
Abstract

Recent violent tragedies in schools, universities, and in public spaces have focused increased attention on the symptoms and consequences of maladaptive traumatic stress and posttraumatic stress disorder (PTSD) in children and adolescents. Child maltreatment and its consequences continue to be prevalent in the United States. Recent changes to diagnosis in the Diagnostic and Statistical Manual, 5th edition (DSM-5) identify new criteria for PTSD in young children as well as in school-age children and adolescents. There is a growing body of knowledge about what psychological treatments are effective in children. Pediatricians are often the first to identify and treat traumatized children. 1 An update on this topic is relevant because data show that only 18% of primary care pediatricians’ self-report adequate knowledge of childhood PTSDs, and only 10% report frequent experience in the assessment and treatment of posttraumatic stress symptoms. 2
Epidemiology and Prevalence
Exposure to traumatic stress events including physical abuse, sexual abuse, violence, witnessing violence in the home or community, severe family dysfunction/psychopathology, natural disasters, severe accidents, and/or their own or their caregivers’ life-threatening illness is not uncommon in children and adolescents. Estimates from epidemiological studies range from 25% of youths experiencing at least 1 traumatic event by age 16 years 3 to more than 60% by ages 16 to 18 years in the United States and internationally.4,5 The Centers for Disease Control and Prevention reports that in 2010 more than 740 000 children and youths were treated in hospital emergency departments as a result of violence and that more than 3 million reports of child maltreatment are received each year by state and local agencies. 6
Toxic stress in childhood may result from intense, frequent, or prolonged activation of the body’s neurobiological stress systems in the absence of the buffering protection afforded by a supportive adult caregiving relationship and may result in physiologic, behavioral, and emotional stress-related vulnerabilities to a wide variety of physical and mental illnesses throughout the lifespan. 7 Risk factors for the development of clinically significant problems include exposure to multiple types of trauma (cumulative traumatization or polyvictimization) 8 in the context of a compromised family or extrafamilial social support system (eg, chronic poverty, parental mental illness or substance abuse, interpersonal isolation or affiliation with delinquent peers, multiple out-of-home placements), when children 3 or adolescents 4 experience psychological trauma(s). As the cumulative burden of childhood adversity increases, the likelihood of developing emotional and behavioral problems that persist into adulthood increases in a dose-response manner, including vulnerability to serious medical as well as mental health disorders. 9
Most children experience transient psychological distress following exposure to traumatic events, which may manifest in the form of distinct changes in behavior (eg, regression, irritability) and physical complaints in young children10,11 or peritraumatic (ie, in the immediate wake of trauma exposure) states of distress, heightened arousal, or dissociation. 12
Children with exposure to traumatic stressors may develop the syndrome of PTSD linked to a traumatic event and characterized by intrusive, avoidant, emotional numbing, and hyperarousal symptoms accompanied by pervasive negative changes in mood, cognition, and self-concept. 13 Associated symptoms may include depression, anxiety, impulsivity, aggression, hyperactivity, agitation, irritability, behavior problems, sleep difficulties, and attentional deficits that further impair daily functioning.14,15 The reported overall lifetime prevalence of PTSD in the general youth population is 3% to 9%16,17 and varies by gender with approximately 4% of male adolescents and 7% of female adolescents meeting full diagnostic criteria for PTSD.4,18 The 1-month posttrauma incidence of PTSD is 15.9%. 19 Least at risk appear to be boys exposed to noninterpersonal trauma (PTSD 1-month incidence of 8.4%). Most at risk for PTSD are girls exposed to interpersonal trauma (32.9%). 19
It is important to note that a subgroup of youngsters develop persistent symptoms of traumatic stress that often extend beyond PTSD and may be quite varied, including anxiety/fears, anhedonic/dysphoric, angry/aggressive, and/or dissociative symptoms as well as problems with sleep, eating, concentration, substance use, sexuality (primarily following sexual trauma or interpersonal violence), reckless or avoidant behavior, self-harm, or suicidality. 20 In clinical pediatric samples, symptoms of traumatic stress have been found in approximately 90% of sexually abused children, 75% of children exposed to school violence, 50% of children who are physically abused, and in 35% of children exposed to community violence. 21 It is estimated that between 60% and 90% of children presenting for outpatient mental health treatment may have been exposed to at least 1 traumatic stressor. 21
Trajectories of Posttraumatic Adaptation: Risk and Protective Factors
Outcomes for children after exposure to traumatic stress vary widely and often change over time. Trajectories of poor outcomes include severe initial reactions followed by persistent or episodic posttraumatic impairment (chronic PTSD) and mild to moderate initial reactions followed by severe impairment (delayed PTSD). 22 Delayed PTSD was considered rare until recent findings from prospective studies showed that as many as 2 in 10 youth, as well as adults, do not manifest clinically significant PTSD symptoms for several months or even years following initial exposure to traumatic stressors. 23
Risk factors for chronic pediatric PTSD include pretraumatic psychiatric disorder, impaired caregivers/family, poverty, low IQ, avoidant/anxious coping, and generalized arousal and negative affect, exposure to interpersonal traumatic stressors (eg, maltreatment, sexual assault, domestic violence) or cumulative (multiple type/polyvictimization or recurrent) traumatic stressors, peritraumatic distress (fear, perceived life threat, dissociation, acute PTSD), and posttraumatic low social support, social withdrawal, comorbid psychological problems, poor family functioning, and cognitive alterations (rumination, distraction, thought suppression, and attention bias toward threat).4,11,20,24
On the other hand, many children are resilient and either are relatively asymptomatic following exposure to the adverse effects of trauma and able to adapt and preserve both functioning and development (resilient) or have moderate to severe initial reactions or early-onset PTSD (ie, within 3 months of exposure) but improve and regain normative functioning over time with or without treatment (recovery). 22 Resilience in the face of exposure to traumatic or other stressors and a capacity for posttraumatic growth is facilitated by protective factors such as individual self-control and problem-solving skills, and relational and environmental factors such as good schools, safe neighborhoods, positive relationships with supportive caregivers, socioeconomic advantage, religious faith, success at school and with peer friendships, and older age at time of traumatic exposure.17,25 Lower traumatic event frequency, number, and intensity of exposure also are important in determining resilient childhood posttraumatic outcomes. Individual capacity for adaptive resilience in the face of traumatic threat largely depends on human adaptive systems embedding the exposed child in a supportive caregiving web involving caregivers, families, friends, communities, and cultures.26,27
Diagnostic Criteria for PTSD
In the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5), PTSD is no longer considered an anxiety disorder, but instead is included in a new chapter on trauma- and stressor-related disorders. PTSD is a psychiatric disorder in which exposure to a traumatic or stressful event is explicitly required as part of the diagnosis and characteristic symptoms follow exposure to one or more traumatic events. For children aged 7 years and older, diagnostic criteria include 4 clusters of symptoms that emerge or are exacerbated following exposure to actual or threatened death, serious injury, or sexual violence through direct experience, witnessing an event, learning of a traumatic event occurring to a close family member or friend, or exposure to aversive details of a traumatic event (see Table 1). These symptoms must occur for duration of greater than 1 month and be associated with clinical distress and impairment in functioning.
Posttraumatic Stress Disorder (PTSD) Diagnostic Criteria. a
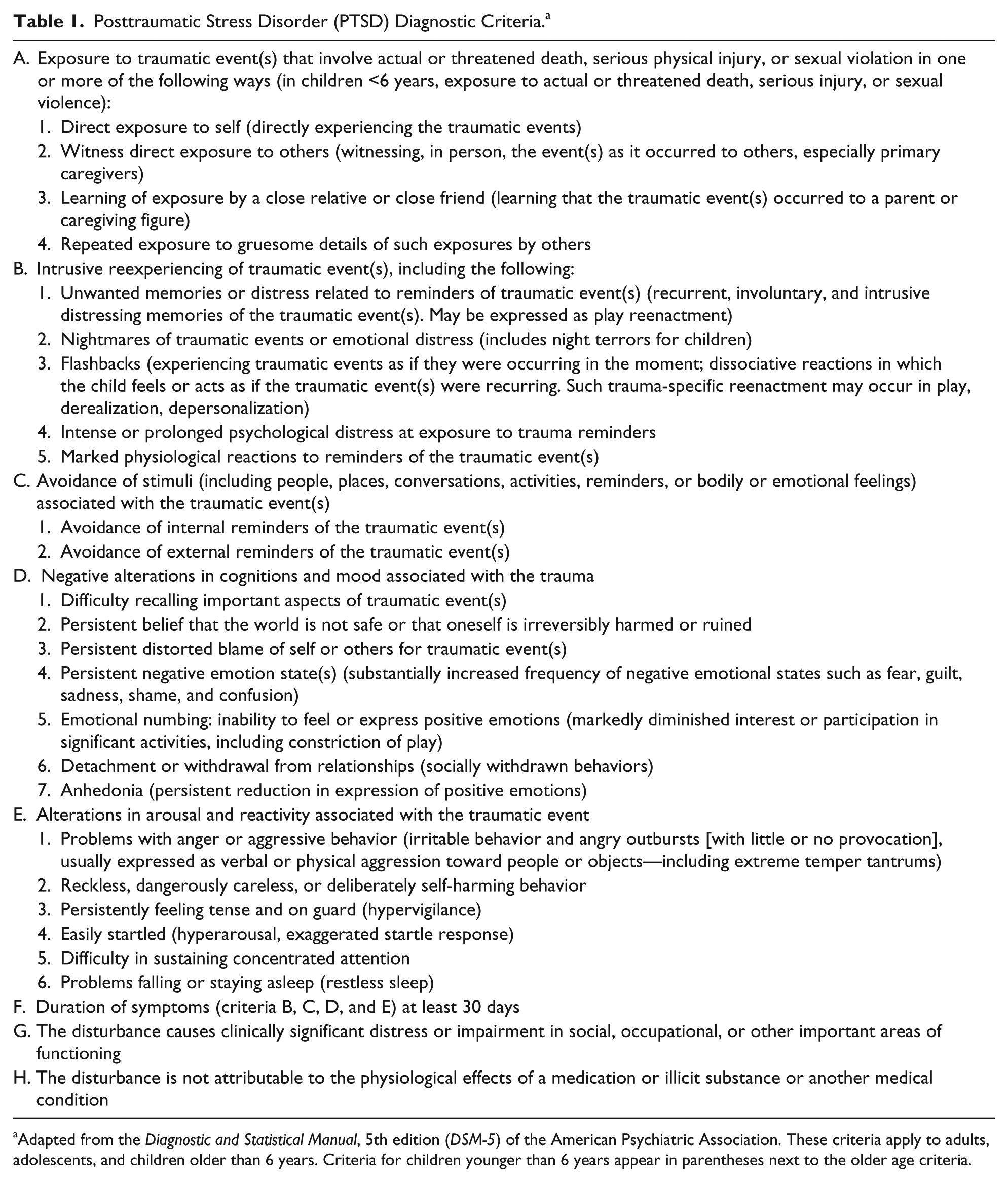
Adapted from the Diagnostic and Statistical Manual, 5th edition (DSM-5) of the American Psychiatric Association. These criteria apply to adults, adolescents, and children older than 6 years. Criteria for children younger than 6 years appear in parentheses next to the older age criteria.
For young children, there now exist explicit PTSD criteria, which include developmentally specific manifestations of symptoms. Acute stress disorder is diagnosed when traumatic stress or dissociative symptoms begin within 3 days of trauma exposure and resolve within 1 month. 13
Evaluation of PTSD in Children
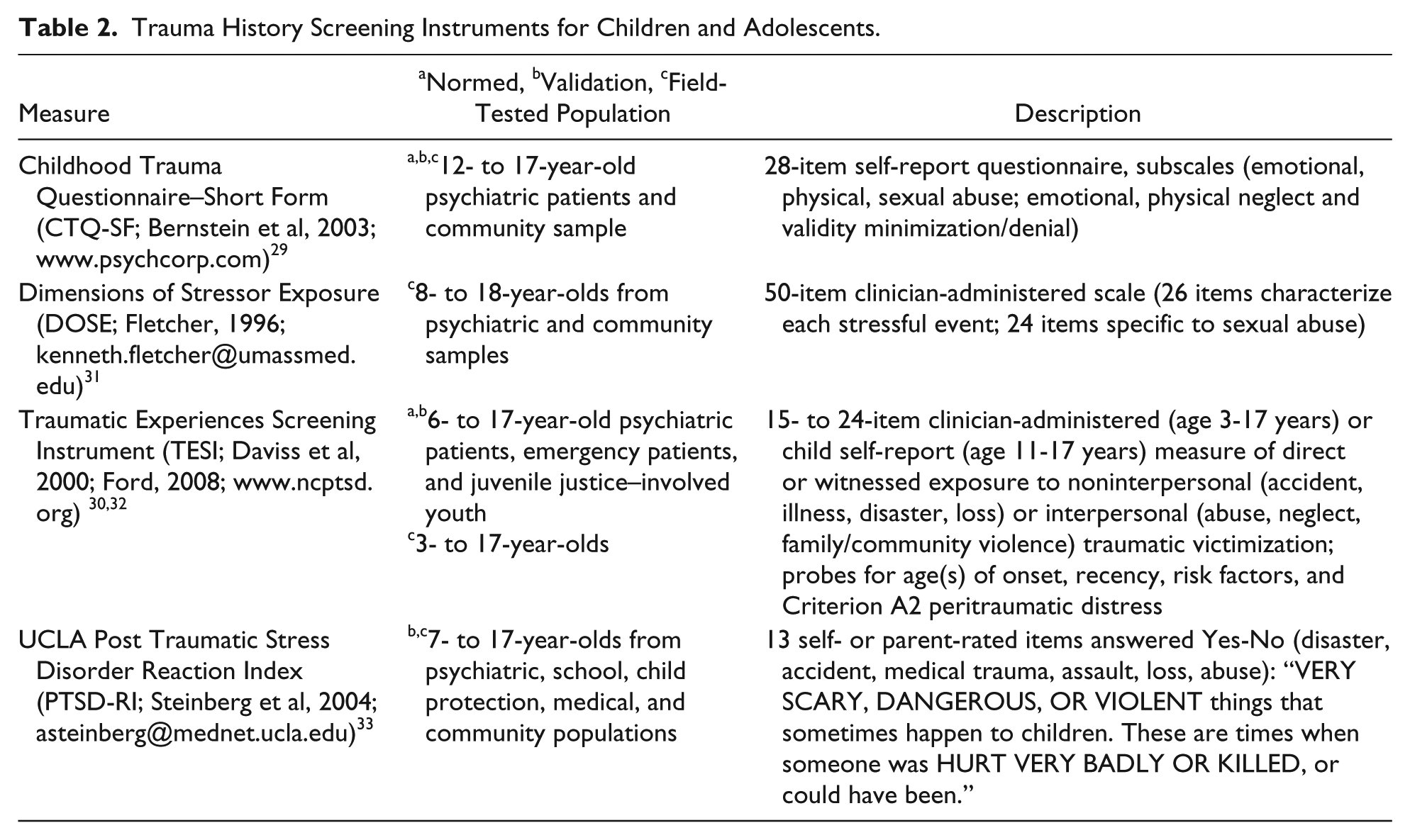
Pediatric providers cannot practically assess every type, let alone incident, of the potentially traumatic events that their patients may have experienced. However, careful listening and selective probing for details of recent or distal events that may have been traumatic is an efficient way to conduct ongoing surveillance when reviewing records or getting the history or progress updates from parents/caregivers and children. 28 It is helpful to refer to carefully constructed and thorough trauma-screening instruments (see Table 2 for examples) as a guiding framework for selective inquiry rather than as formal screening interview.29-33 It is important to consider traumatic events that happen to others as well as directly to the child, especially those affecting the child’s parents or caregivers, which the child witnessed or learned about (eg, domestic violence, severe injuries, or illnesses).
Trauma History Screening Instruments for Children and Adolescents.
A complementary approach to pediatric surveillance of children’s trauma history is careful observation and eliciting caregiver reports of children’s symptoms consistent with PTSD. Children and caregivers may be unaware of or reluctant to disclose potentially traumatic events. Parents may not know what has happened to their child, but they can identify abrupt changes or persistent deterioration in their child’s behavior and functioning. With both young children and with older children and adolescents, such changes or deterioration in behavior or emotion are not exclusively the result of traumatic events but have been found to be associated with traumatic exposure.10,11 In addition, most children who experience potentially traumatic events do not develop lasting debilitating posttraumatic stress problems, 34 whereas other children develop PTSD despite their caregivers not being aware of any traumatic exposures. 35 Therefore, pediatric providers should be knowledgeable of brief systematic PTSD screening measures (see Table 3) in order to be able to detect symptoms or functional impairment that may be indicators of PTSD.28,30,33,36-40 Both parent/caregiver and child self-report versions of brief PTSD screening instruments have been validated and can be administered as a part of routine screening—or used by the pediatric provider as a framework and guide for conducting surveillance during history taking and at subsequent visits or checkups.
Validated Screening Measures for Child/Adolescent PTSD Symptoms (Ford et al, 2013). 28
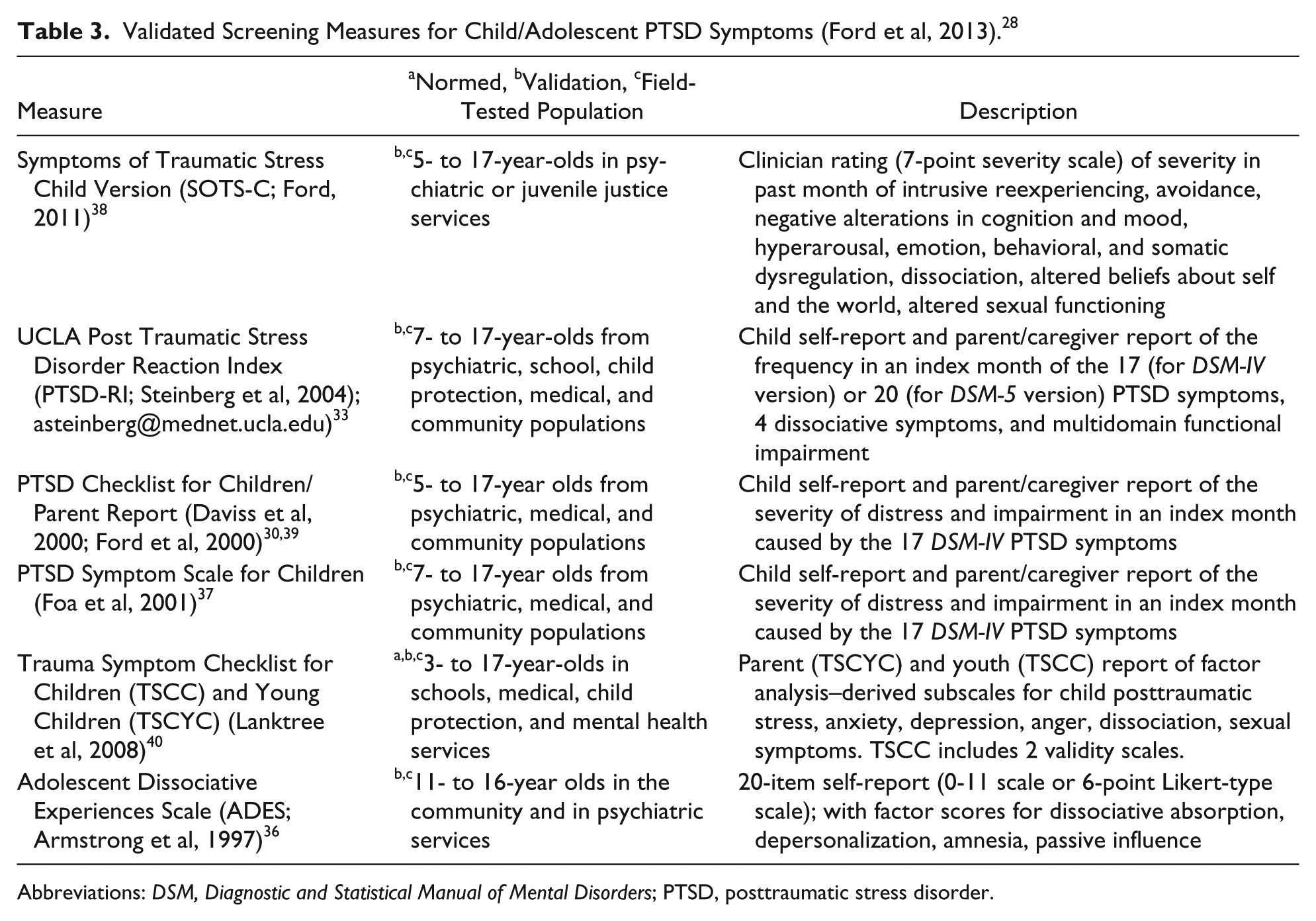
Abbreviations: DSM, Diagnostic and Statistical Manual of Mental Disorders; PTSD, posttraumatic stress disorder.
Treatment
Psychosocial Therapies
Although childhood PTSD is highly impairing and has heterogeneous affective, anxiety, behavioral, somatic, and relational symptoms, it is a highly treatable condition. Over the past 20 years several empirically supported psychotherapies have been developed for both acute and chronic pediatric PTSD (see Table 4).1,41-52,56
Trauma-Focused Therapies. a
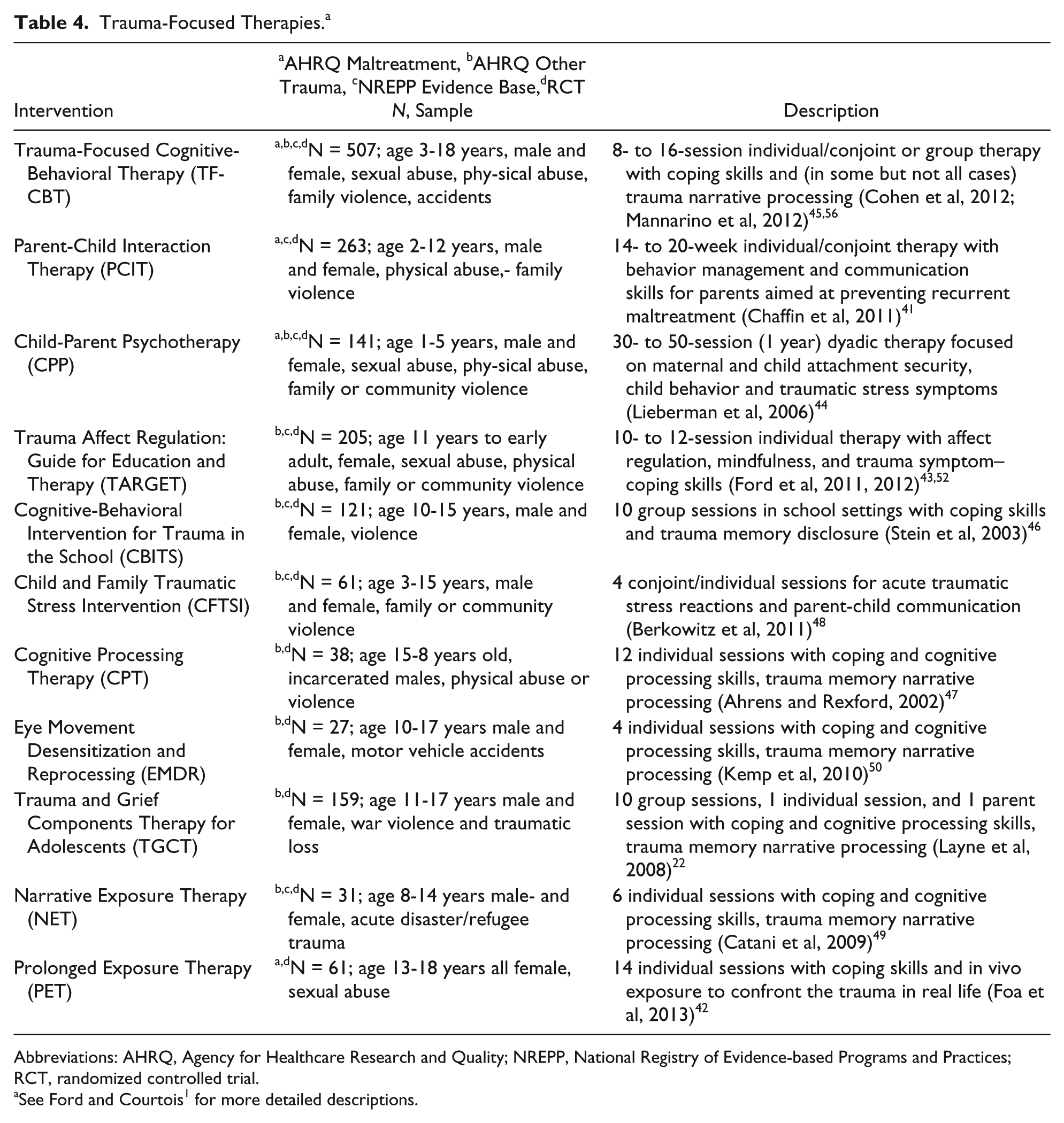
Abbreviations: AHRQ, Agency for Healthcare Research and Quality; NREPP, National Registry of Evidence-based Programs and Practices; RCT, randomized controlled trial.
See Ford and Courtois 1 for more detailed descriptions.
Child traumatic stress treatment research is investigating specific therapeutic mechanisms that appear effective in trauma therapy with children and adolescents.21,53 Common treatment elements include (1) psychoeducation about PTSD, (2) relaxation and coping skills, (3) affect monitoring and emotion regulation skills, (4) cognitive processing of reactions to trauma, (5) helping the child construct a therapeutic trauma narrative, (6) in vivo exposure to trauma reminders and practicing of coping skills, (7) conjoint parent-child sessions, and (8) monitoring and enhancing individual safety. 53
Evidence-based psychotherapy interventions for youngsters with PTSD and/or trauma exposure psychological symptoms have been developed for individual, group, and parent-child formats and delivered in therapist’s offices, schools, and in the home or community. 54 When children (or their parents) are reluctant or unwilling to talk about specific trauma memories, there are evidence-based therapeutic options for either (a) preparing the child and parents to feel sufficiently safe, confident, and able to modulate distressing emotions so that the child is able to experience the trauma narrative portion of treatment successfully55,56 or (b) to enable the child and parent to develop cognitive-behavioral 57 and self-regulation 52 skills that address PTSD by reducing everyday traumatic stress reactivity and increasing emotion regulation, self-efficacy, and social support. A randomized controlled trial also supports the use of in vivo trauma exposure—carefully orchestrated encounters with cues in the youth’s natural environment that are not traumatic but that are associated with past trauma—when coping skills are first taught to teenagers exposed to sexual abuse. 42
Early identification of children who have experienced traumatic stressors and preventive intervention addressing risk factors for the development of PTSD is recommended but not as yet widely implemented or evidence based,58,59 with the positive exception of cognitive-behavioral interventions for traumatized children following disasters 60 or medical trauma. 61 Collaborative care strategies are indicated for integrated pediatric mental health treatment of traumatized children. 62 When pediatric and mental health providers explicitly share the responsibility for assisting traumatized children and their families to restore safety and recover from trauma-related behavioral and emotional problems, this can ensure the necessary continuity and coordination of care—as illustrated by 2 case vignettes. Note that all case materials are disguised to protect patients’ privacy.
Case Vignette 1
Alex is an 8-year-old boy who attends third grade at his neighborhood elementary school. Six months ago, he was riding his bike on the sidewalk in front of his house when he was hit by a car backing out of a nearby driveway. He suffered a broken arm, several bruised ribs, and severe lacerations. Prior to the accident, Alex was a friendly, outgoing boy who did well in school, had lots of friends, and enjoyed spending time with his younger brother and parents. Although his physical wounds have healed, Alex’s parents have noticed several changes in his behavior since the accident. He climbs into their bed almost every night complaining of nightmares and he refuses to ride his bike or even play outside with the other neighborhood kids. In fact, he mostly seems to keep to himself, declining invitations to play dates and birthday parties. Recently, Alex’s parents suggested that they go on a family bike ride thinking that this would “help him get back out there.” Alex immediately declined. When his parents gently urged him, he began to scream and cry, and locked himself in his room. His teachers have also noticed changes in Alex. They frequently have to repeat instructions to him several times, and even then he rarely finishes his school work. They often observe him staring out the window. At recess, Alex no longer climbs on the playscape or runs around with his friends as he used to, preferring instead to play quietly in the sand box or sit on a bench and read. On several occasions, he has burst into tears over small setbacks or frustration, or yelled at other kids for accidently bumping into him.
Case Vignette 2
Danielle is a 16-year-old girl referred for treatment after her adoptive mother called emergency mobile psychiatric services because Danielle was unable to calm down following an argument. Danielle was removed from her biological mother’s care at the age of 4 because of her mother’s neglect, substance use, and domestic violence between her mother and her boyfriend. She was placed in a series of foster homes, moving frequently between placements because of tantrums and accusations that she was stealing food and hiding it under her bed. At the age of 6, her biological father gained custody of her, but she was removed from his care and placed in a foster home at the age of 9 because he and her stepmother were physically and emotionally abusive toward her. She was adopted by her foster mother when she was 11 years old. Initially, Danielle got along well with her adoptive mother and did well in school, where she was a friendly and hardworking student. However, about 3 years ago, she began to exhibit a number of concerning behaviors. She started smoking cigarettes and marijuana and engaged in self-injurious cutting. She began wearing suggestive clothing and spending more time with a group of older adolescents, including a 16-year-old boy she referred to as her boyfriend. She became easily angered when she was told she could not do something, and she and her adoptive mother began to have increasingly heated arguments, often culminating in Danielle running away. Her adoptive mother reported that she did not feel able to control Danielle or keep her safe. In the past 2 years, Danielle has been involved in several individual outpatient and intensive outpatient therapy programs. She has been taken to the emergency department 3 times for evaluation because of behavioral concerns and has been hospitalized in an inpatient unit once because of an attempted overdose of pills. Her teachers report that she appears angry much of the time and seems to have difficulty paying attention in class. She is frequently defiant toward authority figures, and she has been suspended twice for fighting with other students. She often skips classes and leaves school grounds without permission, and is at risk of failing several of her classes. Danielle frequently has trouble falling asleep and in recent months she has had repeated nightmares of being murdered.
Case Discussion
These 2 cases illustrate different characteristics in the presentation of pediatric PTSD and highlight different evidence-based therapeutic approaches to address the 2 individuals’ different trajectories of posttraumatic adaptation, symptom presentation, developmental stage, number and type of traumas experienced, amount of social support, and level of current impairment.
In case 1, Alex is a typically developing school-aged child, with good attachment relationships, consistent social support, and a stable and safe home environment. He experienced acute PTSD with anxious and depressed symptoms (internalizing symptoms) after a single traumatic accident. After emergency department treatment of his broken bones and lacerations, he was referred for follow-up with his outpatient pediatrician. The role of the pediatrician is to recognize symptoms of traumatic stress in Alex, provide psychoeducation to the family, and recognize the need for and refer Alex to appropriate mental health treatment. The goals of mental health treatment are to address not only Alex’s symptoms of traumatic stress but also associated internalizing symptoms. Trauma-focused cognitive-behavioral therapy (TF-CBT) is an evidence-based approach to addressing posttraumatic stress symptoms and internalizing symptoms in children. 45 TF-CBT involves a series of skill-based components presented to children and parents in parallel sessions, and culminates in conjoint sessions in which the child shares his or her “trauma story” with his or her parent(s).
Using this approach, the therapist first provided psychoeducation to both Alex and his mother about trauma and PTSD to help them understand Alex’s symptoms and behaviors as common responses to stressful events. Next, Alex was taught relaxation skills to help him recognize, understand, and reduce the physiological reactivity he is experiencing. His parents were taught positive parenting techniques to help them address specific concerns and behaviors. Next, affective recognition and modulation (including feelings identification, intensity ratings, and positive self-talk) was addressed and then cognitive coping skills. Once Alex was able to effectively identify and express his feelings, regulate his emotions, and use cognitive coping skills to address distressing thoughts, his therapist told him that he was ready to create his trauma narrative, which could take the form of any developmentally appropriate undertaking that engaged him in thinking about his traumatic experience, including creation of a story, comic, or song. Alex chose to create a book about his life, his family, and the accident. Through exposure and therapist-guided cognitive processing, Alex increased his ability to tolerate thinking and talking about his accident and identified and altered unhelpful and inaccurate beliefs about what happened (“it was my fault”), himself (“I’m a bad boy”), and the world (“it’s not safe to go outside”). When his trauma narrative was complete, Alex shared it with his parents, who had been carefully prepared by the therapist for this meeting, including engaging in role-plays of supportive and validating responses, praise, and feedback for Alex, thus providing the family the opportunity to practice talking about the trauma together, and simultaneously enhancing the parents’ role as supportive and careful listeners for Alex. The therapist also kept track with Alex’s mother of subsequent pediatric visits and provided the pediatrician with a brief summary of the therapy and Alex’s progress prior to each visit. With this information, his pediatrician was able to efficiently check with Alex’s mother about her perception of Alex’s recovery and the therapy, and to observe how Alex was doing behaviorally in each visit.
By contrast, Danielle (case 2) is an adolescent girl who endured multiple interpersonal victimization events and traumatic losses throughout her early childhood, including emotional and physical abuse at the hands of both her mother and father, twice being removed from her biological parents’ home, and multiple placements in foster homes. Although initially Danielle was relatively asymptomatic despite her significant trauma history, the onset of adolescence brought with it a delayed posttraumatic response. Danielle exhibited some of the more typical symptoms of PTSD, including intrusive reexperiencing (nightmares), avoidance of school, and hypervigilance (sleep and concentration problems), along with dysphoric, angry, and aggressive (externalizing) symptoms. Danielle had limited and inconsistent pediatric care until she was adopted, but her adoptive mother identified a pediatric practice that specialized in adolescent female health issues and scheduled regular checkup visits twice yearly to help Danielle develop better self-care and physical hygiene.
Danielle had been required to undergo emergency psychiatric treatment in several of her previous preadoptive placements. Danielle felt that none of these therapies had been helpful, because either the clinician seemed critical and “made me feel like there was something wrong with me, that I needed to be fixed” or the contact was only for a very limited time period and “as soon as I started to like [the therapists] I had to stop seeing them because I was moved to another group home or foster family.” Danielle had been indifferent toward and unwilling to engage with 2 therapists who the Child Protective Services worker had required her to see, and her adoptive mother did not want to force Danielle to be in therapy. The adoptive mother talked privately about this dilemma with a nursing case manager in the pediatrics office, and the case manager then talked with both Danielle and her mother about what Danielle viewed as helpful in her positive past experiences with therapy and how they could identify therapists with a similar style and orientation whom Danielle could “audition” and then work with for as long as necessary without fear of untimely terminations. Danielle shifted from being unwilling to consider therapy to being skeptical but open to seeing if there was a therapist with whom she felt comfortable who could help—but not “fix”—her.
Danielle’s therapist developed treatment goals that addressed the multiple domains of self-regulation and relatedness difficulties that were affected by the emotional and physical violence and the disruption of primary attachment bonds that occurred within the context of Danielle’s developmental upbringing. In addition, addressing the strained relationship between Danielle and her adoptive mother, and helping her mother to provide consistent care, structure, and monitoring of Danielle’s high-risk behaviors while also supporting Danielle’s normative adolescent strivings for autonomy and privacy, were important components of her treatment. The therapist, with Danielle’s knowledge and permission (and her mother’s consent), updated the pediatric nurse case manager on a monthly basis about the progress, and setbacks, in Danielle’s therapy. When Danielle had her next semiannual pediatric visit, the pediatrician and the nurse case manager were able to ask her and her mother what seemed helpful or not in the therapy, and how they each viewed Danielle’s progress in dealing with emotional and behavioral challenges. With the preparation provided by the therapist’s updates, this discussion was efficient and enabled the pediatric professionals to support Danielle’s progress and her continued therapeutic involvement.
The mental health clinician used a combination of Parent Management Training and Trauma Affect Regulation: Guide for Education and Therapy (TARGET) to achieve these goals. 28 Danielle presented to therapy with the same defiant and angry presentation that her adoptive mother and teachers reported. She quickly told her therapist that she was “fine,” that she would not talk about her past experiences, and that she did not need any therapy. She followed this up with the assertion that she had already been in lots of therapy and “it didn’t help, anyway.” Danielle’s therapist reassured her that she would not have to talk about her worst memories unless she chose to do so, and that therapy would involve her and her mother learning about how coping with trauma turns on an alarm in the brain (the amygdala) that stays on even when it’s not needed unless a trauma survivor knows how to reset it. Danielle liked the idea that her brain had become so proficient at protecting her when she was being abused that now it was stuck in a high alarm state, which was the source of her difficulty with anxiety and anger in relationships and school. As a result, now even small stressors were causing her brain to send out signals to prepare her body for extreme danger (the “fight-flight-freeze” response).
Danielle’s therapist further explained to Danielle and her mother that therapy would help Danielle learn skills to deal with these extreme stress reactions by developing abilities that she already had—but had not known to apply to handle stress reactions—to think clearly and focus on her core values when she recognized that her brain and body were going back into “alarm mode.” In subsequent sessions, Danielle (and her mother in parallel sessions) learned TARGET’s mental focusing skills to help her clear her mind and think before acting, and started to identify the triggers that activated her brain’s alarm response. Together, these 2 skills were the first steps in helping Danielle learn how to prepare for and manage her alarm reactions. Next, Danielle’s therapist introduced TARGET skills aimed at helping Danielle to become aware of her emotions and thoughts in order to identify and differentiate those that were “reactive” (generated by her alarm) from those that reflect her “main” values, hopes, and goals (those that occur when her alarm is reset by focused thinking). Danielle then worked with her therapist to define her “main” goals and identify the choices and behaviors that would help her achieve them. Once Danielle was able to recognize and modulate what had seemed to be uncontrollable stress reactions, she began to recognize her strengths and the many positive qualities she had to offer. As a result, she was able to become closer with her adoptive mother, enjoy her company, and earn her respect and trust, and ultimately regain a stabilizing sense of hope and self-esteem. Although she still felt troubled and saddened by memories of trauma, her PTSD symptoms subsided.
Neurobiology of Psychotherapy
Neurobiological studies in animals have shown that a sense of control over a stressful situation is key for protecting higher brain functions and allowing top-down regulation of behavior, attention, and emotion by the dorsolateral prefrontal association cortex.63,64 When a subject feels out of control, the stress response is activated. High levels of catecholamine and cortisol release take the prefrontal cortex “off-line” while strengthening primitive brain circuits, producing unconscious, reactive behaviors and emotions, and loss of top-down executive control. In contrast, when a subject comes to feel in control of a stressful situation, the prefrontal cortex inhibits the stress response and stays “online” to thoughtfully guide behavior. Effective psychotherapy, which restores a sense of control and insight, likely acts by enhancing prefrontal cortical control over the stress response.63,65
Psychopharmacology
Despite advances in psychotherapy, randomized psychopharmacology clinical trials are noticeably lacking for pediatric PTSD. Selective serotonin reuptake inhibitors (SSRIs) are considered to be first-line medications for adults with PTSD, and paroxetine and sertraline have a US Food and Drug Administration indication in adults. However, 2 independent controlled trials of sertraline in pediatric PTSD failed to demonstrate efficacy when compared with placebo.66,67 Pediatric PTSD is highly comorbid with other psychiatric disorders and SSRIs are effective for the treatment of pediatric anxiety disorders 68 and depression. 69 Adrenergic medications such as guanfacine extended release and prazosin may have a role in the adjunctive treatment of dysregulated behavior associated with pediatric traumatic stress.70,71 However, no randomized controlled trials have yet been completed to support their use for this condition.
Discussion
Recent and continuing community violence has focused attention on the symptoms and consequences of maladaptive traumatic stress and PTSD in children and adolescents. Children suffering from neglect and abuse are not uncommon in the population. Given high rates of traumatic stress exposure in children and adolescents primary care clinicians and pediatricians may increasingly be asked to identify disorders of posttraumatic stress in their treatment practices. DSM-5 has new diagnostic PTSD criteria for children younger than 6 years. With these diagnostic changes, the prevalence of young child PTSD diagnoses may increase in the population and may increasingly present to the pediatrician for screening, evaluation, and referral.
Current standards-of-practice support TF-CBT as an evidenced-based first-line psychotherapeutic treatment for children with PTSD following abuse or community violence.53,66 Despite its overall efficacy, many children and parents decline therapy involving intensive discussion of traumatic experiences, between one quarter to one third of children do not respond to this type of treatment, and in community samples, up to 40% drop out before treatment is complete. 72 Although there is a national network of trained TF-CBT psychotherapists (http://www.nctsn.org), most mental health clinicians have not received TF-CBT training and certification, leading to long waiting lists for PTSD treatment in many mental health practices and clinics. As illustrated by the second case example, trauma-specific emotion regulation psychotherapy (eg, the TARGET intervention) is a viable evidence-based approach for older children and adolescents who either refuse trauma-narrative therapy or whose externalizing behavior problems interfere with therapeutic engagement. 57 Psychopharmacology remains adjunctive to evidence-based psychotherapies for pediatric PTSD.
Progress in the treatment of early-onset disorders of maladaptive traumatic stress is being facilitated by emerging knowledge of phenomenology, prognosis, risk and protective factors, and the neurobiology of stress. Ongoing research in this field offers hope to children and adolescents suffering from the effects of traumatic stress exposure in the developing years. By staying informed about the rapidly developing science and the expanding evidence-based clinical options for the treatment of children’s posttraumatic behavioral and emotional disorders, pediatric professionals can respond efficiently and effectively to ensure that traumatized children in their practice receive timely, well-coordinated, and ultimately beneficial treatment.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.