
Abstract
Background
More than 1.5 million older adults survive their intensive care unit (ICU) stay annually and older adults comprise 45% of all ICU stays.1,2 The ICU survivors and their caregivers are often burdened with complex medication changes following their hospital stay, such as the addition of new medications, discontinuation of prior therapies, and increased complexity of therapeutic regimens, further compounded by the cognitive and physical adjustments frequently experienced after hospital discharge. These potential adverse medication consequences are substantiated by work by Morandi et al. that indicated 4 out of 5 older adult ICU survivors had one or more potentially inappropriate medications prescribed at hospital discharge, increasing their risk for adverse drug events.3,4 Although older adult ICU survivors are considered to be at highest risk for adverse drug events due to comorbidities and polypharmacy, younger ICU survivors are also at risk for medication-related problems due to severity of their illnesses resulting in complex outpatient medication regimens.
Many medications initiated for specific indications to the inpatient stay are often continued inappropriately to the outpatient setting and can result in iatrogenic harm and unnecessary costs.3-12 An example is antipsychotics started for ICU delirium. Antipsychotics are associated with QTC prolongation, new-onset diabetes, extrapyramidal symptoms, and increased risk of death in older adults—but are often inappropriately continued after the ICU.6-8,13 Likewise, chronic medications used prior to the ICU stay, such as anticoagulants, antiplatelet agents, or statin cholesterol medications, are often intentionally held during acute illness or inadvertently stopped, resulting in potential emergency department visits, hospitalizations, or death. 14
Intensive care unit recovery clinics are being established to address the needs of survivors during this high-risk transition period. These clinics provide an ideal setting for pharmacists to address medication-related problems. Although the ideal composition of an ICU recovery clinic team is unknown, some institutions are mirroring the members of the interprofessional team that works collaboratively in the ICU including a pharmacist. 15 These ICU recovery clinics are typically supported by the interdisciplinary expertise of multiple health care professionals (eg, physician, pharmacist, nurse, social worker, physical and occupational therapist) to provide a holistic approach considerate of the health, cognition, and social challenges that the ICU survivor may encounter during their recovery. The critical need for inclusion of pharmacist oversight and intervention for this vulnerable population was seen in a single-center study. 16
Although inpatient critical care pharmacists have collaborated with health care teams for decades to improve outcomes and costs,17-23 little is known about different practice models for pharmacists and their services in the innovative, interprofessional ICU recovery clinic setting. Likewise, a knowledge gap exists around pharmacists’ perceptions of differing facilitators and barriers to implementation of pharmacist services within the ICU recovery clinics. Therefore, the purpose of this study was to explore the perspectives of a cohort of ICU recovery clinic pharmacists’ perceived barriers and facilitators to practicing in ICU recovery clinics, their activities, and their roles across different institutions and practice settings.
Methods
A cross-sectional survey of an expert panel of ICU recovery clinic pharmacists was conducted. The expert panel consisted of a work group of the Society of Critical Care Medicine (SCCM) Thrive Collaborative ICU recovery clinic pharmacists. This expert panel was chosen due to the limited number of ICU recovery clinics in the United States. This survey was used as a tool to gain the expert panel’s de-identified responses. The survey was administered through a REDCap e-mail invitation in July 2018.
A 15-item questionnaire was developed to assess the study’s objectives. It contained items about pharmacist characteristics (years in practice, education, training, and board certification) and items about the ICU recovery clinic in which each pharmacist practices (setting, patient population, and practicing health care professionals). Items also ranked pharmacist agreement on a scale from never (<5%), rarely (5%-33%), often (34%-66%), routinely (67%-95%), to always (>95%). These items included pharmacist’s perceptions on which services each pharmacist provides (medication reconciliation, comprehensive medication reviews; medication-related problems assessed; and medication-related problems identified).24,25
Checklist items assessed how pharmacists are embedded in the ICU recovery clinic (eg, see every patient, referral), interaction type with other clinicians both inside and outside of the ICU recovery clinic (eg, face-to-face, case conference), and their role in the ICU recovery clinic (eg, clinic design, patient care). Additional questions assessed pharmacists’ perceptions of facilitators and barriers to practicing as a pharmacist in the ICU recovery clinic.26,27 One open-ended question provided pharmacists the opportunity to give additional comments. All questions with an “Other” response option requested that the participant to describe the “Other.” The survey is included in Supplemental Appendix 1.
Survey items were developed through consensus of the pharmacist work group, review by 2 critical care medicine experts involved with SCCM Thrive Initiative, and literature review. The survey was revised for clarity and readability. The survey contained no identifiable information. Descriptive statistics were used to analyze all responses. SAS for Windows version 9.4 was used for data analysis (SAS Institute Inc, Cary, North Carolina). The University of Michigan Institutional Review Board approved this study.
Results
Pharmacist Training
A total of 9 ICU recovery clinic pharmacists completed the survey. The number of pharmacists responding to the survey is limited, representing the low number of known ICU recovery clinics. The average number of years in practice was 16.5 years (SD = 13.5, range = 2-38). The majority of pharmacists reported completing a PharmD degree (8 [89%]), 8 (89%) pharmacists completed a postgraduate year 1 (PGY1) pharmacy practice residency, 7 (78%) pharmacists completed a PGY2 critical care pharmacy residency, with 7 (78%) pharmacists completing both a PGY1 and a PGY2. Other training included a fellowship and a master’s degree in clinical pharmacy (each n = 1, 11%). Board Certified Pharmacotherapy Specialist (BCPS) and Board Certified Critical Care Pharmacist (BCCCP) certification was held by 4 (44%) of the pharmacists, one (11%) pharmacist reported BCCCP certification only, one (11%) reported BCPS certification only, and one (11%) pharmacist previously held Board Certified Nutrition Support Pharmacist certification.
ICU Recovery Clinic and Pharmacist Role
All 9 (100%) pharmacists worked in ICU recovery clinics associated with an academic medical center, with one ICU recovery clinic sharing an additional affiliation with a community hospital. Furthermore, each clinic was associated with a single center except for one site. The types of patients seen in these ICU recovery clinics were primarily from medical (8 [78%]), cardiac (1 [11%]), or surgical (1 [11%]) ICUs.
Of the ICU recovery clinics represented in this sample, all clinic teams (9 [100%]) included a physician lead, 7 (78%) had a nurse, 4 (44%) had a physical therapist, 4 (44%) had a social worker, 3 (33%) had an occupational therapist, 3 (33%) had a respiratory therapist, 2 (22%) had a nurse practitioner, and 2 (22%) had a case manager. The physician leads were pulmonology/critical care and anesthesia/critical care physicians. Medical assistants, neuropsychometricians, research nurses, Citizen’s Advice Bureau representatives, and Brain Injury Trust representatives also played a role in some ICU recovery clinics.
To address ICU survivor’s medication management needs, pharmacists communicated with other health care providers in the ICU recovery clinic through several mechanisms. Communication methods within the ICU recovery clinic included the following: 9 (100%) pharmacists interacted face-to-face with other clinic providers, 4 (44%) interacted through case conference, 3 (33%) through e-mail, 2 (22%) provided written documentation in the electronic medical record (EMR), and 2 (22%) communicated via telephone. Communication methods by pharmacists to providers outside of the ICU recovery clinic included the following: 6 (67%) used e-mail, 5 (56%) left notes in the EMR, 4 (44%) utilized telephone calls, and 3 (33%) interacted face-to-face.
Direct patient care was provided by the 9 (100%) pharmacists surveyed in every patient visit. Outside of direct patient care, pharmacists had several roles within the ICU recovery clinic, including 8 (89%) pharmacists engaging in research, 4 (44%) assisting with clinic design, and 4 (44%) aiding with clinic governance or administration. Patient selection and enrollment for the ICU recovery clinic was also a role for one (11%) pharmacist. In addition to their role in the ICU recovery clinic, many of the pharmacists practiced as inpatient ICU pharmacists or in faculty/specialty clinics; served as PGY2 critical care pharmacy, PGY1 pharmacy residency program directors, or affiliated pharmacy residency program directors/preceptors; chaired several hospital-wide committees; and served as pharmacy school faculty.
With regard to activities performed by pharmacists in ICU recovery clinic patient visits, 7 (78%) always and 2 (22%) routinely conducted medication reconciliation and performed a comprehensive medication review. A summary of pharmacists’ perceptions of the frequency of comprehensive medication review activities performed and medication or health-related problems identified by pharmacists in ICU recovery clinic patients is provided in Figure 1. This expert panel of ICU recovery clinic pharmacists indicated that they often or routinely identified need for medication education (8 [89%]), medication adherence problems (7 [78%]), medication side effects (7 [78%]), subtherapeutic medication dosage (5 ([56%]), medication use without an indication (4 [44%]), failure to receive medication after discharge (4 [44%]), and need for preventive health measures (4 [44%]) in ICU survivors. Other items reported as assessed in a comprehensive medication review were exposure to medications during an ICU stay that may predispose the patient to long-term effects (eg, paralysis, high-dose steroids, vasopressors), drug cost, and formulary evaluation.
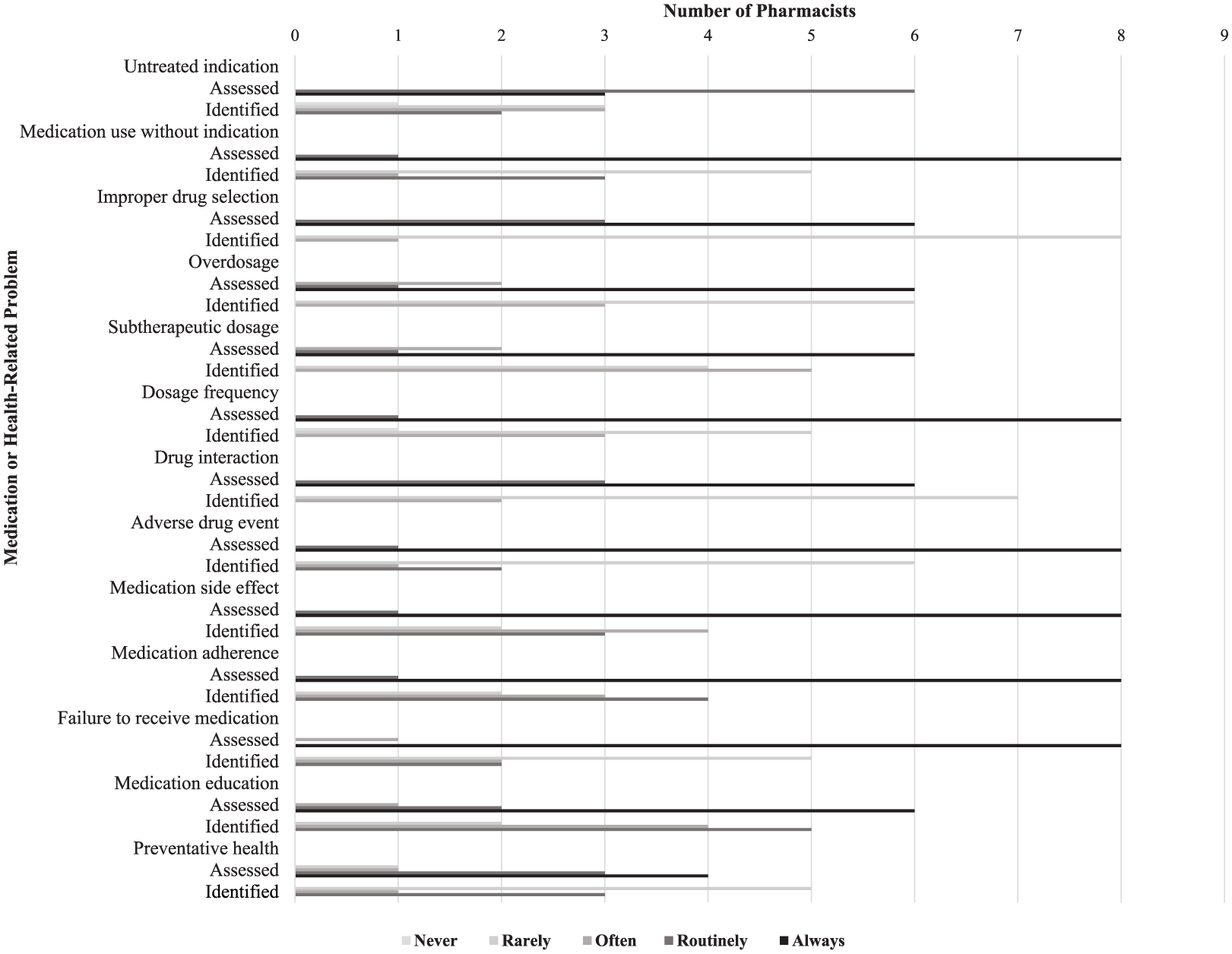
Frequency of medication or health-related problems assessed and identified in intensive care unit recovery clinic pharmacist visits.
Facilitators and Barriers to Pharmacists Practicing in an ICU Recovery Clinic
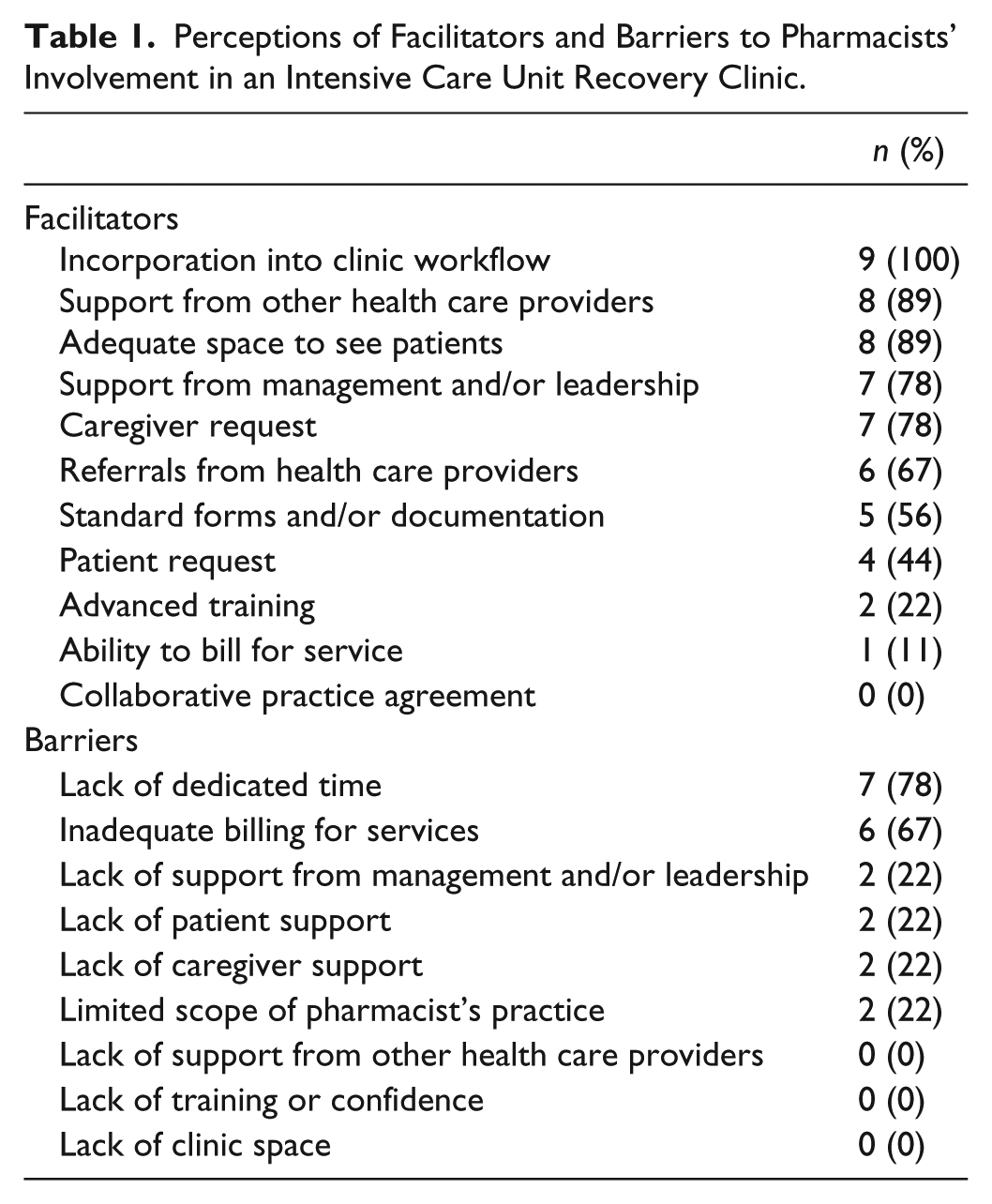
The facilitators most commonly perceived as ensuring the success of the pharmacists’ involvement in an ICU recovery clinic, as well as barriers to success, are listed in Table 1. The 3 most common facilitators to successful participation in an ICU recovery clinic reported were incorporation into clinic workflow, support from other health care providers, and adequate space to see patients. The ICU recovery clinic pharmacists perceived the key barriers to be lack of dedicated time and inadequate billing for services.
Perceptions of Facilitators and Barriers to Pharmacists’ Involvement in an Intensive Care Unit Recovery Clinic.
Discussion
This is the first multicenter report of ICU recovery clinic pharmacists on their role, activities, and facilitators and barriers to practicing in this setting. This study identified that incorporation into the clinic workflow, adequate space to see patients, and support from management or leadership were the key facilitators for pharmacists practicing in the ICU recovery clinic setting, whereas lack of time and ability to bill for services were the main barriers. This expert panel of ICU recovery clinic pharmacists had a variety of roles beyond direct patient care in the clinic itself, including research, clinic design, and governance. In addition, the myriad of pharmacist’s responsibilities outside of the ICU recovery clinic provides insight into the perceived lack of time as a main barrier to practicing within this setting.
While momentum is growing for the establishment of ICU recovery clinics in the United States,28,29 ICU recovery clinics have existed in Europe for years—but almost always without pharmacists to help address ICU survivors’ and their caregivers’ medication-related needs. 30 Studies surveying ICU senior respiratory critical care physiotherapy clinicians, lead clinicians, or nurses about practices in ICU recovery clinics in the United Kingdom revealed that none of the ICU recovery clinics reported involvement of a pharmacist or medication interventions made by another provider.31,32
In the United States, a prospective, observational feasibility study including 62 ICU survivors was conducted in an ICU recovery clinic at an academic medical center between July 2012 and December 2015. A comprehensive medication review was performed by the ICU recovery clinic pharmacist in 56 (90%) of the 62 patients. The median number of pharmacy interventions made by the pharmacist per patient was 4. At least one pharmacy intervention was made in all 56 patients; medications were stopped at the clinic appointment in 22 (39%) patients, and new medications were started in 18 (32%) patients. The ICU recovery clinic pharmacist also identified an adverse drug event (ADE) in 9 (16%) patients, indicating a role for preventing iatrogenic medication harm. Adverse drug event preventive measures were implemented in 18 (32%) patients. Preventive health was also a focus for ICU survivors with influenza vaccination administered to 13 (23%) patients and pneumococcal vaccination administered to 2 (4%) patients. 16
Our results extend beyond this past report to suggest that the main medication-related problems identified by ICU recovery clinic pharmacists across diverse settings were issues with medication adherence, medication-related side effects, and need for medication education. These results provide guidance to pharmacists practicing in or aiming to set up an ICU recovery clinic by revealing core areas to prioritize in a medication review. In addition, the identification of patient’s failure to receive medications has implications for improving ICU survivors’ care transitions, suggesting early follow-up to assess discharge medication receipt or methods to increase access to discharge medications. As the implementation of ICU recovery clinics including pharmacists in the United States expands, additional research is warranted to describe the medication management needs of ICU survivors and their caregivers including strategies to mitigate medication-related problems in this vulnerable population.
Moreover, the practice of pharmacists in an ICU recovery clinic provides a remarkable opportunity for pharmacists to have an equal, independent clinical role and a co-equal role in management, clinic design, and driving the research agenda of the clinic. This provides an important, innovative area of growth for pharmacist services and development. Currently, although pharmacists are recognized as providers in some states, most institutions are not supporting billing due to the low reimbursement rates of pharmacists and the associated administrative burden. Pharmacy professional societies and health care payers should explore encouraging the expansion of pharmacists practicing in this space and reimbursement for their services. Pharmacy professional organizations can influence state or nationwide reimbursement policies to ensure pharmacists’ ability to continue the necessary work in this setting and overcome financial barriers. The reimbursement of pharmacist services is also in the substantial interest of payers given the exceptional opportunity for cost savings by pharmacists in this setting. There are modest costs of a pharmacist providing care relative to the substantial costs of a physician specialist managing medication ICU survivors’ needs, continuing unnecessary high-cost medications, or the potential cost of an ICU survivor’s readmission or nursing home stay related to an adverse event from one of these medications.
When initiating an ICU recovery clinic, first, the pharmacist needs to seek support from their management or leadership. This support would include not only coverage of activities such as order verification or emergency code response from other pharmacists during their clinic time, but also support to bill for services if the pharmacist is considered a licensed provider in that state. Second, the pharmacist needs to determine how to manage their schedule to enable attendance at the clinic. This might require the pharmacist to share their contact information with the rounding team and how to contact them while in the clinic. Third, the pharmacist will need to create a list of questions for not only the patient but also their family members to perform a full medication review and detect any ongoing medication problems. Fourth, the pharmacist should develop a data collection tool to quantify interventions to help justify sustainment of pharmacist services. Last, the pharmacist should seek feedback from other members of the interdisciplinary clinic team to determine how to perform their job more effectively. These activities are summarized in Figure 2.
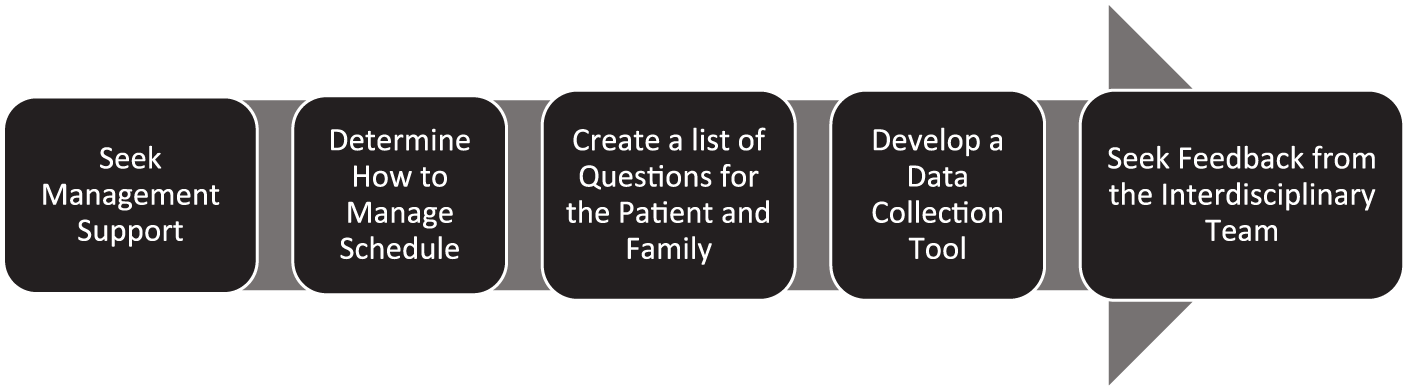
Activities to initiate and sustain pharmacist services in an intensive care unit recovery clinic.
This study has several strengths including being the first to report perceptions of a pharmacist’s role within ICU recovery clinics and barriers and facilitators to pharmacists practicing in this setting. Although the ideal composition of the interprofessional team that comprises an ICU recovery clinic has not been established, many of the ICU recovery clinics in the United States do include a clinical pharmacist. The current article adds to the body of literature by providing practice patterns, facilitators, and barriers encountered by pharmacists who work in ICU recovery clinics. These findings can provide guidance to other pharmacists beginning to practice or involved with implementation of services within an ICU recovery clinic. This study also includes one pharmacist who practices in Europe. This international representation is important as the National Institute for Health and Care Excellence (NICE) guidelines recommend adults who have stayed in an ICU for greater than 4 days have a medical review within 2 to 3 months following ICU discharge. 33
This study also has some limitations which should be recognized. This study only included 9 pharmacists who practice in ICU recovery clinics and are active participants in an international collaborative focused on ICU recovery efforts. We expressly sought an expert panel to describe certain leading edge practices; however, this may not represent an all-inclusive group of pharmacists who provide clinical services within this setting. In the future, this work could be complemented by a systematic survey of the ways in which ICU survivors’ medication-related needs are—or are not—met through other models.
Conclusions
The ICU recovery clinic pharmacists address ICU survivors’ medication-related needs by providing direct patient care in collaboration within the interdisciplinary ICU recovery clinic setting. Strategies to mitigate a pharmacist’s barriers to practicing in ICU recovery clinics, such as lack of dedicated time and inability to adequately bill for pharmacist services, warrant a multifaceted solution, potentially including advocacy and policy work by national pharmacy professional organizations.
Supplemental Material
Appendix_1._Post-ICU_Clinic_Pharmacist_Survey_Questions – Supplemental material for Pharmacists’ Perceptions on Their Role, Activities, Facilitators, and Barriers to Practicing in a Post-Intensive Care Recovery Clinic
Supplemental material, Appendix_1._Post-ICU_Clinic_Pharmacist_Survey_Questions for Pharmacists’ Perceptions on Their Role, Activities, Facilitators, and Barriers to Practicing in a Post-Intensive Care Recovery Clinic by Antoinette B. Coe, Rebecca E. Bookstaver, Andrew C. Fritschle, Michael T. Kenes, Pamela MacTavish, Rima A. Mohammad, Robert J. Simonelli, Jessica A. Whitten and Joanna L. Stollings in Hospital Pharmacy
Footnotes
Acknowledgements
The authors would like to thank Theodore J. Iwashyna, MD, PhD, and Carla Sevin, MD, for their valued assistance and critical insight in this study and acknowledge the THRIVE Post-ICU Clinic Collaborative for advancing this work.
Authors’ Note
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Antoinette B. Coe is supported by the National Center for Advancing Translational Sciences of the National Institutes of Health under Award Number KL2TR002241.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.