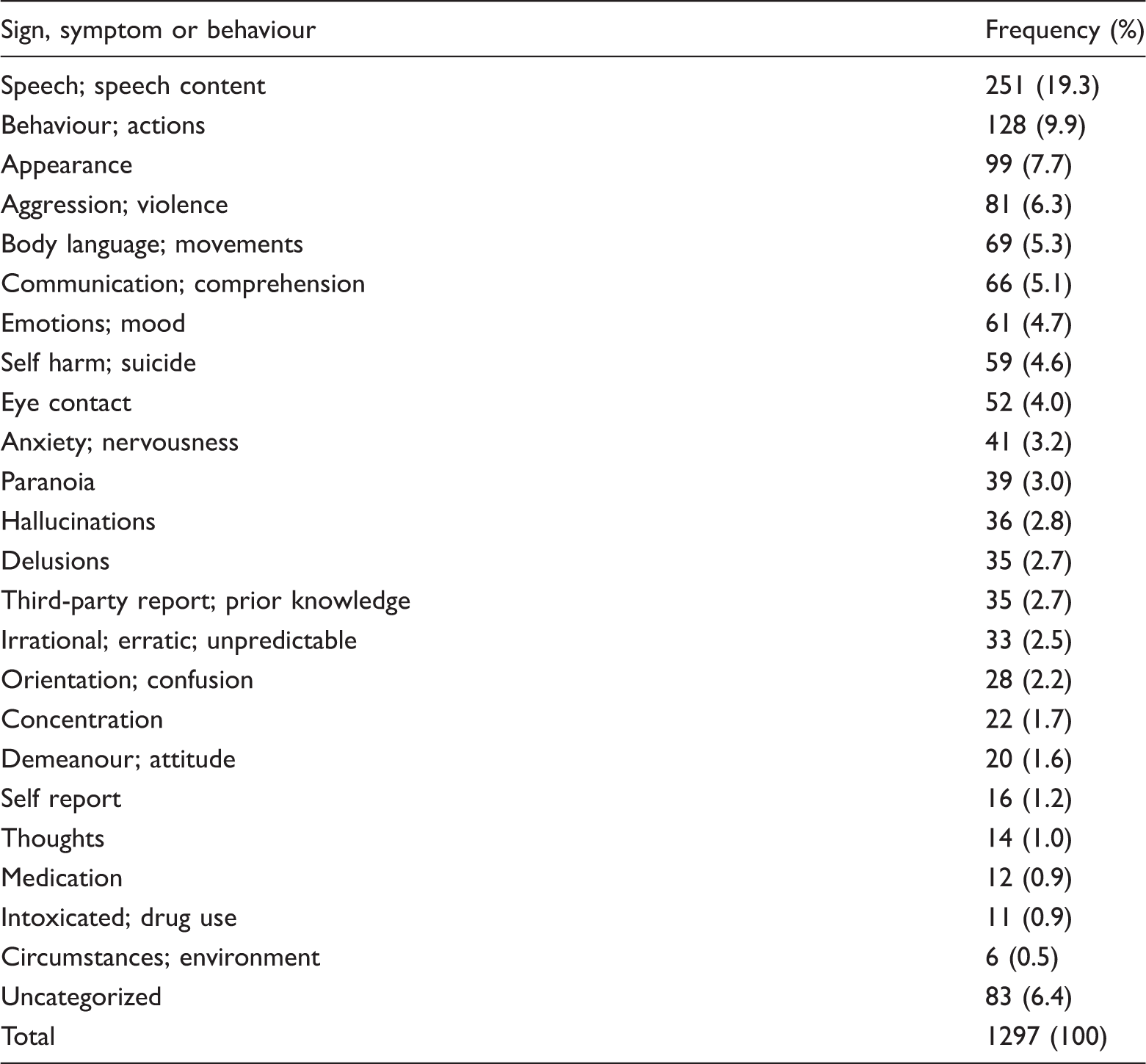
Signs, symptoms and behaviours police officers associated with mental illness
According to participants’ responses on a Likert-type scale, the category of ‘sources of information used to determine if someone is mentally ill’ used most often was ‘person-based information’ (M = 4.90, SD = 1.02), followed by ‘police sources’ (M = 4.65, SD = 1.23) and ‘medical practitioners’ (M = 3.79, SD = 1.53). None of these variables were related to the measure of social desirability. It should be noted that some of these themes represent aggregate items, as their relationships were revealed following a factor analysis. For example, the items ‘previous knowledge of the individual’, ‘behaviour observed at the scene’, and ‘other’ were combined to form the aggregate item ‘person-based information’. Similarly, the items ‘information provided on dispatch’, and ‘information from police database’ were combined to form ‘police sources’.
According to participants’ responses on another Likert-type scale, participants’ ‘bases of knowledge regarding mental illness’ were most likely drawn from ‘on-the-job experience’ (M = 4.46, SD = 1.21), followed by ‘personal experience’ (M = 4.22, SD = 2.00) and ‘Victoria Police training and education’ (M = 3.57, SD = 1.30). It should be noted that ‘personal experience’ was made a composite factor based on items including ‘interactions in private life’ and ‘personal experience’, after a factor analysis revealed these items were related.
3. Outcomes following police encounters with mentally ill people
In response to the item ‘how frequently do you use the following outcomes following your encounters with mentally ill people’ the item with the highest rating was ‘mental health apprehension’ (M = 4.31, SD = 1.40), followed by ‘arrest’ (M = 3.71, SD = 1.31), ‘no further action’ (M = 3.23, SD = 1.20) and ‘referral to another agency’ (M = 3.17, SD = 1.31).
A canonical correlation was conducted using the outcome variables ‘mental health
apprehension’ (Section 10 of the Mental Health Act 1986 (Vic)), ‘arrest’, ‘no
further action’ and ‘referral to another agency’ as the dependent variables and
the sources of knowledge, including (i) on-the-job, and (ii) personal
experience, and sources of information, including (a) ‘police sources’, (b)
‘person-based information’, and (c) ‘medical practitioner’, as covariates. The
first canonical correlation attained significance, Wilk’s Λ = .64
F(24, 10826.28) = 62.44, p < .001.
Canonical loadings pertaining to the dependents and covariates are shown in
Figure 1 and
interpreted in Text box 1. Standardized canonical coefficients
for the dependents (outcomes) and covariates
(predictors).
Mental-health apprehension: The
likelihood of a mental health apprehension increases as
information is garnered from police sources and the
person; Help-centred outcome: The likelihood
of referring to another agency increases as knowledge is
derived from personal experience and information is gathered
from medical practitioners, but decreases as information is
garnered from the police; Subjective-client centred approach:
The likelihood of taking no further action increases as a
police officer’s knowledge is derived from personal
experience and information is garnered from the person
rather than medical practitioners. Criminal apprehension: The likelihood
of arrest increases as knowledge is derived from
‘on-the-job’ and personal experience and information is
garnered from police sources rather than the
person.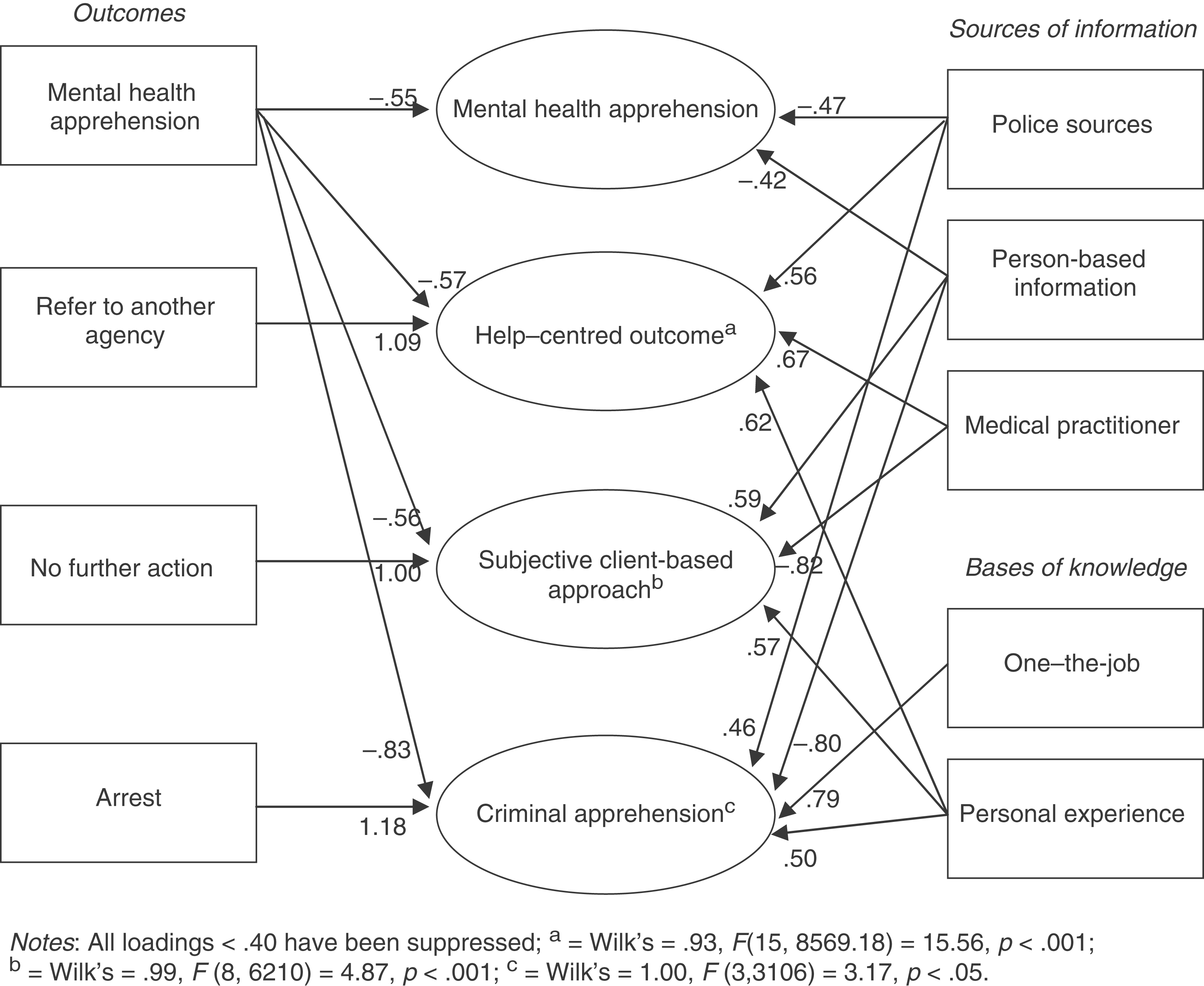
Box
1. Interpretation of approach style
components
Notably, the ‘help-centred outcome’, ‘subjective client-centred approach’ and ‘criminal apprehension’ canonical variates were all negatively related to the decision to make an apprehension under the Mental Health Act 1986 (Vic).
4. Biggest challenges
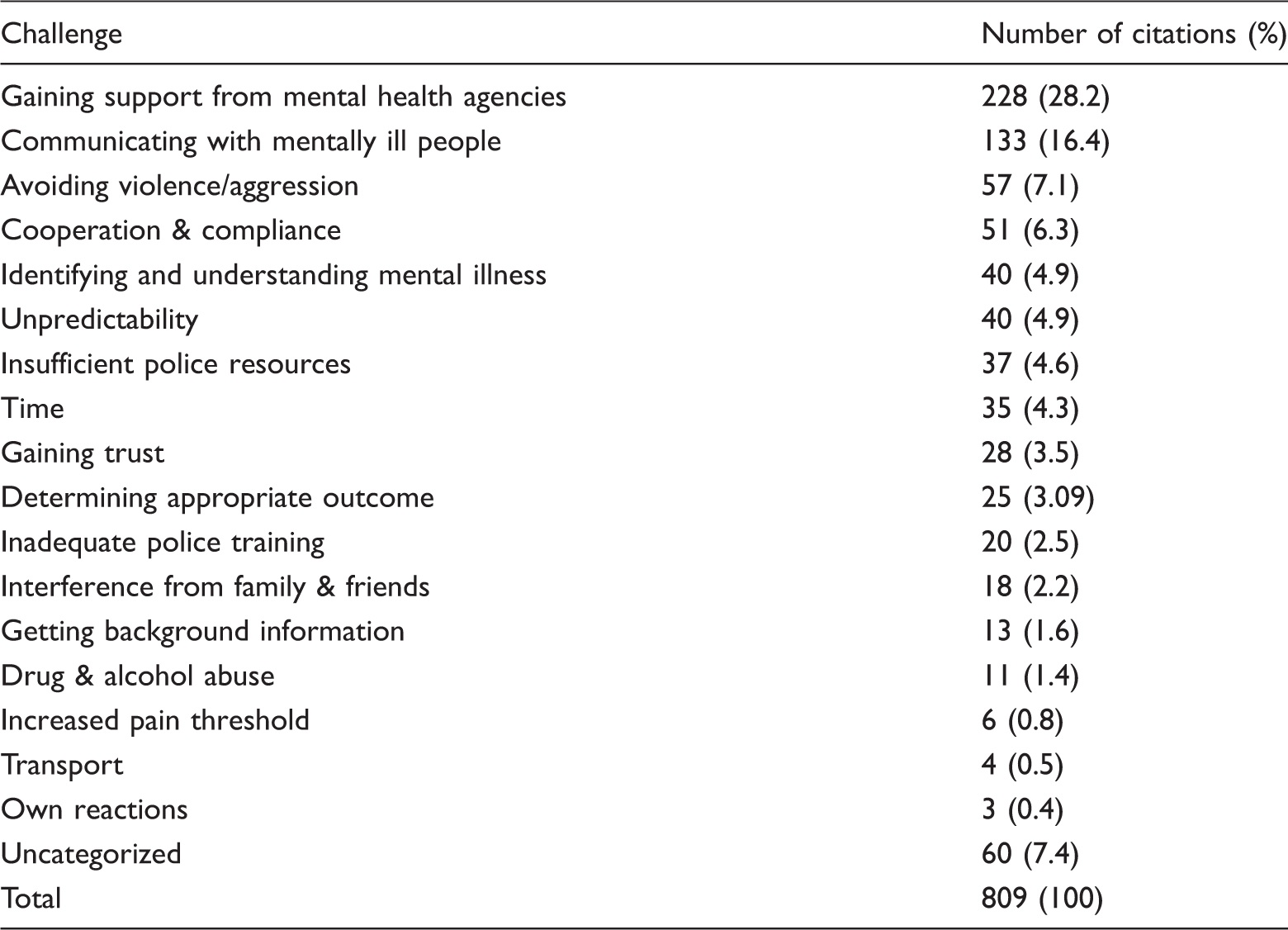
Challenges faced by police when dealing with mentally ill people
Discussion
The aim of this study was to examine the estimated frequency of contact between police officers and people experiencing a mental illness, the process by which officers evaluate whether someone is mentally ill, the bases of officers’ knowledge and sources of information used when dealing with people who have a mental illness and the challenges faced by officers when performing these duties.
1. Frequency of contacts
Surveyed police officers reported coming into contact with people experiencing mental illness on a regular basis; with almost half coming into contact with at least one to two people who have a mental illness each week, and over one-third of respondents reported coming into contact with between three and 10 mentally ill people each week. This suggests that a significant amount of police time is taken up dealing with people experiencing mental illness; a finding that is consistent with previous research (Fry et al., 2002). For decades now, the factors which have been associated with increasing contacts between the police and people who have a mental illness have been debated. These include deinstitutionalization and restrictive commitment criteria, which have been said to culminate in the ‘criminalization of the mentally ill’ (Abramson, 1972). More recently, however, relatively high levels of violence (Wallace et al., 2004) and substance abuse (Junginger et al., 2006) among people experiencing mental illness have been claimed to account for these encounters. Further research should establish whether these specific types of suspect/offender encounters are increasing and if and how these encounters are resolved.
Of particular note, though, these results further suggest that the social welfare role is now indeed commonplace in contemporary community policing (e.g. Stenning and Shearing, 2005), with police indicating that roughly equal proportions of their contacts with people experiencing mental illness were as suspects, victims, persons in need of assistance and vulnerable persons. It becomes increasingly important, therefore, to start to acknowledge the significant role police are playing supporting vulnerable members of the community; a role above and beyond traditionally defined and envisaged policing functions (e.g. Foster, 2005). More objective and descriptive accounts of the frequency and nature of these broader policing functions has a real potential to meaningfully contribute to a dialogue concerning the need for closer working partnerships between police and health service providers. This is an area under current study by some of the authors.
2. Police identification of mental illness
Police officers reported a wide range of signs, symptoms and behaviours that they believed to be associated with mental illness. Four out of the top five signs cited by officers – ‘speech/speech content’, ‘behaviour’, ‘appearance/hygiene’ and ‘body language’ – might be used by a mental health professional for the purposes of a mental status examination; all of these signs are readily observable and can provide valuable insight into a person’s mental functioning. Of some importance was the identification of ‘aggression/violence’ as being indicative of mental illness. Several officers reported an ‘increased pain threshold’ or ‘high pain tolerance’ as being a sign of mental illness. Extant evidence suggests that such beliefs are associated with more negative assumptions about dangerousness (i.e. increased dangerousness) and thus contribute to differential engagement, containment and resolution strategies (Finn and Stalans, 1997; Watson et al., 2004). Even if police can identify common signs and symptoms of mental illness, the more pressing concern when engaged in an encounter with a person in emotional distress does not relate to the identification of such indicators, but how to approach, engage and reassure the distressed person most effectively. The latter arguably represents a much more pressing training need for police officers in relation to mental health awareness.
An examination of the sources of information used by officers to determine whether someone is mentally ill revealed that person-based sources and police information were used more frequently than reliance on medical practitioners. Possibly, this reflects the limited availability of medical practitioners to provide such advice. Consistent with previous research (Fry et al., 2002) police officers felt unsupported by mental health agencies. However, previous Australian research reported that 98 per cent of police officers had no knowledge regarding the availability of a 24-hour crisis service available to assist them with interventions involving people experiencing mental illness (Wylie, 1990). This suggests a significant information gap and points to the need for improved and enhanced information sharing and collaborations between service providers.
This study also indicated that officers were more likely to base their understanding of mental illness on their on-the-job training and personal experience, rather than information gained from more formalized courses provided by Victoria Police or other external agencies. This model of learning is consistent with the apprenticeship-type model adopted in community policing, whereby junior officers are paired with more senior, experienced officers. To maximize the impact of training, it is most important that training is delivered in a style consistent with officers learning preferences. While police may not be so enthusiastic about certain elements of training, such as role plays (Vermette et al., 2005), a multi-modal learning programme is in fact consistent with specialized training in other core elements of policing (Price, 2005). Given the frequency of contact with people experiencing mental illness and the challenges that arise, there is an ongoing need for formalized policies and training for police regarding mental illness with proper systematic evaluation. To overcome potential concerns about police providing all of the training due to the need to overcome underlying aspects of organizational culture, the more proactive involvement of mental health professionals in devising and/or delivering training content should be emphasized (Hails and Borum, 2003). This modality of expert-developed scenario-based training, where police have the opportunity to rehearse their skills, is now being rolled out by Victoria Police and will be the subject of ongoing evaluation and review.
3. Outcomes following police encounters with mentally ill people
Figure 1 reveals the nature of the relationship between: (1) the bases of officers’ knowledge and sources of information used to determine whether someone is mentally ill; and (2) the four outcomes they might engage in following their encounters with people experiencing mental illness. According to the results, the likelihood of engaging in a mental health apprehension increased as information was gathered from the police and the person. Indeed, the Mental Health Act 1986 (Vic) allows officers to apprehend someone if they ‘appear to be mentally ill’. As indicated in the Act, officers are not required to exercise ‘clinical judgement’. This research suggests that the addition of pre-recorded information from police sources regarding an individual may influence or otherwise reinforce an officer’s ‘layperson’ assessment that a mental health apprehension is the most appropriate course of action.
The results indicated that the likelihood of referring an individual to another agency increased as knowledge was derived from personal experience and information gathered from medical practitioners, but decreased as information was garnered from police sources. This suggests that a reliance on personal experience is more strongly associated with ‘help-centred outcomes’ than more restrictive options for dealing with people experiencing mental illness. The finding that referrals to other agencies are associated with advice from medical practitioners is not surprising, as advice from a medical practitioner represents a referral to another agency in itself. The finding that this outcome is associated with decreasing information from Victoria Police sources might be associated with the absence of police information regarding the person, and thus the need to seek third-party advice.
It was also revealed that the likelihood of taking no further action increased as a police officer’s knowledge was derived from personal experience and information garnered from the person rather than medical practitioners. This is consistent with previous research that years of police officer experience has a positive effect on the likelihood that police take no further action (Green, 1997). Figure 1 also indicates that the ‘no further action’ outcome was positively related to information garnered from the person and negatively related to information from medical practitioners. Perhaps individuals who adopt this ‘subjective client-based approach’ feel confident in their own decision making. On the other hand, it might be that officers viewed both ‘arrest’ and ‘hospitalization’ as unfavourable outcomes due to concern the person would not get care and/or the time involved. Thus, taking no further action might have been considered the ‘least bad’ option.
The likelihood of arrest increased as knowledge was derived from ‘on-the-job’ and personal experience, and information was garnered from police sources rather than the person. The use of ‘arrest’ for dealing with mentally ill people has been cited as a ‘last resort’ option for handling mentally ill people (Teplin and Pruett, 1992). If this were the case, however, officers who chose this option would be likely to rely on information garnered from the person and, in particular, their observations of the individual. These results suggest that police-based information was associated with the decision to arrest; that is, existing information regarding a person’s previous misdemeanours might increase the likelihood of a ‘criminal apprehension’, irrespective of an individual’s apparent mental health needs and presentation.
Notably, previous research has established that the outcomes of police officer encounters with people who have a mental illness are strongly dependent on situational variables: for example, the presence or absence of a complainant (Patch and Arrigo, 1999); the systems available to the police for dealing with people in crisis (Borum, 2000); and the offence type (Green, 1997), among others. Nevertheless, these data suggest that the relative frequency of each outcome was also related to the bases of police officers’ knowledge and the relative weight placed on sources of information regarding the people with whom they have contact.
Challenges
The dominant theme arising from the challenges listed by participants was ‘gaining support’. This included support from different mental health agencies including hospitals and emergency psychiatric teams. One participant noted ‘hospitals haven't got the resources to assess mentally ill patients… therefore takes up valuable police time to find alternative answers’. Several officers also expressed frustration at having to ‘baby-sit mentally ill people’ in hospital waiting rooms, while others found the mental health system to have a ‘revolving door policy’, indicating that, often times, people are released from mental health services only to come back to the attention of police officers. Other themes included ‘communicating with the mentally ill’ and ‘identifying and understanding mental illness’. For example, one officer reported difficulty in ‘being able to communicate with someone who is not rational’. Another participant reported problems with ‘knowing different types of mental illness [and] what approach to take’. Other frequent themes included ‘avoiding violence/aggression’ and ‘cooperation and compliance’. Within these themes were concerns regarding keeping individuals calm, avoiding harm to both people experiencing mental illness and police officers and getting people to comply with instructions. For example, one participant listed the challenge ‘gaining trust from [the] mentally ill person to enable you to ultimately get them to medical facility without physical confrontation’.
These challenges highlight broad areas which can be considered for improvement in the interface between the police and people experiencing mental illness. First, and perhaps most importantly, police organizations might benefit from more formal partnerships with mental health services; police officers need to be able to refer mentally ill people to mental health agencies without consuming an unreasonable level of police resources (Borum, 2000). Although officers are not required to diagnose individuals with mental illness, officers would benefit from knowing how specific mental illnesses, such as psychotic disorders, might affect a person’s thinking and behaviour. Such training could be coupled with strategies for improving communication and compliance when dealing with mentally ill people, especially those who present in an irrational state. Added to this, a common issue that arose from participants’ responses was the lexicon used for describing mentally ill people. In the instance that officers were equipped with an appropriate discourse for dealing with mentally ill people, one benefit might be improved communication between police officers and mental health professionals.
Several limitations should be noted when interpreting these research findings. Although the response rate among the 3,811 police officers who were invited to participate was 92.7 per cent, the actual number of police officers who attended OSTT during the data collection phase was 7,914; however, surveys were only given to 44.6 per cent of the available population by the OSTT facilitators at the time of sampling. Nevertheless, our response rate was substantially higher than recent research of a similar nature (e.g. Cooper et al., 2004). Due to the size and scope of the research undertaken, a cross-sectional methodology was adopted; however, this brings with it some limitations, particularly concerning interpretations of causality and directionality of relationships between variables. The research also relied on self-report by consenting police, thus increasing the anonymity of respondents, but leaving an opportunity for increased risk of socially desirable responses; the latter was essentially controlled for by considering and measuring social desirability alongside other police responses. Complementary methodologies, combining the scaled responses with more focused follow-up discursive questions delivered via a face-to-face method may have helped uncover some of the stark differences and more subtle nuances between individual decision-making processes. Research of this nature is currently underway, the details of which are available from the authors.
To most recruits, joining the police force is about dealing with those people who break the law and their victims. While this remains the essence of what is popularly considered ‘real police work’, it is increasingly only filling a small portion of their role (Foster, 2005: 200). One of the key challenges therefore is for police to consider the significant social welfare dimension of community policing an integral and important core component of their role. Despite the reported enthusiasm by large numbers of police to undertake training about mental illness, there potentially remains a real challenge in translating this new-found knowledge into practice when there is an underlying culture that measures and rewards ‘real police work’, but does little to formally recognize the broader supportive roles the police perform on a daily basis. This kind of cultural shift is an endeavour that cannot occur in isolation in any one agency; instead such an initiative will require a whole of system response. Only with a concerted, focused and sustained programme of interagency collaboration will the police become better equipped for resolving encounters at this interface and recognized for their pivotal role in this vital community service.