
Abstract
Objective. To assess current practices of New York State pediatricians as they transition youth with special health care needs to adult-oriented medical care. Methods. A survey of New York State pediatricians included 6 critical steps from 2002 consensus statement, 11 essential steps adapted from recent literature, and questions targeting age of starting transition and availability of transition policy. Results. Of 181 respondents, only 11% have a transition policy. Most assist patients in transition process; identify an adult provider (92%); and create portable medical summary (57%). Only 3% start planning process at recommended age. No respondents are compliant with all 6 critical steps; subspecialists were more likely to report compliance to more than 4 steps. Conclusions. Participating pediatricians are making gains, yet effort is needed, to incorporate the essential steps into practice for transitioning youth with special health care needs. Recognition of barriers, use of electronic tools, and clarifying subspecialist’s approach, may improve compliance with transition recommendations.
Keywords
Introduction
The numbers of children with special health care needs who are surviving to adulthood nationally is growing. 1 Approximately 750 000 (90%) of youth with special health care needs (YSHCN) survive to adulthood each year in the United States. 2 In New York State (NYS) there are approximately 570 000 children with special health care needs, and about 15% of them are between the ages of 12 and 17 years. 3 An uninterrupted transition to adulthood and adult-oriented medical care is a necessary process to accommodate YSHCN.4-6
The challenge of providing such transition has been recognized in research and practice for at least a quarter century, especially bought to attention at a conference led by the US Surgeon General. 4 A Healthy People 2020 goal is to increase the overall rate of YSHCN whose primary care provider discuss transition planning with the youth and/or his/her adult caretaker. 7 A 2002 consensus statement, 5 and an updated clinical report of 2011, 6 outlined recommended steps for primary care providers to help guide patients through the transition process. The 2002 consensus statement, 5 developed by the American Academy of Pediatrics (AAP), the American Academy of Family Physicians, and the American College of Physicians, highlighted 6 “critical first steps” of the transition process: (1) creation of a transition plan for YSHCN, (2) identifying the adolescent’s core knowledge and skills, (3) identifying a health professional in the medical home to coordinate care, (4) maintaining an up to date medical summary, (5) ensuring ongoing preventive health care until transfer to the adult practice, and (6) ensuring affordable health care insurance. 5 Recent literature has emphasized 5 additional steps to optimize the ongoing transition process: (7) identifying an adult medical provider to accept the transferred youth,8-10 (8) creating an emergency plan for the youth, 11 (9) discussing legal aspects of transition, 11 (10) discussing realistic future goals with the adolescent alone, 10 and (11) discussing realistic goals jointly with the adolescent and the family. 10 Together, these “11 essential steps” are crucial to ensuring a seamless transition from pediatric to adult-oriented care (see Table 1), and are echoed in the AAP’s 2011 clinical report. 6 The report also highlights the previously recognized importance of starting the transition planning early and the creation of a written transition policy. 6 Transition planning for YSCHNs should start between 11 and 14 years old6,11 to allow time for a developmentally-appropriate process. A written transition policy6,8,12,13 promotes practice uniformity and communicates to patients and families how transition planning and transfer should proceed.
Eleven Essential Steps of Health Care Transitioning. a
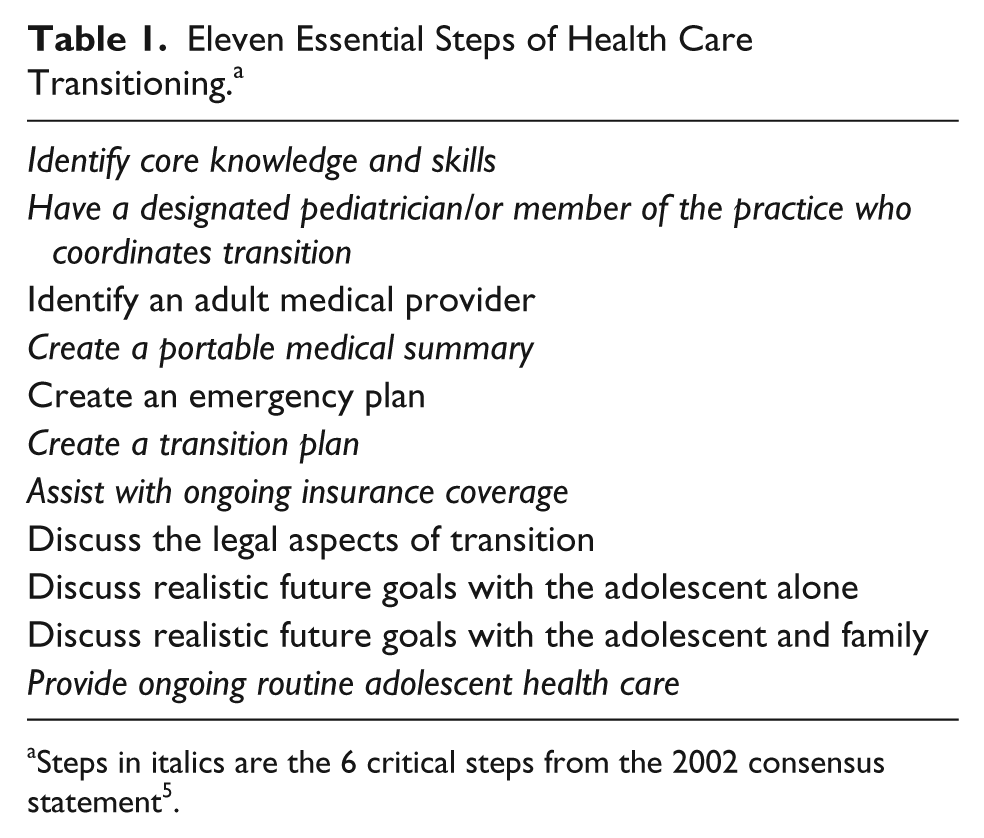
Steps in italics are the 6 critical steps from the 2002 consensus statement 5 .
To our knowledge, no prior study has examined, either nationally or locally, provider compliance with the 2002 recommendations 5 as an aggregate measure, or the differences in practice between subspecialists and generalist pediatricians with regard to transition planning for YSHCN. These gaps in the literature are the focus of this study. Given the current national emphasis on transition planning, 1 and anticipating the changes that might occur in response to the 2011 AAP Clinical Report, 6 examining current practices and barriers to best practice will assist in planning for resources and provider educational needs at the regional and institutional level.
The purpose of this study is to assess current transitioning practices of NYS pediatricians caring for YSHCN. The membership of the 3 NYS chapters of the AAP represents a diverse group of pediatricians, who practice in academic institutions as well as in private practice, generalists as well as subspecialists with an ethnically and geographically diverse patient population. To further improve child health, and in concert with the advancing literature, the strategic plan for 2010 New York State chapter 3 of the AAP American Academic of Pediatrics included improving “Transition planning to adult medicine for adolescents with special health care needs” as a goal for the future.
The study sought to determine (1) the proportion of NYS pediatricians with a written transition policy, (2) the proportion of physicians who report assisting their patients’ transitions to adult care providers, (3) when providers start the transition process for their patients, (4) what proportion of providers are compliant with the 6 critical steps outlined in the 2002 consensus statement and the aggregate 11 essential steps identified in recent transitioning literature, (5) the differences between generalists and subspecialists in compliance with the recommended steps, and (6) identifying barriers within the transitioning process and how they affect the providers’ transitioning practices.
Methods
A survey was developed via adaptation of existing measures and through intense literature review to ascertain practice patterns for NYS pediatricians treating YSHCN.5,8,9,11,14 This survey was a cross-sectional voluntary survey sent along with consent information via email and link to all NYS AAP members (n = 4000) in late spring of 2011. Four reminders were sent—via email (twice), a postcard (once), and through a Web-based newsletter, between May and September 2011. Data obtained through end of September 2011 are reflected in this article. Respondents were included who had direct patient care of youth ≥12 years old. Survey was administered via Survey Monkey and is available on request. Institutional review board approval was obtained from the Montefiore Medical Center Institutional Review Board.
Development of the Survey
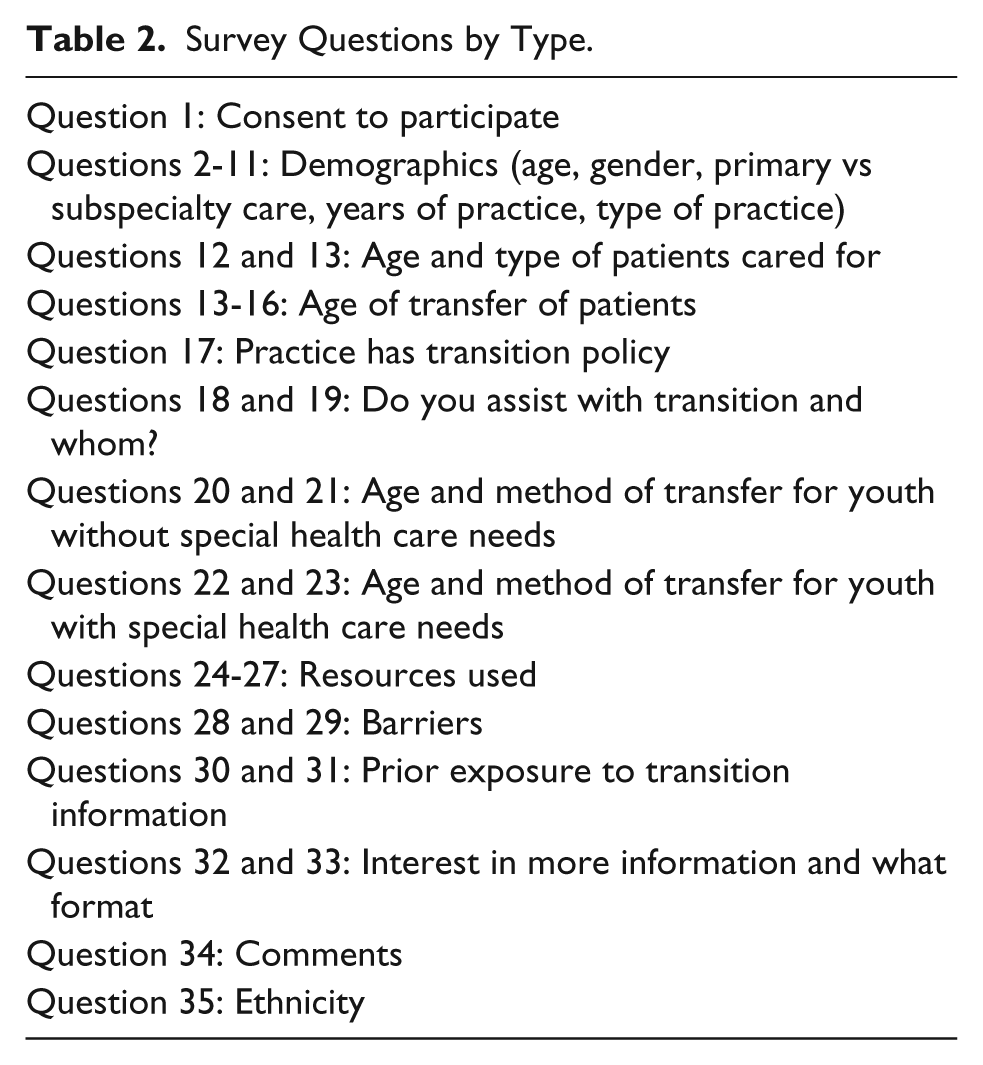
The 6 critical first steps from the 2002 consensus statement 5 and the 2008 survey by McManus et al 13 were used as the basis for the survey adaptation and development (see Tables 1 and 2). Based on literature review, certain questions were added regarding presence of a written transition policy, 8 the age to start transition planning 5 details of transition support services,5,6,8,9,11 and barriers to transition.9,14 The survey expanded on previous provider surveys and broadened the scope of the information requested. Prior to distribution, a paper version of the survey was pilot-tested with 15 pediatricians in a large hospital-based teaching practice. The input from these providers was used to clarify and finalize the questions in the survey. For this survey, YSHCN were defined as children/adolescents with any chronic medical, physical, or emotional problem. The survey contained 35 questions, 17 questions were closed ended, 5 questions were open ended, and the rest were a mix, including an option to write in additional information (see Table 2).
Survey Questions by Type.
Data Analysis
Descriptive statistics of the demographic characteristics and the responses are presented as proportions for categorical variables and mean (standard deviation) for normally distributed continuous variables. Continuous variables that did not meet normality assumptions were presented as median and interquartile range. Age of respondent was collected as age-group categories and dichotomized to <50 and ≥50 years old. Years in practice were recorded in categories and dichotomized to ≤20 and >20 years. Participants did not always answer every question so that proportions were calculated with the denominator of those who responded to the particular question.
To evaluate which respondents were adherent with the 11 essential steps, a compliance score (CS11) was calculated for each participant, as the sum of these steps (0-11) with 1 point assigned to each step. A subset of CS11 that coincided with the 6 critical steps (0-6) was turned into a second compliance score (CS6) for each respondent. CS6 was dichotomized as good compliance (≥4) or less than good compliance. We picked ≥4 as the top quintile of responses. CS6 was subdivided from the 11 steps to document level of incorporation of the 2002 consensus statement almost a decade after its publication. Odds ratios (ORs) and 95% confidence intervals (CIs) were calculated for associations of good compliance with respondent characteristics. Independent-samples t test was used to compare mean scores (CS6 and CS11) between those reporting any barriers and those reporting none. Data analyses were performed with SPSS v2.0 for Windows. A 2-tailed α of .05 was used to denote statistical significance.
Results
Population/Demographics
The survey was sent to 4000 pediatricians; 199 responded to the survey (5% response rate). Eighteen were excluded because they did not have direct patient care of youth ≥12 years old leaving a study sample of 181; 70% of respondents were female and 77% were within the 30- to 64-year age group. At the time of the survey, a similar percentage (72%) of all NYC AAP members were between 30 and 64 years old and females represented 59% of the membership. The respondents represented 22 NYS counties; which house the workplace of 90% of all NYS AAP pediatricians. The majority of the respondents (72%) were practicing primary care only, 12% practiced a subspecialty only, and 15% practiced both primary and subspecialty care. Approximately one-third of the respondents were in private practice (38%), approximately one-third were in hospital-based practice (33%), about a sixth (17%) were clinic based, and the remaining practiced in varied settings (Table 3). Approximately equal numbers of providers had predominantly urban-residing patients versus those who have a mix (Table 3). Pediatric subspecialists came from the following fields: adolescent medicine, endocrinology, hospitalist medicine, infectious disease, emergency medicine, child psychiatry, critical care, hematology-oncology, gastroenterology, and neurology.
Survey Respondent Characteristics.
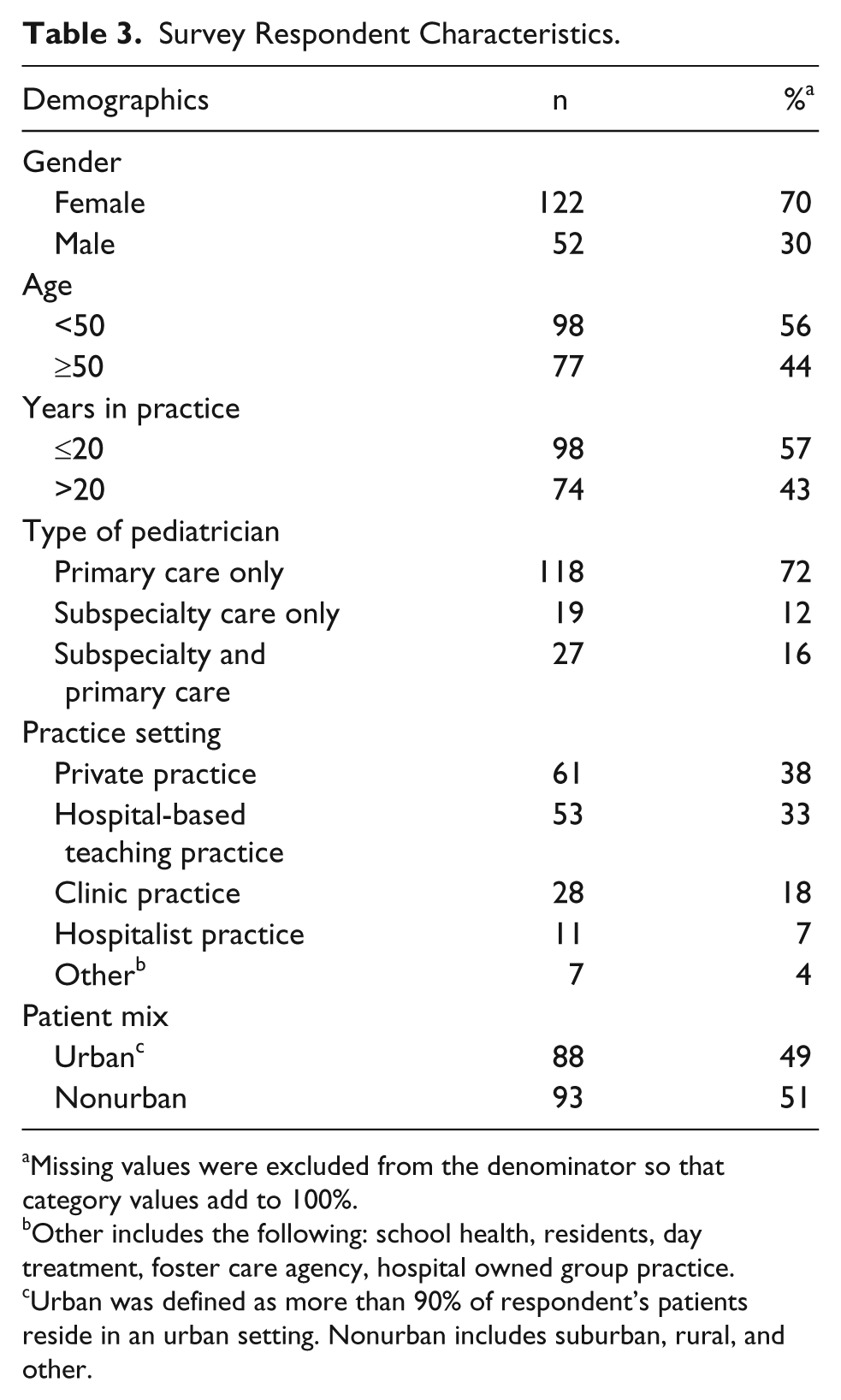
Missing values were excluded from the denominator so that category values add to 100%.
Other includes the following: school health, residents, day treatment, foster care agency, hospital owned group practice.
Urban was defined as more than 90% of respondent’s patients reside in an urban setting. Nonurban includes suburban, rural, and other.
Who Has a Written Transition Policy?
Of the sample, only 11% reported having a written transition policy (95% CI, 6-16). Those <50 years old were more likely to have a written transition policy compared with those ≥50 years old (17.3% vs 3.8 %, P = .005, OR 5.2, 95% CI, 1.5-18.6). Similarly, those practicing pediatrics ≤20 years were more likely to have a written transition policy compared with those practicing >20 years (17.3 vs 4.1%, P = .007, OR 5.0, 95% CI, 1.4-17.7). No significant differences were found between those respondents with and without a written transition policy with regard to gender (P = .96), primary versus subspecialty practice (P = .31), or percentages of patients living in an urban setting versus those living in nonurban settings (P = .22).
Do Pediatricians Assist Patients With Transition Process and When Do They Start?
Of the eligible respondents, 133 (73%) indicated that they assist their patients in transitioning to an adult practice. More than half (63%) of these reported assisting all adolescents and 27% reported assisting only YSHCN. Of the remaining 10%, the majority responded that they assisted those who requested assistance. Sixty-eight percent of the 133 who did assist patients transitioning reported that they start the transition process between ages 18 and 20 years for their YSCHN patients. Only 3% of these 133 reported starting transition planning for their YSCHN at the recommended age of 12 to 14 years.
Are Pediatricians Compliant With the 6 Critical First Steps in the Transition Process for YSHCN?
Of the 133 who reported assisting in transition, 128 responded to the question about methods of transition for YSHCN. None of them were fully compliant with the 6 critical first steps; 17% had CS6 ≥4, and the overall mean ± SD CS6 score was 2.2 ± 1.4. Subspecialists had 3 times greater odds of having a CS6 score ≥4 compared with primary care physicians (33.3% vs 13.0%, OR 3.3, 95% CI 1.3-8.6). Gender (P = .67), age of practitioner (P = .63), years in practice (P = .46), or practice mix (urban vs nonurban P = .25) was nonsignificantly associated with the 6 critical step compliance score.
Do Pediatricians Perform the 11 Essential Steps for Transition of YSHCN?
Of the 128 respondents who answered about methods of transition, 92% reported identifying an adult medical provider for their YSHCN, 57% reported that they create a portable medical summary, 66% reported discussing realistic future goals with the adolescent and family, and 60% reported providing ongoing routine adolescent care. These respondents reported performing the remaining essential steps less than 40% of the time (range from 13% to 48%; see Figure 1). Of note, only 37.5% discussed legal aspects of transition and 28.5% assisted with ongoing insurance coverage. Few in the study identify patient’s core knowledge and skills (34.4%), create a transition plan (30.5%), discuss future goals with the adolescent alone (28.9%), create an emergency plan (16.4%) or have a designated coordinator for transition practices (12.5%).
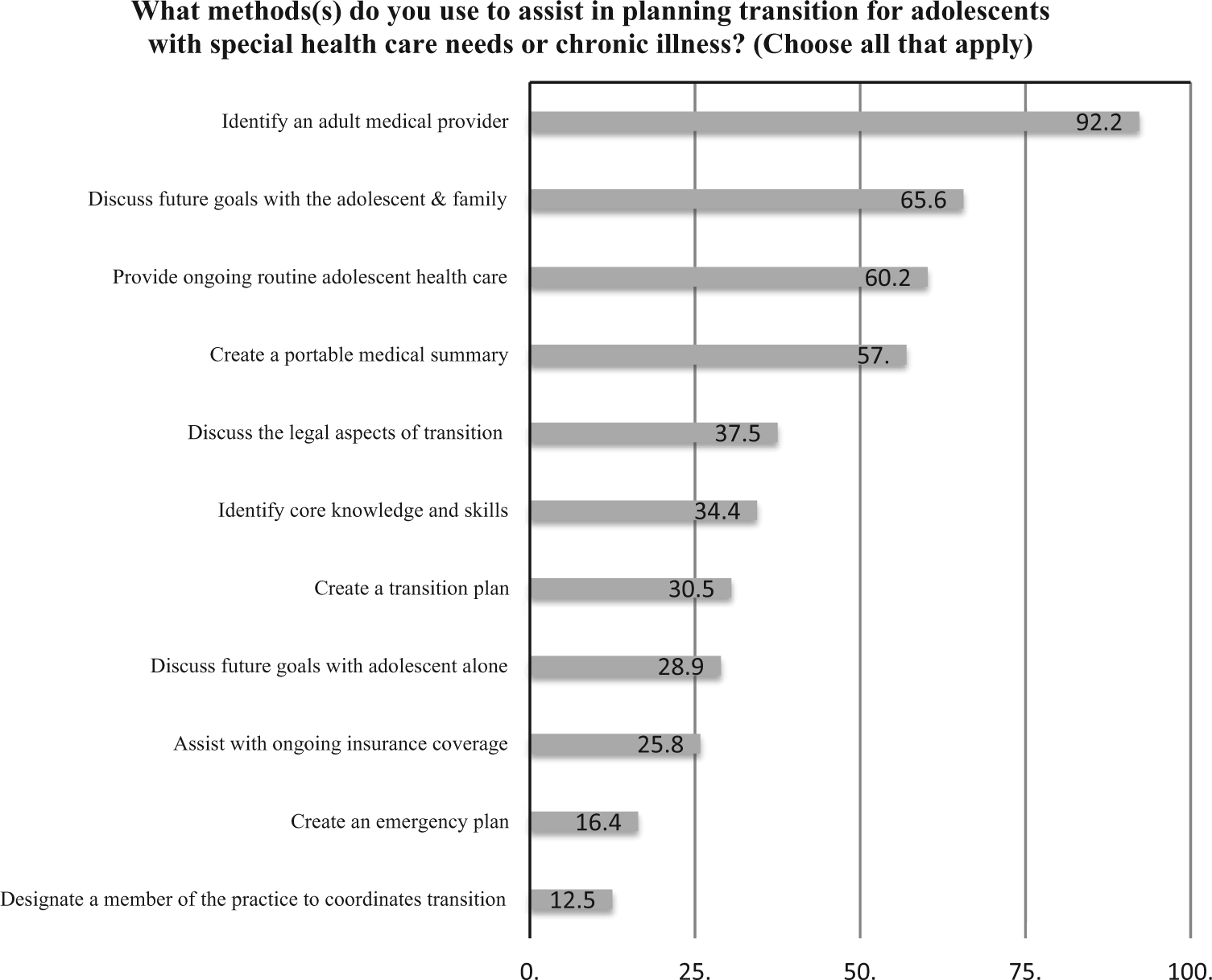
Methods used by New York State pediatricians to assist in transition planning.
What Are the Barriers to Transition?
Of the 133 who reported assisting in transition, 59% reported barriers. The barriers reported by those respondents included: difficulty finding an adult provider (86%), lack of time (49%), difficulty letting go (40%), and financial reimbursement (29%).
Is There an Association Between Perceived Barriers to Transition of YSHCN and With Compliance With the 2002 Six Critical First Steps, and the 11 Essential Steps?
Of the 133 who reported assisting in transition, those who reported barriers to transition had a modestly higher mean steps on the CS11 and CS6 although not statistically significant (P = .06 and P = .13, respectively).
Discussion
Our findings suggest that a substantial majority of our respondents from the NYS AAP assist their patients in transitioning to adult practice. This is an improvement over a study of pediatricians in 2008, which found that fewer than 50% of pediatricians nationally reported assisting with the transition process of their patients. 9 It is also noteworthy that 92% of our respondents, compared with 47% nationally in 2008, 9 reported assisting with identifying an adult medical provider for transfer, as well as 57% of the respondents in our study reported creating a portable medical summary, compared with 27% nationally in 2008. 9
Although results of this study suggest that we are moving closer to the Healthy People 2020 goal 7 to increase the overall rate of YSHCN whose primary care provider discuss transition planning with the youth and/or his/her adult caretaker most respondents begin the process later than recommended. Prior surveys similarly report that almost two-thirds of pediatricians did not report starting transition planning until patients are between 18 and 21 years old. 9 Only a small minority of NYS AAP pediatricians responding to the survey have a written transition policy in their workplace (11%). Those who have a policy are more likely to be younger pediatricians and practicing less than twenty years. The percentage of pediatricians who have a written transition policy is practically unchanged if not slightly worse than a previous survey in 2008 (13%). 8 That younger pediatricians currently have transition policies could be a reflection of current resident education or exposure to the recent literature on transition practices.
Our study also shows that no responding NYS AAP pediatricians have incorporated all eleven essential steps or the 6 critical first steps. 5 Pediatric subspecialists were more likely to report employ more of these 6 steps than primary care providers. The volume of YSHCN cared for, the increased complexity of medical issues, and more frequent experiences with transfer to adult practices may explain the greater compliance among subspecialists.
Prior research has also emphasized the difficulty of providers’ incorporating guidelines into clinical practice and the importance of evaluating barriers to overcome. 15 Typical barriers to transition include lack of time, lack of resources in the community, and lack of financial incentives.8,9,12,16,17 This survey confirmed the known barriers that need to be overcome.9,12
Overwhelmingly in this survey, difficulty finding adult providers was the primary barrier. Pediatricians report that it is often very difficult to find adult providers who are willing or prepared to accept young adults with special health care needs.8,14 Forty percent of the pediatricians responding to a 2008 survey 9 reported an inability to find an available and/or appropriate adult care provider as the major barrier related to the transition process. Building partnerships and ongoing communication with adult providers can assist with some of the barriers that the pediatric providers encounter.9,12,13 Patient (and family) meeting the new adult-oriented provider(s) prior to transfer from pediatrics is highly recommended. 18
We noticed a modest but not significant trend of those who reported barriers had higher scores on the CS6 and CS11. Although this may be chance findings, those who are more attuned to the guidelines may be more cognizant about the barriers.
Less than 40% of the study respondents addressed legal aspects of transition, core knowledge and skills of the patients, assist in creating a transition or emergency plan, assist with insurance, or have a designated practice member to coordinate transition. Poorly planned health care transitions often result in excessive emergency room visits, unnecessary tests and hospitalizations, 19 loss of insurance, and patients lost to follow-up.19-21 The legal ramifications of becoming an adult must also be considered for YSHCN, as issues of privacy, consent, and advanced directives necessitate attention, as well as guardianship or conservatorship for those with reduced capacity to consent.6,11
Recent initiatives should improve practice and help overcome some of the barriers. Expanded recommendations from the 2011 clinical report 6 combined with tools, resources and learning collaborative information from The National Healthcare Transition Center (also known as “Got Transition?”)12,22 can be used to educate current pediatric and adult providers. Online continuing education modules for both pediatricians and adult providers are another source of educational tools (eg, http://illinoisaap.org/e-learning/). Three national initiatives, the patient-centered medical home, the Affordable Care Act, 1 and accountable care organizations 1 further reinforce this need and encourage effective transitions. 12 As part of the certification requirements of patient-centered medical home, the medical home should provide a smooth transition to adult medical care.6,12,13 The Affordable Care Act recognizes transition as “an essential health home service.” 13 Accountable care organizations encourage a smooth transition by keeping patients within the same health organization and a consistent electronic medical record.12,13 The move toward accountable care organizations may streamline the ease of finding adult providers and improve ongoing communication between adult and pediatric providers. The widespread adoption of electronic medical records may also facilitate communication between providers, particularly when situated within an umbrella organization. 12
Limitations
The survey has selection bias in that it includes only NYS pediatricians who are AAP members. Although low response rates to Web-based clinician surveys are not uncommon, 23 with a response rate of 5%, our results may not be generalizable to all NYS pediatricians or nationally. If the respondents self-selected because they are the providers most invested in the process of transition from adolescence to adulthood, it could mean our results overestimated adherence. In addition, the number of subspecialists who responded to the questionnaire was low, and was not representative of the breadth of subspecialties in pediatrics. On the other hand, despite the limited number of respondents, the geographic distribution of respondents represents the counties of 90% of NYS AAP pediatricians. There are other indications of consistency between the survey respondents and the general AAP NYS populations with regard to age. A higher percentile of females answered the survey compared with the AAP NYS membership (67% vs 59%, P = .04, OR 1.4, 95% CI 1.0-1.95). This may reflect that female clinicians are more likely to answer surveys. 21 Although we observed slight differences in gender ratio between the respondents and the NYS AAP membership, results did not show any difference when adjusting for gender. No information is available about the transition practices or other variables of nonresponders to this survey.
Conclusion and Future Directions
Our study suggests that NYS pediatrician respondents report performing important recommended steps of transition for YSCHNs. More than half of pediatrician respondents are assisting their YSHCNs in the transition process, identifying an adult provider for transfer, creating a portable medical summary, and discussing future goals with the adolescent and family. However, respondents generally start the transition process later than recommended, are not likely to have written transition policies. Although subspecialists respondents report better compliance than generalist none are fully compliant with the 2002 consensus statement recommendations or the eleven essential steps. Identified barriers to the transition process are ongoing and have not been overcome. Education and easily accessible tools and resources for providers may help to increase provider skills and should improve adherence with the complicated process of transition of YSCHN. Continuing medical education is now available in-person, online, and in Webinar, as well as online tools 22 are easily accessible to the pediatrician. The increasing use of the electronic medical record may assist with assessing patient transition readiness measures as well as with communication between pediatric and adult providers.
Needs for future research include further study of the perspectives of adult medical providers, the experiences and outcomes of pre- and posttransition patients and their families, and the differences between generalist and subspecialists in their transitioning challenges and learning needs. By improving the transition from pediatric to adult-oriented care, it may be possible to reduce costs to society and ensure that youth with special health care needs maintain health and become empowered and successful adult consumers of their medical care.
Author Contributions
LFD substantially contributed to the conception and design, contributed to the acquisition, analysis, and interpretation of data, drafted the manuscript, critically revised the manuscript for important intellectual content and agrees to be accountable for all aspects of the work. RC, CL and AR contributed to the design, contributed to analysis and interpretation, critically revised the manuscript, gave final approval and agree to be accountable for all aspects of the work. HWC and PD contributed to analysis and interpretation, critically revised manuscript, gave final approval and agree to be accountable for all aspects of the work.
Footnotes
Acknowledgements
The authors thank all the staff and membership of the New York State American Academy of Pediatrics who participated and supported this study. Special thanks to Jon Lukomnik, Maya Doyle, LCSW-R, PhD, Suzette Oyeku, MD, MPH, Peter F. Belamarich MD, and the CHAM Division of General Pediatrics Investigator Group for their assistance in preparation of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a 2011 Community Access to Child Health (CATCH) Planning Fund Grant, “Pediatrician’s Current Practices—Transitioning to Adulthood.” This publication was supported in part by the CTSA Grant 1 UL1 TR001073-01, 1 TL1 TR001072-01, 1 KL2 TR001071-01 from the National Center for Advancing Translational Sciences (NCATS), a component of the National Institutes of Health (NIH).