
Abstract

Introduction
Respiratory diseases are a very common source of morbidity and mortality among children. 1 In the United States, the rate of pneumonia in children is 20 to 40 cases per 100 000 and pneumococcal pneumonia comprises 20% to 60% of community-acquired cases.2,3 Pleural effusions develop in approximately 40% of children hospitalized with bacterial pneumonia. 4 There has been a decrease in the incidence of bacterial pneumonia. 5 part of it attributed to the debut of the conjugate pneumococcal vaccine. 6 However, rates of parapneumonic effusion (PPE) were noticed to increase5,7-9 In children younger than 2 years, the PPE rate significantly raised in North America from 3.5 cases per 100 000 children in 1996-1998 to 7.0 cases per 100 000 children in 2005-2007. 8 During the same periods, the PPE rate increased from 3.7 to 10.3 cases per 100 000 children between the age 2 and 4 years. 10
In Europe, there was a substantial increase in the incidence of PPE from 1.25 cases per 100 000 persons to 13.65 cases per 100 000 from the period from 2000 to 2012. 11 The overall mean age of children with PPE in developed countries and Southeast Asia is 3 to 6 years. 12
The steps that lead to the development of PPE and empyema are the following: stage 1, also described as the early exudative phase, constitutes the collection of thin reactive fluid and few cells in the pleural space; stage 2, described as the fibropurulent phase, involves the formation of loculations; and stage 3 is the organizing phase and it involves the creation of a thick layer of fibrin that encloses the lung. 13
The management of pleural effusion in children has been a topic of dispute between physicians and surgeons. Many treatment modalities have been suggested and applied, including intravenous antibiotics with or without thoracocentesis, chest drain insertion, intrapleural fibrinolytics, and video-assisted thoracoscopic surgery (VATS). In this review, we detail up-to-date review of pleural effusion in children, including medical and surgical modalities.
Microbiology
The probability to identify an organism in the pleural fluid specimens is low.4,14-20 The British Thoracic Society (BTS) recommends that Gram stain, acid fast bacilli stain, and microbiologic culture be obtained on all pleural fluid samples. 21 In addition, nucleic acid amplification through polymerase chain reaction (PCR) and antigen testing are indispensable tools in the detection of microorganisms in cases with PPE.17,22 In a study conducted in Spain, pneumococci were detected in 79% of culture-positive and 84% of culture-negative samples using real-time PCR; almost 50% were serotype 1. 4 Le Monnier et al 17 found that the sensitivity and specificity of the latex antigen detection in PPE were 90% and 95%, respectively.
It is also recommended to obtain a pleural fluid white blood cell (WBC) count, with cell differential analysis to differentiate between bacterial, mycobacterial and malignancy etiologies. 22
Although different organisms can cause PPE and empyema, Streptococcus pneumoniae is considered to be the most common cause.12,23-29 The effect of age on PPE was not consistent reliable among studies; for instance Ampofo et al found that children affected with complicated pneumococcal pneumonia were older than those with other forms of invasive pneumococcal disease (37 vs 25 months; P < 0.001). 30 In addition, the percentage of complicated pneumococcal pneumonia increased from 26.4% in infants to 53% in children older than 61 months. 31 However, a study conducted in Southeast Asia showed that the highest percentage of PPE among children were in those younger than 4 years. 12
In terms of pneumococcal serotypes, type 1 and 19A displayed strong associations with pneumococcal PPE and empyema worldwide.16,26 In the United States, serotype 3 was the most frequent cause of pneumococcal necrotizing pneumonia and serotype 1 was the most prevalent in uncomplicated pneumococcal pneumonia. 32 In Taiwan, serotypes 14 and 3 were the most common serotypes causing complicated pneumococcal pneumonia. 33 Furthermore, in England, serotypes 1 and 3 were the common serotypes found in children with PPE. 34
Other organisms that cause PPE are methicillin-sensitive Staphylococcus aureus (MSSA),35,36 methicillin-resistant S aureus (MRSA),29,37-39 S pyogenic,19,29,38 Haemophilus influenzae type b,21,40 Mycoplasma pneumoniae, viridians streptococci, and streptococci of Lancefield group F39, 21 Enterobacteriaceae, Klebsiella spp and Pseudomonas aeruginosa, and Yersinia,21,36 Bacteroides species, Peptostreptococcus, 41 Streptococcus milleri,38,41 Fusobacterium necrophorum infection (Lemierre syndrome) in older children,38,43 and Mycobacterium tuberculosis. 21 PPE can be also due to fungal species such as C albicans, C tropicalis, C krusei, C glabrata,44,45 which can sometimes lead to gastrointestinal perforation. 46
Imaging
Chest Radiograph
Chest radiography is usually the first imaging modality in the work up of PPE, but it cannot confirm the diagnosis. Chest radiograph might show early signs of PPE such as obliteration of the costophrenic angle and a meniscus shape area up the lateral chest wall. 47
Ultrasonography
Ultrasonography (U/S) is a safe and inexpensive mode of imaging and can be used to confirm the presence of pleural effusion. 48 In addition, it can be used to guide catheter insertion and percutaneous drainage. 49 Furthermore, U/S can differentiate between pleural and parenchymal involvement, 21 and many clinicians prefer this mode of imaging over computed tomography (CT) for diagnosis.48,50 A lenticular shape might imply the presence of a loculation when using this mode of imaging. 47 The efficacy and safety of the U/S were reported in 2 large studies indicating that PPE can be managed properly without the use of chest CT.51,52 However, U/S is inferior to CT of chest in detecting loculated effusions in the mediastinal area and in the fissures. 53
Computed Tomography
A CT scan is not indicated for the initial diagnosis and management of uncomplicated PPE.48,50 A CT scan of the chest is warranted in complicated cases of PPE because it can detect lung pathology and pulmonary abscess 54 and it is also recommended in preoperative cases of PPE.21,22
However, the disadvantages of chest CT are the exposure of a patient to relatively high radiation, 53 the inability to visualize thin pleural septations or fibrin, 55 and the possibility of the need for sedation. 53
Diagnostic Tap
If the health care provider suspects that the effusion is not of infectious etiology, then it will be recommended to perform a diagnostic tap for cytological analysis before chest drain insertion to avoid complications associated with anaesthesia, surgery or sedation. 21
Biochemistry/Microscopy
Fluid from bacterial infections, and sometimes tuberculosis, are predominantly neutrophils while lymphocytosis is detected in autoimmune diseases, tuberculosis, chylothorax, and malignancy; moreover, turbid indicates high cell count or high lipid content. 53
Serous fluids are categorized into transudates and exudates. Transudative effusion usually refers to a noninflammatory process (alteration of hydrostatic or colloid osmotic pressure), where it infers from ultrafiltration process across a membrane and it is usually low in protein. On the other hand, exudates refer to an inflammation or inflammatory process, where it infers capillary permeability. 21 A pleural fluid:serum protein ratio greater than 0.5, a pleural fluid lactate dehydrogenase activity greater than 200 U/L, or a pleural fuid:serum lactate dehydrogenase ratio greater than 0.6 is usually diagnostic of exudative effusion. 56 However, the BTS states that pleural fluid parameters, such as glucose, protein, lactate dehydrogenase levels, and pH are not recommended since they do not change the management of PPE. 21
Management
Prevention
The preferred treatment of PPE is prevention via up-to-date immunization. 53
Antibiotics Use
Many practitioners opt for antibiotics alone when managing a small PPE in patients with no respiratory distress; although it is an acceptable option, further intervention must be followed if the effusion is enlarging or patient is deteriorating.5,21
The initial treatment of all pleural effusion should be the use of antibiotics. For children with small effusions (<10 mm on lateral decubitus chest radiograph or opacification of less than one-fourth of the hemithorax), the choice of broad-spectrum antibiotics, chest radiographs, and good clinical exam should suffice on an outpatient basis. 22
Children with larger pleural effusion should be hospitalized and the use of intravenous antibiotics is warranted. 21
Intravenous cefotaxime or ceftriaxone could be used as empiric treatment until cultures results are known. Clindamycin or vancomycin could be added if community-acquired MRSA is suspected. 22 The current practice of first-line empiric treatment of antibiotics is cefotaxime plus vancomycin because of the increased prevalence of drug resistant organisms. 57
Physicians’ adequate awareness of most common causes of community acquired pneumonia in their communities is crucial in selecting the initial antibiotic empiric treatment; for instance, ampicillin or penicillin G might also be considered as first-line drugs in fully immunized children in areas where local penicillin resistance in invasive strains of pneumococcus is uncommon. 22
Prior to the discovery of antibiotics, S pneumoniae was the common organism found in the pleural fluid, followed by S pyogenes and S aureus 21 ; penicillin-resistant S aureus eventually emerged after the introduction of antibiotics.21,25
Two independent studies showed that all pneumococcal serotype 1 isolates were penicillin susceptible in children with PPE.16,25 However, 70% of serotype 14 isolates were penicillin resistant. 25 Furthermore, the Centers for Disease Control and Prevention reported an increased number of cases in children caused by antimicrobial resistance pneumococcal serotype (19A) in the United States. 58 Other studies showed also that serotype 19A is related with decreased sensitivity to antibiotics; for instance, Lai et al 59 found in a study conducted in Taiwan that serotype 19A isolates from pediatric PPE had lower levels of susceptibility to cefotaxime than non-19A isolates. Analogous results were reported in Spain, where 11% of cases of pediatric PPE were caused by serotype 19A isolates and were nonsusceptible to cefotaxime. 26
For patients allergic to penicillin, clindamycin is a reasonable option or meropenem if no improvement is observed. 60
The selection of antibiotics should be tailored per patient populations; children with risk of aspiration, coverage of anaerobes is recommended; moreover, coverage of Gram-negative organisms in children with PPE due to nosocomial infection is also indicated. 57
The spectrum of antibiotics is narrowed per pleural fluid culture results; however, in culture-negative PPE, continuation of the initial blind antibiotic treatment is recommended, especially if the patient is clinically improving. 60 The duration of treatment differs among practitioners, but the majority of medical centers maintain the ill child on intravenous antibiotics until the patient is afebrile or when the chest tube is removed. Usually, amoxicillin–clavulanic acid is given at discharge for 1 to 4 weeks, but definitely longer if needed. 21
Amphotericin-B, fluconazole, and voricanazole are the agents commonly used to treat fungal PPE. 44 As far as M tuberculosis is concerned, treatment is warranted only if the index of suspicion is high. 21
Thoracocentesis and Chest Tube
Thoracocentesis is recommended for small PPE in older children and it can guide the physician toward the appropriate antibiotic use; however, if repeated thoracocentesis is required, then chest tube will be the better choice. 21 Small tubes (8-12 French) are reported as good as larger tubes. 53 However, Shoseyov et al 61 revealed in their study that there is no difference between repeated ultrasound-guided needle thoracocentesis (RUSGT) and chest tube insertion in terms of mean duration of temperature, mean fluid drained, duration of antibiotic use, and duration of hospitalization stay.
The indications for chest tube drainage as recommended by the Pediatric Infectious Diseases Society (PIDS) and the Infectious Diseases Society of America 22 are as follows:
There is no indication for chest tube insertion in pleural effusion less than 10 mm on a lateral decubitus radiograph or if the opacification constitutes less than one-fourth of the hemithorax.
There is no indication for chest tube insertion in pleural effusion if there is more than 10 mm of fluids but the opacification constitutes less than half of the hemithorax, the effusion is not consistent with empyema and if the patient is not in respiratory distress.
A chest tube is indicated in opacities larger than half of the hemithorax and with quantity of fluids of more than 10 mm and consistent with empyema in children with respiratory distress.
The insertion of a chest tube should also be considered if a patient fails to respond despite 48 to 72 hours of antibiotic therapy, hypoxia, hepercapnia, large amounts of free-flowing pleural fluid and if there is evidence of fibropurulent effusions (pH <7.0, glucose <40 mg/dL [2.22 mmol/L], lactate dehydrogenase >1000 IU [16.67 kat/L]. 57
Fribrinolytics
The use of intrapleural fibrinolytics has been in use globally with success for the management of PPE and empyema. Its use improves drainage without systemic fibrinolysis or hemorrhage, and the global success ranges from 44% to 100%. 62
The American Pediatric Surgical Association and the BTS recommend fibrinolytic therapy as a part of the medical option for patients with thick or loculated pleural fluid.21,63
Several studies have shown that fibrinolytics are preferable over chest tube alone in the management of PPE in children.42,64-70
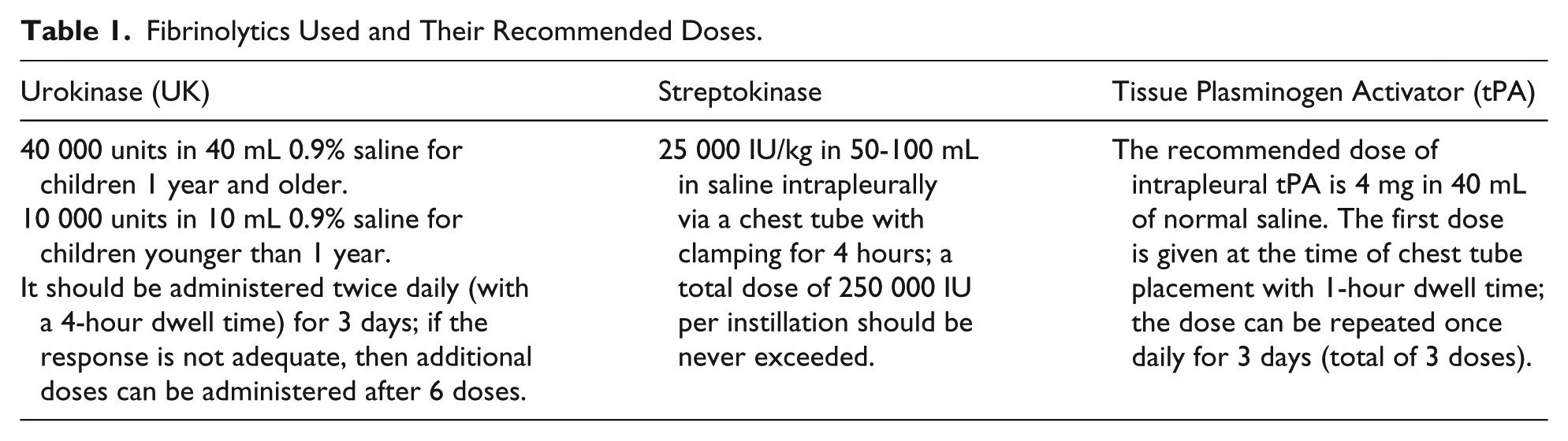
The 3 fibrinolytics that have been in use are streptokinase, urokinase, and tissue plasminogen activator (tPA) (Table 1). 71
Fibrinolytics Used and Their Recommended Doses.
Urokinase
Urokinase is a fibrinolytic agent that specifically catalyzes the cleavage of the arginine–valine bond in plasminogen 72 .
BTS 21 and PIDS 22 recommend the usage of urokinase as follows: 40 000 units in 40 mL 0.9% saline for children 1 year and older, and 10 000 units in 10 mL 0.9% saline for children younger than 1 year. This dose should be administered twice daily (with a 4-hour dwell time) for 3 days; if the response is not adequate, then additional doses can be administered after 6 doses. Intrapleural bupivacaine (0.5-1.0 mL/kg of a 0.25% solution) can be used for pain control.
A multicenter randomized placebo-controlled trial involving children with PPE, 42 showed that the length of hospital stay was shorter with the use of UK compared with patients in whom normal saline was administered alone. Stefanutti et al 73 also supported the use of UK and their study showed that intrapleural UK has been shown to be effective in the treatment of PPE in children.
Streptokinase
Streptokinase has same mechanism of action of UK; however, it is of bacterial origin rather than a recombinant human enzyme. 73 The recommended dose is 25 000 IU/kg in 50 to 100 mL in saline intrapleurally via a chest tube with clamping for 4 hours; a total dose of 250 000 IU per instillation should be never exceeded. 69
A study published by Yao et al 65 showed that intrapleural fibrinolytic treatment with streptokinase is safe and effective and it can avert the need for surgery in most cases; safety was measured by the lack of major side effects after streptokinase instillation while efficacy was measured by pleural fluid drainage of 4-fold higher compared to the control group. 65
Since streptokinase is of bacterial origin, possible side effects are fever, allergic reactions, and anti-streptokinase antibody production. 74
Tissue Plasminogen Activator
Tissue plasminogen activator binds to fibrin in a thrombus then converts the entrapped plasminogen to plasmin, and finally initiates local fibrinolysis. The half-life of tPA in the serum is 4 to 6 minutes, but can be prolonged when alteplase is bound to fibrin in a clot; the instillation of intrapleural tPA usually does not lead to plasma pharmacologic concentrations. 75
The recommended dose of intrapleural tPA is 4 mg in 40 mL of normal saline. The first dose is given at the time of chest tube placement with 1-hour dwell time; the dose can be repeated once daily for 3 days (total of 3 doses). 57
A study conducted at the Hospital for Sick Children in Toronto, Ontario, Canada, showed that intrapleural tPA led to a higher pleural fluid drainage compared to normal saline (691 vs 360 mL); the duration of chest tube placement was 84 hours for the early administration of intrapleural tPA group compared with 130 hours for the control group. The authors did not report local or systemic bleeding after intrapleural tPA administration. 76
Deoxyribonuclease
Deoxyribonuclease (DNase) is a mucolytic agent that enhances the performance of pleural space debridement. 77 Light et al 78 studied the effectiveness of streptokinase, urokinase, and varidase (the combination of streptokinase and streptodornase) on pleural drainage and found that DNase in conjunction with streptokinase, was superior compared with either UK or streptokinase alone. 78 Moreover, Zhu et al 79 found that DNase in conjunction to tPA was superior to saline, tPA, or DNase alone. Furthermore, Rahman et al 80 concluded in their prospective study that intrapleural combination of tPA and DNase therapy improved fluid drainage in patients with pleural infection and reduced the duration of the hospital stay and frequency of surgical referral. 80
So Which Fibrinolytic to Use?
The efficacy of fibrinolytics use can reach 90%. 81 UK and streptokinase have the same effectiveness in treating PPE and empyemas. 62
Urokinase is preferred over streptokinase because of its lower allergenic risk, but it is more expensive. 73 UK and tPA were compared in a retrospective review study that included 71 children with PPE. The study concluded that primary management achievement was 98% for alteplase and 100% for UK, with no reported major complications. However, tPA was superior to UK in terms of pleural drainage in the first 2 days of fibrinolytic therapy. 82
No randomized control trials comparing the effectiveness of streptokinase and tPA in the management of PPE in children were allocated in the literature review.
Video-Assisted Thoracic Surgery
Some pediatric surgeons consider primary surgical intervention as the best mode of managing PPE. 83 However; literature does not fully support their approach. 13
It is warranted to consult pediatric surgeons if there is failure of chest tube drainage, antibiotics and fibrinolytics; moreover, surgical approach is indicated with persisting sepsis in combination with PPE despite the use of antibiotics and insertion of a chest tube. Furthermore, surgery is required in cases of empyema with significant lung pathology, bronchopleural fistula with pyopneumothorax, and secondary empyema. 21
The benefits of VATS are drainage of purulent material, decortications of the fibropurulent septa, irrigation of the pleural cavity and visualization of the evacuation to allow reexpansion of the lung. 84
Fibrinolytics Versus Video-Assisted Thoracic Surgery
A study conducted by Kilic et al 64 suggested that the use of intrapleural fibrinolytics is an effective and safe in children with thoracic empyema and can obviate a thoracotomy in most cases. In a different study, 60 children were randomized to receive either percutaneous chest drain with intrapleural UK or VATS; the authors concluded that treatment with UK is better economically, while no difference in clinical outcome between the 2 groups was noted. 85 In addition St. Peter et al 86 concluded that there was no difference in days of hospitalization after intervention, days of oxygen requirement, and days until afebrile or analgesic requirements in hospitalized patients with PPE. In addition, Faber et al 87 echoed the effectiveness of the nonoperative approach. The study evaluated 75 pediatric empyema cases and it showed that nonoperated children were admitted to the pediatric intensive care unit less frequently than those who were operated and there was no significant statistical difference in overall hospitalization.
On the other hand, Cohen et al 83 conducted a systematic review that showed the superiority of primary operative therapy compared with nonoperative approaches. Operative management was associated with a lower mortality rate, lower reintervention rate, shorter length of hospitalization, decreased time with a thoracostomy tube, and shorter course of antibiotic therapy, compared with nonoperative therapy. A Cochrane Systematic Review on surgical versus nonsurgical management of pleural empyema conducted by Coote et al 88 was also in favor of the operative approach showing that the surgical group had higher primary treatment success. In addition, the study showed that all streptokinase medical failures required VATS and surgical patients had shorter hospital stay. Moreover, in a large study, Shah et al 89 included 3500 patients with pleural effusion that underwent different procedures: chest tube without fibrinolysis (n = 1762), chest tube with fibrinolysis (n = 623), VATS (n = 408), and thoracotomy (n = 797). The study concluded that length of stay was similar in patients that underwent VATS and chest tube insertion with or without fibrinolysis.
Outcome and Prognosis
Children with pleural effusion usually do well and their lung functions return to normal in the majority of children regardless of the management mode of pleural effusion. 39
Follow-up
Children with pleural effusion should have a follow-up within 4 to 6 weeks of hospital discharge depending on the child’s clinical status at discharge; chest radiography findings are abnormal at discharge, and a radiograph should be obtained at 4 to 6 weeks. 21 Complete radiological resolution is usually expected by 3 to 6 months.62,90
Summary and Recommendations
A conscientious path must be followed when managing a case of PPE in children. The severity of the case and the progress of the disease usually dictate the approach. It is therefore, prudent not to rush into invasive procedures for children.
Antibiotics Use
All infants and children with pleural effusion should be initiated on broad-spectrum antibiotics. If the organism is known, then narrowing the antibiotic spectrum is recommended. If the patient is hospitalized, then intravenous antibiotics should be continued until the child is afebrile.
Oral antibiotics such as amoxicillin–clavulanic acid are then given at discharge for 1 to 4 weeks, but longer if there is residual disease.
For atypical cases such as nonbacterial pleural effusion or suspected tuberculosis, a consultation with the specialist will be warranted.
Imaging
Imaging studies can guide the decision for intervention in PPE. A plain chest film should be the initial imaging test. A lateral/decubitus view might help in the diagnosis. Chest ultrasound will confirm the pleural fluid and might show loculations. Chest CT should be reserved for the complicated or doubtful cases to avoid unnecessary radiation exposure.
Chest Tube
Chest tube is definitely indicated in opacities larger than half of the hemithorax and with quantity of fluids of more than 10 mm in children with respiratory distress and fluid consistent with empyema.
Fibrinolytics
Intrapleural administration of fibrinolytics is an effective treatment for complicated parapneumonic effusions and pleural empyemas (pleural effusion is thick or loculated).
Any of the 3 fibrinolytics can be used (UK, streptokinase, and alteplase); however, UK is the most studied among the 3 options and is probably the preferred agent if available.
Video-Assisted Thoracic Surgery
Video-assisted thoracic surgery should be contemplated in ill children with a persistent pleural collection, despite antibiotics use, chest tube drainage, and fibrinolytics therapy.
Follow-up
Children with pleural effusion or empyema should be seen for follow up within 4 to 6 weeks of discharge. Chest radiographs are usually abnormal at discharge, and a radiograph should be obtained after 4 to 6 weeks.
Limitations
Our article portrays a comprehensive review of pleural effusion in children, especially the management options. However, our limitation was the inability to conduct a meta-analysis; this is mostly attributed to the lack of published articles comparing different modes of management of pleural effusion in children.
Author’s Contribution
MAH designed the manuscript,searched for articles, reviewed the literature, wrote the first draft and approved the final version.
IAJ assisted in writing the manuscript, provided expert opinion, criticality reviewed the manuscript and approved the final version.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.