
Abstract

Case Report
A male infant was born to a 33-year-old gravida 5, para 4 mother with depression, anemia, asthma, nicotine dependence, and a 14-year history of phencyclidine (PCP) abuse. Prescribed prenatal medications included sertraline and ferrous sulfate. The mother reported near daily use of PCP while pregnant, as recently as 2 days prior to delivery. She denied use of other illegal drugs. Maternal urine drug screen at delivery was positive only for PCP. There was scant prenatal care, but prenatal laboratory results were unremarkable and there was no intrauterine growth restriction. Paternal history was unknown.
The infant was delivered by repeat caesarean at 41 weeks. The delivery was complicated by meconium and late placental abruption. Resuscitation was routine, with Apgar scores of 8 and 9. Physical examination revealed a birth weight of 3845 g (84th percentile), length of 52 cm (87th percentile), and head circumference of 35.5 cm (79th percentile). No facial dysmorphism or abnormalities were noted. At 10 minutes of life, the infant developed respiratory distress requiring continuous positive airway pressure and was admitted to the neonatal intensive care unit (NICU). He was weaned to room air and required no further respiratory support by 22 hours of life. However, he could not be discharged from the NICU secondary to feeding issues.
The NICU team attempted to allow him to PO (per os) ad lib, but he was noted to have limited interest in feeds and poor suck and swallow coordination. Despite being term, nasogastric feeds were initiated by day of life (DOL) 3 for persistent poor oral intake. Concurrently, the infant began to exhibit various neurological symptoms: irritability, central hypotonia, peripheral hypertonicity, and brisk (3/4) deep tendon reflexes (DTRs). He had no tremors, vomiting, diarrhea, or vital sign abnormalities. He developed opsoclonus on DOL 3 (Figure 1). His constellation of symptoms prompted Toxicology, Neurology, and Ophthalmology evaluations.

Image of initial abnormal eye movements.
Head ultrasound on DOL 4 was normal with no ventriculomegaly or intracranial hemorrhage. Brain magnetic resonance imaging on DOL 7 was complicated by motion artifact and prominent deep cerebral medullary veins suggesting venous congestion, but demonstrated no areas of abnormal parenchymal signal intensity. Routine electroencephalogram on DOL 5 was normal with no abnormalities correlating with abnormal eye movements. Audiology and newborn screening were normal. Urine VMA/HVA (vanillylmandelic acid/homovanillic acid) testing was negative on DOL 5. Urine testing was positive for PCP on DOL 0, 1, and 5. Ophthalmology suggested a differential of drug-related exposure versus congenital idiopathic motor nystagmus given a normal structural eye examination with nystagmus in the setting of a normal brain magnetic resonance imaging.
Phenobarbital was started on DOL 12, as the infant continued to have poor oral feeding, and PCP exposure was the suspected etiology. Based on case reports, a loading dose of 10 mg/kg followed by a maintenance dose of 4 mg/kg/day was used to treat the neurological symptoms and feeding difficulties.1,2 The infant completed a 26-day course of phenobarbital without any significant change in his examination or feeding abilities, so phenobarbital was weaned starting on DOL 39 and discontinued by DOL 42.
The infant ultimately underwent G-tube placement on DOL 47 given persistent failure of oral intake despite consistent speech therapy, phenobarbital treatment, and time. He was discharged from the NICU with follow-up including Neurology, Ophthalmology, Nutrition, Gastroenterology, General Pediatrics, and Developmental Pediatrics. As an outpatient, the infant was only taking minimal formula by mouth at age 2 months, but by 3 months of age, he had begun to take increasing amounts orally. He was able to take goal feeding volume by mouth over an hour at 4 months of age. However, in the setting of slow weight gain, continued G-tube use and limiting oral feeding to 30 minutes was recommended by gastroenterology. The infant demonstrated coordinated sucking without coughing or choking when evaluated by a speech-language pathologist at that time.
The infant’s neurological status also improved over time, with jitteriness and hypertonicity resolving by 2 months of age, although he continued to have mild nystagmus. By 3 months of age, he had a reassuring ophthalmologic examination, with pseudostrabismus, age-appropriate hyperopia, and no nystagmus. The infant had an age-appropriate neurological examination when evaluated by neurology at 4 months of age, including 2+ DTRs bilaterally in upper and lower extremities and appropriate tone. During evaluation in the Neonatal Follow-up Program at 4 months, the infant was found to be developmentally on track for his chronological age. He was competent in all 5 domains of the Bayley Screener, third Edition.
Final Diagnosis
Prenatal PCP exposure.
Discussion
Phencyclidine, also known as “angel dust,” is a hallucinogen commonly used for its dissociative effects. 3 While use peaked in the 1970s, PCP remains a present and increasingly popular drug of abuse. In the United States, 6.1 million (2.2%) individuals aged 12 years and older reported using PCP in their lifetime and 96 000 reported using PCP within the past month. 4 PCP is known to cross the placenta, and due to its lipophilicity, abuse during pregnancy can result in prolonged exposure of the developing fetal brain to its negative effects.5-7 Providers caring for neonates exposed to PCP in utero should be aware that it is associated with short-term and long-term side effects. This case highlights feeding difficulties, neurological and ocular findings, the limitations of symptomatic treatment, and the necessity of multidisciplinary care.
Few articles examine infant feeding in PCP-exposed neonates, and to our knowledge, long-term oral feeding intolerance has never been described. Several reports note short-term gastrointestinal symptoms associated with in utero PCP exposure, although the reported frequency of these symptoms varies widely (Table 1).1,2,8-11 In one case report, a late-preterm PCP-exposed infant required readmission to the hospital on DOL 34 due to poor feeding, weight loss, respiratory distress, and persistent jaundice. The infant gained weight and was discharged after 25 days, although feeding details were not described. 10 In the present case, it is unclear whether the feeding difficulties were acute PCP intoxication, withdrawal, or a sequelae of prenatal PCP exposure. Given that oral feeding difficulties persist even at 4 months of age, it seems more likely a sequelae of prenatal PCP exposure rather than intoxication or withdrawal. Our case emphasizes the importance of long-term monitoring of oral feeding and growth in infants exposed to PCP prenatally.
Clinical Features of Infants Exposed Prenatally to PCP a .
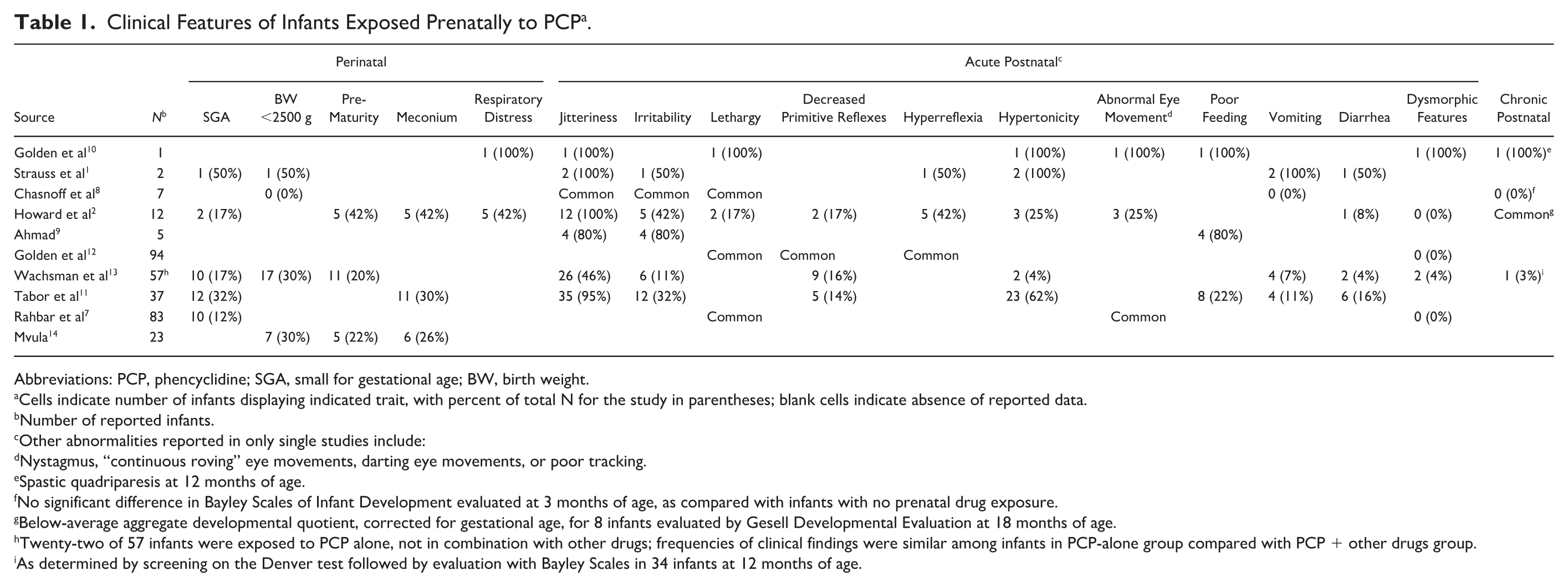
Abbreviations: PCP, phencyclidine; SGA, small for gestational age; BW, birth weight.
Cells indicate number of infants displaying indicated trait, with percent of total N for the study in parentheses; blank cells indicate absence of reported data.
Number of reported infants.
Other abnormalities reported in only single studies include:
Nystagmus, “continuous roving” eye movements, darting eye movements, or poor tracking.
Spastic quadriparesis at 12 months of age.
No significant difference in Bayley Scales of Infant Development evaluated at 3 months of age, as compared with infants with no prenatal drug exposure.
Below-average aggregate developmental quotient, corrected for gestational age, for 8 infants evaluated by Gesell Developmental Evaluation at 18 months of age.
Twenty-two of 57 infants were exposed to PCP alone, not in combination with other drugs; frequencies of clinical findings were similar among infants in PCP-alone group compared with PCP + other drugs group.
As determined by screening on the Denver test followed by evaluation with Bayley Scales in 34 infants at 12 months of age.
Common neurobehavioral symptoms in infants exposed to PCP, including jitteriness, irritability, and hypertonicity, have been widely reported in both case reports and larger studies (Table 1).1,2,7-11 Abnormal eye movements are commonly reported in PCP-exposed infants but are not well characterized in the literature. 3 Golden et al described an infant with nystagmus and poor visual tracking who continued to have roving eye movements at 2 months of age. 10 In a case series of 12 neonates exposed to PCP, 25% had bizarre eye movements and staring spells, although the exact nature of the eye movements was not described. 2 The infant in our case had abnormal eye movements, characterized initially as opsoclonus and later as horizontal pendular nystagmus, that developed on DOL 3 and resolved by 3 months of age.
There is limited evidence regarding the best treatment for symptoms of in utero neonatal PCP exposure. Strauss et al discussed 2 cases in which phenobarbital was given as treatment for jitteriness, hypertonicity, diarrhea, and emesis. In the first case, the infant continued to have jitteriness and hypertonicity, but the diarrhea subsided. In the second case, the infant continued to have fine tremors on stimulation. 1 In a 12-infant case series, 58% required symptomatic treatment for 2 to 14 days with diazepam, phenobarbital, or paregoric to treat neurobehavioral symptoms. The number of infants treated with each specific drug was not detailed, nor was treatment effect. 2 In the present case, treatment with phenobarbital for 26 days was associated with partial improvement in hypertonicity, but had no effect on nystagmus or oral feeding skills.
Given the limited literature on management of symptoms in the PCP-exposed neonate, a multidisciplinary team was consulted including Toxicology, Neurology, Ophthalmology, Pharmacy, Gastroenterology, Nutrition, and Speech therapy to discuss management, treatment options, and rule out other possible diagnoses (including seizures and neuroblastoma). A major clinical challenge was distinguishing whether the infant’s symptoms were due to acute PCP toxicity versus PCP withdrawal versus long-term effects of prolonged in utero PCP exposure. The persistence of his feeding and ocular abnormalities beyond the neonatal period suggests potential long-term neurodevelopmental sequelae of in utero PCP exposure, making outpatient follow-up with multiple subspecialty services, including developmental pediatrics, essential. Previous studies suggest that developmental outcomes of infants exposed to PCP in utero are similar to nonexposed controls.8,13 The infant described in our case was also found to be developmentally on track at 4 months chronological age, although further follow-up is needed. He also had resolution of short-term neurologic and ocular symptoms with time. While the infant still relies on a G-tube for adequate nutrition, he continues to improve. He has ongoing follow-up with the Neonatal Follow-up Program, gastroenterology, speech therapy, and nutrition.
Conclusion
Pediatricians should be aware of possible short-term and long-term side effects of PCP exposure in utero. This case highlights the importance of long-term monitoring of oral feeding and growth in infants exposed to PCP prenatally. It also demonstrates the necessity of longitudinal follow-up by a multidisciplinary team.
Author Contributions
All authors have met and treated the patient. Drs Flynn, Hill, and Rood drafted the initial manuscript. All authors reviewed and revised the manuscript. All authors have read and approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The authors received written informed consent for patient information and images to be published provided by the patient’s legally authorized representative.