
Abstract

Introduction
Sleep disorders are an underlying cause of attention deficit/hyperactivity disorder (ADHD), 1 but they are underdiagnosed in children. 2 Finding and treating sleep disorders is important because, as Chervin et al,3(p1185) stated, “Our data suggest that . . . 25% of all children with ADHD . . . could have their ADHD eliminated if their habitual snoring and any associated [sleep-related breathing disorders] were effectively treated.”
The reported prevalence of children with ADHD varies among countries, from 3% to 16%. These differences have been attributed to differences among diagnostic methods.4-7 In the United States in 2009, the prevalence of ADHD in children and adolescents was 9%, and the diagnosis rate was increasing. 8 Furthermore, contrary to earlier medical opinion, it is clear that up to 60% of individuals who suffered ADHD as children also experience symptoms as adults, often with profound effects, including more substance abuse, lower socioeconomic status, and higher divorce rate.4-7
ADHD and sleep disorders are also associated with other psychiatric, medical, and neurodevelopmental problems, such as major depression, bipolar disorder, autism spectrum disorders, aggression, poor communication and social skills, and obesity.9-14 Mitigating or eliminating the symptoms of ADHD and possibly other behavioral disorders by treating an underlying sleep disorder may reduce or eliminate the need for treatment with medications.15,16 This is of special importance to avoid potentially unnecessary long-term medication use.
This article describes the sleep disorders commonly affecting children and adolescents with ADHD and other disorders, the office assessment of these sleep disorders, and treatment strategies. Figure 1 provides a checklist for the office assessment.
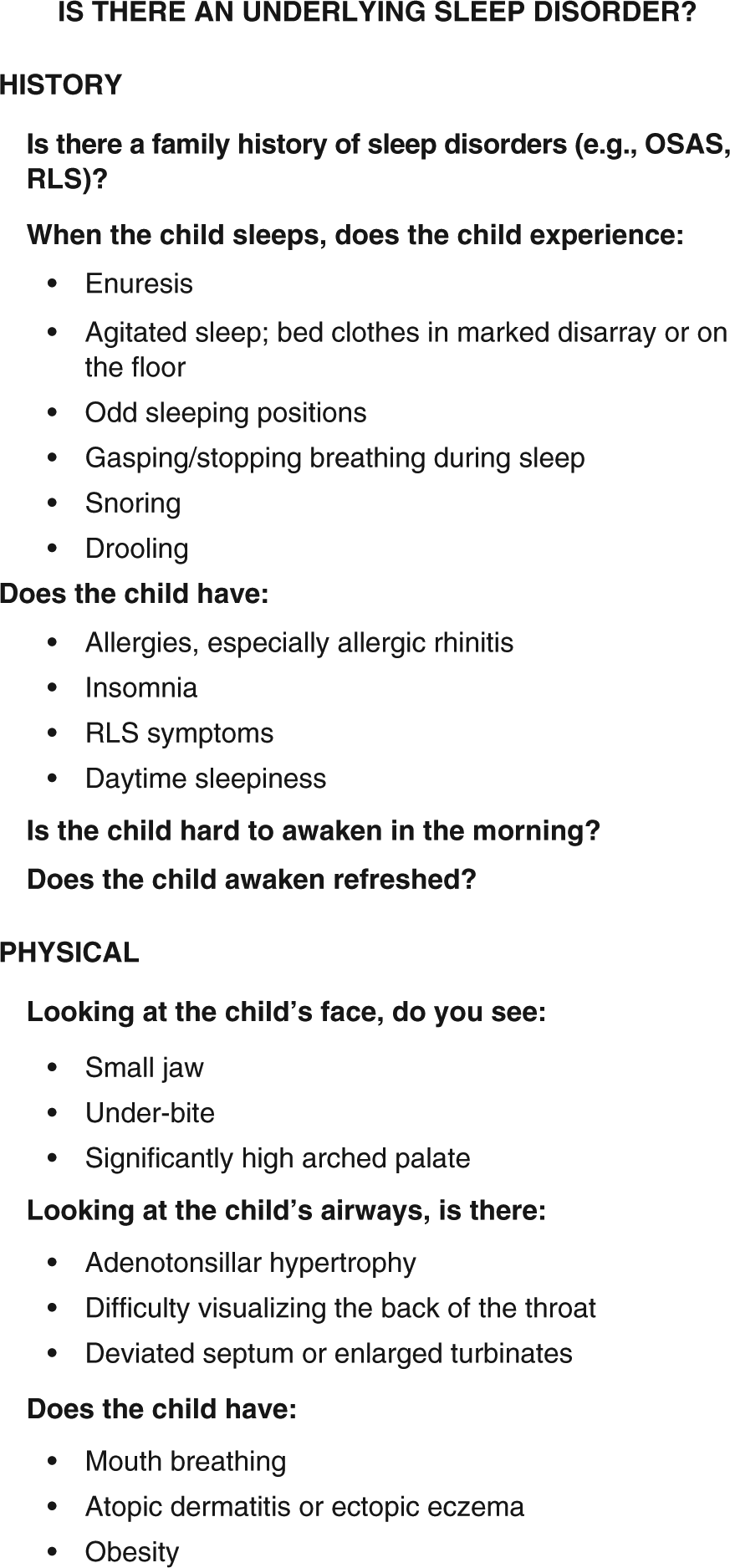
Summary of Symptom Assessment.
Sleep Disorders
Obstructive Sleep Apnea Syndrome/Sleep-Disordered Breathing
The American Academy of Pediatrics recognizes obstructive sleep apnea syndrome (OSAS) as a common disorder, with a prevalence of 1.2% to 5.7%.17,18 It is characterized by episodes in which the airway becomes blocked during the deepest, restorative levels of sleep.19,20 The blockage causes blood oxygen levels to fall, and the carbon dioxide levels rise, triggering the arousal of the individual. These episodes can occur many times per hour, interfering with restorative sleep, and leading, in time, to chronic sleep deprivation.
The airway system is complicated, and it becomes even more so during deep states of sleep. 21 For example, nasal congestion, soft tissue hypertrophy (such as enlarged or swollen tonsils and adenoids), septal deviation, and the placement of the soft palate and uvula, as well as the arch of the hard palate, can significantly diminish airflow into the lungs.
Sleep-Related Movement Disorders (Restless Legs Syndrome)
Not all sleep disruptions are related to breathing problems. Sleep-related movement disorders, such as restless legs syndrome (RLS), can also contribute to ADHD. 22 Children with ADHD are diagnosed with RLS more often than controls.23-25 Those with both conditions have slightly worse ADHD symptoms than ADHD children without RLS.24,26,27
Narcolepsy
Narcolepsy, a disorder of hypersomnia, is often diagnosed in adulthood; it is said to be underdiagnosed in children.28-30 Excessive daytime sleepiness is a common complaint in childhood narcolepsy, and the restlessness that children use to combat the sleepiness can be misdiagnosed as ADHD.29-31 In fact, many adults diagnosed with narcolepsy report a history of ADHD. 32 The 2 disorders can be confused even in adults. 33
Diagnosing Sleep Disorders: History
Family History
Often, genetically determined craniofacial structures, such as a small or retrognathic jaw, may significantly impede the airway during restorative sleep.34-39 One study suggested that up to 40% of the differences in sleep quality could be genetic. 40 As a result, a family history of OSAS can be helpful in the diagnosis. A patient with an immediate family member suffering from OSAS is up to twice as likely to receive that diagnosis; if there are multiple such family members, the odds increase still further.41-43
Race
Race, as it identifies common phenotypes, can also inform an OSAS evaluation. For example, compared with Caucasians, African American children are at higher risk of OSAS 44 ; Asians appear to have a similar risk to Caucasians, but their symptoms are often more severe45-47; and Hispanics might have a higher risk, but it is unclear. 48
Sleep Positions and Behavior
Children with ADHD often have restless sleep.49-51 Frequent changes in sleep position could indicate OSAS: Everyone changes sleep position occasionally, but changing so frequently that bedclothes are tangled or on the floor by morning frequently indicates a sleep disorder. 52 A child with OSAS could also have night sweats as a symptom.47,53
Sometimes the sleep positions that children choose suggest sleep-disordered breathing. Some children try to minimize obstruction by adopting odd positions, such as prone, curled on hands and knees, with the neck hyperextended.54,55 Many position themselves so they can breathe through their mouths and therefore awaken thirsty, with dry mouths. 56 A parent might also notice excessive nighttime drooling.
Excessive Daytime Sleepiness
Although many children with OSAS have difficulty awakening, excessive daytime sleepiness is often not a presenting complaint. One study that examined the sleepiness and hyperactivity of children with suspected sleep-disordered breathing found that they were both sleepier and more hyperactive than a control group. 57
Though children with sleep disorders are more tired, their parents might not be aware because the indications might be obscured by the child’s hyperactive behaviors, which are likely to be secondary to exhaustion. Therefore, the apparent absence of daytime sleepiness should not be used to rule out sleep-disordered breathing.
A commonly used questionnaire for evaluating patients with suspected sleep disorders is the Epworth Sleepiness Scale. Unlike adults, however, children’s scores on the scale were only weakly correlated with the results from their sleep studies. 57 A recent review of existing sleep questionnaires suggested others that were better indicators for children. 58 The 2 recommended questionnaires were the Sleep Disorders Inventory for Students and the Sleep Disturbance Scale for Children. 59
Snoring
A 4-year study showed that snoring is a predictor of the worsening of a child’s hyperactivity, as are other symptoms of sleep-disordered breathing. 60 Note, however, that although snoring can be a problem in children with OSAS, snoring is not always present. In one study, children with OSAS used home cardiorespiratory monitors to monitor their sleep and 25% to 47% of them did not have “loud snoring at least 1 to 2 times per week.”44,61 Another study checked for OSAS in children who either did not snore or rarely snored: 5% did, in fact, have obstructive sleep apnea.61,62
In adults, snoring is a common presenting symptom of OSAS; this is less true for children and this symptom, although helpful, is not critical for diagnosis. About 50% of adults snore, while estimates of the percentage of children who snore range from 3% to 27%.37,63,64 The disparity in the estimates for children may have many causes, including parental reporting. One study found that although parents reported that their children did not snore or only occasionally snored, 2.3% actually had “pathologic” snoring, and another 6% had significant hypopnea when tested. 61
Enuresis
Enuresis is more common in children with ADHD. 65 The frequency of enuresis is also positively correlated with snoring and adenotonsillar enlargement.66,67 The National Kidney & Urologic Diseases Information Clearinghouse reports that, in the general population, the percentage of children with enuresis decreases with age, affecting 10% of 5-year-olds and dropping to 1% by age 18. 68 In contrast to the general population, 41% of children 4 years and older who were referred to a sleep center for suspected sleep-disordered breathing reported enuresis. After all the children in the study had polysomnography, it was found that those with OSAS were 30% more likely to have enuresis than those without. 66
Based on these observations, it is not only important to ask patients presenting with symptoms of ADHD about enuresis but also to consider sleep disorders in any patient presenting with the complaint of enuresis.65,69-71 Of great clinical importance is that treating OSAS is likely to decrease or resolve related enuresis.71-75
Restless Legs Syndrome
Symptoms of RLS can be difficult for a child to describe, so asking about a family history of the disorder may be very helpful.76,77 Note that it is not necessarily helpful to ask the parent whether the child has these symptoms: One study showed that fewer than half of the parents of children diagnosed with definite or probable RLS were aware of the child’s symptoms. 78
Symptoms include paresthesias in the lower extremities and an intense need to move the legs, especially when resting or sleeping, since movement temporarily relieves the symptoms. In addition, some children report RLS symptoms when trying to sit quietly during the day, for example at school. The resulting restlessness and difficulty maintaining concentration can mimic the symptoms of ADHD. 78
Growing pains in a child with ADHD can indicate restless legs syndrome. One small study found that of children with both ADHD and growing pains, 91% had RLS. In another study of more than 10 000 families, significantly more children with RLS had growing pains, compared with controls. 78
Allergies
Children with ADHD are more likely to have allergies and, more specifically, allergic rhinitis, than controls.79-82 Similarly, children with allergic rhinitis are more likely to have ADHD than controls.83-85 The link between the 2 is likely the sleep disruption caused by the nasal congestion of allergic rhinitis.83-85
Of particular importance, allergic rhinitis can also result in mouth breathing, which can lead to changes in facial growth that may exacerbate the sleeping problem and therefore the ADHD. The changes can begin to reverse if treating the allergic rhinitis stops the mouth breathing.86,87
Diagnosing Sleep Disorders: Physical Examination
Soft Tissue and Craniofacial Problems
A number of soft tissue and craniofacial problems can predispose a child toward OSAS. Adenotonsillar hypertrophy is the most common.34,36,88 Other soft tissue problems include enlarged turbinates and nasal congestion, possibly due to allergies, chronic rhinosinusitis, or a deviated septum.88-90 Children with these issues often breathe through their mouths when awake.
Mouth breathing can cause a child to develop a narrow maxilla and mandibular retrognathia (also called mandibular hypoplasia), which are craniofacial problems also associated with OSAS. 91 Treating sleep-disordered breathing may lead to whole or partial reversal of craniofacial problems, according to 2 studies.86,87 In one study, the mean age at the start of treatment was approximately 5 and a half years. 87
A narrow skeletal maxilla and mandibular retrognathia are not the only craniofacial problems associated with OSAS. Midface hypoplasia can also indicate OSAS.92,93 A child with midface hypoplasia can seem to have large eyes, forehead, and lower jaw; there is often an underbite. This problem appears, for example, in patients with Down’s syndrome, as well as those with achondroplasia.94,95
Another soft tissue problem indicating possible OSAS is more opaque paranasal sinuses on MRI or CT scans. 89 Opacification can be caused by thick mucus or inflammation, especially from chronic sinus infections.
Obesity
Obesity and ADHD demonstrate significant comorbidity.96-100 Obesity and OSAS do, too.36,39,101-103 ADHD children with sleep-disordered breathing are more likely to be obese than ADHD children without sleep-disordered breathing. 38 ADHD is also common among morbidly obese adults, and a study that checked for other comorbid conditions found that these patients also had a very high rate of sleep apnea.104,105
Atopic Dermatitis/Atopic Eczema
A child with both ADHD and atopic dermatitis (also called atopic eczema) should be evaluated for OSAS. The three conditions are strongly correlated, demonstrating that a child with ADHD and atopic dermatitis very often has a sleep disorder. 43 Similar results were obtained by Camfferman et al. 84
Following up on Sleep Disorder Symptoms
If, after medical evaluation, OSAS or other sleep disorders are suspected, it should be confirmed by polysomnography and appropriate blood tests (eg, serum iron, ferritin, and total iron-binding capacity). The blood tests may assist with the diagnosis and treatment of RLS, especially in teenagers. 106
If there are indications that allergic rhinitis is present, the problem should be confirmed through testing by an allergist so that it can be aggressively treated. Resolving congestion that causes mouth breathing can prevent craniofacial changes that cause continuing risk of OSAS, or possibly begin to reverse them if they are already present.86,87,91
Treatment Options
Surgical and nonsurgical options are available depending on the etiology and severity of the sleep disorder. 91
Nonsurgical Options
Sleep Hygiene Training
Sleep hygiene training, sometimes combined with CBT, is an important part of improving sleep regularity and duration. Sleep hygiene includes having a calm, predictable bedtime routine in a dark and quiet room that is comfortable and without distractions. There should be no lights on clock faces. Similarly, turn off computers, cell phones, televisions, and so on since it is important to minimize exposure to bright lights.
Minimizing exposure to bright lights for 1 to 1.5 hours before bedtime is important because the light subdues or delays the adequate release of the melatonin necessary for sleep. 107 A 6-month follow-up showed that the improvements gained through sleep hygiene therapy were maintained.108,109
Continuous Pressure
CPAP is very effective in the treatment of OSAS, although there are issues that may interfere with its use in children. For example, as children grow, the masks require frequent refitting.110,111
Medication and Immunotherapy
Medication, immunotherapy, or both, are available to treat allergic rhinitis. Medications include oral and intranasal antihistamines, intranasal corticosteroids, and decongestants.91,112-115 Immunotherapy, subcutaneously or orally delivered, has been shown effective for children in reducing sensitivities that lead to allergic rhinitis.91,113,115-119 Immunotherapy is a longer term treatment: It produces lasting results, but they are not immediate.
Melatonin
Melatonin, in dosages of 3 to 6 mg, has been shown to be an effective treatment of insomnia in 6- to 14-year-old children with ADHD. 120 Studies suggest, however, that the decreased sleep latency did not affect the ADHD symptoms.111,122 It could be that although the children using melatonin sleep more, they are still not sleeping enough. In the studies cited, even with the increased sleep, the children were getting less than the recommended amount for their age groups.
Orthodontia
Rapid maxillary expansion may be used to help correct an overly high arched palate. In one study, patients retained the improvements in their sleep apnea when rechecked 24 months following the completion of this treatment. 123
Rapid maxillary expansion is not the only orthodontic treatment available to help resolve OSAS. A number of appliances are available, many of which reposition the jaw during sleep. 124 A jaw repositioning appliance has been shown effective for children as young as 3 years.125,126
Iron Supplements
Iron supplements for patients with RLS, especially if their serum ferritin and/or iron levels are low, have been shown in one study to help adolescents; however, more information is needed.106,127,128
Medication
Medications for patients with RLS, such as anticonvulsants, dopaminergic agents, opiates, and benzodiazepines have been reported as useful in adults.129,130 As of 2011, none of these medications was approved for children by the Food and Drug Administration. 131
Music Therapy
Learning to play a double-reed instrument (oboe or bassoon) or the didgeridoo (an Australian Aboriginal instrument) was found to be helpful in relieving mild to moderate OSAS in adults.132,133
Surgical Options
Adenotonsillectomy
Adenotonsillectomy appears to be the most common and effective surgical treatment of OSAS in children when soft tissues are involved. In a child with adenotonsillar hypertrophy or an enlarged uvula, this procedure is expected to treat not only the soft-tissue problem but also any accompanying OSAS. 134
Adenotonsillectomy often also improves the hyperactivity that accompanies the OSAS. One study tested children with the problem who, pre-surgery, were significantly more hyperactive than a control group. At one year following their adenotonsillectomies, the hyperactive children had improved enough that the 2 groups were indistinguishable. 135
Adenotonsillectomy is not necessarily a cure-all for OSAS and the associated ADHD if the child also has other OSAS risk factors, however. An observation that is highly correlated to the outcome of adenotonsillectomy in treating OSAS is to look at the child’s throat when the child is sitting, neck extended, with tongue out. If you can see just the soft palate and base of the uvula at the soft palate, or even less, additional treatment after the adenotonsillectomy may be needed to cure the OSAS. 136
Other Corrective Surgeries
Other corrective surgeries include septoplasty for a deviated septum, turbinectomy for enlarged and obstructing turbinates, corrective jaw surgery for mandibular hypoplasia, and the more extensive maxillomandibular advancement or maxillomandibular expansion surgery when required to open the airway.91,113,137-143 Note that some surgeries, such as septoplasty, are not necessarily appropriate in young children. 91
Conclusion
When assessing ADHD and other disorders such as depression, autism spectrum disorders, and obesity, physicians should consider sleep disorders as an underlying cause. This article has surveyed the literature, and described steps for determining whether a sleep disorder is likely: the family history; other clinical information, such as whether the patient has enuresis, snoring, or eczema; and a standard examination of the nose, throat, and other presenting physical features of the patient (see Figure 1). If the physician suspects a sleep disorder, the patient can be referred to a sleep specialist for confirmation. This review has also outlined possible treatments for sleep disorders.
Footnotes
Acknowledgements
We wish to thank Dr Rafael Pelayo, MD, Clinical Professor, Sleep Medicine Center, Stanford University School of Medicine, for providing suggestions about the article.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.