
Abstract
Background:
Childhood overweight and obesity are increasing public health concerns internationally, contributing to significant long-term health risks. School-based interventions integrating policy and behavioural strategies are needed to address this issue.
Objectives:
This study aimed to evaluate the effects of a school-based intervention informed by the Thailand Healthy Living Strategy (THLS) for weight control and obesity prevention among school-age children.
Design:
Cluster randomised controlled trial.
Setting:
Eight primary schools located in Northeastern Thailand.
Methods:
A total of 214 students were randomly assigned to intervention and control groups. The intervention consisted of five structured education sessions delivered over a 3-month period but also included policy development and parental engagement. Data were collected using a structured questionnaire at baseline (pretest) and at 1-month posttest following the intervention. Independent and paired t-tests were used to compare outcomes between and within groups.
Results:
At posttest, the intervention group showed significant improvements in self-efficacy (mean difference = 1.85, p = 0.03), outcome expectation (mean difference = 1.71, p = 0.03), and practice scores (mean difference = 8.40, p = 0.01). Between-group comparisons demonstrated significantly higher outcome expectations (p < 0.001) and practice scores (p < 0.001) in the intervention group compared to the control group. No significant differences were observed for knowledge between groups.
Conclusions:
The THLS-integrated school-based intervention improved self-efficacy, outcome expectations and obesity prevention practices among schoolchildren. These findings support the implementation of multi-component, school-based strategies involving policy, education, and family engagement to promote healthy lifestyles.
Keywords
Introduction
Childhood overweight and obesity have become major global public health issues driven by unhealthy eating behaviour and physical inactivity (Majabadi et al., 2016). These conditions are associated with increased risks of chronic diseases, poor quality of life, and premature mortality later in life (Marcus et al., 2022; Powell-Wiley et al., 2021).
In Thailand, childhood overweight and obesity have become an increasing public health concern. National data from the Thai National Food Consumption Survey conducted in 2003–2005 reported that among children aged 3–18 years, 9.1% were overweight and 6.5% were obese (Jitnarin et al., 2011). More recent evidence indicates that the burden has continued to rise, particularly among school-age children and adolescents. For example, recent estimates suggest that approximately 14% of Thai adolescents are affected by overweight or obesity, reflecting a growing upward trend (UNICEF, 2025). This trend has been driven by changes in dietary patterns, urbanisation, and reduced physical activity among children. In response to these challenges, the Ministry of Public Health introduced the Thailand Healthy Living Strategy (THLS), aiming to address obesity through integrated approaches including policy development, social mobilisation, and community-based interventions (Office of the Permanent Secretary MoPH, 2011).
Since it was first implemented in 2011, the THLS has been used as a national framework to address non-communicable diseases, including childhood obesity. Previous research and programme evaluations in Thailand have suggested that school-based and community-based interventions aligned with national health promotion strategies, such as the THLS, can change health-related behaviours, including dietary practices and physical activity among children (Chawla et al., 2017; Kanchanachitra and Angeles, 2023). However, evidence evaluating the effects of the THLS as an integrated, theory-based intervention delivered within a structured school setting remains limited.
In response to rising childhood obesity, Thailand has implemented national policies promoting healthy eating, physical activity and healthy lifestyle behaviours among school-age children. The THLS for 2011–2020 particularly emphasised lifestyle modification through nutrition, physical activity, and emotional well-being (Office of the Permanent Secretary MoPH, 2011). Evidence has shown that school-based interventions can improve self-efficacy, dietary habits, and physical activity among children (Brown et al., 2016; Wang et al., 2015). In Thailand, approaches to achieving these goals have included health-promoting schools providing healthy food and physical education (Phaitrakoon et al., 2014) as well as parent-involvement programmes (Santiprabhob et al., 2014).
However, the impact of THLS-integrated school-based interventions has not been systematically evaluated. This study aimed to provide insight into this with respect to weight control and obesity prevention among primary school children.
Methods
Study design
This study took the form of a school-based cluster randomised controlled trial conducted in Northeastern Thailand. Data collection took place in 2013 and included baseline (pre-intervention) assessment and a follow-up assessment 1 month after completion of the intervention.
Participants and sampling
The sample size for study, calculated using a variance inflation factor and assuming a 5% non-response rate, suggested a required sample of 381 participants. Multi-stage random sampling technique was used to select schools and students for inclusion in the evaluation. The study took place in Northeastern Thailand, which is administratively divided into five geographical areas. Four geographical areas were selected using simple random sampling for inclusion in the study. From each selected area, one province was randomly chosen. Each province was further divided into five regions, and one region from each province was then randomly selected. Schools were then chosen based on predefined criteria, including school size (large: >300 students; medium: 121–300 students), willingness to participate in the THLS, parental and community engagement, and agreement to implement school-level policy and lunch programme modifications. Small schools (<120 students), schools with fewer than 10% obese students, and schools with any students undergoing medical treatment for chronic health conditions were excluded. In line with these criteria, eight schools were included in the study. All eligible students from these schools (n = 398) were invited to participate. Of these, 239 students consented and were enrolled. After excluding participants with incomplete questionnaires (n = 15) and dropouts (n = 10), the final analytical sample comprised 214 students. Participants were primary school students aged 9–12 years. Baseline characteristics were assessed descriptively to evaluate comparability between the intervention and control groups. A participant flow diagram was developed in accordance with the CONSORT guidelines for cluster randomised trials, clearly distinguishing between cluster-level (schools) and individual-level (students) processes (Figure 1).
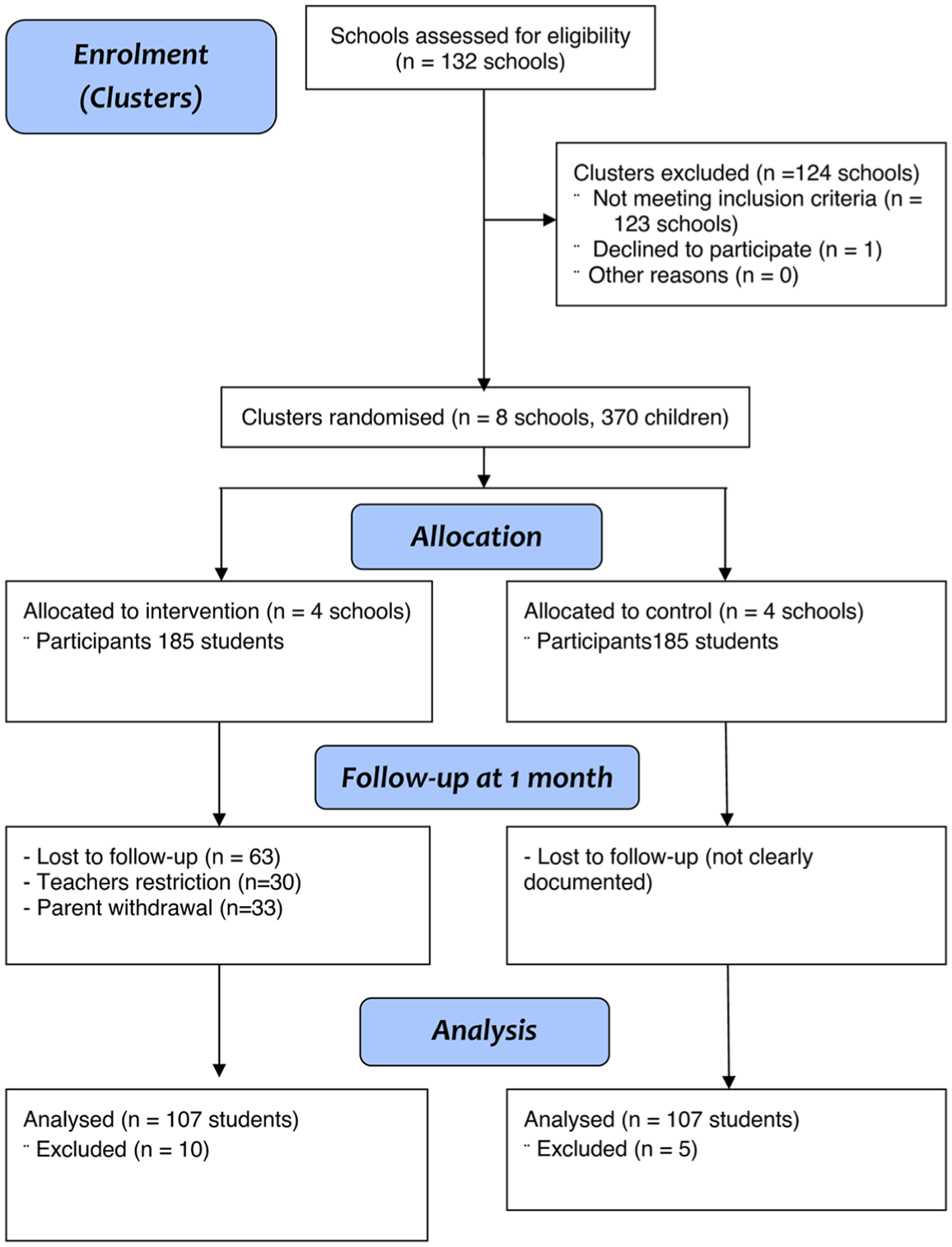
CONSORT flow diagram showing cluster-level (schools) and participant-level (students) flow through recruitment, allocation, follow-up, and analysis.
Intervention
The intervention consisted of five structured sessions delivered over a 3-month period, based on the THLS framework. The programme integrated policy development, educational activities, and family engagement in efforts to promote obesity prevention among schoolchildren. The first session was a one-day workshop conducted for school administrators and teachers focusing on the development and implementation of school-level policies for obesity prevention. The second session was delivered to students and introduced weight control guidelines aimed at promoting healthy behaviours among students. The third session consisted of monthly meetings held once per month for 3 months. Separate meetings were conducted with teachers and parents to discuss strategies for supporting students’ healthy dietary behaviours and physical activity both at home and at school. These meetings were facilitated by the members of the research team. The fourth session took the form of a school-based programme designed to enhance students’ knowledge and skills related to healthy eating and physical activity using interactive and participatory approaches. The final session focused on reinforcing behavioural changes through experience sharing and recognition of student participation.
The first, second, and fourth sessions were delivered as 1-day sessions (approximately 6–8 hours each), while the third session comprised periodic meetings over the intervention period. The interval between sessions ranged from 2 to 4 weeks, allowing time for participants to implement and reinforce behaviour change between activities. Parents and school personnel (teachers and administrators) supported the intervention through participation in meetings, the reinforcement of healthy dietary practices at home, and the implementation of school-level policies. However, they were not included as study participants, and their outcomes were not formally assessed. No additional structured THLS-related interventions or external health programmes were formally implemented in either the intervention or the control schools during the study period. However, as schools are part of the communities they serve, the possibility of informal exposure to health-related information or activities cannot be entirely excluded.
Data collection
Data were collected from participating primary school students aged 9–12 years using a self-administered questionnaire adapted from the Weight Efficacy Lifestyle Questionnaire (Clark et al., 1991) and the International Physical Activity Questionnaire (Al-Hazzaa, 2007). The questionnaire included items on demographic characteristics, body weight perceptions, knowledge, attitudes, beliefs related to diet and physical activity, and behavioural factors, including enabling and reinforcing influences. The instrument underwent content validation by subject experts and was pilot-tested with 30 primary school students aged 9–12 years from a school not included in the main study to assess clarity and internal consistency prior to the main study. Minor adaptations were made to ensure age-appropriate language and comprehension for primary school children. Anthropometric measurements (weight, height, and waist circumference) were collected separately by trained personnel using standardised procedures. Body mass index (BMI) was calculated and classified according to age- and sex-specific criteria based on the International Obesity Task Force guidelines.
Statistical analysis
Data analysis was conducted using STATA version 18.0 (College Station, TX, USA). Descriptive statistics, including frequencies, means, and standard deviations, were used to summarise the data. Prior to inferential analysis, the distribution of continuous outcome variables was assessed for normality using histograms, Q-Q plots, and the Shapiro–Wilk test. The variables were found to be approximately normally distributed; therefore, parametric tests were considered appropriate. Paired t-tests were applied to assess within-group changes, from baseline to post-intervention while independent t-tests were used to compare mean scores between the intervention and control groups. Baseline characteristics, including age, sex distribution, and outcome variables, were assessed descriptively to evaluate comparability between the intervention and control groups prior to the intervention. Statistical significance was set at p < 0.05 with 95% confidence intervals. Given the cluster randomised design, potential clustering effects at the school level were considered. However, due to limitations in the available data, formal adjustment using cluster-level analytical methods or the estimation of the intra-cluster correlation coefficient (ICCs) was not performed. This limitation should be considered when interpreting the results.
Results
Baseline measurements for the intervention and control groups are shown in Table 1 prior to the implementation of the intervention.
Comparison of pretest and posttest mean score for knowledge, self-efficacy, outcome expectations and practices within the intervention and control groups.
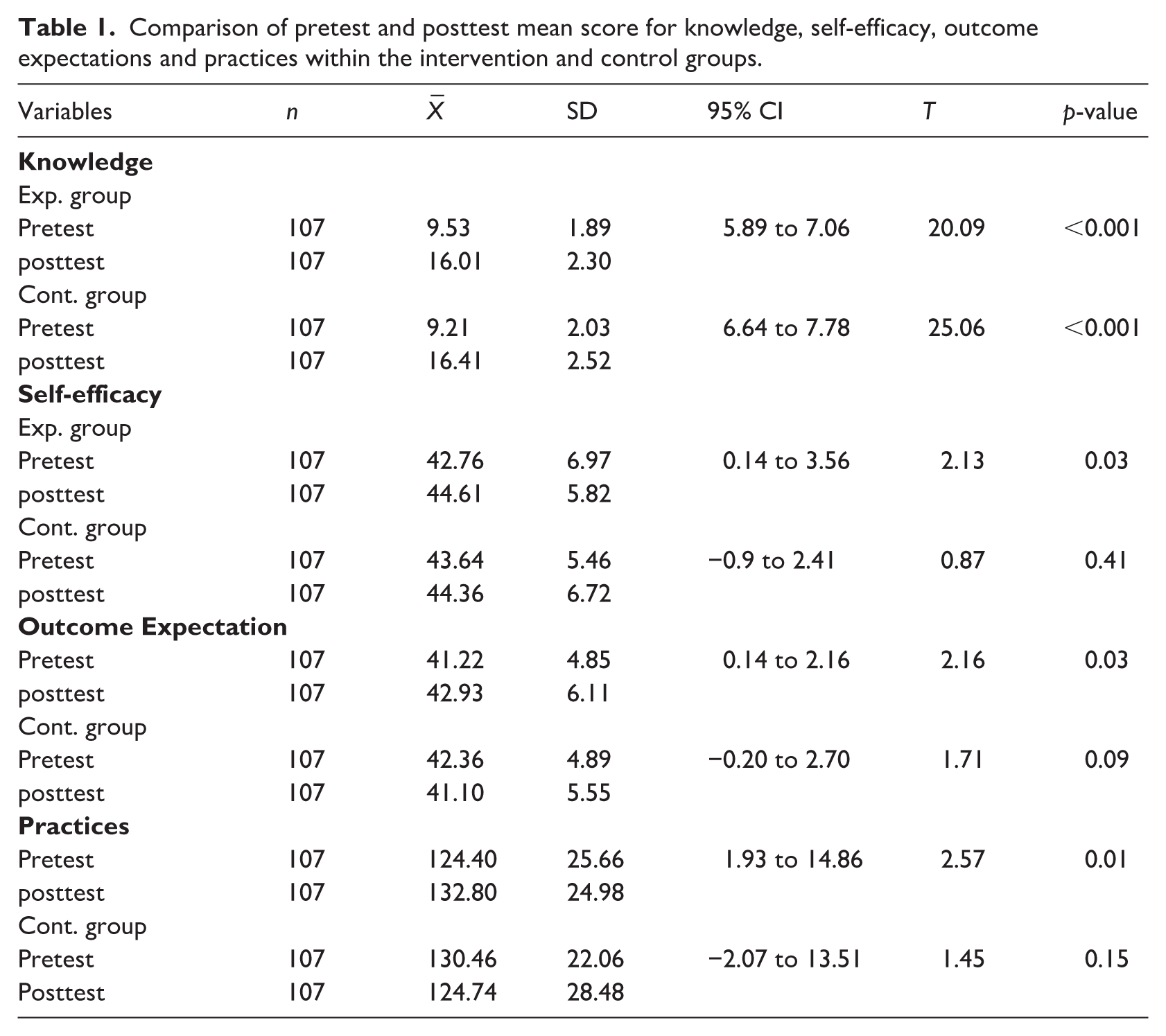
The analysis revealed differences between the experimental and control groups from pretest to posttest. In the experimental group, the mean knowledge score increased from 9.53 ± 1.89 at pretest to 16.01 ± 2.30 at posttest with a significant mean difference (95% CI: 5.89 to 7.06, p-value < 0.001). Similarly, the control group’s knowledge score rose from 9.21 ± 2.03 to 16.41 ± 2.52, also showing a significant improvement (95% CI: 6.64 to 7.78, p-value < 0.001). For self-efficacy, the experimental group demonstrated a significant increase from 42.76 ± 6.97 to 44.61 ± 5.82 (95% CI: 0.14 to 3.56, p-value = 0.03), whereas the control group’s change from 43.64 ± 5.46 to 44.36 ± 6.72 was not statistically significant (95% CI: −0.90 to 2.41, p-value = 0.41). Outcome expectations also improved significantly in the experimental group, rising from 41.22 ± 4.85 to 42.93 ± 6.11 (95% CI: 0.14 to 2.16, p-value = 0.03), while the control group’s change from 42.36 ± 4.89 to 41.10 ± 5.55 was not significant (95% CI: −0.20 to 2.70, p-value = 0.09). Practice scores in the experimental group increased from 124.40 ± 25.66 to 132.80 ± 24.98, indicating a significant improvement (95% CI: 1.93 to 14.86, p-value = 0.01). In contrast, the control group’s change from 130.46 ± 22.06 to 124.74 ± 28.48 was not statistically significant (95% CI: 2.07 to 13.51, p-value = 0.15) (Table 1).
At post-test, significant differences were found between the experimental and control groups for outcome expectation and practice. The experimental group had a higher outcome expectation score (42.93 ± 4.85) compared to the control group (41.10 ± 5.50), with a mean difference of −1.83 (95% CI: −3.11 to −0.47, p-value < 0.001). Practice scores were also significantly higher in the experimental group (132.80 ± 24.98) than in the control group (124.74 ± 24.48), with a mean difference of −0.33 (95% CI: −6.67 to −7.34, p-value < 0.001). No other variables demonstrated statistically significant differences between the groups at either pre-test or posttest (Table 2).
Comparison of mean score differences of student outcomes related to obesity prevention between intervention and control groups.
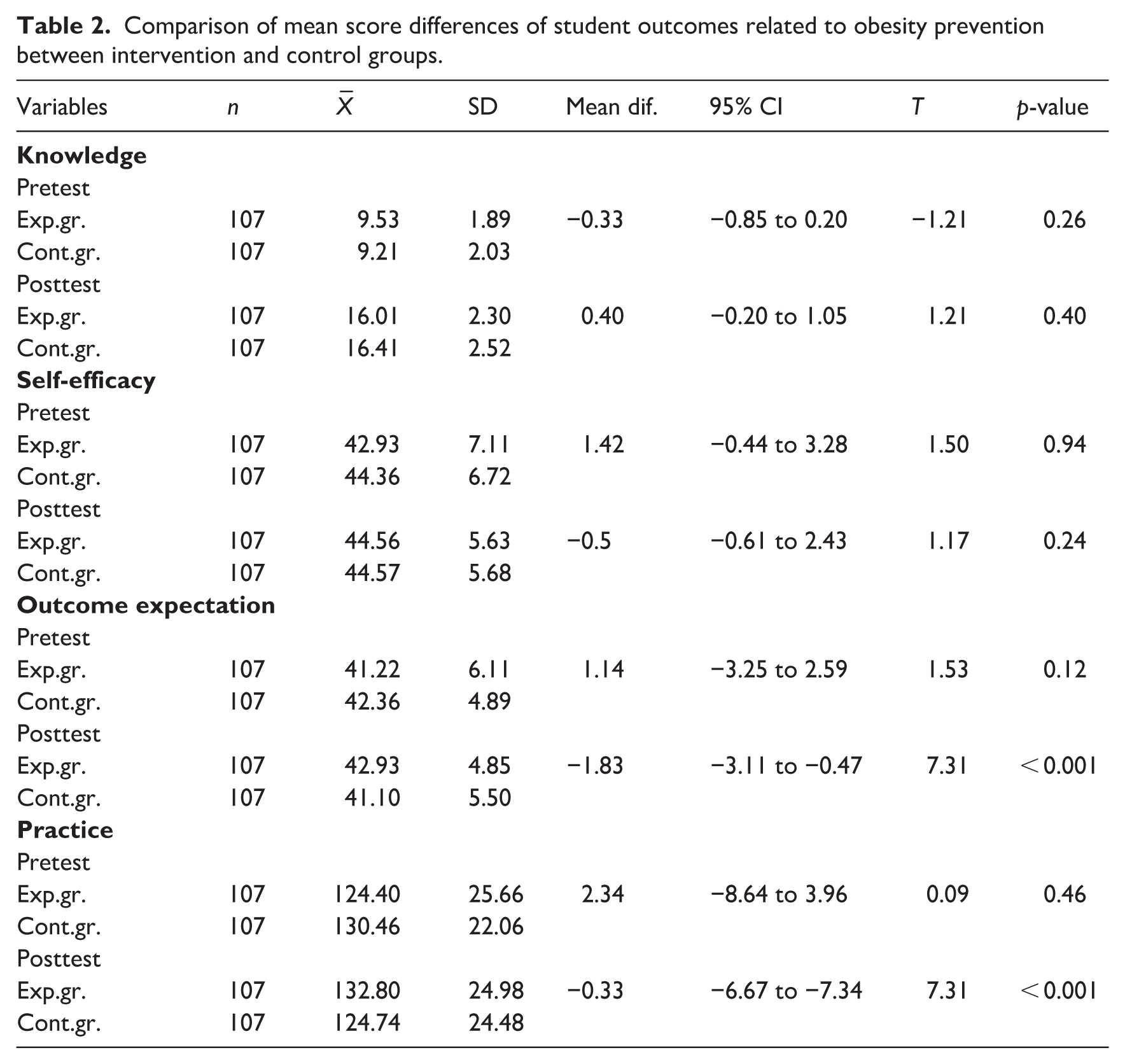
Table 3 shows the percentage distribution of students’ nutritional status before and after the intervention in the control and experimental groups. For analytical purposes, nutritional status was grouped into five categories: thin, slight thin, normal, slight overweight, and obese. In the control group, there was a deterioration in nutritional profile after the intervention: the proportion with normal nutritional status decreased sharply from 70.10% to 40.20%, while overweight rose from 6.50% to 14.00% and slight overweight from 3.70% to 15.90%. The prevalence of thinness also increased from 3.70% to 12.10%. Obesity remained unchanged at 8.40%. In contrast, the experimental group demonstrated an improvement in nutritional status following the intervention. The proportion of students with normal nutritional status increased from 52.30% to 66.40%, while obesity decreased from 14.00% to 7.50% and overweight from 11.20% to 9.30%. The proportions of slight thin and thin students also decreased after the intervention.
Student classification by nutritional status at pre- and post-test.
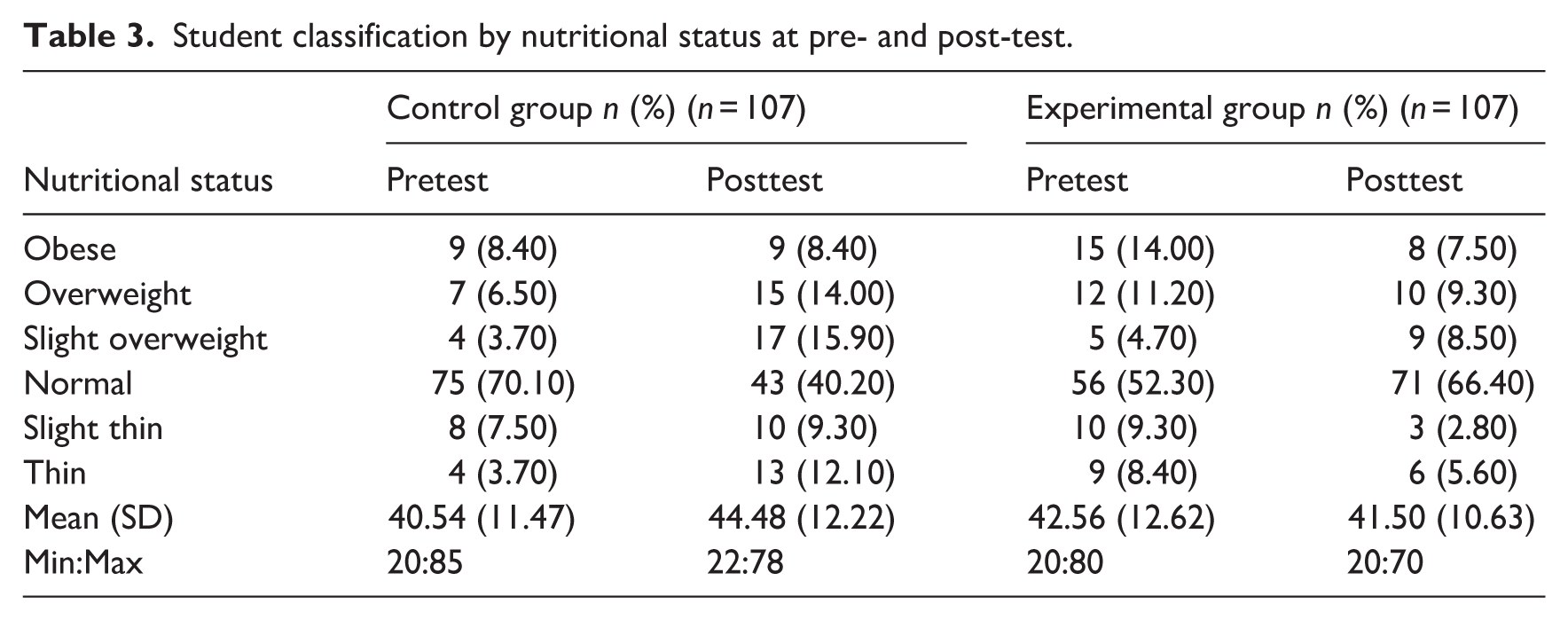
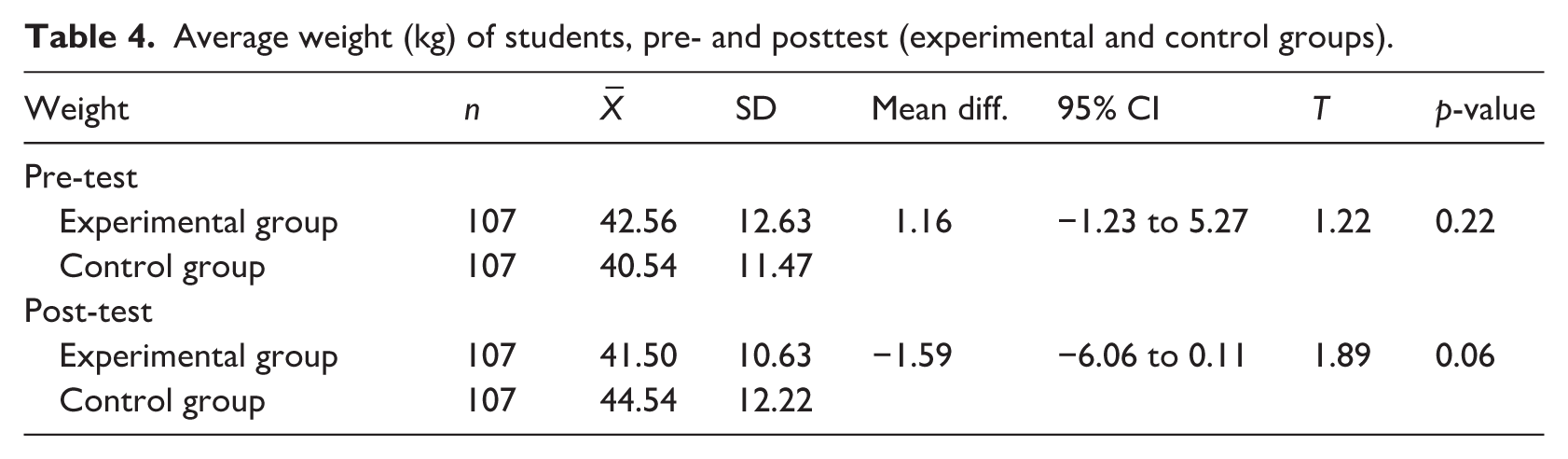
Table 4 compares the average weight of students in the experimental and control groups before and after the intervention. At pre-test, the experimental group had a slightly higher mean weight (42.56 ± 12.63 kg) compared to the control group (40.54 ± 11.47 kg), but the difference was not statistically significant (mean difference = 1.16 kg, 95% CI: –1.23 to 5.27, p-value = 0.22). At posttest, the experimental group’s mean weight (41.50 ± 10.63 kg) was slightly lower than that of the control group, but again the difference was not statistically significant (mean difference = −1.59 kg, 95% CI: −6.06 to 0.11, p-value = 0.06).
Average weight (kg) of students, pre- and posttest (experimental and control groups).
Discussion
This study demonstrated that the THLS interventions positively influenced schoolchildren in four key areas: knowledge, self-efficacy, outcome expectations, and practice. The success of THLS can be attributed to its two main factors: first, the introduction of school policies aimed at controlling the consumption of unhealthy foods while promoting healthier choices; and second, active collaboration between schools, families, and communities, which fostered cooperation in implementing school-based interventions. Practical examples of these strategies included replacing high-fat foods with low-fat options in school lunches, encouraging increased fruit and vegetable consumption, and involving parents and teachers in supporting healthy eating and physical activity behaviours among students. More generally, beyond this study, the THLS has organised successful programmes such as “Moving for Health” and the “Three-Concept Behavioral Change Program” focusing on healthy eating, regular physical activity and avoiding emotional eating. Additional policies implemented in some schools such as “No soft drinks and unhealthy snacks in school,” “Increase vegetables and fruits in school lunches,” and “Promote physical activity every day” have created an enabling environment for sustainable change. These combined efforts led to greater improvements in self-efficacy, outcome expectations and obesity prevention practices in the experimental group compared to the control group, echoing WHO’s (2012) emphasis on supportive environments for school health promotion (WHO, 2012).
The observed decline in the proportion of students classified as having normal nutritional status in the control group over the short follow-up period may have been influenced by several factors. First, changes in BMI classification among children can occur due to growth in height and weight, even within a short timeframe. Second, the absence of a structured intervention in the control group may have contributed to unfavourable outcomes related to diet and physical activity. Finally, external environmental factors, such as dietary habits and sedentary behaviours, may also have influenced these changes. Ultimately, however, we cannot be sure what the key factors were that contributed to these results. Therefore, these findings should be interpreted with caution.
From a psychosocial perspective, the experimental group’s gains in self-efficacy and outcome expectations, in addition to knowledge and practice, are particularly notable. These findings align with Social Cognitive Theory (SCT), which highlights self-efficacy and outcome expectations as key drivers of behaviour change. Higher self-efficacy is known to predict the initiation and maintenance of healthy behaviours, including physical activity, and can mediate intervention effects (Luszczynska and Schwarzer, 2015). While this study did not measure physical activity directly, the observed improvements suggest that enhanced self-efficacy and positive expectations may have supported healthier nutrition-related behaviours.
Regarding nutritional status, the intervention helped stabilise or reverse negative trends in the experimental group, with the proportion of students in the normal category increasing. In contrast, the control group’s profile deteriorated, with increases in overweight and thinness, and a reduction in the normal weight category. Interestingly, mean weight did not significantly differ between groups at baseline or posttest. This outcome is consistent with a randomised controlled trial in Hanoi, Vietnam, where a multicomponent school-based intervention reduced the incidence of overweight but not obesity itself (Pham et al., 2024). These findings suggest that short-term or school-based programmes are unlikely to yield immediate measurable changes in body weight but can still influence behaviours that prevent progression towards overweight or obesity.
Similar patterns have been observed in eHealth and digital interventions. A study conducted among adolescents in Spain reported significant improvements in BMI percentile trajectories and healthy habits among adolescents using eHealth strategies. Although such digital approaches are scalable, the traditional, face-to-face programme used in this study produced comparable psychosocial benefits (Benítez-Andrades et al., 2020). Furthermore, a recent quasi-experimental study grounded in the Health Belief Model (HBM) found that educational interventions significantly enhanced self-efficacy with respect to weight control, particularly regarding diet and exercise (Raman et al., 2024). This parallels our findings, further validating the role of theory-based, educational strategies in promoting healthy behaviours among school-age children.
Due to the short follow-up period of 1 month in this study, the sustainability of the observed behavioural changes could not be assessed. The findings primarily reflect short-term improvements in behavioural and psychosocial outcomes. Long-term follow-up studies are required to evaluate whether these changes are maintained over time. Although parents and schools played an important supportive role in reinforcing healthy behaviours, their contribution was not quantitatively assessed in this study. Future research should also include family and school-level evaluations to better understand their impact on intervention effectiveness.
Limitations
Although the THLS intervention demonstrated positive effects on student behaviour related to weight control and obesity prevention, several limitations should be recognised. First, variability in implementation across schools, influenced by differences between school administrators, teachers, and parents, may have affected the consistency of intervention delivery. Despite efforts to encourage it, parental participation was limited in the study, and records of attendance and engagement were not systematically collected, restricting the ability to assess its contribution to the observed outcomes. Beyond this, the study was unable to control for key behavioural factors that might have influenced outcomes, such as screen time (e.g. television viewing and online gaming), due to the constraints of the school-based design. In addition, the relatively short follow-up period (1 month) limits the ability to assess the long-term sustainability of outcomes. Detailed baseline comparative analyses between groups were limited by the available dataset and should be considered when interpreting the findings.
In addition, certain operational details of the intervention (including exact session duration, educational media and approaches used) were not comprehensively documented. Although the core components of the intervention were implemented, this may limit reproducibility and any assessment of intervention fidelity. Furthermore, school-level contextual characteristics (such as school size and environment) were not fully captured, which may restrict any assessment of comparability between clusters. Potential contamination between groups cannot be ruled out, as schools may have been exposed to parallel ongoing informal health promotion activities within the community. In addition, reliability coefficients (e.g. Cronbach’s alpha) for the questionnaire scales were not available, limiting assessment of their internal consistency. Finally, although this study employed a cluster randomised design, the statistical analysis did not fully account for clustering effects at the school level. The absence of multilevel modelling and intra-cluster correlation coefficient (ICC) estimation may have influenced variance estimates and should be considered when interpreting the findings.
Conclusion
In this study, the THLS-integrated school-based intervention improved a range of psychosocial outcomes, including self-efficacy, outcome expectations, and health-related practices among schoolchildren. However, no significant changes were observed in anthropometric outcomes over the short follow-up period. These findings suggest that the intervention exerted an impact in promoting early health-relevant changes, which may in the longer term make a contribution to overweight and obesity prevention.
Footnotes
Acknowledgements
The authors thank all participating students, parents, teachers, and school administrators for their valuable cooperation and support. We also acknowledge the contribution of the research team and supporting institutions involved in this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by National Research Council of Thailand (NRCT) (Grant Number 81706). Additional institutional support for the work was provided by Khon Kaen University.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The datasets generated and/or analysed during the current study may be made by the corresponding author upon reasonable request.
Declaration of AI Use
Artificial intelligence (AI) tools (ChatGPT, OpenAI) were used solely for language editing and refinement of the manuscript. The authors confirm that all scientific content, analysis, and interpretations are original and take full responsibility for the accuracy and integrity of the work.