
Abstract

Case Report
A previously healthy and fully vaccinated 5-year-old girl presented in October 2018 with 19 days of fever, bitemporal headaches, fatigue, 6-pound weight loss, and recent diagnosis of streptococcal pharyngitis. Her fevers occurred daily, primarily in the afternoons and early evenings, and temperature measured orally as high as 104°F. The patient’s review of systems was negative for sore throat, oral ulcers, rashes, arthralgia, gastrointestinal symptoms, or lymphadenopathy. Her family history was significant for a grandmother with rheumatoid arthritis. Her exposure history was notable for exposure to cows, unvaccinated cats, and mosquitos. She had no history of recent travel.
Patient’s vital signs on admission were within normal limits, and she was afebrile throughout admission. Physical examination was normal, with pertinent negatives including no lymphadenopathy, hepatosplenomegaly, or rash. On the second day of hospitalization, the patient developed left-sided facial droop consistent with Bell’s palsy (Figure 1).
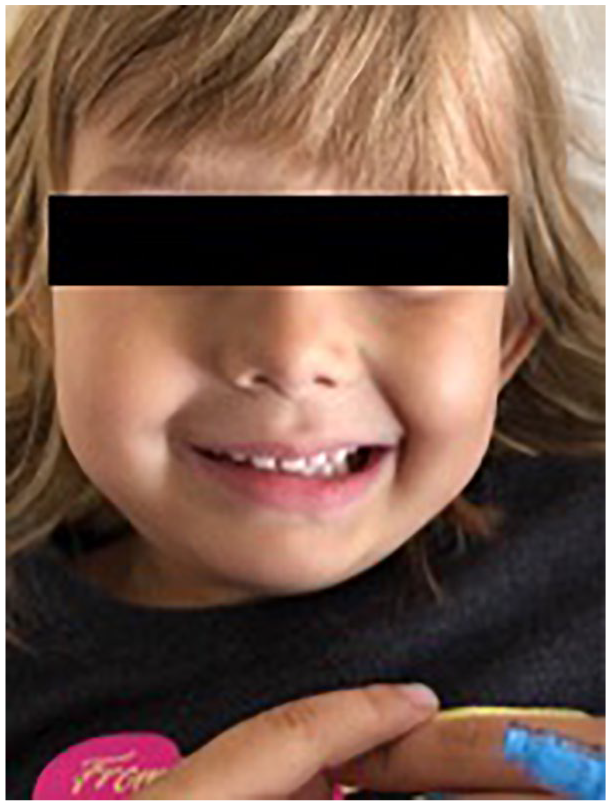
Left-sided facial droop.
Diagnostic evaluation was notable for an elevated C-reactive protein of 8.1 mg/dL (reference range, <1.0 mg/dL) and erythrocyte sedimentation rate of 70 mm/h (reference range, 0-20 mm/h). Blood cultures remained negative. To evaluate the patient’s new facial droop, she underwent computed tomography head scan without contrast, which demonstrated no acute intracranial process. Infectious Diseases was consulted and recommended additional serologic and polymerase chain reaction testing for bacterial and viral pathogens (including for Rickettsial infection, Lyme disease, West Nile virus, varicella, mumps, Epstein-Barr virus, cytomegalovirus, and herpes simplex viruses 1 and 2), high-resolution abdominal ultrasound, and a dilated ophthalmologic examination. An abdominal ultrasound was notable for multiple subcentimeter hypoechoic lesions throughout her liver and spleen, consistent with disseminated cat scratch disease (CSD; Figure 2).

Hepatic lesions seen on abdominal ultrasound.
Final Diagnosis
Disseminated cat scratch disease.
Hospital Course
Given the concern for disseminated CSD and the patient’s neurological findings of facial nerve palsy, both Ophthalmology and Otolaryngology teams were consulted. Ophthalmologic examination was negative for neuroretinitis. Otolaryngology was consulted to evaluate the patient’s parotid glands for possible granulomas adjacent to her facial nerve, which could contribute to her new facial nerve palsy. Magnetic resonance imaging brain was negative for parotid granulomas around the facial nerve. Due to the clinical suspicion for CSD, treatment with azithromycin and rifampin was initiated for a 14-day course, after which the patient had resolution of fevers and facial nerve palsy. After discharge, Bartonella henselae immunoglobulin M and immunoglobulin G both resulted as positive at 1:256.
Discussion
This case consists of a 5-year-old girl with almost 3 weeks of fever with associated fatigue, headaches, 6-pound weight loss, and late-onset left-sided facial palsy. Her initial presentation was consistent with fever of unknown origin (FUO) due to the length and severity of her fevers, in the absence of a diagnosis after initial evaluation. A broad differential for underlying etiologies must be considered when presented with FUO as an initial complaint, but infectious causes make up the majority of identifiable etiologies. A prospective study of pediatric FUO showed that bartonellosis was responsible for 10.4% of all FUO pediatric cases. 1
The most common presentation of CSD is cutaneous inoculation from a feline carrier, followed by a primary inoculation lesion with subsequent development of proximal lymphadenopathy over the course of 2 or more weeks. About 85% of cases include lymphadenopathy, although only 60% of cases have an identified inoculation lesion, 2 perhaps because the lesion is not noticed by patients or because disease was transmitted through fleas or mucous membrane contact with cat saliva. As imaging is not routine, the incidence of hepatosplenic lesions is unknown; however, roughly 12% of patients have notable splenomegaly, and these patients frequently lack peripheral lymphadenopathy. 2 Our patient had no identified inoculation site, had no regional lymphadenopathy, had hepatosplenic involvement, and later developed facial nerve palsy.
The presence of facial nerve involvement is highly unusual for Bartonella infection. We were able to identify 6 prior cases,3-8 of which only 4 were in pediatric patients. Three of these were associated with Parinaud syndrome, regional lymphadenopathy, parotitis, or granuloma formation causing a direct mass effect on the nerve. Only one case has been described in a pediatric patient without parotid involvement or granuloma formation. 3 Our patient stands out for the absence of focal findings to suggest mass effect on the facial nerve with normal imaging of the region. This case opens the question of the mechanism of facial nerve palsy in these patients. If not due to direct mass-effect, then the facial nerve palsy may be mediated by a vasculitis, which has been suggested as the cause of encephalitis in rare cases. 9
The treatment of Bartonella infection is not formalized and varies, depending on the specific symptoms. Our patient had hepatosplenic lesions and received a course of rifampin and azithromycin, which are individually supported by case series in children for disseminated Bartonella. 10 Developing more formalized therapies for Bartonella infection has been stymied by the fact that in vitro sensitivities often do not match observed in vivo efficacy for this organism, likely due to its culture requirements and intracellular pathogenesis. To our knowledge, azithromycin and rifampin have not been specifically evaluated in combination in the pediatric population for this severity of disease, though our patient recovered quickly after beginning therapy.
Conclusion
Our patient represents an atypical case of FUO caused by disseminated Bartonella henselae infection associated with late-onset facial nerve palsy. The finding of facial nerve palsy is highly novel, particularly in the absence of granulomas or parotid involvement, suggesting that other mechanisms of pathogenesis may be relevant. The types of clinical disease caused by Bartonella henselae are broad, and this organism is likely to become more frequently recognized as culture and molecular techniques advance. Further study of the spectrum of disease attributable to this organism as well as additional evaluation of treatment regimens is warranted.
Author Contributions
CPM and RDK drafted the manuscript and conducted literature search. CPM, RDK, DMF, VR, and GJD critically revised the manuscript. All authors gave final approval and agree to be held accountable for all aspects of the work’s integrity.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient’s legal guardian for patient information and images to be published prior to manuscript preparation.