
Abstract
Each month, subscribers to The Formulary Monograph Service receive 5 to 6 well-documented monographs on drugs that are newly released or are in late phase 3 trials. The monographs are targeted to Pharmacy & Therapeutics Committees. Subscribers also receive monthly 1-page summary monographs on agents that are useful for agendas and pharmacy/nursing in-services. A comprehensive target drug utilization evaluation/medication use evaluation (DUE/MUE) is also provided each month. With a subscription, the monographs are available online to subscribers. Monographs can be customized to meet the needs of a facility. Through the cooperation of The Formulary, Hospital Pharmacy publishes selected reviews in this column. For more information about The Formulary Monograph Service, contact Wolters Kluwer customer service at 866-397-3433.
Indications
Betibeglogene autotemcel is indicated for the treatment of adult and pediatric patients with beta thalassemia who require regular red blood cell (RBC) transfusions. 1
Beta thalassemia is an autosomal recessive blood disease caused by β-globulin gene mutations that either reduce (β+) or abrogate (β0) production of functional β-globulin. In beta thalassemia, an excess of unpaired α-globulin accumulates and precipitates in the erythroid precursors forming inclusion bodies that cause oxidative membrane damage and impedes red cell development and survival, leading to ineffective erythropoiesis, hemolysis, chronic anemia, and compromised quality of life. Patients with severe anemia (thalassemia major) require lifelong treatment with RBC transfusions and iron chelation to prevent iron overload.2,3 Allogeneic hematopoietic stem cell (HSC) transplantation is potentially curative therapy, with the best outcomes observed in patients younger than 14 years who have a human leukocyte antigen (HLA)-identical donor; however, HSC transplantation is limited by a lack of suitable unaffected histocompatible donors and by the risk of transplantation-related death, graft failure, and graft-versus-host disease.2-4
Betibeglogene autotemcel is also under evaluation for treatment of sickle cell disease, another β-globulin gene disorder.4-6
Clinical Pharmacology
Betibeglogene autotemcel is a βA-T87Q-globin gene therapy consisting of autologous CD34+ cells, containing HSCs, transduced with BB305 lentiviral vector (LVV) encoding βA-T87Q-globin, suspended in cryopreservation solution. It is intended for 1-time administration to add functional copies of a modified form of the β-globulin gene (βA-T87Q-globin) into the patient’s HSCs. 1 The modified β-globulin gene contains an amino acid substitution (T→Q) at position 87. 2
Betibeglogene autotemcel is manufactured from the patient’s own HSCs, which are collected via apheresis. The autologous cells are enriched for CD34+ cells, then transduced ex vivo with the BB305 LVV, a self-inactivating LVV. The promotor, a regulatory element of the LVV that controls the expression of the transgene selected for BB305 LVV, is a cellular (nonviral) promoter that controls gene expression specific to the erythroid lineage cells (RBCs and their precursors). BB305 LVV encodes βA-T87Q-globin. The transduced CD34+ cells are washed, formulated into a suspension, and cryopreserved in patient-specific infusion bag(s). 1
After betibeglogene autotemcel administration, transduced CD34+ HSCs engraft in the bone marrow and differentiate to produce RBCs containing biologically active βA-T87Q-globin that will combine with α-globin to produce functional adult hemoglobin containing βA-T87Q-globin (HbAT87Q). βA-T87Q-globin can be quantified relative to other globin species in peripheral blood using high-performance liquid chromatography. βA-T87Q-globin expression is designed to correct the β/α-globin imbalance in erythroid cells of patients with beta thalassemia and has the potential to increase functional adult HbA and total hemoglobin to normal levels and eliminate dependence on regular packed RBC transfusions. 1
HbAT87Q generally increased steadily after betibeglogene autotemcel infusion and stabilized by approximately month 6 after infusion. Patients had a month 6 median HbAT87Q of 8.7 g/dL (range, 0-12 g/dL) in ongoing phase 3 studies (N = 35). HbAT87Q remained durable, with a median month 24 level of 8.8 g/dL (range, 0.3-12.4 g/dL) in ongoing phase 3 studies (N = 30). 1
Pharmacokinetics
Betibeglogene autotemcel is an autologous gene therapy comprised of HSCs that have been genetically modified ex vivo; therefore, conventional studies on pharmacokinetics, absorption, distribution, metabolism, and elimination are not applicable. 1
Comparative Efficacy
Indication: Transfusion-Dependent Thalassemia
Guidelines
Studies
All patients received full myeloablative conditioning with busulfan prior to treatment with betibeglogene autotemcel. The planned dose of busulfan for patients 18 years and older was 3.2 mg/kg/day as a 3-hour intravenous (IV) infusion daily for 4 consecutive days, with a recommended target AUC0-24h of 3800 to 4500 mcM/minute. The planned dose of busulfan for patients younger than 18 years was 0.8 mg/kg as a 2-hour IV infusion every 6 hours for a total of 16 doses, with a recommended target AUC0-6h of 950 to 1125 mcM/minute. Busulfan dose adjustments were made as needed based on pharmacokinetic monitoring. All patients received antiseizure prophylaxis with agents other than phenytoin prior to initiating busulfan. Prophylaxis for hepatic veno-occlusive disease/hepatic sinusoidal obstruction syndrome was required with ursodeoxycholic acid or defibrotide, per institutional guidelines. A washout period of at least 48 hours was required before betibeglogene autotemcel infusion.
Betibeglogene autotemcel was administered at a median dose of 9.4 × 106 CD34+ cells/kg (range, 5 × 106-42.1 × 106 CD34+ cells/kg) as an IV infusion. G-CSF was not recommended for 21 days after betibeglogene autotemcel infusion; however, 10 of 41 patients (24%) in the combined phase 3 studies (Northstar-2 and Northstar-3) received G-CSF within 21 days after betibeglogene autotemcel infusion. Because betibeglogene autotemcel is autologous, long-term immunosuppressive agents were not required in clinical studies.
After betibeglogene autotemcel, patient iron removal therapy was managed at physician discretion.
Results
Transfusion independence after infusion of betibeglogene autotemcel, defined as weighted average hemoglobin level of 9 g/dL or greater without any packed RBC transfusions for a continuous period of at least 12 months at any time during the study, was achieved in 20 of 22 evaluable patients (91% [95% CI, 71% to 99%]).
Median weighted average hemoglobin during transfusion independence was 11.8 g/dL (range, 9.7-13 g/dL).
All patients who achieved transfusion independence maintained independence, with a median duration of 20.4 months (range, 15.7-21.6 months) according to the published report and a minimum and maximum duration of ongoing transfusion independence of 15.7+ and 39.4+ months reported in the prescribing information.
Median time to last packed RBC transfusion prior to transfusion independence was 0.9 months (range, 0.5-2.4 months) following betibeglogene autotemcel infusion.
For the 2 evaluable patients who did not achieve transfusion independence, a reduction in transfusion volume requirements of 32% and 31% and a reduction in transfusion frequency of 30% and 26% were observed from 6 months postinfusion to last-follow-up compared with pre-enrollment requirements.
Median HbAT87Q at month 6 (n = 18) was 8.9 g/dL (range, 5.2-10.6 g/dL).
Median HbAT87Q at month 24 (n = 18) was 8.9 g/dL (range, 5-11.4 g/dL).
Median hemoglobin at month 6 for patients who did not have packed RBC transfusions in the prior 60 days (n = 20) was 11.7 g/dL (range, 9.3-13.3 g/dL).
Median hemoglobin at month 24 for patients who did not have packed RBC transfusions in the prior 60 days (n = 17) was 12.5 g/dL (range, 9.5-13.3 g/dL).
Neutrophil engraftment occurred at a median of 23 days (range, 13-32 days) after betibeglogene autotemcel infusion.
Platelet engraftment occurred at a median of 46 days (range, 20-94 days) after betibeglogene autotemcel infusion. Platelet counts of at least 100 000/mm3 were observed in 13 of 23 patients (57%) by day 90 and in 22 of 23 patients (96%) by day 365.
Median duration of hospitalization from conditioning through discharge was 45 days (range, 30-92 days).
After betibeglogene autotemcel, patient iron removal therapy was managed at physician discretion. A 13 of 20 patients who achieved transfusion independence are not on chelation therapy as of last follow-up. Of these, 9 of 13 (69%) patients did not restart chelation. A 4 of 13 (31%) patients restarted and then stopped iron chelation, with a median time from last iron chelation to last follow-up of 22.7 months (range, 7.1-23.4 months). Of the 20 patients who achieved transfusion independence, 7 patients (35%) received phlebotomy to remove iron.
Median liver iron concentration was 5.1 mg/g of dry weight at baseline (n = 20) and 4.9 mg/g at 24 months (n = 17).
Change from baseline in cardiac T2* on MRI in patients with transfusion independence did not change over time and was maintained within the normal range in all patients except 1 patient whose baseline value of 21 ms decreased to 15 ms at 12 and 24 months.
Quality-of-life measures were prespecified secondary end points; however, results have not been reported.
In phase 1/2 studies (HGB-204 and HGB-205) including adolescents and adults, 11 of 14 patients with beta thalassemia and a non-β0β0 genotype had transfusion independence after betibeglogene autotemcel infusion; however, hemoglobin levels after treatment were lower than normal hemoglobin levels. Among patients with β0β0 genotype or homozygosity, 3 of 9 had not required transfusions for 14 to 20 months of follow-up and 6 of 9 continued to receive transfusions; however, reductions in the annual number of transfusions and transfusion volumes were observed.2,5,8 The vector copy number and percentage of LVV-positive cells in betibeglogene autotemcel were shown to be associated with hemoglobin levels, and the transduction process was then refined to increase the vector copy in betibeglogene autotemcel and to increase the levels of gene therapy-derived adult hemoglobin with a T87Q amino acid substation. The phase 3 studies were conducted with the updated manufacturing process.2,8 In an analysis of the phase 1/2 studies HGB-204 and HGB-205 and phase 3 studies HGB-207 and HGB-212, peripheral blood vector copy numbers and gene therapy-derived HbAT87Q levels were higher in the phase 3 studies. Additionally, in the phase 3 studies, more patients achieved transfusion independence and total hemoglobin levels were higher than in the phase 1/2 studies. 9
All patients received full myeloablative conditioning with busulfan prior to treatment with betibeglogene autotemcel. The planned dose of busulfan for patients 18 years and older was 3.2 mg/kg/day as a 3-hour IV infusion daily for 4 consecutive days, with a recommended target AUC0-24h of 3800 to 4500 mcM/minute. The planned dose of busulfan for patients younger than 18 years was 0.8 mg/kg as a 2-hour IV infusion every 6 hours for a total of 16 doses, with a recommended target AUC0-6h of 950 to 1125 mcM/minute. Busulfan dose adjustments were made as needed based on pharmacokinetic monitoring. All patients received antiseizure prophylaxis with agents other than phenytoin prior to initiating busulfan. Prophylaxis for hepatic veno-occlusive disease/hepatic sinusoidal obstruction syndrome was required with ursodeoxycholic acid or defibrotide, per institutional guidelines. A washout period of at least 48 hours was required before betibeglogene autotemcel infusion.
Betibeglogene autotemcel was administered at a median dose of 9.4 × 106 CD34+ cells/kg (range, 5 × 106 to 42.1 × 106 CD34+ cells/kg) as an IV infusion. G-CSF was not recommended for 21 days after betibeglogene autotemcel infusion; however, 10 of 41 patients (24%) in the combined phase 3 studies (Northstar-2 and Northstar-3) received G-CSF within 21 days after betibeglogene autotemcel infusion. Because betibeglogene autotemcel is autologous, long-term immunosuppressive agents were not required in clinical studies.
After betibeglogene autotemcel, patient iron removal therapy was managed at physician discretion.
Results
Transfusion independence after infusion of betibeglogene autotemcel was achieved in 12 of 14 evaluable patients (86% [95% CI, 57% to 98%]).
All patients who achieved transfusion independence maintained independence, with a median duration of 19.45 months (range, 12.5-21.7 months) according to the FDA statistical analysis and with a minimum and maximum duration of ongoing transfusion independence of 12.5+ and 32.8+ months reported in the prescribing information.
Median weighted average hemoglobin during transfusion independence was 10.2 g/dL (range, 9.3-13.7 g/dL). Median time to last packed RBC transfusion prior to transfusion independence was 0.8 months (range, 0-1.9 months) following betibeglogene autotemcel infusion.
For the 2 evaluable patients who did not achieve transfusion independence, a reduction in transfusion volume requirements of 92% and 3% and a reduction in transfusion frequency of 87% and 21% were observed from 6 months postinfusion to last-follow-up compared to pre-enrollment requirements.
Median HbAT87Q at month 6 (n = 11) was 8.9 g/dL (range, 3.8-12 g/dL).
Median HbAT87Q at month 24 (n = 8) was 9.8 g/dL (range, 7.9-12.4 g/dL).
Median hemoglobin at month 6 for patients who did not have packed RBC transfusions in the prior 60 days (n = 12) was 10.2 g/dL (range, 8.8-13.2 g/dL).
Median hemoglobin at month 24 for patients who did not have packed RBC transfusions in the prior 60 days (n = 9) was 10.9 g/dL (range, 9.7-14 g/dL).
Neutrophil engraftment was reported on median day 26 (range, 13-39 days) after betibeglogene autotemcel infusion.
Platelet engraftment, defined as 3 consecutive platelet values of 20 000 cells/mcL or greater obtained on different days after betibeglogene autotemcel infusion with no platelet transfusions administered for 7 days immediately preceding and during the evaluation period, occurred at a median of day 46 (range, 20-94 days) in the combined phase 3 clinical studies. Patients without a spleen achieved platelet engraftment earlier compared with those with an intact spleen (median day 42; range, 21-53 days, compared with median day 50; range, 20-94 days).
After betibeglogene autotemcel, patient iron removal therapy was managed at physician discretion. A 7 of 12 patients who achieved transfusion independence are not on chelation therapy as of last follow-up. Of these, 3 of 7 patients (43%) did not restart chelation. A 4 of 7 patients (57%) restarted and then stopped iron chelation, with a median time from last iron chelation to last follow-up of 7.2 months (range, 6-21.4 months). Of the 12 patients who achieved transfusion independence, 1 patient (8%) received phlebotomy to remove iron.
Case reports have also described individual patient experiences from this study, including reports of functional cure and improved quality of life. 12
Contraindications, Warnings, and Precautions
Contraindications
The betibeglogene autotemcel prescribing information states there are no contraindications to its use. Though not stated in the product labeling, a potential contraindication is hypersensitivity to an inactive ingredient (ie, dimethyl sulfoxide). The risk of hypersensitivity reactions, including anaphylaxis, is included as an associated warning. 1
Warnings and Precautions
Delayed platelet engraftment has been observed with betibeglogene autotemcel treatment. Bleeding risk is increased prior to platelet engraftment and may continue after engraftment in patients with prolonged thrombocytopenia; 15% of patients had grade 3 or grade 4 decreased platelets on or after day 100. Patients should be advised of the risk of bleeding until platelet recovery is achieved. Patients should be monitored for thrombocytopenia and bleeding. Platelet counts should be conducted frequently until platelet engraftment and platelet recovery. Blood cell counts should be performed whenever clinical symptoms suggestive of bleeding occur. 1
There is also a risk of neutrophil engraftment failure after treatment with betibeglogene autotemcel. Neutrophil engraftment failure is defined as failure to achieve 3 consecutive absolute neutrophil counts of at least 500 cells/mcL obtained on different days by day 43 after betibeglogene autotemcel infusion. Neutrophil counts should be monitored until engraftment is achieved. If neutrophil engraftment failure occurs, provide rescue treatment with the back-up collection of CD34+ cells. 1
There is a risk of LVV-mediated insertional oncogenesis after treatment with betibeglogene autotemcel. Patients treated with betibeglogene autotemcel may develop hematologic malignancies and should be monitored lifelong. Patients should be monitored for hematologic malignancies with a complete blood count (with differential) at months 6 and 12 and then at least annually for at least 15 years after treatment, and integration-site analysis should be performed at months 6 and 12, and as warranted. In the event of malignancy, the manufacturer should be contacted for reporting and to obtain instructions on collection of samples for testing. 1
Allergic reactions may occur with the infusion of betibeglogene autotemcel. Dimethyl sulfoxide, an ingredient in betibeglogene autotemcel, may cause hypersensitivity reactions, including anaphylaxis. 1
Patients should not take prophylactic HIV antiretroviral medications or hydroxyurea for at least 1 month prior to mobilization, or for the expected duration for elimination of the medications, and until all cycles of apheresis are completed. If a patient requires antiretrovirals for HIV prophylaxis, a negative test for HIV should be confirmed before beginning mobilization and apheresis of CD34+ cells. 1
Patients who have received betibeglogene autotemcel are likely to test positive by polymerase chain reaction assays for HIV due to integrated BB305 LVV proviral DNA, resulting in a false-positive test for HIV. Patients who have received betibeglogene autotemcel should not be screened for HIV infection using a polymerase chain reaction−based assay. 1
Betibeglogene autotemcel recipients should not donate blood, organs, tissues, or cells at any time in the future. 1
Betibeglogene autotemcel has not been studied in patients with renal or hepatic impairment. Patients should be assessed for renal impairment (defined as creatinine clearance [CrCl] 70 mL/minute/1.73 m2 or less) or hepatic impairment to ensure HSC transplantation is appropriate. 1
There are no data on use of betibeglogene autotemcel during pregnancy, and no reproductive and developmental toxicity studies in animals have been conducted with betibeglogene autotemcel to assess the potential for fetal harm. It is unknown whether betibeglogene autotemcel has the potential to be transferred to a fetus. Betibeglogene autotemcel should not be administered to patients who are pregnant. A negative serum pregnancy test must be confirmed prior to the start of mobilization and reconfirmed prior to conditioning procedures and before betibeglogene autotemcel administration. The risks associated with myeloablative conditioning agents on pregnancy and fertility must also be considered. Pregnancy after betibeglogene autotemcel infusion should be discussed with the treating physician. Females of childbearing potential and males of reproductive potential should use an effective method of contraception (intra-uterine device or combination of hormonal and barrier contraception) from the start of mobilization through at least 6 months after the administration of betibeglogene autotemcel. There are no data on the effects of betibeglogene autotemcel on fertility. Because of the risk of infertility with myeloablative conditioning, patients should be advised of the option to cryopreserve semen or ova before treatment, if appropriate. 1
There are no data regarding the presence of betibeglogene autotemcel in human milk, or its effects on breastfeeding infants or milk production. Because of the potential for adverse reactions in a breastfeeding infant, betibeglogene autotemcel is not recommended during breastfeeding, and breastfeeding after betibeglogene autotemcel infusion should be discussed with the treating physician. 1
Safety and efficacy of betibeglogene autotemcel have been established in pediatric patients with beta thalassemia requiring regular transfusions. About 27 pediatric patients were included in the 2 phase 3 studies supporting approval, including 16 children younger than 12 years of age and 11 adolescents 12 years to younger than 18 years. No differences in efficacy or clinical safety were observed between adult and pediatric patients. The safety and efficacy of betibeglogene autotemcel have not been established in pediatric patients younger than 4 years of age. 1
Adverse Reactions
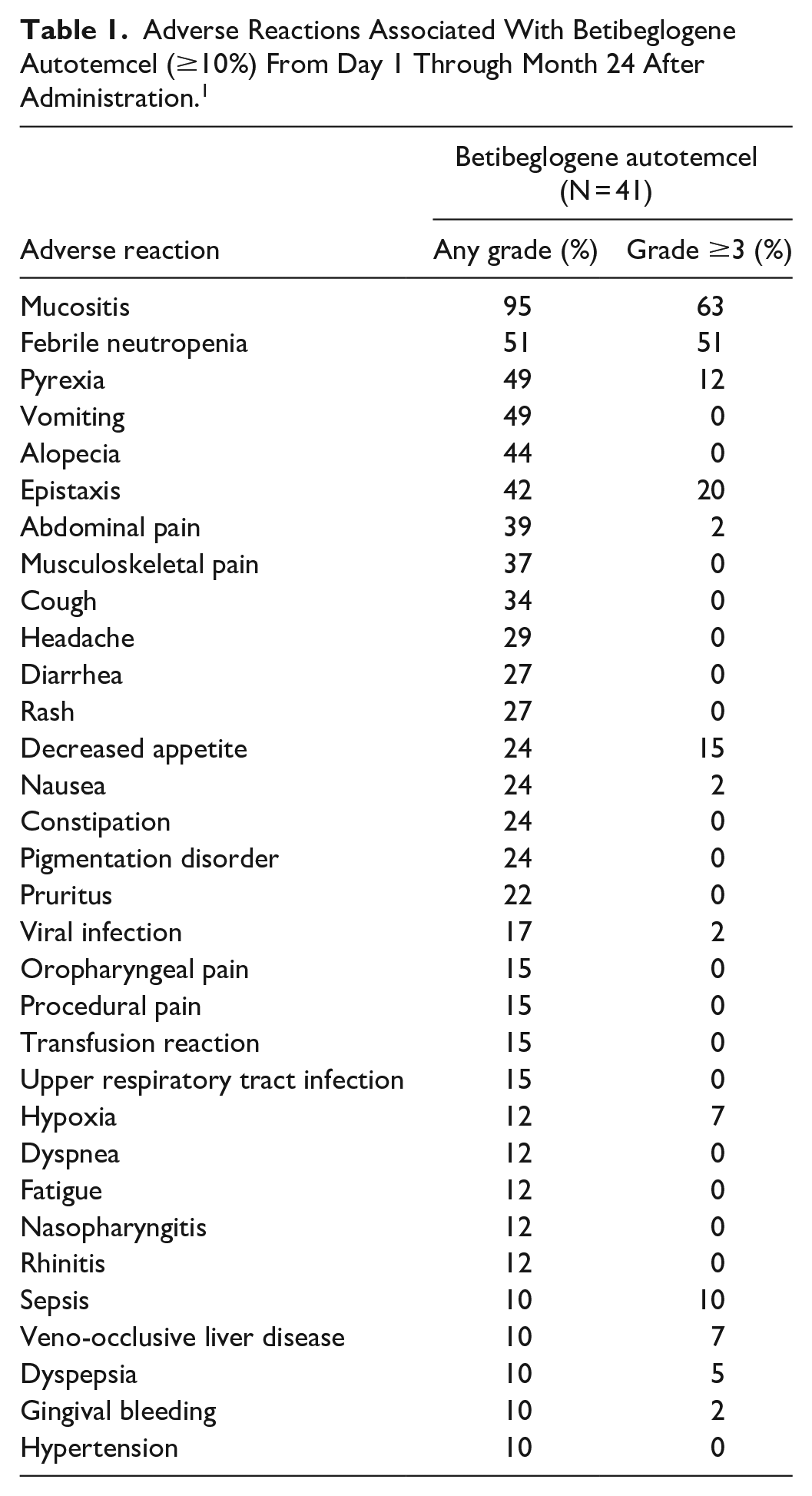
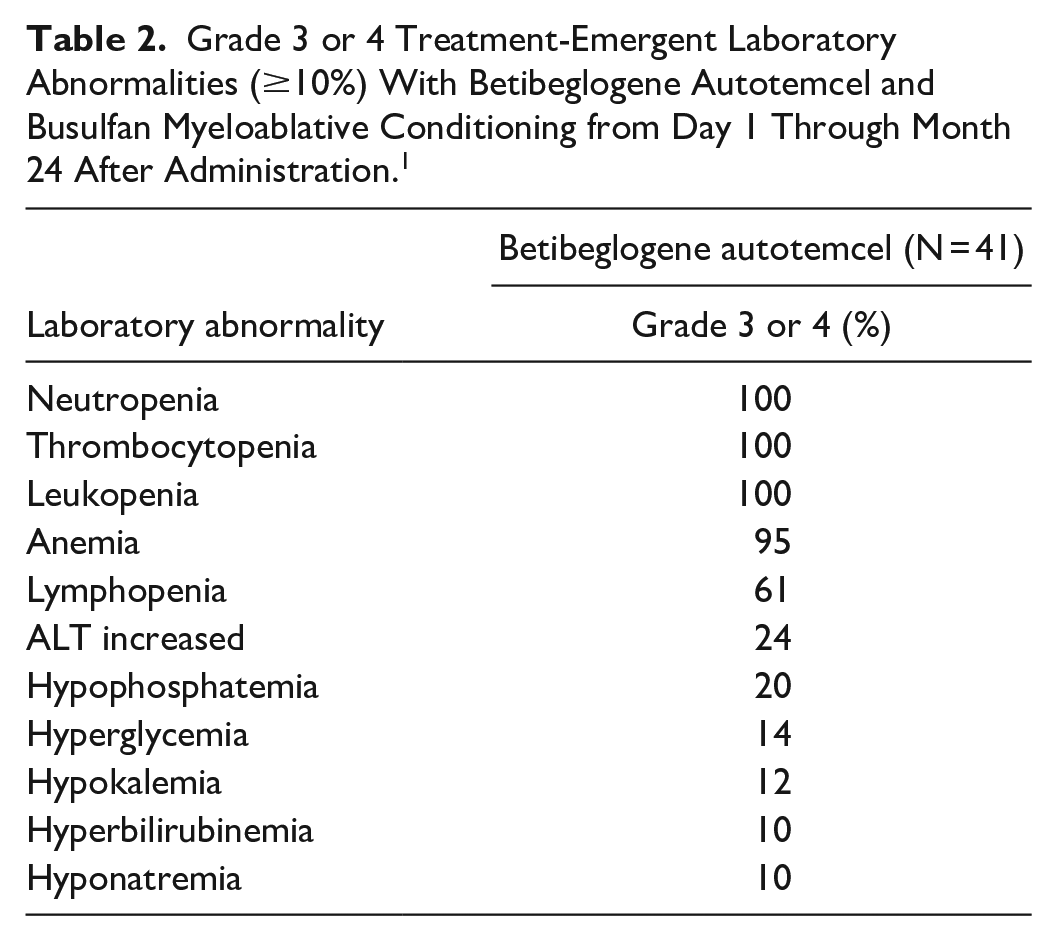
The most common nonlaboratory adverse reactions observed in clinical trials and occurring in at least 20% of patients were mucositis, febrile neutropenia, vomiting, pyrexia, alopecia, epistaxis, abdominal pain, musculoskeletal pain, cough, headache, diarrhea, rash, constipation, nausea, decreased appetite, pigmentation disorder, and pruritus. The most common grade 3 or 4 laboratory abnormalities, occurring in more than 50% of subjects, include neutropenia, thrombocytopenia, leukopenia, anemia, and lymphopenia. The most common serious adverse reactions were pyrexia, thrombocytopenia, liver veno-occlusive disease, febrile neutropenia, neutropenia, and stomatitis. There were no deaths. 1 Tables 1 and 2 summarize the nonlaboratory adverse reactions occurring in at least 10% of patients and the grade 3 and grade 4 laboratory adverse reactions occurring in at least 10% of patients, respectively.
Adverse Reactions Associated With Betibeglogene Autotemcel (≥10%) From Day 1 Through Month 24 After Administration. 1
Grade 3 or 4 Treatment-Emergent Laboratory Abnormalities (≥10%) With Betibeglogene Autotemcel and Busulfan Myeloablative Conditioning from Day 1 Through Month 24 After Administration. 1
Drug Interactions
No formal drug interaction studies have been performed with betibeglogene autotemcel. Betibeglogene autotemcel is not expected to interact with hepatic CYP-450 enzymes or drug transporters. 1
The use of antiretroviral medications or hydroxyurea should be avoided for 1 month prior to mobilization or for the expected duration for elimination of the medications, and until all cycles of apheresis are completed. Antiretroviral medications may interfere with manufacturing of the apheresed cells. 1
Drug-drug interactions between iron chelators and the myeloablative conditioning agent must be considered. Iron chelation treatment should be discontinued 7 days prior to initiation of myeloablative conditioning. Some iron chelators are myelosuppressive; these iron chelators should not be used for 6 months after betibeglogene autotemcel infusion. If iron chelation is needed, consider administration of nonmyelosuppressive iron chelators. Phlebotomy can be used in lieu of iron chelation, when appropriate. 1
There is no clinical experience with the use of erythropoiesis-stimulating agents in patients treated with betibeglogene autotemcel. 1
Institutional guidelines should be followed for vaccine administration. The safety of live viral vaccines during or following betibeglogene autotemcel treatment has not been studied. 1
Recommended Monitoring
Screening for hepatitis B virus (HBV), hepatitis C virus (HCV), human T-lymphotropic virus 1 and 2 (HTLV-1 and HTLV-2), and HIV-1 and HIV-2 should be performed before collection of cells for manufacturing. Betibeglogene autotemcel has not been studied in patients with HIV-1, HIV-2, HTLV-1, or HTLV-2. Confirm a negative HIV test prior to beginning mobilization and apheresis of CD34+ cells if antiretrovirals are required for HIV prophylaxis. Assess kidney function (including CrCl) and hepatic function prior to treatment (to ensure appropriate for therapy). 1
Evaluate pregnancy status prior to therapy; patients who could become pregnant should have a negative serum pregnancy test prior to beginning mobilization, prior to conditioning procedures, and prior to administering betibeglogene autotemcel. 1
Hemoglobin and iron status should be routinely monitored in patients with transfusion-dependent beta thalassemia. Patient hemoglobin should be maintained at 11 g/dL or greater for at least 30 days prior to mobilization and 30 days prior to myeloablative conditioning. Hemoglobin monitoring should continue after treatment to assess response. 1
Patients should be monitored for thrombocytopenia and bleeding. Platelet counts should be conducted frequently until platelet engraftment and platelet recovery. Blood cell counts should be performed whenever clinical symptoms suggestive of bleeding occur. 1
Neutrophil counts should be monitored until engraftment is achieved. 1
Patients should be monitored for hematologic malignancies, with a complete blood count (with differential) at months 6 and 12 and then at least annually for at least 15 years after treatment, and integration-site analysis should be performed at months 6 and 12, and as warranted. In the event of malignancy, the manufacturer should be contacted for reporting and to obtain instructions on collection of samples for testing. 1
Dosing
Betibeglogene autotemcel is provided as a 1-time, single dose for IV infusion containing a suspension of CD34+ cells in 1 or more infusion bags. The minimum recommended dose is 5 × 106 CD34+ cells/kg. The lot information sheet provided with the product shipment should be consulted for additional information pertaining to dose. Betibeglogene autotemcel is for autologous use only. 1
Prior to initiating mobilization, apheresis, and myeloablative conditioning, confirm that HSC transplantation is appropriate for the patient. Screening for HBV, HCV, HTLV-1/HTLV-2, and HIV-1/HIV-2 should be performed before collection of cells for manufacturing. Patient hemoglobin should be maintained at 11 g/dL or greater for at least 30 days prior to mobilization and 30 days prior to myeloablative conditioning. In clinical trials, G-CSF and plerixafor were used for mobilization, and busulfan was used for myeloablative conditioning. The prescribing information for the mobilization agent(s) and the myeloablative conditioning agent(s) should be consulted prior to treatment. 1
HSC mobilization is required followed by apheresis to obtain CD34+ cells for product manufacturing. The target number of CD34 + cells to be collected is at least 12 × 106 CD34+ cells/kg. If the minimum dose of 5 × 106 CD34+ cells/kg is not met, the patient may undergo additional cycles of mobilization and apheresis separated by at least 14 days to obtain more cells for product manufacture. Up to 2 product lots may be administered to meet the target dose. A back-up collection of CD34+ cells of at least 1.5 × 106 CD34+ cells/kg (if collected by apheresis) or greater than 1 × 108 total nucleated cells/kg (if collected by bone marrow harvest) is required. These cells must be collected from the patient and be cryopreserved prior to myeloablative conditioning. This back-up collection is for rescue treatment if there is compromise of HSCs or betibeglogene autotemcel before infusion, primary engraftment failure, or loss of engraftment after infusion of betibeglogene autotemcel. 1
Full myeloablative conditioning must be administered before the betibeglogene autotemcel infusion but should not begin until the complete set of betibeglogene autotemcel infusion bags has been received and stored at the treatment center, and the availability of the back-up collection is confirmed. Iron chelation must be stopped at least 7 days prior to myeloablative conditioning. Prophylaxis for hepatic veno-occlusive disease is recommended. Prophylaxis for seizures should be considered. A minimum of 48 hours should be allowed between completion of myeloablative conditioning and initiation of the betibeglogene autotemcel infusion. 1
Timing of betibeglogene autotemcel thaw and infusion must be coordinated with all involved parties. The infusion time should be confirmed in advance and the start time of the thaw adjusted to ensure the infusion will be ready at the designated time. To prepare for administration, each metal cassette should be removed from liquid nitrogen storage and each infusion bag should be removed from the metal cassette. Confirm that “Zynteglo” is printed on the infusion bag(s), and confirm that the patient identity matches the unique patient identifiers located on the infusion bag(s). Ensure the correct number of bags are present, and use the accompanying lot information sheet to confirm each infusion bag is within the expiration date. If more than 1 bag is provided, thaw and administered each infusion bag completely before proceeding to thaw the next infusion bag. Thaw betibeglogene autotemcel at 37°C (98.6°F) in a water bath or dry bath. Thawing of each infusion bag takes approximately 2 to 4 minutes. Do not leave betibeglogene autotemcel unattended while thawing and do not submerge the infusion ports in the water bath. After thawing, mix gently by massaging the infusion bag to disperse clumps of cellular material. Do not filter, wash, spin down, and/or resuspend betibeglogene autotemcel in new media prior to infusion. 1
Betibeglogene autotemcel must be administered within 4 hours of thawing. Before infusing, again confirm the patient’s identity matches the unique patient identifiers on the infusion bag(s). Use the lot information sheet to confirm the total number of infusion bags to be administered. Administer each bag via IV infusion over a period of less than 30 minutes. Do not use an in-line blood filter or an infusion pump. Flush all betibeglogene autotemcel remaining in the infusion bag(s) and any associated tubing with at least 50 mL of sodium chloride 0.9% solution to ensure as many cells as possible are infused into the patient. 1
Standard procedures for patient management after HSC transplantation should be followed after betibeglogene autotemcel infusion. Any blood products required within the first 3 months after betibeglogene autotemcel infusion should be irradiated. G-CSF is not recommended for 21 days after infusion. Restarting iron chelation may be necessary after infusion and should be based on clinical practice; phlebotomy can be used in lieu of iron chelation if appropriate. 1
Product Availability and Storage
Betibeglogene autotemcel was approved by the Food and Drug Administration on August 17, 2022. 13 It is a cell suspension for IV infusion supplied in up to 4 infusion bags containing 2 × 106 to 20 × 106 cells/mL suspended in cryopreservation solution. Each infusion bag contains approximately 20 mL of betibeglogene autotemcel and is individually wrapped within an overwrap in a metal cassette. 1
Betibeglogene autotemcel will be distributed to a limited network of treatment centers selected for their expertise in stem cell transplantation, cell and gene therapy, and beta thalassemia. 14 Betibeglogene autotemcel is shipped to the treatment center in the vapor phase of liquid nitrogen shipper. Patient identifiers should be confirmed on the product label and lot information sheet within the shipper. The infusion bag(s) should be kept in the metal cassette(s) and transferred from the vapor phase of liquid nitrogen shipper to the treatment center vapor phase of liquid nitrogen storage at −140°C (−220°F) or lower. Product should be stored in the vapor phase of liquid nitrogen at −140°C (−220°F) or lower until ready for thaw and administration. 1
Once thawed, betibeglogene autotemcel must be infused within 4 hours. Do not sample, alter, irradiate, or refreeze betibeglogene autotemcel. 1
Universal precautions and biosafety guidelines (biosafety level 2) should be followed for handling and disposal of betibeglogene autotemcel to avoid potential transmission of infectious diseases. 1
Drug Safety/REMS
No REMS is required for betibeglogene autotemcel. 13
The manufacturer is required to conduct a postmarketing, prospective, observational study to assess long-term safety and the risk of secondary malignancies. This study needs to be completed by March 2043, with the final report submitted by March 2044. 13
Conclusion
Betibeglogene autotemcel is indicated for the treatment of adult and pediatric patients with beta thalassemia who require regular RBC transfusions. Betibeglogene autotemcel is a βA-T87Q-globin gene therapy consisting of autologous CD34+ cells, containing HSCs, transduced with BB305 LVV encoding βA-T87Q-globin, suspended in cryopreservation solution. It is intended for 1-time administration to add functional copies of a modified form of the β-globulin gene (βA-T87Q-globin) into the patient’s HSCs. Treatment with the current formulation in 2 phase 3 studies produced transfusion independence in the majority of patients (91% and 86%). Betibeglogene autotemcel provides a potentially curative therapy for patients with transfusion-dependent beta thalassemia who are not candidates for HSC transplantation. Additional long-term follow-up is necessary to determine whether outcomes are maintained long-term without complications.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.