
Abstract

Educational Objectives
Respiratory distress combined with abnormal renal function should raise suspicion for pulmonary renal syndromes.
It is important to have a high index of suspicion in patients who present with anemia and respiratory symptoms in the setting of an inflammatory disease process as pulmonary hemorrhage may present as the first sign of a new autoimmune disease.
Case Report
A previously healthy, fully immunized, 15-year-old girl presented with a 2-month history of migratory joint pain and swelling, rash described as “red dots” involving bilateral feet, and unintentional subjective weight loss of 20 pounds. Her swelling and pain initially began in her feet and ankles, and then progressed to involve her elbows, knees, and hands. She has additionally experienced 2 weeks of daily fever (maximum temperature of 103 degrees Fahrenheit) and headaches as well as 3 days of nonproductive cough, rhinorrhea, and shortness of breath. She denies trauma or inciting factors for joint pain, sick contacts, recent travel, night sweats, oral or nasal sores, photosensitivity, diarrhea, vomiting, hematuria, dysuria, hematochezia, epistaxis, dysphagia, morning stiffness, or chest pain.
Her initial vitals were blood pressure 103/63 mm Hg, temperature 37.4 degrees Celsius, tachycardia at 123 beats/min, tachypnea at 22 breaths/min, and SpO2 94% on room air. Her physical examination revealed a young woman with normal work of breathing on room air; lungs were clear to auscultation bilaterally. There was observed swelling without warmth or erythema of her ankles and feet bilaterally with pain in her fourth and fifth metatarsophalangeal and proximal interphalangeal joints. There was additionally swelling with erythema but no warmth of her left hand with tenderness in her fourth and fifth metacarpophalangeal and proximal interphalangeal joints. She exhibited normal range of motion in all joints in her upper and lower extremities and normal 5/5 proximal and distal muscle strength. Her skin examination revealed a petechial rash on the dorsum of her feet extending to the ankles bilaterally, 2 non-blanching erythematous patches on the lateral dorsal aspect of her left foot, and 1 erythematous patch on the dorsum of her left hand. The remainder of her examination was normal.
Laboratory evaluation was significant for normocytic anemia with hemoglobin of 5.8 g/dL, elevated blood urea nitrogen of 24.0 mg/dL, and elevated creatinine of 1.56 mg/dL. Electrolytes, liver transaminases, and coagulation studies including prothrombin time (PT) and activated partial thrombin time (aPTT) were unremarkable. Inflammatory markers were elevated with erythrocyte sedimentation rate of 116 mm/h and C-reactive protein of 11.6 mg/dL. Urinalysis was abnormal with white blood cell count of 63/µL, red blood cell count of 43/µL, protein of 70 mg/dL, and 3+ blood. She denied menstruation at the time of collection. Urine protein/creatinine ratio was elevated at 0.7. Serum troponin was elevated at 0.724 ng/mL.
Chest x-ray revealed diffuse ground-glass opacities bilaterally, with no evidence of cardiomegaly or pleural effusion (Figure 1A). Chest computed tomography (CT) without contrast showed interstitial and rounded alveolar opacities and alveolar ground-glass density representing areas of hemorrhage (Figure 1B).
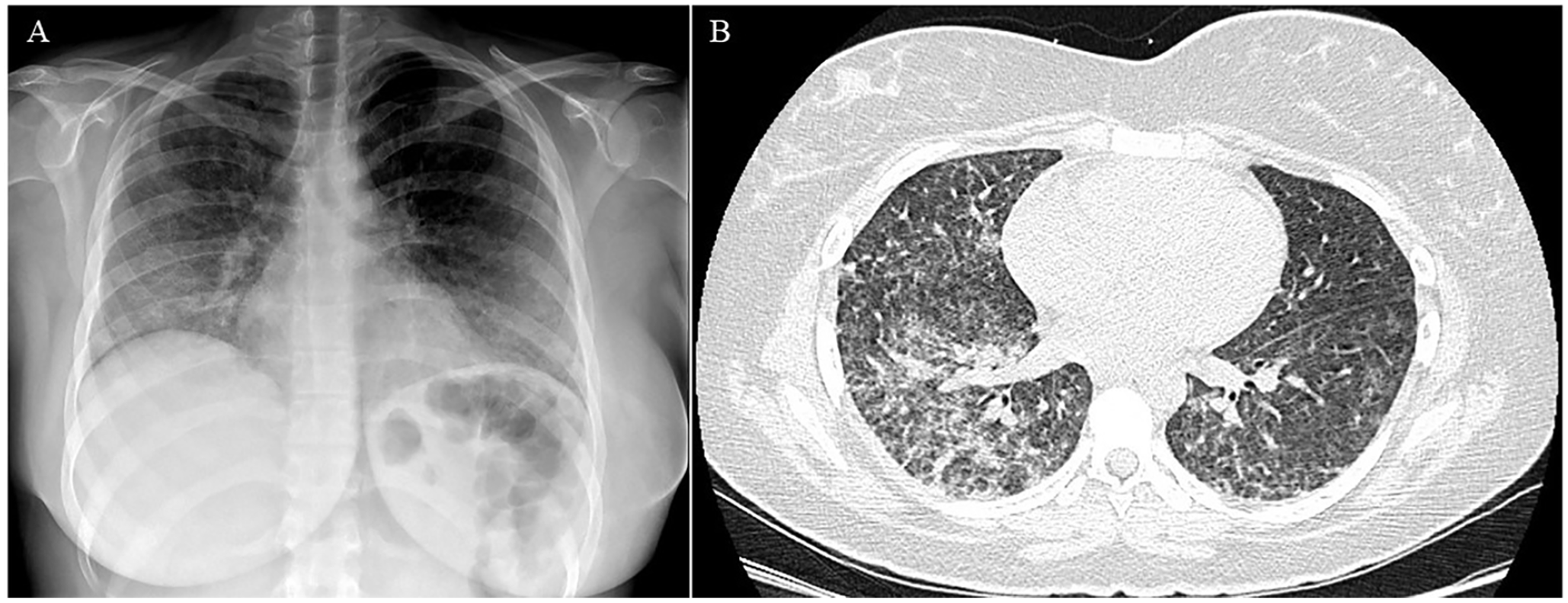
Chest x-ray (A) and chest CT (B) showing pulmonary hemorrhage.
Pulmonary renal syndromes were considered as the leading differential diagnoses for her presentation, including systemic lupus erythematosus, vasculitides such as granulomatosis with polyangiitis (GPA), goodpasture syndrome, microscopic polyangiitis, or immunoglobulin A (IgA) nephropathy. Other causes of pulmonary hemorrhage were considered, including pulmonary hemosiderosis and infectious causes such as cytomegalovirus, adenovirus, mycoplasma, legionella, and Staphylococcus aureus pneumonia. Rocky Mountain spotted fever was considered given her rash, joint pain, and renal and pulmonary failure.
Discussion
Hospital Course
Our patient was admitted to the pediatric intensive care unit (PICU) for further workup and management. Her acute severe anemia, worsening respiratory symptoms, and abnormal chest x-ray were suspicious for pulmonary hemorrhage, confirmed on chest CT. Due to the extent of her anemia, she received a packed red blood cell (pRBC) transfusion. She continued to have symptoms of respiratory distress requiring high-flow nasal cannula. Through further testing, she was found to have normal complement C3 of 149.4 mg/dL, decreased complement C4 of 10.0 mg/dL, and elevated cytoplasmic antineutrophil cytoplasmic antibody (c-ANCA) directed against serinse protease 3 (PR3) IgG at 148 AU/mL, consistent with a likely rheumatologic process. Workup additionally returned reassuring against an infectious etiology. She was thus started on methylprednisolone pulse 30 mg/kg/dose (max 1000 mg) intravenous (IV) for 3 days, with subsequent improvement in respiratory symptoms. She was then transitioned to methylprednisolone 1 mg/kg (max 30 mg) IV 3 times a day and additionally started on epogen and ferrous sulfate for anemia of chronic disease. After stabilization, she underwent a kidney biopsy due to her acute kidney injury on presentation and concern for pulmonary renal syndrome, which revealed severe crescentic glomerulonephritis with approximately 75% glomerular involvement by cellular/fibrocellular crescents with focal necrotizing features. Her serum studies with elevated c-ANCA combined with her renal biopsy results revealed a diagnosis of GPA. Due to the extent of her renal involvement, with 75% glomerulonephritic crescents, she was started on cyclophosphamide with plan to infuse monthly for 6 months. Toward the end of her hospital stay, she was noted to have increased clotting with attempted placement of her peripheral IV. An ultrasound of her bilateral upper extremity veins was performed, which revealed a nonocclusive thrombus in the right radial vein with extension to the proximal and mid-right brachial vein, consistent with deep vein thrombosis (DVT), which was unrelated to her IV line. An ultrasound of her bilateral lower extremities was also performed which was negative for DVT. Coagulation studies were performed which were significant for decreased aPTT of 21.9 seconds, D-dimer elevated at 17.78 µg/mL fibrinogen equivalent units, and antithrombin III elevated at 138%. She was started on enoxaparin sodium. Due to persistent anemia with Hgb 6.3 g/dL, she received a second pRBC transfusion. Given her critical multiorgan involvement with pulmonary hemorrhage, glomerulonephritis, and coagulopathy, she was additionally started on Rituximab. After stabilization, she was discharged home on prednisone 30 mg orally twice daily with close follow up with rheumatology, nephrology, and hematology.
Final Diagnosis
Elevated c-ANCA/anti-PR3 IgG was consistent with c-ANCA-positive vasculitis. This combined with renal biopsy findings of severe crescentic glomerulonephritis with cellular/fibrocellular crescents and focal necrotizing features confirmed the diagnosis of GPA.
Discussion of Case and Literature
ANCA-associated vasculitides (AAV) are a group of autoimmune diseases that present with systemic inflammation and necrosis of blood vessels. Antineutrophil cytoplasmic autoantibodies are serum markers of small vessel vasculitides which are directed against antigens within the cytoplasm of neutrophils. 1 ANCA-associated vasculitides may present with systemic inflammation affecting multiple organ groups, most often the lungs or kidneys. Granulomatosis with polyangiitis is a small vessel necrotizing vasculitis, commonly associated with c-ANCA. Diagnostic criteria for childhood GPA has been defined by the European Alliance of Associations for Rheumatology (EULAR)/Pediatric Rheumatology International Trials Organization (PRINTO)/Pediatric Rheumatology European Society (PRES) classification criteria, requiring at least 3 of the following 6 criteria: (1) histopathology revealing granulomatous inflammation; (2) upper airway involvement with chronic purulent or bloody nasal discharge or recurrent epistaxis/crust/granulomata, nasal septum perforation or saddle nose deformity, or chronic or recurrent sinus inflammation; (3) laryngotracheobronchial involvement with subglottic, tracheal, or bronchial stenosis; (4) pulmonary involvement with chest x-ray or CT showing nodules, cavities, or fixed infiltrates; (5) ANCA positive; and (6) renal involvement with proteinuria, hematuria or RBC casts, or necrotizing pauci-immune glomerulonephritis. 2 By this definition, our patient met 4 of the 6 criteria (histopathology, pulmonary involvement, ANCA positive, and renal involvement), confirming a diagnosis of childhood GPA.
Childhood GPA is rare, and few studies have evaluated the epidemiology of this disease. A recent 2018 cohort study found an incidence of 1.8 cases/million person-years, compared with 12.8 cases/million person-years in working-age adults 18 to 65 years of age, with a female predominance in both age groups. This study revealed higher rates of hospitalizations and hematologic complications in children compared with adults, but similar rates of infection and end-stage renal disease (ESRD). 3
Pulmonary involvement is extremely common in childhood GPA, occurring in 75% of cases. 4 It presents in a variety of ways, ranging from asymptomatic radiographic findings to severe pulmonary hemorrhage. The most common pulmonary manifestation in childhood GPA is pulmonary nodules, which are made of granulomatous inflammation and necrosis, and may be asymptomatic. The most severe and life-threatening pulmonary manifestation is diffuse alveolar hemorrhage. 5 Our patient presented with respiratory distress and was found to have anemia and ground-glass opacities on imaging, consistent with pulmonary hemorrhage. Hypocomplementemia has been identified as a risk factor for alveolar hemorrhage, which our patient did exhibit. 6 The leading cause of morbidity and mortality in patients with GPA is respiratory complications such as pulmonary hemorrhage and chronic lung disease as well as infection due to their chronic immunosuppressive therapy. 7
ANCA-associated vasculitides additionally often affects the kidneys; renal involvement in GPA is characterized by pauci-immune crescent forming focal segmental necrotizing glomerulonephritis. 8 The severity of renal involvement on presentation is closely related to the risk of ESRD and overall survival in patients with AAV. 1 Other complications of AAV include venous thromboembolism (VTE), such as occurred with our patient, with studies revealing an occurrence rate around 10%.9,10 The pathogenesis of VTE formation in AAV remains unclear; however, inflammation in active disease is thought to play a role. Interestingly, a recent study identified patients with AAV with pulmonary hemorrhage or positive PR3-ANCA, both of which were present in our patient, as having increased risk for VTE. 11
Treatment for GPA is critical for survival, and appropriate treatment can lead to clinical remission. Treatment is broken into 2 phases: induction and maintenance. Induction involves treatment with systemic corticosteroids and an immunosuppressant for 3 to 6 months. Methotrexate may be used for localized/limited GPA, whereas cyclophosphamide or rituximab should be considered in severe/refractory disease, such as with pulmonary hemorrhage and renal disease. 4 Plasmapharesis may additionally be considered in patients with these severe manifestations. 12 Following remission, maintenance therapy lasts 18 to 24 months, combining oral steroids with azathioprine or methotrexate. Patients should additionally be treated with sulfamethoxazole/trimethoprim for Pneumocystis jirovecii prophylaxis. 8
Conclusion
ANCA-associated vasculitides are a group of autoimmune diseases affecting the small vessels of the body, most commonly the lungs and the kidneys. They present with systemic inflammation, with respiratory complaints being one of the most common symptoms on presentation. Pulmonary hemorrhage is a life-threatening complication of GPA and may present with respiratory distress and anemia. Patients with hypocomplementemia have been shown to be at higher risk of developing pulmonary hemorrhage. Other complications in GPA include VTE formation, which has been shown to be associated with pulmonary hemorrhage and PR3-ANCA. It is important to consider pulmonary hemorrhage in patients who present with respiratory symptoms and anemia and to consider AAV in patients who present with pulmonary and renal involvement, as early treatment is critical to survival. Treatment involves an induction and maintenance phase using corticosteroids and an immunosuppressant, with therapy tailored to the severity of disease in each individual patient.
Author Contributions
YM: Composed the case report and discussion and identified the radiographic images.
RP: Reviewed and revised the manuscript.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval/Consent
Our study did not require an ethical board approval as there were no ethical concerns. Written informed consent was obtained from the patient’s mother regarding the publication of this case report.