
Abstract
Background
Children affected by the novel human coronavirus, severe acute respiratory syndrome-coronavirus disease-2019 (SARS-CoV-2, causing the COVID-19 [coronavirus disease-2019] pandemic) have been reported to have concurrent or postinfectious disorders of both the central and peripheral nervous systems 1 . Examples of central nervous system disorders associated with COVID-19 in children include headache, seizure, cerebral edema, demyelination, and ischemic or hemorrhagic stroke1-3. While certain case series have noted the increased incidence of stroke in adults (21% increased risk of any thromboembolic events, with a 2.5% increased risk of ischemic stroke) affected by COVID-19, there are limited data in children4-6. To some extent this may be due to baseline variation in the prevalence of stroke in children compared with adults.
Aims
The primary aim of this study was to compare the incidence of stroke in a tertiary care children’s hospital between January and December 2020 (pandemic) with a similar period in 2019 (pre-pandemic).
Our secondary aims were to characterize the demographic, clinical characteristics of affected children, nature of the stroke (arterial ischemic vs venous sinus thrombosis vs hemorrhagic), vascular territory affected (anterior circulation vs posterior circulation), and outcomes in the 2 groups.
Materials and Methods
We conducted a retrospective chart review of children ≤18 years of age who were presented to a tertiary care children’s hospital between January and December 2020 and compared the incidence, demographics, and stroke characteristics to the same time period in 2019 (pre-pandemic). Study patients were identified using 2 sources:
Stroke pager activation and evidence of stroke on neuroimaging that was confirmed by both neuroradiologist and pediatric neurologist on call.
Discharge ICD (International Classification of Diseases)-10 diagnoses for acute cerebral infarction, acute ischemic stroke, embolic stroke, cerebral sinus thrombosis, and hemorrhagic stroke (and subgroups thereof).
The latter method was used to capture those patients in whom the stroke pager was not activated. Our hospital utilizes a stroke protocol that can be activated both in the emergency department and inpatient units when a stroke is suspected. This allows a team consisting of a pediatric neurologist, anesthesiologist, radiologist, and hematologist to be notified simultaneously and allows for rapid mobilization of resources 7 . The protocol allows for the performance of computed tomography (CT) scan of the head followed by rapid sequence magnetic resonance imaging (MRI) if no hemorrhage is identified on CT. Rapid sequence MRI consists of diffusion-weighted images, apparent diffusion coefficient, and fluid attenuated inversion recovery sequences (DWI, ADC, and FLAIR). Children with a positive rapid sequence MRI subsequently undergo full sequence MRI, magnetic resonance angiogram, and magnetic resonance venogram of the head and neck. CT angiograms of the head and neck are performed on an individual basis as indicated by results of neuroimaging and the nature of the stroke.
The following study variables were abstracted into a standardized data collection form on REDCap (Research Electronic Data Capture) by the primary investigator: patient demographics, history of previous stroke, risk factors for stroke, presenting symptoms, neurologic examination including National Institute of Health Stroke Scale (NIHSS), laboratory tests including hypercoagulability workup, results of neuroimaging, interventions, details regarding treatment, and immediate outcomes 8 . For those patients who presented during the pandemic, additional data collected included exposure to SARS-CoV-2, signs symptoms and treatment of COVID-19 disease if applicable, and type of SARS-CoV2 testing that was performed (RT-PCR [reverse transcription polymerase chain reaction], IgG [immunoglobulin G], or both) with results. This study was approved as an exempt protocol by our institutional review board under study number 2021-514.
Statistical Analysis
Data variables were systematically coded and entered into the REDCap database by the study primary investigator. Demographic and clinical variables were compared between pre-pandemic and pandemic periods using nonparametric univariate procedures 8 . Variables that were categorically scaled were compared between study group periods using a nonparametric Fisher’s exact test. Variables continuously scaled were compared using a Mann Whitney U test. All statistical procedures were performed using SPSS Version 26 (IBM Inc). Significance level was set at .05.
Results
We identified 16 strokes in children during the pre-pandemic period and 30 strokes during the pandemic. There was a higher incidence of stroke in Caucasian children during the pandemic period (Table 1). Though there was no significant difference in the median age in children with stroke between the 2 study periods, a higher number of strokes were noted in the older age group during the pandemic period. There was no difference in the proportion of children with underlying risk factors for stroke during the study periods. While ischemic strokes with involvement of the anterior circulation were the predominant type during both study periods, there were significantly more strokes affecting the posterior circulation during the pandemic (36.7% vs 6.3%; P = .04; Table 2). Figure 1 illustrates a posterior circulation stroke with the following findings. NIHSS was significantly lower in the pandemic (median 3; interquartile range: 0-5) compared with the pre-pandemic period (median 7; interquartile range: 5.25-11.75). Although there was no statistically significant difference in outcomes during the study periods, a higher proportion of children were discharged to the rehabilitation unit or died during the pandemic period.
Demographics and Characteristics of the Study Cohort.
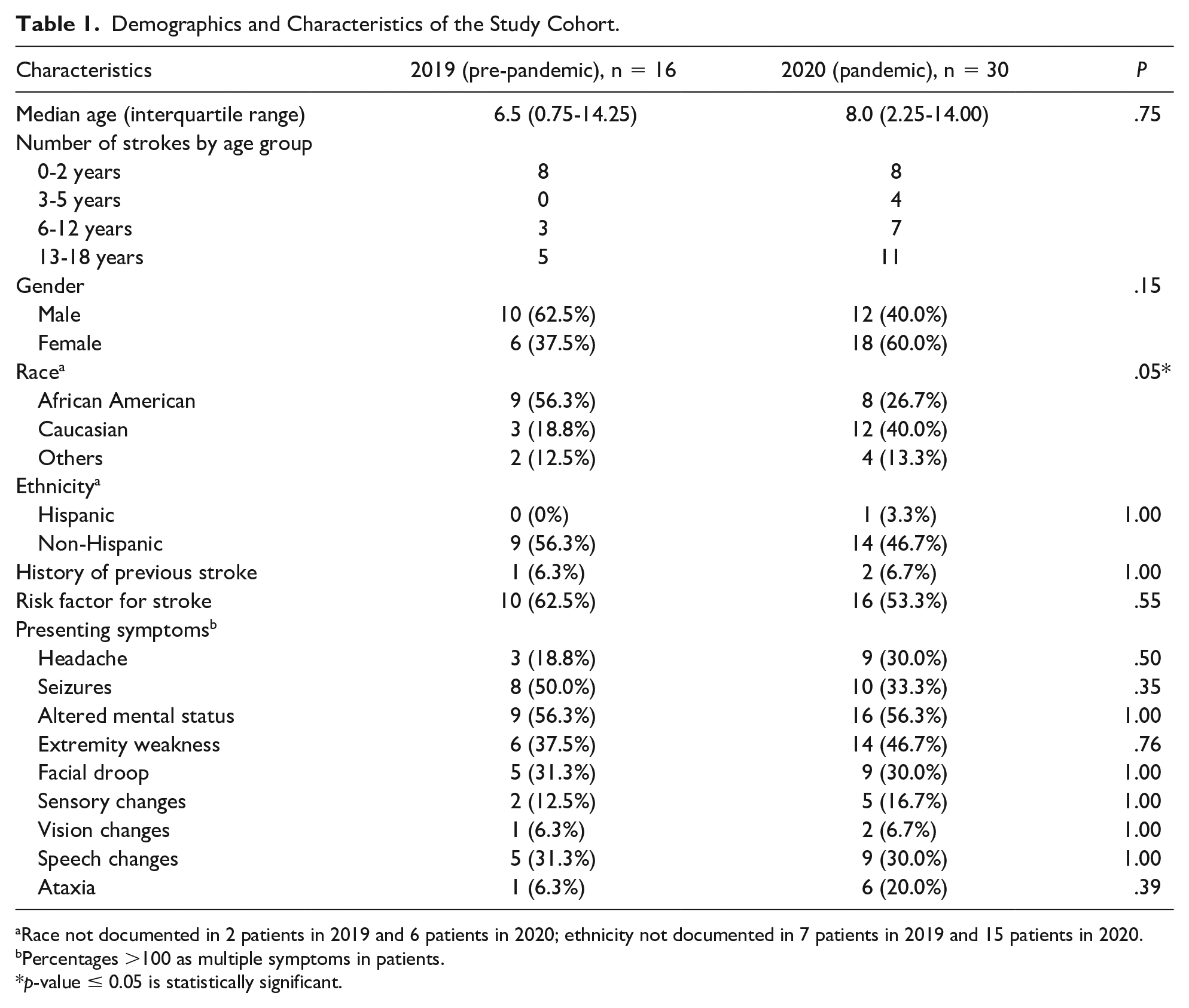
Race not documented in 2 patients in 2019 and 6 patients in 2020; ethnicity not documented in 7 patients in 2019 and 15 patients in 2020.
Percentages >100 as multiple symptoms in patients.
p-value ≤ 0.05 is statistically significant.
Comparison of Acute Childhood Strokes During the Pre-Pandemic and Pandemic Periods.
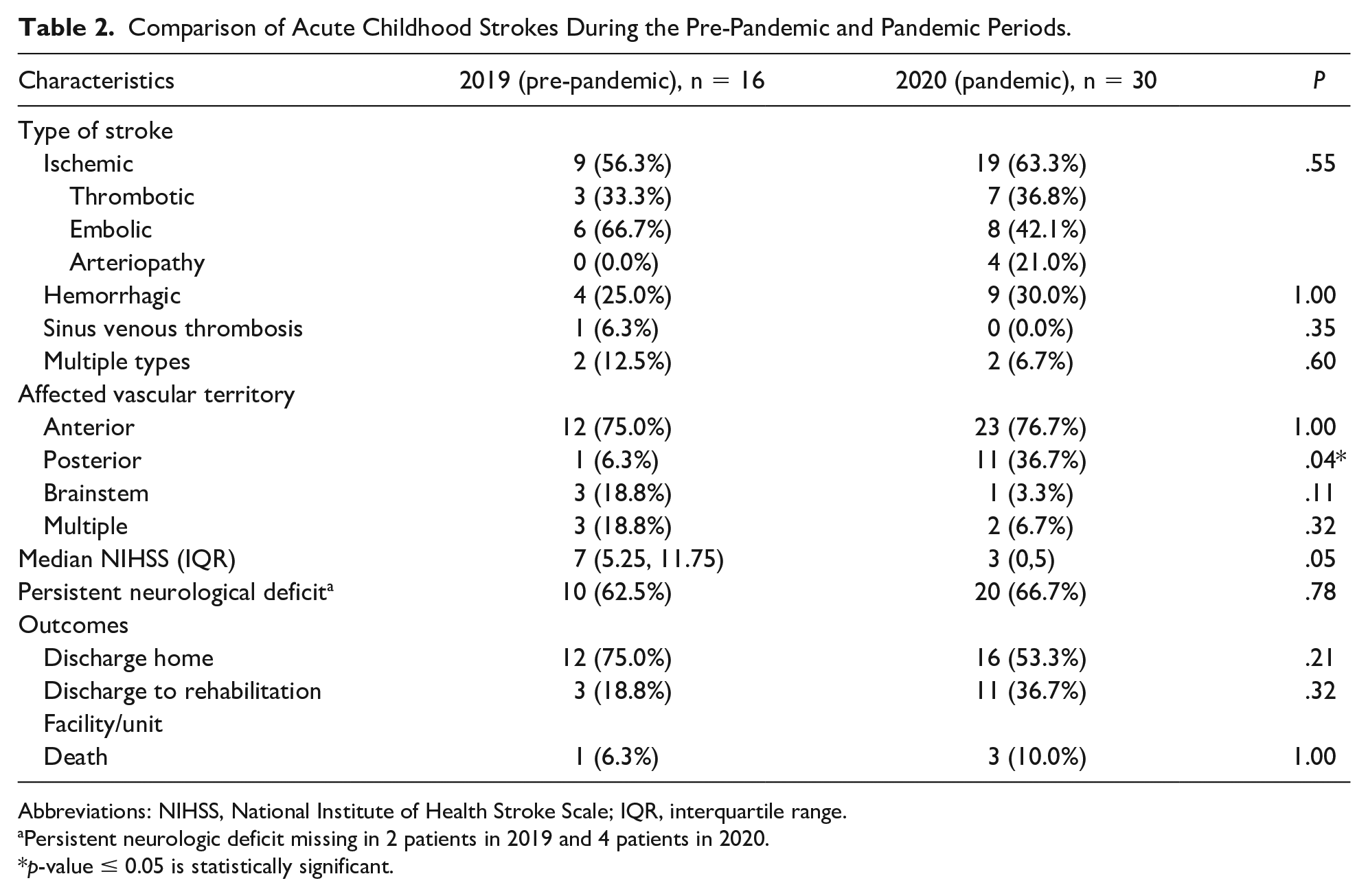
Abbreviations: NIHSS, National Institute of Health Stroke Scale; IQR, interquartile range.
Persistent neurologic deficit missing in 2 patients in 2019 and 4 patients in 2020.
p-value ≤ 0.05 is statistically significant.
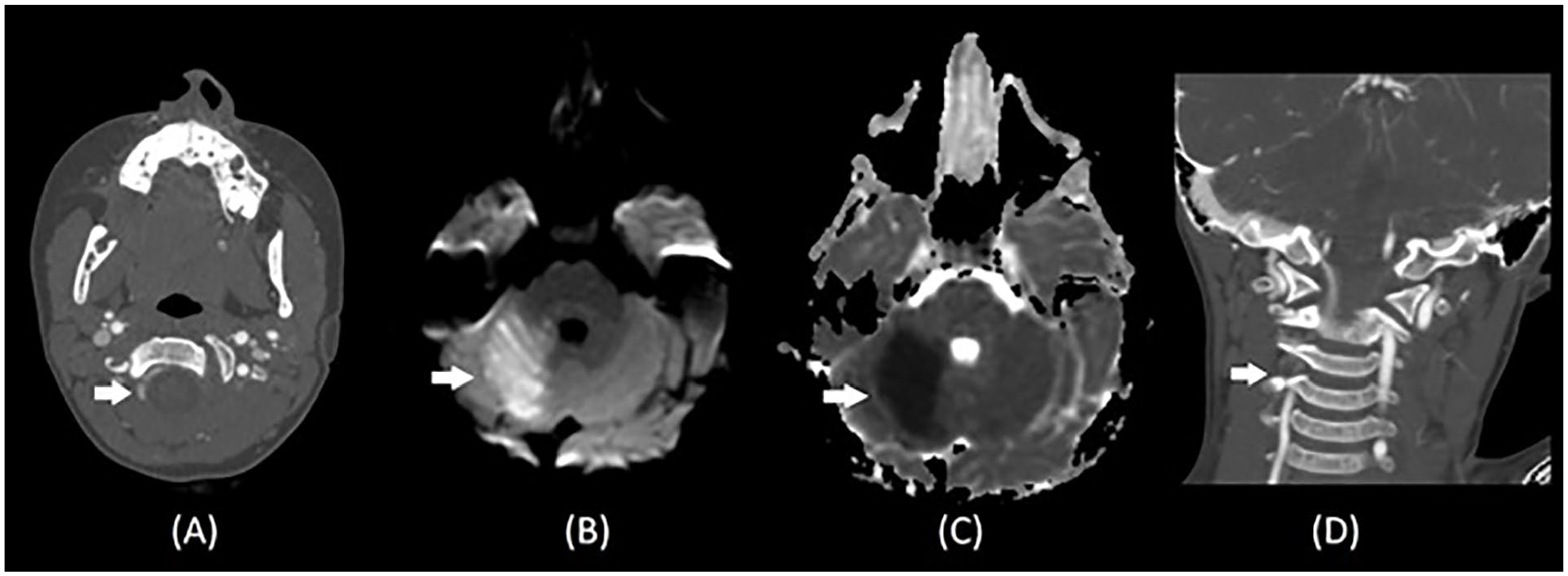
Illustration of stroke involving posterior circulation in our study cohort. (A) Brain magnetic resonance imaging showing acute ischemic stroke with increased signal intensity on T2 FLAIR imaging (arrow). (B) Increased signal intensity on diffusion-weighted imaging (arrow) in the territory of right medial cerebellum extending into the right aspect of the vermis. (C) Corresponding area of low apparent diffusion coefficient value in imaging C (arrow). (D) Magnetic resonance angiogram demonstrates hypoplastic right vertebral artery compared with left (arrow).
During the pandemic, 2 patients (2/30; 6.7%) with stroke had a history of exposure to COVID-19 in the household. None of the patients in 2020 had symptoms suggestive of COVID-19 disease at the time of presentation or in the past 2 weeks. Diagnostic testing for SARS-CoV-2 was performed in 20 children at the time of admission to the hospital (20/30; 66.7%; RT-PCR: 15; RT-PCR and SARS CoV-2 IgG antibody: 5) in 2020 and none were positive.
Discussion
There was a higher incidence of stroke at our tertiary care pediatric institution during the pandemic compared with baseline. There was a predisposition toward affecting Caucasian children. While anterior circulation strokes were still the predominant type there was a higher rate of posterior circulation strokes during the pandemic with ataxia and headache being the most common presenting symptoms. However, these findings must be interpreted in light of the fact that only 20 of 30 children were tested for SARS-CoV-2 and none tested positive by either RT-PCR or IgG antibody testing. Therefore, the findings we discuss must be considered circumstantial.
The overall incidence of neurological complications in children with COVID-19 is estimated to be as high as 22% 9 . The true incidence of COVID-19-related stroke in children is hard to ascertain given the relative rarity of stroke in children even at baseline, which is estimated to be 1 to 2 per 100 000 per year 10 . A recent case series of a large cohort of children with COVID-19 notes that the incidence may well be within the reported pre-pandemic range though the incidence of stroke in adults with COVID-19 is reportedly higher10,11. The large number of strokes identified at our institution during the pandemic cannot be directly correlated to COVID-19 infection, carrier state or presence of MIS-C (multisystem inflammatory syndrome in children), but is an epidemiological observation that deserves further study in a multicenter setting. The number of strokes at the study institution ranged from 12 to 16 per year in the years between 2015 and 2019.
About half of all patients with stroke during the pandemic had a risk factor that included underlying congenital heart disease, previous stroke, or a genetic syndrome that predisposed them to the event. Since no child had MIS-C-like disease process during the pandemic, the strokes that occurred are unlikely to be related to the hypercoagulopathy, endothelial damage, or cytokine storm reported with COVID-19-related strokes12-14. The number of children who had an underlying risk factor for stroke is in keeping with other reported studies in children 15 . Investigations for hypercoagulability were performed in 76% of all children with ischemic stroke or venous sinus thrombosis during the pandemic period and none had abnormalities of note.
The involvement of the posterior circulation in 11 of 30 children constitutes a small but significant minority. There is some evidence from adult stroke data that the posterior circulation appears to be more commonly affected than in the non-COVID-19 setting, as is the involvement of multiple vascular territories and large vessel disease pathology 10 . Strokes in the vertebrobasilar territory can be hard to recognize in children and carry high morbidity and mortality 16 . This is substantiated by the fact that a higher proportion of children passed away or required rehabilitative services following the strokes that occurred during the pandemic.
Limitations
The most salient limitation was that we did not have any patient with stroke with a positive test for SARS-CoV-2, which significantly limits our ability to draw any conclusions regarding the association between increased strokes in children to COVID-19 infection. Furthermore, this was a single center study with a small sample size. The retrospective nature of the study could have limited the data that were available, especially ascertainment of exposure history to SARS-CoV-2 infection in the study cohort. SARS-CoV-2 testing was not performed in the entire cohort in 2020 and type of testing performed also varied.
Conclusions
We noted a higher incidence of strokes in children during the pandemic compared with the pre-pandemic period. However, only two thirds of the cohort were tested for SARS-CoV-2 in 2020, and none of the children tested positive. Large-scale, multicenter prospective studies are needed to evaluate the incidence of strokes in children during the COVID-19 pandemic.
Author Contributions
RS: Contributed to conception and design; contributed to interpretation; drafted manuscript; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
LS: Contributed to conception and design; contributed to interpretation; drafted manuscript; critically revised manuscript; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
SM: Contributed to acquisition.
RT: Contributed to acquisition, analysis, and interpretation.
NK: Contributed to conception and design; contributed to acquisition, analysis, and interpretation; critically revised manuscript; gave final approval; agrees to be accountable for all aspects of work ensuring integrity and accuracy.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.