
Abstract
In recent years, healthcare typologies are increasingly scrutinized. Prevailing healthcare system categorizations draw on comparative–institutional welfare state arrangements that constitute the “rules of the game” for healthcare provision. Challenging these perspectives, health policy perspectives suggest that ongoing policy changes shifted the “rules of the game” in ways that are not adequately captured by traditional comparative–institutional typologies. As a result, new questions arise about which categorization is most salient for understanding public attitudes about healthcare. We adjudicate between these two perspectives by examining the association between healthcare system typology and two different and important types of attitudes about healthcare provision: government responsibility and spending. Using hierarchical linear models, we find that traditional welfare state conceptions of healthcare systems are more closely associated with public opinions about healthcare provision. In general, respondents in countries with healthcare systems that have greater state involvement and rely more on public financing, which are traditional, institutional–comparative factors, report greater support for government responsibility in and spending on healthcare. We highlight how rallying broad public support for changes to healthcare systems in the wake of the COVID-19 pandemic will require that researchers and policy makers understand what the public has come to expect about healthcare, as well as the institutional arrangements around healthcare that set the “rules of the game.”
Introduction
The COVID-19 pandemic focused greater attention on healthcare systems around the world (Lal et al., 2021; Tanne et al., 2020). Studies found that healthcare arrangements shaped pandemic successes and failures. For instance, centralized healthcare arrangements were more effective at halting the spread of COVID-19 and reducing mortality than decentralized and fragmented systems (Armocida et al., 2020; Lal et al., 2021). Among researchers and policy makers, the severity of the COVID-19 pandemic stimulated new discussions about reimagining the role of the state in providing healthcare and the efficacy of government-led efforts (Sturmberg et al., 2020). Less discussed, but nevertheless integral to this reimagining, are public attitudes regarding healthcare and the current and historical realities of healthcare systems (Beckfield, Olafsdottir, and Sosnaud, 2013; Kikuzawa et al., 2008; Stevens, 2001). Thus, reimagining the role of the state in healthcare requires understanding of the “rules of the game”—the institutions that arrange a country’s political economy and, consequently, impact public perceptions and expectations (Beckfield et al., 2015: 5). Healthcare typologies play a vital role in identifying and articulating these rules and, consequently, in examining how they influence public expectations about healthcare provision.
Traditional typologies of healthcare systems are viewed through the lens of broader welfare state categorizations, and scholars in this tradition largely see healthcare as constrained by similar historical institutional arrangements as pensions or unemployment (e.g. Esping-Andersen, 1990). Some research suggests that these institutional–comparative approaches adequately capture the association between healthcare systems and public attitudes regarding healthcare provision (e.g. Kikuzawa et al., 2008; Roosma et al., 2014; Stevens, 2001; von dem Knesebeck et al., 2016). However, following the dramatic rise of healthcare expenditures, seemingly consistent support for government involvement, and broad concern that income-related health inequalities are unfair, new questions arise over whether healthcare systems are distinct from the welfare state (Maldonado et al., 2019; Naumann, 2014; von dem Knesebeck et al., 2016). Thus, a recent strand of research attempts to capture healthcare’s distinctiveness from other forms of welfare production. Building on this line of inquiry, new approaches to categorizing healthcare systems based on health policy emerged, but questions remain about whether these new conceptualizations are more salient for understanding public attitudes about healthcare.
In this article, we compare traditional healthcare system typologies based on past institutional, welfare state conceptions with a recent approach to categorizing healthcare systems that integrates health policy perspectives. Specifically, we examine the association between healthcare system categorizations and public attitudes related to healthcare provision. Drawing on past work about the public’s view of institutional legitimacy, we utilize a multidimensional approach to analyzing public attitudes by examining two aspects of opinion: general functioning (government responsibility) and spending (government financing) (Kikuzawa et al., 2008; Kohl and Wendt, 2004; Missinne et al., 2013; Roosma et al., 2014; Rothstein, 2001).
Pooling the two most recent waves (i.e. 2006 and 2016) of the International Social Survey Programme (ISSP) “Role of Government” module, we utilize hierarchical linear models to analyze data from 26 OECD (Organisation for Economic Co-operation and Development) countries. We find that traditional welfare state conceptions of healthcare systems are more closely associated with public opinions about healthcare provision. In general, respondents in countries with healthcare systems that have greater state involvement and rely more on public financing, which are traditional, institutional–comparative factors, report greater support for government responsibility in healthcare. We observe a similar pattern of results for attitudes about government spending on healthcare—respondents in countries whose healthcare systems boast a high degree of state involvement and public financing are more likely to support higher spending. The results suggest that traditional healthcare system typologies may sufficiently capture dynamics related to normative attitudes about the role of government in healthcare over more recent healthcare typologies that further incorporate health policy measures. However, we note that the newer typology may be more appropriate for understanding attitudes related to satisfaction with healthcare and health equity because of its focus on healthcare quality and performance (Rydland et al., 2020). We highlight how rallying broad public support for changes to healthcare systems in the wake of the COVID-19 pandemic will require that researchers and policy makers understand what the public has come to expect about healthcare, as well as the institutional arrangements around healthcare that set the “rules of the game.”
Comparative–institutional conceptions of healthcare systems
Past work that examines the relationship between healthcare arrangements 1 and attitudes about healthcare provision largely relies on comparative–institutional perspectives (Reibling et al., 2019). They are rooted in a theoretical tradition of path dependency and based on the organizational configuration and roles of the principal actors, including the medical profession, the state, and the payers (Kikuzawa et al., 2008; Stevens, 2001). In Table 1, we highlight the characteristics of the historical–comparative typology (Kikuzawa et al., 2008; Stevens, 2001).
Institutional–comparative healthcare system categorizations from Kikuzawa et al. (2008) and Stevens (2001).
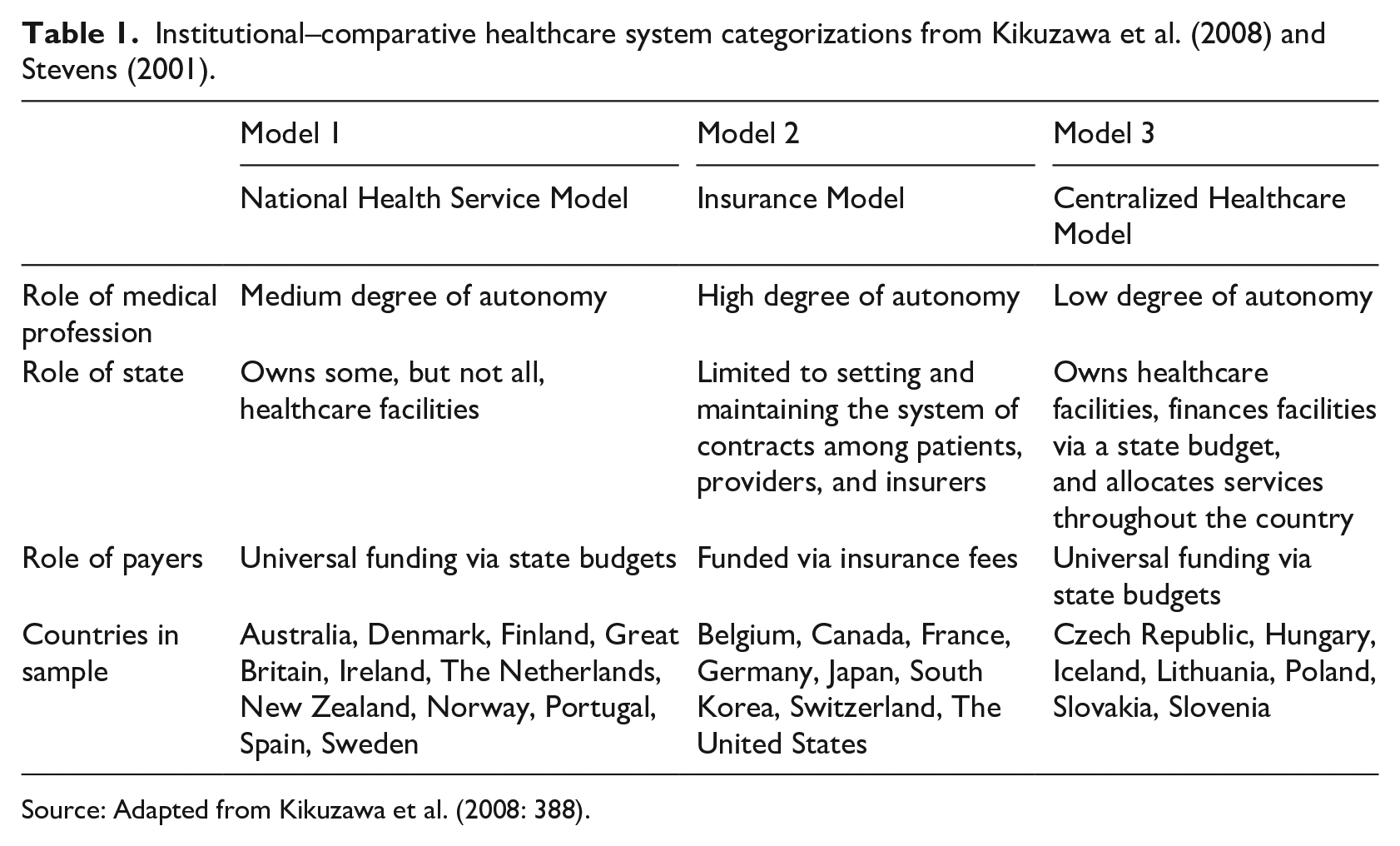
Source: Adapted from Kikuzawa et al. (2008: 388).
Past work suggests that welfare state conceptions of healthcare explain attitudes about healthcare provision well (Kikuzawa et al., 2008; Roosma et al., 2014; Stevens, 2001; von dem Knesebeck et al., 2016). These studies contend that the institutionalization of certain aspects of healthcare parallel that of other domains of welfare in setting “existential standards” for citizens that center on issues like the unfairness of healthcare inequalities, the right to healthcare access, and notions of health justice (Immergut and Schneider, 2020). These standards also generate ideologies about the appropriate relationship between the market and the state via socialization processes that tend to reinforce path dependencies (Immergut and Schneider, 2020; Kikuzawa et al., 2008). For instance, citizens of countries with a high degree of public healthcare funding—via setting expectations that the state should provide healthcare—tend to agree that it is the government’s responsibility to guarantee adequate healthcare, support higher levels of public financing for healthcare, and express higher levels of trust in their government (Cammett et al., 2015; Immergut and Schneider, 2020; Kikuzawa et al., 2008). In this way, “healthcare institutions may play a key role in legitimating the outcomes they produce” (Immergut and Schneider, 2020: 113146).
However, following the dramatic rise of healthcare expenditures, consistently high levels of support for government involvement, and broad concern that income-related health inequalities are unfair, new questions emerge over whether healthcare systems are distinct from the welfare state (Maldonado et al., 2019; Naumann, 2014; von dem Knesebeck et al., 2016). A criticism of the comparative–institutional approach is that it does not capture several important characteristics of healthcare systems, including that healthcare is complex and technical in diagnosis and treatment, that it is influenced by dynamic policy environments, and that public health interventions may more readily impact behaviors and attitudes about the government’s role than other types of policy interventions (Reibling et al., 2019; Robinson et al., 2019; Thomson et al., 2018). These substantive differences between welfare and healthcare lie at the heart of critiques that a more dynamic typology is necessary to better capture aspects of the healthcare system that may influence public attitudes. And thus, health policy perspectives often present different typological accounts of healthcare systems than political economy focused literatures.
The health policy turn: integrating institutions and policy
To advance the science of categorizing healthcare systems, a recent strand of research focuses on what is distinct about healthcare. Drawing from health policy perspectives, this work integrates the comparative–institutional framework of prior welfare state-based typologies but with greater sensitivity to dynamic health policy contexts that include factors related to supply and demand, public–private financing, healthcare access regulations, primary care or specialist orientation, and prevention, performance, and quality of healthcare (Reibling et al., 2019; Rydland et al., 2020; Widding-Havneraas and Pedersen, 2020). This multidimensional approach is important for two key reasons. First, it integrates institutional stability common in previous categorization with respect to the dynamic nature of ongoing health policy changes. In this sense, it moves beyond path-dependent historical views of healthcare. Second, the multidimensional conception allows for a mixture of traits between different types of “traditional” (i.e. welfare state) regimes, such as medium–high levels of overall health expenditures coupled with low levels of expenditures on outpatient care. Health policy reforms create healthcare system hybridizations that are not well captured by these traditional regimes (Reibling et al., 2019). Thus, accounting for the policy environment adds important nuance to the social context through which the public views healthcare as an issue and may help to reconcile past mixed findings.
In Table 2, we present a recent typology created by Reibling et al. (2019). It categorizes countries via cluster analyses 2 of 13 indicators related to the dimensions described in the previous paragraph. Table 2 maps five clusters identified by their analyses to each indicator. We also include the countries in our sample for each type of healthcare system.
The five healthcare clusters and their dimensions—Reibling et al.’s (2019) healthcare systems typology.
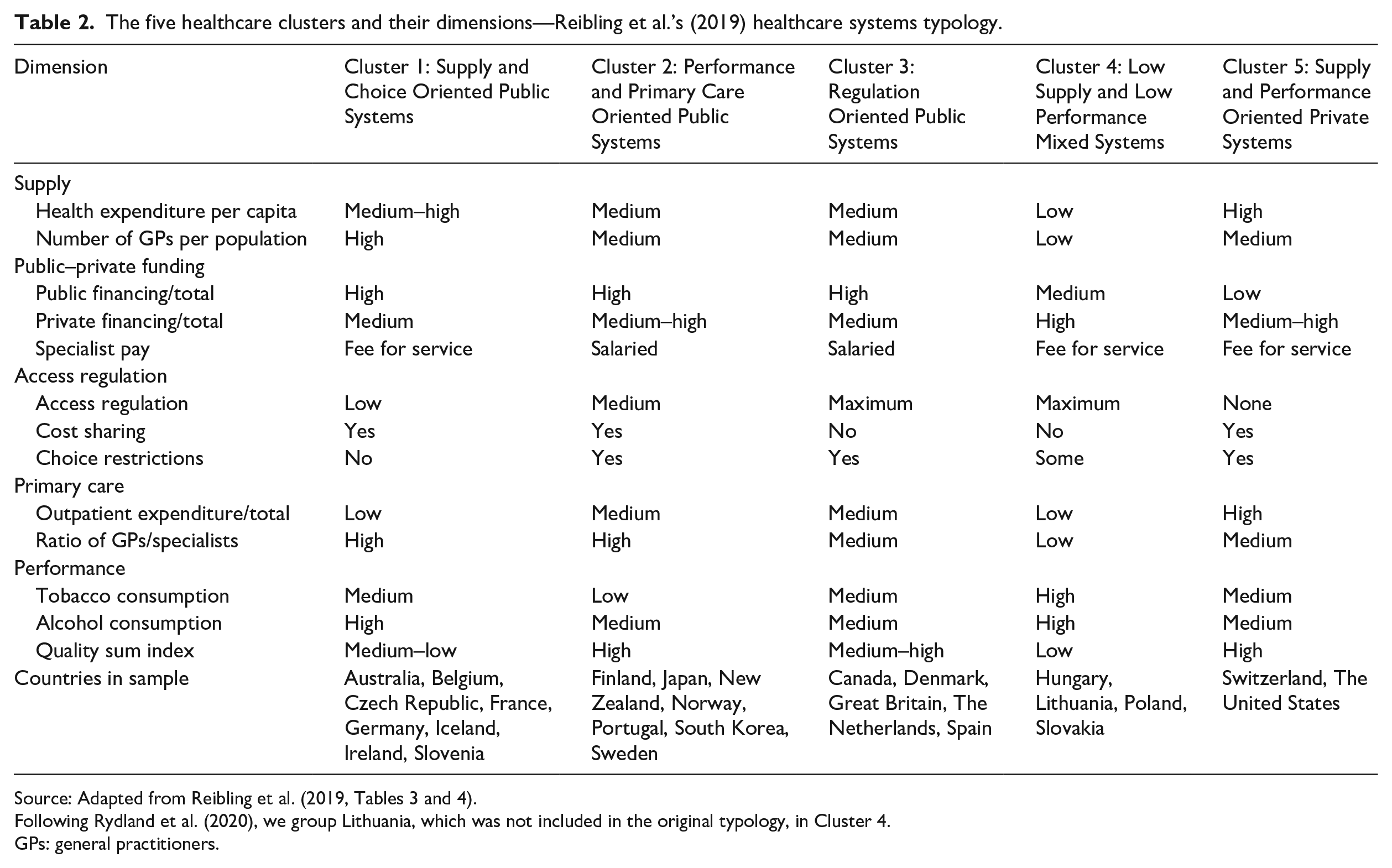
Source: Adapted from Reibling et al. (2019, Tables 3 and 4).
Following Rydland et al. (2020), we group Lithuania, which was not included in the original typology, in Cluster 4.
GPs: general practitioners.
Prior studies find that the degree of public financing is an important predictor of public attitudes about the government’s role in healthcare provision (Missinne et al., 2013; Wendt et al., 2010), as is the density of general practitioners (GPs) and the free choice of providers (Popic and Schneider, 2018; Wendt et al., 2010). Higher out-of-pocket payments also influence attitudes as the public tends to hold negative views about the healthcare system in countries with these arrangements (Popic and Schneider, 2018). These factors provide insight into institutional arrangements of healthcare systems. However, there are good reasons to believe that primary care orientation and performance are important factors that may influence public attitudes (Reibling et al., 2019).
Primary care serves as a low-level point of entry into the healthcare system. As such, it can increase efficiency, equity, and quality of care (Friedberg et al., 2010; Starfield et al., 2005). To the degree that a greater emphasis on primary care facilitates perceptions of healthcare access equity, it may bolster norms that support greater government involvement in healthcare or increased spending (Immergut and Schneider, 2020; Lynch and Gollust, 2010). The degree to which healthcare systems recognize and attempt to achieve prevention and quality performance goals is another salient dimension that legitimizes the government’s role in healthcare in the public’s eyes. Indeed, evidence suggests that some governments’ COVID-19 public health mandates shifted people’s voting intentions, increased trust in government, and led to greater satisfaction with democracy (Bol et al., 2020), while others’ responses led to a “pandemic backslide” toward authoritarianism (Lührmann et al., 2020). Regulatory activities and public health campaigns around risk factors like smoking or alcohol consumption also may improve health outcomes (Reibling et al., 2019), which may lead to greater support for government responsibility in healthcare and increased spending if the public reaps the population health benefits of these regulations.
Thus, several factors may influence how the public perceives the government’s role in healthcare or whether to support greater healthcare spending. Public funding, supply of doctors (particularly GPs), and free choice of doctors may be particularly important for support, perhaps due to the social norms that they create around universal access to healthcare as a human right. Orientations toward primary care and achieving prevention and quality goals may also influence public attitudes via their effects on health equity and improved population health. In these ways, health policy perspectives often expand on traditional typologies that do not account for the latter.
Comparative–institutional versus health policy conceptions
Compelling reasons exist to believe that traditional conceptions of healthcare systems adequately capture public attitudes about healthcare provision. First, a large body of past research illustrates the salience of institutional factors for public attitudes about the government’s role in healthcare and support for healthcare spending (e.g. Immergut and Schneider, 2020; Kikuzawa et al., 2008; Roosma et al., 2014; Stevens, 2001; von dem Knesebeck et al., 2016). Second, institutional factors are known drivers of normative beliefs about the appropriateness of the status quo, fairness, and distributive justice–related issues (Cammett et al., 2015; Immergut and Schneider, 2020; Vilhjalmsson, 2016). Thus, it may be the case that traditional healthcare system typologies are adequate and indeed preferable for understanding public attitudes about the government’s role in healthcare—both in terms of responsibility and spending.
Health policy perspectives provide equally compelling reasons to believe that healthcare may be distinct from the welfare state and warrant separate consideration when establishing healthcare system typologies. First, healthcare costs often outpace other types of social expenditures and potentially generate large reform pressures (Reinhardt et al., 2004; Thorpe et al., 2005). For example, discussions about healthcare costs, inefficiencies, and wasteful spending dominate welfare provision conversations in OECD countries (Ebbinghaus and Naumann, 2018; OECD, 2019). Second, even as healthcare costs expand, government responsibility in healthcare generally enjoys a high degree of public support (Maldonado et al., 2019; Naumann, 2014; von dem Knesebeck et al., 2016). Examining the ISSP data illustrates this point—average level of support for government responsibility in healthcare (3.62; Maximum = 4.00) is much higher than support for government involvement in unemployment (2.98; Maximum = 4.00) or reducing inequality (3.15; Maximum = 4.00).
Some scholars contend that the public views potential health problems and disability differently than other aspects of the welfare state. Health problems are perceived as uncontrollable, unforeseen, and randomly distributed across different types of social groups, and thus necessitate a government safety net (Jensen and Petersen, 2017; van Oorschot, 2000). This conception differs from other aspects of the welfare state, such as unemployment benefits, where in-group considerations, self-interest, and ideological divides often impact support (Jensen and Petersen, 2017; Kuhn and Kamm, 2019). Thus, most people in OECD countries perceive healthcare inequalities 3 as unfair, particularly unequal access and quality of services, regardless of institutional factors (cf. Immergut and Schneider, 2020; Jensen and Petersen, 2017; von dem Knesebeck et al., 2016).
Third, unlike benefits related to pensions or unemployment, healthcare often covers services rendered by the state (Bambra, 2007). Factors related to need and quality, key dimensions of services, are not based on social transfers, which is the foundation for traditional welfare typologies (Bambra, 2007; Quadagno, 2010; Reibling et al., 2019; Zhang et al., 2010). Because healthcare is a service, rising costs and higher utilization may not necessarily equate to better patient outcomes in the public’s mind (Mechanic and McAlpine, 2010). Traditional welfare typologies focus on coverage, funding, and ownership and as a result may fail to capture these additional complexities related to normative attitudes about receiving quality healthcare (Bambra, 2005, 2007).
Yet, even as a service, healthcare differs from other social services, such as education, because it is often perceived as necessary throughout the life course, rather than disproportionately benefitting certain portions of the population. Consequently, healthcare does not appear to present a trade-off between rising cost and diminishing support. Rather, it is characterized by relatively growing levels of expenditures across countries, regardless of welfare state context, unlike other social care services (e.g. pre-school, elder care) that appeal to certain segments of the life course (Jensen, 2008).
All these factors may explain why healthcare-related measures often fail to adequately map onto traditional welfare regime concepts (Jensen, 2008; Quadagno, 2010). Typologies that introduce health policy factors may better capture these dynamics because orientations toward primary care and achieving prevention and quality goals may influence public attitudes above and beyond traditional institutional factors. Centralization of primary care and public health initiatives may support the legitimacy of government responsibility in healthcare via facilitating health equity and improved population health. Higher quality healthcare may warrant greater government spending in the public’s eyes.
Despite competing perspectives over healthcare system typologies, a key limitation of existing studies is that they do not evaluate whether different conceptions of healthcare systems better account for different types of political attitudes (i.e. support for greater government responsibility vs. support for more spending). Divergent results and the lack of an agreed upon taxonomy of healthcare systems portend a need to evaluate the validity of different types of healthcare system typologies for different types of attitudes (Bambra, 2007; Quadagno, 2010). Thus, we address this shortcoming by comparing institutional–comparative perspectives on healthcare systems to conceptions that account for health policy and the distinct nature of healthcare. We examine which perspective better captures the association between healthcare systems and public attitudes about government responsibility in healthcare and healthcare spending.
Data and method
We draw our data from the fourth (2006) and fifth (2016) waves of the ISSP Role of Government Module (i.e. the most recent waves to date). The pooled design nearly doubles the number of countries from existing studies, allows for a longitudinal analysis, and covers important time periods before and after marked shocks to healthcare systems. The 2008 financial crisis, the enactment of the 2010 Affordable Care Act, and policy shifts toward greater privatization in European countries and formerly Communist countries offer an opportunity to revisit past findings that utilize traditional typologies that draw upon older data, to include more sophisticated country-level controls for disease burden from non-communicable diseases (NCDs), and to compare the traditional welfare state typology with the newer health policy one (Kikuzawa et al., 2008; Maarse and Paulus, 2003; Quadagno, 2010). We do not analyze earlier waves of the ISSP Role of Government Module because the Reibling et al. (2019) typology formulates clusters drawing on 2016 OECD Health Data. We opted against including earlier waves as their typology may not extrapolate to countries observed more than a decade earlier than the OECD Health Data used to construct the more recent typology.
A clear strength of ISSP data is that survey modules are standardized across countries and between survey years from nationally representative samples (ISSP, 2019). Our sample includes 26 OECD countries and 35,533 to 35,538 respondents for the government spending and responsibility models, respectively.
Dependent variables
Past research on government attitudes primarily focuses on spending-related concerns and support for government responsibility in healthcare (Jensen and Naumann, 2016; Maldonado et al., 2019; Naumann, 2014). These types of attitudes reflect normative value judgments about the general function and financing role of government in healthcare (Andreß and Heien, 2001; Kikuzawa et al., 2008). Following past work (e.g. Missinne et al., 2013; Popic and Schneider, 2018; Wendt et al., 2010), we analyze the most widely studied aspects of government involvement: support for government responsibility in healthcare and support for greater government spending on healthcare.
Respondents were asked, “On the whole, do you think it should or should not be the government’s responsibility to provide healthcare for the sick.” Responses were measured on a 4-point scale that included the following: definitely should not be (coded 1), probably should not be (coded 2), probably should be (coded 3), and definitely should be (coded 4). For the spending variable, respondents were asked, “Should the government spend more or less for healthcare?” with responses measured on a 5-point scale that included the following: spend much less (coded 1), spend less (coded 2), spend the same as now (coded 3), spend more (coded 4), and spend much more (coded 5). We treat all these variables as continuous variables in the main models but present results from multilevel mixed effects generalized linear models (GLM) with an ordinal family and a logit link as a robustness check.
Key independent variable: type of healthcare system
We compare two healthcare system typologies: one based on traditional welfare state theoretical perspectives utilized by Kikuzawa et al. (2008) and one that leverages international healthcare policy perspectives devised by Reibling et al. (2019). 4 For the Kikuzawa et al. (2008) typology (hereafter, “KOP” for “Kikuzawa–Olafsdottir–Pescosolido”), the categorizations are National Health Service Model (coded 1), Insurance Model (coded 2; reference category), and Centralized Healthcare Model (coded 3). For the Reibling et al. (2019) typology (hereafter, “RAW” for “Reibling–Ariaans–Wendt”), the categorizations are Cluster 1: Supply and Choice Oriented Public Systems (coded 1), Cluster 2: Performance and Primary Care Oriented Public Systems (coded 2), Cluster 3: Regulation Oriented Public Systems (coded 3), Cluster 4: Low Supply and Low Performance Mixed Systems (coded 4), and Cluster 5: Supply and Performance Oriented Private Systems (coded 5; reference category). We utilize the two privately funded healthcare systems (i.e. the Insurance Model for KOP and the Supply and Performance Oriented Private Systems for RAW) as the reference group for several theoretical reasons. First, healthcare expenditures are important inputs in RAW’s cluster formations. In this respect, countries classified under the KOP Insurance Model and the RAW Supply and Performance Oriented Private Systems are quite similar. For instance, the United States, which appears in both the Insurance Model and the Supply and Performance Oriented Private Systems categorizations, leads all OECD countries in healthcare expenditure as a percentage of gross domestic product (GDP), while also experiencing some of the fastest rate of growth in healthcare spending (Reinhardt et al., 2004). Second, the KOP typology suggests that countries in the Insurance Model are culturally distinct and may favor a limited role of government compared to other healthcare systems, as reflected by their private financing and laissez-faire orientation toward the medical profession. Supply and Performance Oriented Private Systems in RAW are similar in terms of financing and access regulation. However, we also present all possible pairwise contrasts with Bonferroni corrections as a robustness check in Figures 3 (responsibility) and 4 (spending) of Appendix 1.
Country-level controls
We introduce two country-level controls that influence healthcare-related public attitudes: population aging and NCD burden (Kikuzawa et al., 2008). We draw these measures from the World Development Indicators Database (World Bank 2019). For population aging, we utilize the percentage of the population aged 65 and above (% of total population). This measure allows us to capture the degree to which a country is “graying.” For NCD burden, we include the percentage of deaths by NCDs (% of 30-year-olds who would die before age 70). This measure expands on prior studies to include disease burden from cardiovascular disease, cancer, chronic respiratory disease, as well as diabetes (e.g. Kikuzawa et al., 2008).
Individual-level controls
We control for a series of sociodemographic variables that may influence political attitudes about healthcare. Consistent with prior studies, we include the respondent’s age, age squared, educational attainment, employment status, gender, and income (e.g. Brady et al., 2016; Kikuzawa et al., 2008). Vulnerable groups, such as older people, women, and the unemployed, who may benefit from welfare policies are more likely to support greater government involvement in healthcare (Kikuzawa et al., 2008). We measure age in years, and we include a quadratic term to account for non-linear effects. We include educational attainment and gender as dummy variables. Our educational attainment variable is comprised of three categories—primary (reference group; coded as 0), secondary (coded as 1), and tertiary (coded as 2)—while male respondents are the reference group for gender (coded as 0). We measure employment status as a binary variable: unemployed (coded as 0) and employed (coded as 1). Finally, we include country-specific z scores of income to facilitate cross-national comparisons because they obviate the need for currency conversion to account for price differences across countries and inflation adjustments over time (Kwon and Curran, 2016). We also include a control variable for marital status to account for growing changes in traditional family formations that occur within the context of rapid population aging where people live much longer and thus are more likely to experience chronic illnesses. We measure it as a categorical variable with four levels: unmarried (coded as 0), married (includes civil partnerships; coded as 1), divorced (coded as 2), and widowed (coded as 3). We treat unmarried as the reference group.
Finally, we control for period effects between surveys, political party, and religious affiliation. We include political party and religious affiliation because they are associated with rising cross-national polarization in political attitudes, which could be associated with both institutional arrangements and support for government involvement in healthcare (Baldassarri and Bearman, 2007). We include a dummy for survey year (2016 is coded as 1; 2006 is the reference year). We measure political affiliation as a categorical variable with five levels: Left (coded as 0), center (coded as 1), right (coded as 2), no affiliation (coded as 3), and other (coded as 4). We include religious attendance as a 3-point scale: no attendance (coded as 0), low attendance (coded as 1), and high attendance (coded as 2).
In Table 3, we provide descriptive statistics for country- and individual-level covariates by each wave. Comparing the two healthcare system classifications, most of our sample resides in countries with the KOP National Health Model, which is characterized by universal funding via state budgets, medium state ownership of healthcare facilities, and a medium degree of autonomy for the medical profession. We observe a sizable shift of our sample away from residing in countries with the National Health Model by 2016. The minority of the pooled sample live in countries with Centralized Healthcare Model. This type of healthcare system has universal funding via state budgets, complete state ownership of healthcare facilities, and a low degree of autonomy for the medical profession.
Individual- and country-level descriptive statistics.
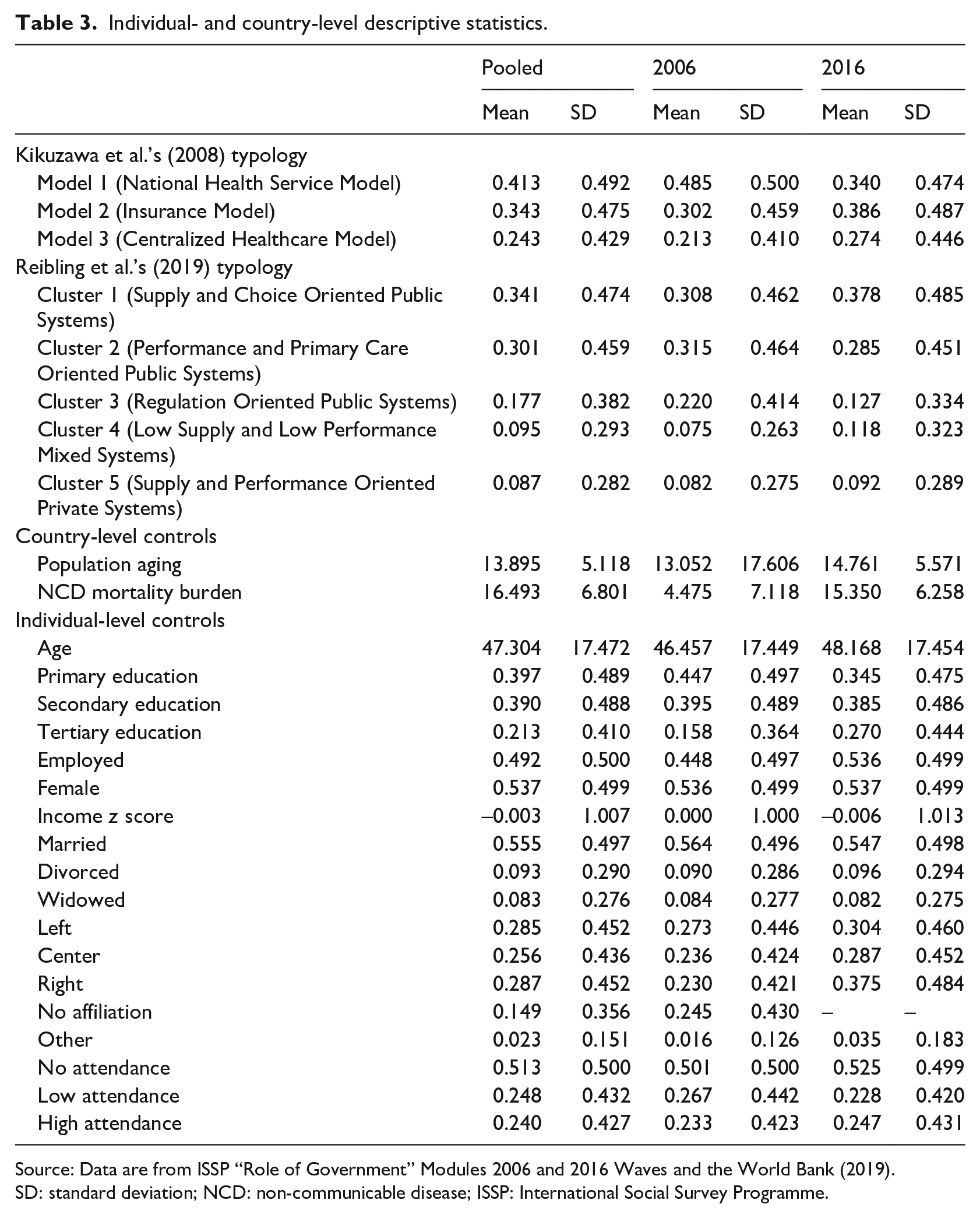
Source: Data are from ISSP “Role of Government” Modules 2006 and 2016 Waves and the World Bank (2019).
SD: standard deviation; NCD: non-communicable disease; ISSP: International Social Survey Programme.
In terms of the RAW typology, most of our pooled sample live in countries characterized by systems with medium to high financial resources (from public financing), high healthcare worker supply, little regulations on healthcare access, and free choice of specialists. These systems have the highest shares of GPs, but low performance in terms of prevention and quality of care. We see a shift in the sample in 2016 toward a larger percentage residing in countries with these types of healthcare systems. The minority of our pooled sample live in countries with Supply and Performance Oriented Private Systems. These systems are characterized by high supply due to high healthcare expenditures. Private and out-of-pocket financing plays a large role, and private and social insurance plans regulate access via mechanisms like deductibles (rather than national laws). They have medium to high levels of prevention and quality performance.
Analytical strategy
We utilize hierarchical linear modeling (HLM) to derive estimates of the association between healthcare systems on healthcare-related attitudes. Conceptually, we generate individual regression coefficients for each of the countries in our sample, which we then regress on country-level covariates. HLM allows us to simultaneously estimate both within- and between-group effects. In addition, the variance components and the intraclass correlation coefficient (ICC) further allow us to evaluate to what degree country-level variables account for the total variation between countries (Raudenbush and Bryk, 2002). The Akaike information criterion (AIC) and the Bayesian information criterion (BIC) indicate how well the model fits the data. In our case, we find that between-country variation accounts for roughly 12 and 11 percent of the total variation in individual political beliefs about responsibility and spending, respectively (F = 208.75, df1 = 25, df2 = 35,512; F = 143.14, df1 = 25, df2 = 35,507).
Despite their ubiquity in cross-national research, HLM has limitations. Estimates for Level 2 units and variance components require samples of at least 25 countries for linear models and substantially more for non-linear models (Bryan and Jenkins, 2016). Although our country samples for responsibility and spending meet this recommendation (N = 26 countries for both), we limit our specification to a random intercept design. We employ linear models, but as a robustness check, we include a non-linear modeling strategy.
Below, we outline the general form of our equations beginning with the individual-level equation and its notation

Public attitude scores (Y) for individual i in country j at time point t are a function of an intercept (β0), a N-k vector of individual-level controls (Xijk), and a grand residual term (R). R is normally distributed with a mean of zero and variance equal to σ2. Next, we outline our two country-level equations. Equation (2) presents country-level equation for the Kikuzawa et al. (2008) typology

The general form of the second-stage equation for the first typology specifies the intercept in individual-level equation as a function of random country intercepts (γ00), healthcare system (γ01 and γ02, Model 2, the Insurance Healthcare Model, is the reference group), population aging (γ03), NCD burden (γ04), and the national-level error term (U0jt).
Equation (3) presents the country-level equation for the Reibling et al. (2019) typology
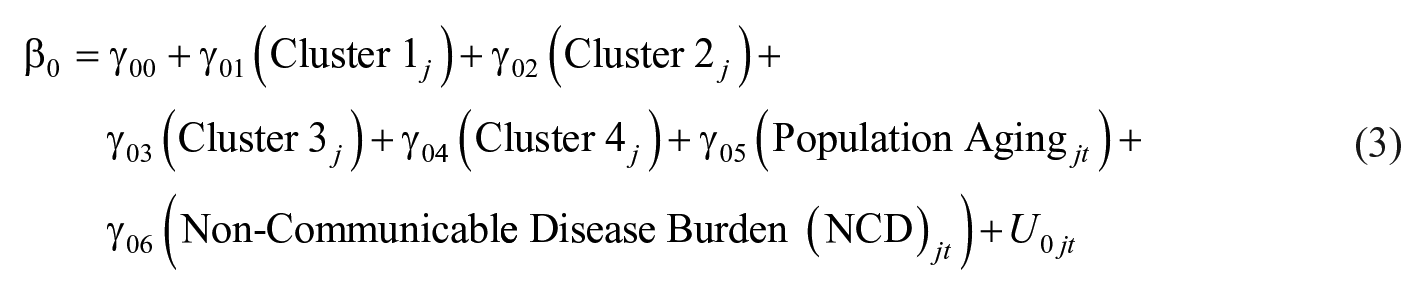
The general form of the second-stage equation for the second typology specifies the intercept in individual-level equation as a function of random country intercepts (γ00), healthcare system (γ01–γ04, Cluster 5, Supply and Performance Oriented Private Systems, is the reference group), population aging (γ05), NCD burden (γ06), and the national-level error term (U0jt). 5
We evaluate how strongly each of these independent variables is associated with healthcare-related public attitudes. Of particular interest for our purposes is how well they improve model fit (i.e. AIC and BIC) and explain the variation between countries once they are introduced into the model (i.e. ICC).
Results
In Table 4, we present estimates from HLM of individual-level political beliefs about government responsibility for providing healthcare. In Model 1, we provide a baseline model that illustrates the amount of the total variation that is due to residing in a particular country before introducing any country- or individual-level covariates. The average score for support for responsibility across 26 countries is 3.63, and about 12 percent of the total variation is due to residing in a particular country. This finding is consistent with past work that shows that support for greater government responsibility in healthcare is generally high, especially when compared with other welfare domains (Jensen and Naumann, 2016; Missinne et al., 2013; Wendt et al., 2009).
HLM regressions of attitudes about government responsibility in providing healthcare on type of healthcare system (N = 26).
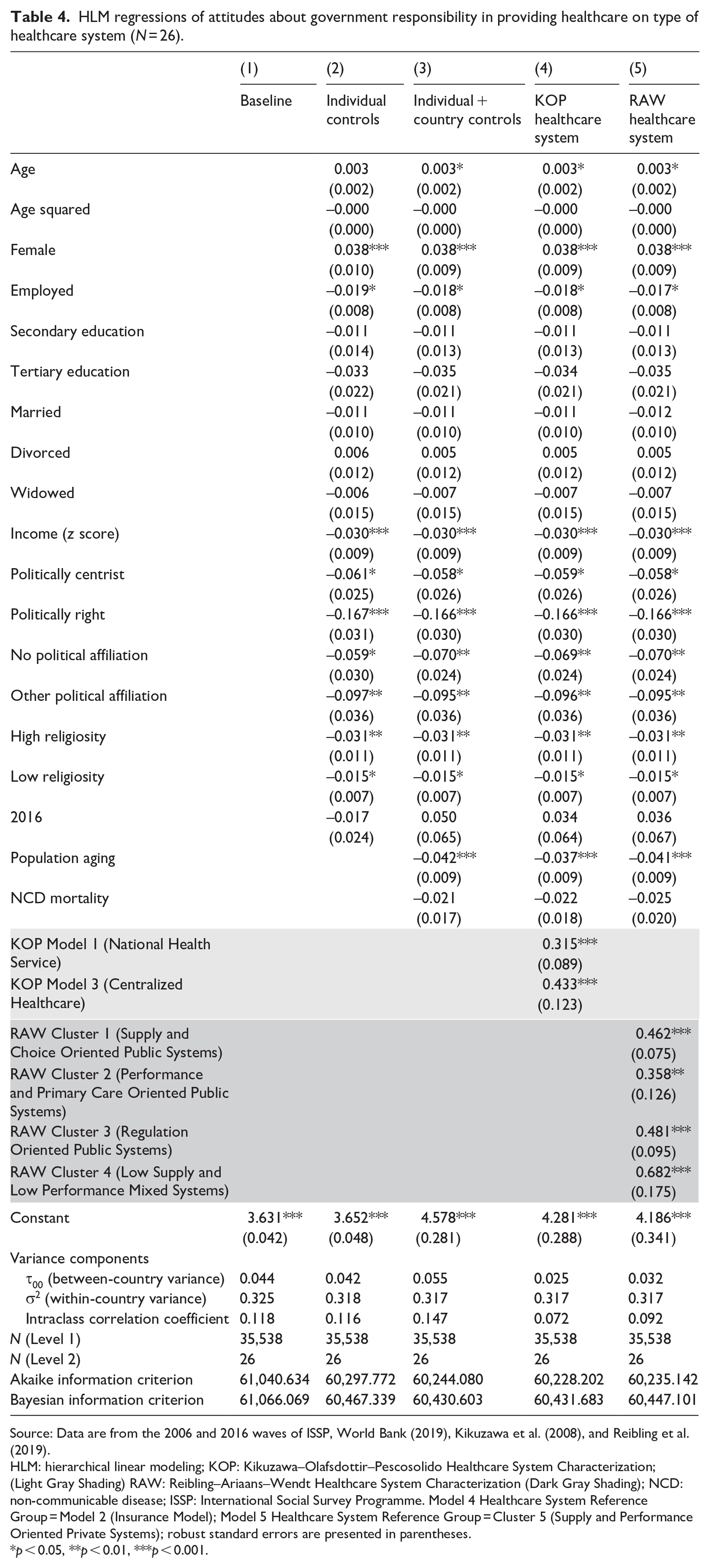
Source: Data are from the 2006 and 2016 waves of ISSP, World Bank (2019), Kikuzawa et al. (2008), and Reibling et al. (2019).
HLM: hierarchical linear modeling; KOP: Kikuzawa–Olafsdottir–Pescosolido Healthcare System Characterization; (Light Gray Shading) RAW: Reibling–Ariaans–Wendt Healthcare System Characterization (Dark Gray Shading); NCD: non-communicable disease; ISSP: International Social Survey Programme. Model 4 Healthcare System Reference Group = Model 2 (Insurance Model); Model 5 Healthcare System Reference Group = Cluster 5 (Supply and Performance Oriented Private Systems); robust standard errors are presented in parentheses.
p < 0.05, **p < 0.01, ***p < 0.001.
Figure 1 presents a plot of the coefficients from the KOP healthcare system categorization (Panel A from Model 4) and the RAW healthcare system categorization (Panel B from Model 5). Panel A shows that compared with those who reside in insurance model countries (reference group), individuals who live in both national health service countries (b = 0.315, p < 0.001) or centralized healthcare countries (b = 0.433, p < 0.001) are more likely to support greater government responsibility in healthcare. Panel B presents results from the RAW healthcare system typology. Individuals who reside in countries with supply and choice public systems (b = 0.462, p < 0.001), performance and primary care public systems (b = 0.358, p < 0.01), regulation public systems (b = 0.481, p < 0.001), and low supply and performance mixed systems (b = 0.682, p < 0.001) are more likely to support greater government responsibility in healthcare than those living in supply and performance private systems (reference group).
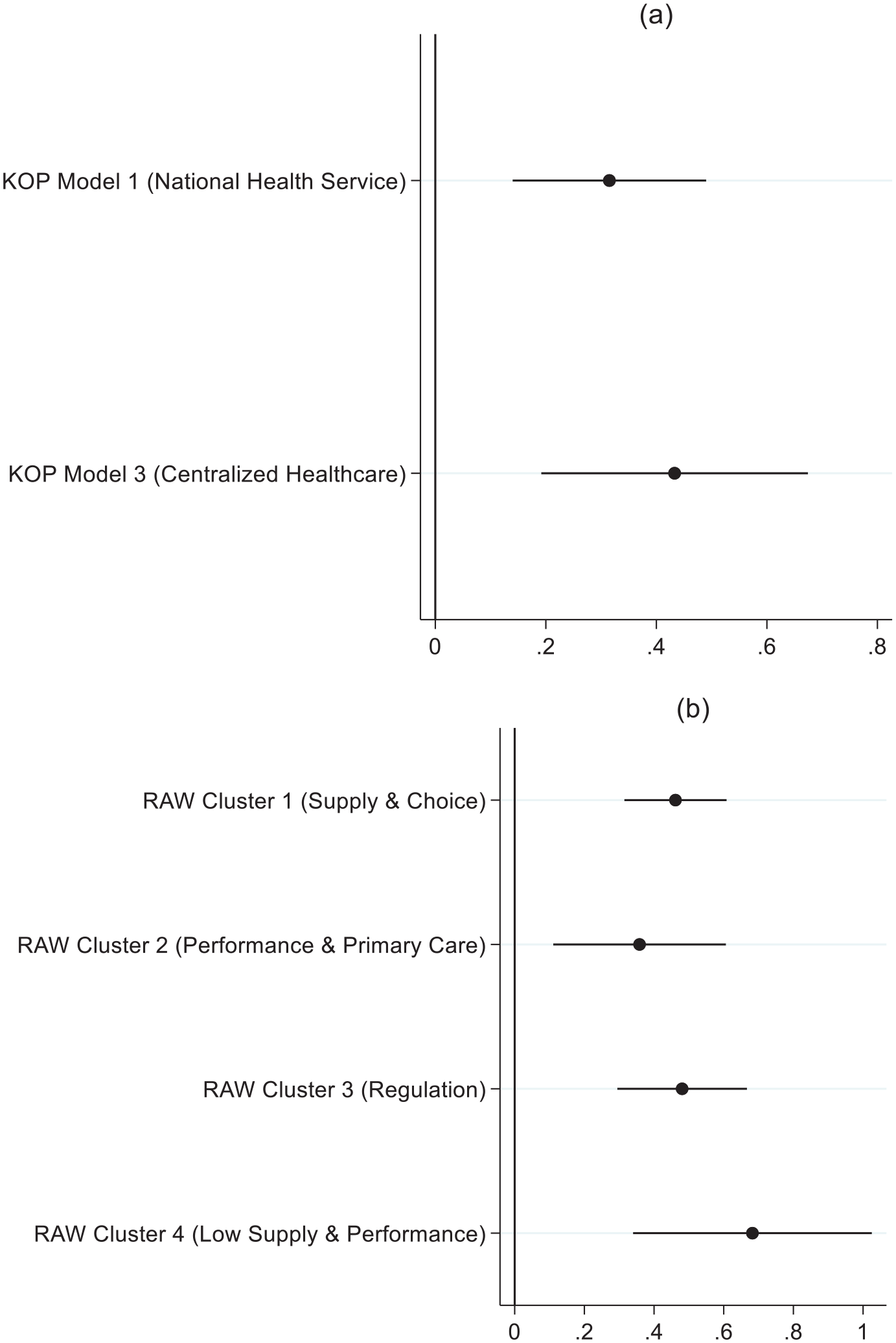
Coefficient plots from hierarchical linear modeling (HLM) regressions of attitudes about government responsibility in providing healthcare on type of healthcare system.
Results suggest some degree of overlap between the KOP and the RAW model. One area of convergence is that countries categorized as supply and performance private systems in the RAW typology and countries in the insurance model under the KOP typology (both are the reference categories for each model) are different compared to other categorizations in each respective typology. For example, when one looks at the key features involved in the overlap, state involvement and public financing come to the fore, suggesting a general association between greater state involvement and public financing and responsibility. Furthermore, the countries in the supply and performance private system categorization in the RAW typology are subsumed completely in the KOP typology insurance model categorization. An area of divergence is the difference in support between RAW low supply and performance healthcare systems and KOP centralized healthcare systems. There is an overlap in the countries in both categorizations (i.e. in both typologies, they are mainly post-Soviet countries). Both typologies show the largest positive association with government responsibility for these post-Soviet systems. However, in the RAW model, the coefficient is about 46 percent larger, despite the reference categories between the two being quite similar.
To gauge explanatory power, we turn to a comparison of the ICC and the goodness-of-fit statistics. We calculate the ICC decreases versus the baseline for the KOP and RAW models in Table 4. Addition of the KOP healthcare system categorization causes a large drop in the ICC (about 39%) versus baseline, suggesting that it explains quite a bit of the between-country variation in attitudes about responsibility. Substituting the RAW healthcare system categorization results in about a 22 percent drop in ICC versus baseline. The KOP healthcare system typology explains more of the between-country variation in attitudes about responsibility than does the RAW healthcare system typology. This finding is also supported by the AIC and BIC statistics, which show that the KOP model fits the data better than the RAW model.
The KOP categorization relies on characterizing healthcare systems by their institutional factors, which are presumed to impact public norms about the government’s role in healthcare. The RAW categorization also includes institutional aspects of healthcare systems, but health policy factors are an important input in the cluster analysis. These findings suggest that institutional categorizations alone may provide a stronger (and perhaps more parsimonious) association with public attitudes about government responsibility in healthcare. The addition of health policy factors does not appear to increase explanatory power above and beyond institutional factors. However, government responsibility speaks to function, not spending, preferences. The RAW typology’s integration of public health concerns and quality of healthcare system may have stronger implications for spending support.
Thus, in Table 5, we provide the results from HLM of individual-level political beliefs about government spending on healthcare. The baseline average score for support for spending across 26 countries is 4.07 and about 11 percent of the total variation is due to residing in a particular country (Model 1). Like the responsibility models, support is generally high for increased spending. Figure 2 provides the coefficients for the saturated models. Panel A presents the coefficients from the KOP healthcare system categorization (Model 4). Compared with those who reside insurance model countries, people who live in national health service (b = 0.287, p < 0.01) countries are more likely to support greater government spending on healthcare. There is no significant difference in support for those living in centralized healthcare countries versus insurance model countries.
HLM regressions of attitudes about government spending on healthcare on type of healthcare system.
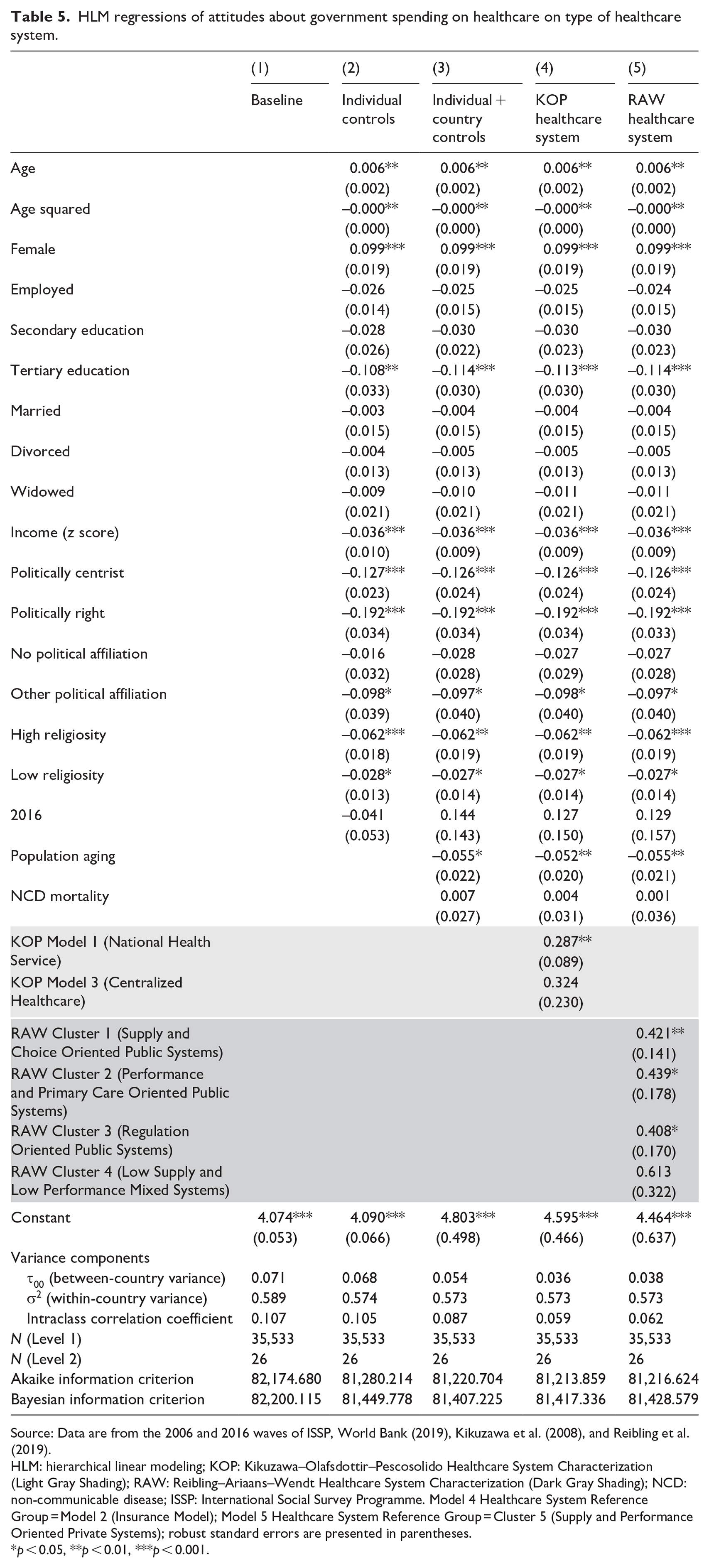
Source: Data are from the 2006 and 2016 waves of ISSP, World Bank (2019), Kikuzawa et al. (2008), and Reibling et al. (2019).
HLM: hierarchical linear modeling; KOP: Kikuzawa–Olafsdottir–Pescosolido Healthcare System Characterization (Light Gray Shading); RAW: Reibling–Ariaans–Wendt Healthcare System Characterization (Dark Gray Shading); NCD: non-communicable disease; ISSP: International Social Survey Programme. Model 4 Healthcare System Reference Group = Model 2 (Insurance Model); Model 5 Healthcare System Reference Group = Cluster 5 (Supply and Performance Oriented Private Systems); robust standard errors are presented in parentheses.
p < 0.05, **p < 0.01, ***p < 0.001.
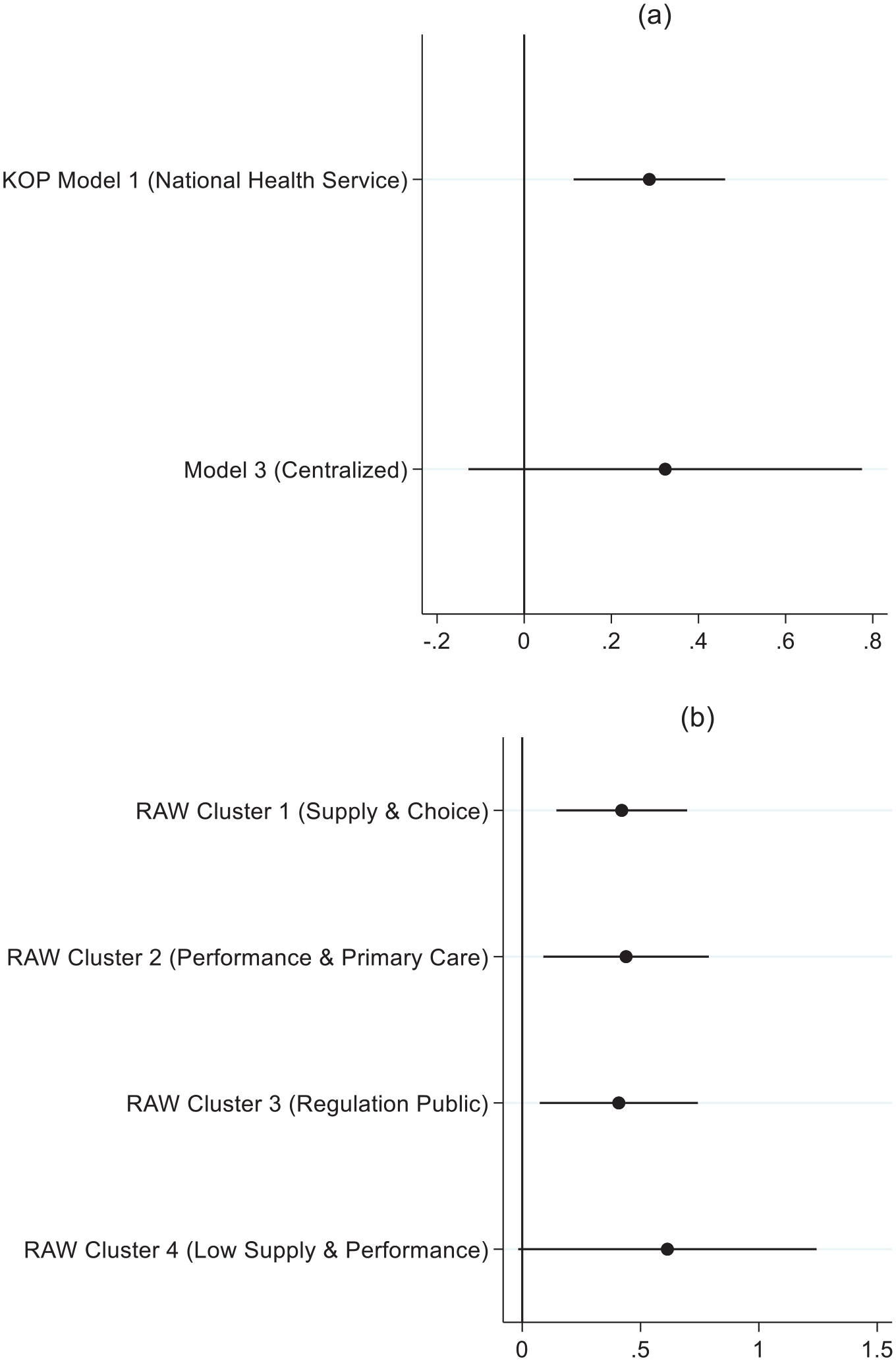
Coefficient plots from hierarchical linear modeling (HLM) regressions of attitudes about government spending on healthcare on type of healthcare system.
In Panel B, we provide the coefficients from the RAW healthcare system typology (Model 5). Individuals who reside in countries with supply and choice public systems (b = 0.421, p < 0.01), performance and primary care public systems (b = 0.439, p < 0.05), and regulation public systems (b = 0.408, p < 0.05) are more likely to support greater spending on healthcare than those living in supply and performance private systems (reference group). People who reside in countries with low supply and performance mixed healthcare systems show no significant difference in support for greater spending. This finding is like that observed in the KOP model with the centralized healthcare system as characterized by post-Soviet countries.
Unlike the responsibility models, the results for spending display less overlap. As noted in the responsibility models, there exists an overlap between the KOP insurance model countries and the RAW supply and performance private system countries, as well as the post-Soviet centralized healthcare systems in KOP and the low supply and performance mixed healthcare systems in RAW. However, no such comparison exists between KOP national health service countries and any one category in the RAW typology. It could be the case that each typology is capturing distinct aspects of healthcare systems that are associated with support for spending.
Table 5 also allows us to calculate the percent ICC reduction versus the baseline for the KOP and RAW models. Like the responsibility models, the addition of the KOP healthcare system typology causes a large drop in ICC versus baseline (about 45%). When we compare this to the ICC decrease with the RAW healthcare system typology in the model (about 42%), we observe that KOP once again edges out RAW. However, the margin is much smaller for the support for spending models than for the responsibility models. The AIC and BIC statistic differences are also marginal.
Other concerns
Our results provide evidence that type of healthcare system matters for understanding healthcare-related public attitudes. However, our results may be influenced by several factors, including modeling strategy and utilizing pooled survey waves. We address these factors in the sections that follow.
Alternative modeling strategy
Our main models rely on HLM to estimate results. However, it is unclear whether these findings are an artifact of the choice of modeling strategy. 6 In Tables 6 and 7 of Appendix 1, we estimate results for responsibility and spending, respectively, using a multilevel mixed effects generalized linear model (GLM) with an ordinal family and a logit link as a robustness check. We present the baseline model and the two healthcare system typology models for each of the dependent variables. Coefficients are reported as odds ratios. Our results do not vary substantially from the linear models in terms of significant associations or ICC reduction trends for our models. Thus, they appear robust to two analytic strategies.
Time trends
The RAW typology utilizes 2016 OECD health data in its categorizations. Since we pool the 2006 and 2016 waves for our main analyses, it may be the case that the RAW typology better captures more contemporaneous dynamics. Thus, in Table 8 of Appendix 1, we estimate each model using 2016 data only. We note that the country-level N on these models is 19, and thus, results from them should be interpreted with caution. Models 1 and 2 present the results for responsibility as the outcome. Results are similar to those using the pooled waves. Compared with those in KOP insurance model countries, respondents in national health service and centralized healthcare countries are more likely to support greater government responsibility in healthcare. RAW results are similar, as well, with one exception: the significant association between responsibility and residing in a low supply and performance mixed healthcare system country does not exist in the 2016 wave. The ICC, AIC, and BIC statistics also are similar to the main model for responsibility: the KOP model shows a larger reduction in ICC, AIC, and BIC than the RAW model.
Models 3 and 4 provide the results for spending as the dependent variable. Again, results are similar to the main model using the pooled data with a couple of exceptions: for the KOP model, citizens in countries with centralized healthcare systems now are significantly more likely to support greater spending. A parallel exists in the RAW model with citizens residing in low supply and performance mixed system countries. They are significantly more likely to support more spending in the 2016 wave. The ICC, AIC, and BIC statistics are similar to the main model for spending, as well. Thus, our findings do not appear to be an artifact of pooling the 2016 wave with one collected a decade earlier.
U.S. exceptionalism?
The United States is distinct and exceptional in that it leads all OECD countries in healthcare expenditure as a percentage of GDP while also experiencing some of the fastest rate of growth in healthcare spending (Reinhardt et al., 2004). In this sense, it is an outlier that may influence the associations between type of healthcare system and public attitudes. Thus, in Table 9 of Appendix 1, we present results with a separate country dummy for the United States. Results are similar to the main model, and the parameterized indicator variable for the United States does not bear a significant association with either responsibility or spending. U.S. exceptionalism does not appear to be driving the results.
Contrasts
Significant associations may be an artifact of reference group choices. Thus, we present results with all contrasts in Figures 3 and 4 of Appendix 1 for responsibility and spending, respectively. We utilize Bonferroni corrections to account for multiple comparisons. In Figure 3 of Appendix 1, Panel A, we present all the pairwise contrasting predictive marginal effects for the KOP healthcare system on responsibility. 7 Here, the comparison between national health service countries and centralized healthcare countries fails to reach significance. Thus, the significant comparisons are between insurance model countries and all others, as reflected in the main model. Panel B provides all the pairwise contrasting predictive marginal effects for the RAW healthcare system model on responsibility. This panel illustrates no significant pairwise contrasting marginal effects for any of the clusters beyond that observed in the main model. As in the main model, these results suggest that the most salient differences are in the comparison of supply and performance private systems with the remaining clusters.
In Figure 4 of Appendix 1, we present all healthcare system comparisons for the spending variable. In Panel A, we present all the pairwise contrasting predictive marginal effects for the KOP healthcare system model on spending. The results reaffirm those in the main model—only the comparison between insurance model countries and national health service countries shows a significant association with spending. Panel B presents all the pairwise contrasting predictive marginal effects for the RAW healthcare system model on spending. After applying the Bonferroni correction, the only comparison that remains significantly associated with spending is that of Cluster 5 (Supply and Performance Oriented Private Systems) with Cluster 1 (Supply and Choice Oriented Public Systems). Thus, we can be sure of robust contrast between those two systems for spending.
Discussion
The COVID-19 pandemic has offered an unprecedented opportunity to rethink healthcare systems (Sturmberg et al., 2020). To rally broad public support for changes to healthcare systems, researchers and policy makers must understand what the public has come to expect about healthcare, as well as the institutional arrangements around healthcare that set the “rules of the game” (Beckfield et al., 2015: 5; Kikuzawa et al., 2008). These “rules of the game” have the potential to constrain future policy proposals. For example, people living in countries with high cost barriers tend to be more tolerant of healthcare inequality, suggesting that those exposed to greater inequality tend to be more accepting of it as the status quo (Immergut and Schneider, 2020). Thus, healthcare institutions and the historical and policy-related normative arrangements that they reflect may help or hinder any attempts to rethink healthcare systems or public health initiatives.
These institutional “rules” are arguably similar to those that dictate welfare state spending because healthcare is embedded in the welfare state. However, a newer typology, based on health policy perspectives, captures factors that are distinct about healthcare (Reibling et al., 2019). This newer typology contends that the “rules of the game” are ever shifting because of the distinct nature of healthcare vis-à-vis other areas of the welfare state (Bambra, 2005; Reibling et al., 2019). In this article, we examined which perspective better captures the association between healthcare systems and public attitudes about government responsibility in healthcare and healthcare spending. Our results indicate that traditional welfare state conceptions of healthcare systems fit the data better for these outcomes, which are related to the normative value of government involvement in healthcare provision. Thus, institutional–comparative perspectives of healthcare rooted in historical path dependencies may better explain how citizens view the guiding principles on which their healthcare system is founded (Kohl and Wendt, 2004; Missinne et al., 2013). This finding illustrates the importance of historical and cultural legacies that shape the guiding principles of political attitudes. The institutionalization of certain aspects of healthcare set norms that center on issues like the unfairness of healthcare inequalities, the right to healthcare access, and notions of health justice (Immergut and Schneider, 2020). Respondents in countries with healthcare systems that have greater state involvement and rely more on public financing report greater support for government responsibility in healthcare. The results for both the KOP and the RAW healthcare typologies support this general finding. When it comes to support for government spending in healthcare, results are similar.
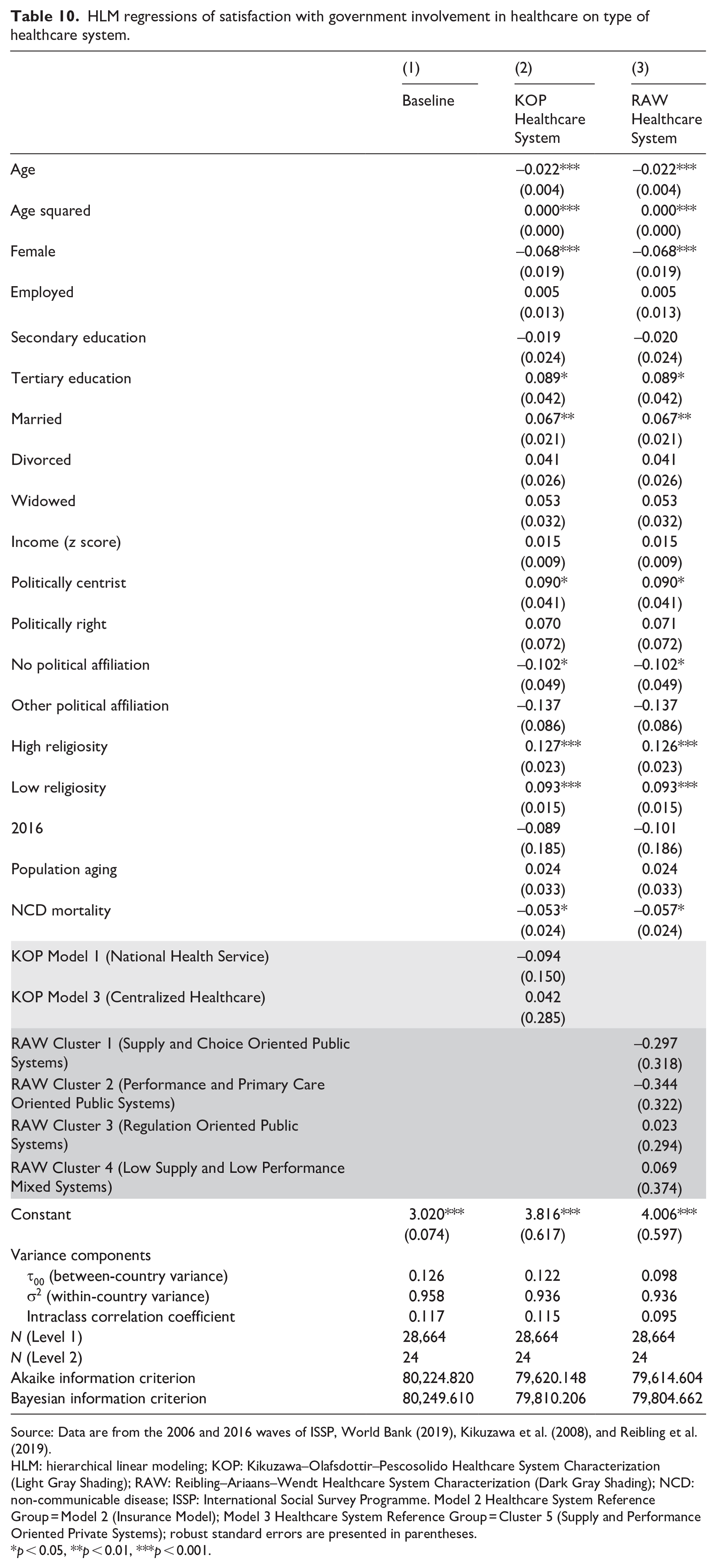
Our findings provide insight into the wider welfare state, especially related to social services, which was largely excluded from prevailing welfare state debates (Bambra, 2005; Reibling et al., 2019). They suggest that traditional welfare state approaches may describe the associations between social services and normative public attitudes (i.e. government responsibility and spending) well enough. We estimated the association between the traditional typology and evaluative public attitudes (i.e. how satisfied people are with their government’s involvement in healthcare) to examine this possibility. Those results (presented in Table 10 of Appendix 1) suggest that the newer typology explains a larger portion of the between-country variance (see ICC) than the traditional typology. These results should be interpreted with caution because the county-level N is lower than the recommended N of 25. It may be the case that the quality and performance measures represented in the Reibling et al. (2019) typology have a stronger association with evaluative attitudes. Indeed, some work proposes that meso-level heterogeneity in social programs within the large institutional conceptions of the welfare state may have more explanatory power for understanding public support for welfare than traditional welfare state categorizations (Laenen, 2018). Evaluative outcomes like satisfaction may capture some of this heterogeneity as they ask respondents to rate how well programs play out in practice. However, data limitations prevent us from robustly examining that association.
A limitation of the study is that we only examined one institutional–comparative typology. Several different typologies that use traditional welfare state perspectives exist, as well as conceptualizations that draw on continuous, rather than categorical, variables to measure type of healthcare system (e.g. Missinne et al., 2013; Wendt and Kohl, 2010). Different institutional–comparative typologies may produce different results. Thus, future work could compare multiple institutional–comparative typologies and measures with the new typology.
Institutional “rules of the game” also may impact health disparities (Beckfield et al., 2015), and the public views disparities in healthcare access and quality as unfair (Jensen and Petersen, 2017; von dem Knesebeck et al., 2016). We did not examine the association between healthcare system typologies and public attitudes about health inequities. It may be the case that the Reibling et al. (2019) typology is strongly associated with perceptions about unfairness of health inequities, as it accounts for the shifting “rules of the game” (i.e. shifting quality and performance). The newer typology may be correlated with population health disparities, which may influence public perceptions about health justice (Rydland et al., 2020). Future work may examine the association between typology and public views of health disparities.
Examining the validity of healthcare system typologies is an important concern in comparative research for several reasons. First, scholars note that “there is little consensus in terms of how countries group together, which types of healthcare regimes exist, or which health outcomes are of relevance” (Shore et al., 2019: 441). Our study addresses several of these gaps by leveraging HLM to compare how political attitudes surrounding the role and spending of governments on healthcare relate to two competing typologies of healthcare systems. In doing so, we provide more guidance for studies moving forward when normative public attitudes are the outcome of interest. Second, we believe our approach also extends beyond measurement evaluation. Our findings illustrate that while novel threats to public health often require flexibility and the rapid implementation of new health initiatives, public attitudes about the appropriate role of government are constrained by historical, cultural, and institutional legacies, and thus are likely to act as significant barriers to rapid health policy regulations.
Footnotes
Appendix 1
HLM regressions of satisfaction with government involvement in healthcare on type of healthcare system.
| (1) | (2) | (3) | |
|---|---|---|---|
| Baseline | KOP Healthcare System | RAW Healthcare System | |
| Age | –0.022*** | –0.022*** | |
| (0.004) | (0.004) | ||
| Age squared | 0.000*** | 0.000*** | |
| (0.000) | (0.000) | ||
| Female | –0.068*** | –0.068*** | |
| (0.019) | (0.019) | ||
| Employed | 0.005 | 0.005 | |
| (0.013) | (0.013) | ||
| Secondary education | –0.019 | –0.020 | |
| (0.024) | (0.024) | ||
| Tertiary education | 0.089* | 0.089* | |
| (0.042) | (0.042) | ||
| Married | 0.067** | 0.067** | |
| (0.021) | (0.021) | ||
| Divorced | 0.041 | 0.041 | |
| (0.026) | (0.026) | ||
| Widowed | 0.053 | 0.053 | |
| (0.032) | (0.032) | ||
| Income (z score) | 0.015 | 0.015 | |
| (0.009) | (0.009) | ||
| Politically centrist | 0.090* | 0.090* | |
| (0.041) | (0.041) | ||
| Politically right | 0.070 | 0.071 | |
| (0.072) | (0.072) | ||
| No political affiliation | –0.102* | –0.102* | |
| (0.049) | (0.049) | ||
| Other political affiliation | –0.137 | –0.137 | |
| (0.086) | (0.086) | ||
| High religiosity | 0.127*** | 0.126*** | |
| (0.023) | (0.023) | ||
| Low religiosity | 0.093*** | 0.093*** | |
| (0.015) | (0.015) | ||
| 2016 | –0.089 | –0.101 | |
| (0.185) | (0.186) | ||
| Population aging | 0.024 | 0.024 | |
| (0.033) | (0.033) | ||
| NCD mortality | –0.053* | –0.057* | |
| (0.024) | (0.024) | ||
| KOP Model 1 (National Health Service) | –0.094 | ||
| (0.150) | |||
| KOP Model 3 (Centralized Healthcare) | 0.042 | ||
| (0.285) | |||
| RAW Cluster 1 (Supply and Choice Oriented Public Systems) | –0.297 | ||
| (0.318) | |||
| RAW Cluster 2 (Performance and Primary Care Oriented Public Systems) | –0.344 | ||
| (0.322) | |||
| RAW Cluster 3 (Regulation Oriented Public Systems) | 0.023 | ||
| (0.294) | |||
| RAW Cluster 4 (Low Supply and Low Performance Mixed Systems) | 0.069 | ||
| (0.374) | |||
| Constant | 3.020*** | 3.816*** | 4.006*** |
| (0.074) | (0.617) | (0.597) | |
| Variance components | |||
| τ00 (between-country variance) | 0.126 | 0.122 | 0.098 |
| σ2 (within-country variance) | 0.958 | 0.936 | 0.936 |
| Intraclass correlation coefficient | 0.117 | 0.115 | 0.095 |
| N (Level 1) | 28,664 | 28,664 | 28,664 |
| N (Level 2) | 24 | 24 | 24 |
| Akaike information criterion | 80,224.820 | 79,620.148 | 79,614.604 |
| Bayesian information criterion | 80,249.610 | 79,810.206 | 79,804.662 |
Source: Data are from the 2006 and 2016 waves of ISSP, World Bank (2019), Kikuzawa et al. (2008), and Reibling et al. (2019).
HLM: hierarchical linear modeling; KOP: Kikuzawa–Olafsdottir–Pescosolido Healthcare System Characterization (Light Gray Shading); RAW: Reibling–Ariaans–Wendt Healthcare System Characterization (Dark Gray Shading); NCD: non-communicable disease; ISSP: International Social Survey Programme. Model 2 Healthcare System Reference Group = Model 2 (Insurance Model); Model 3 Healthcare System Reference Group = Cluster 5 (Supply and Performance Oriented Private Systems); robust standard errors are presented in parentheses.
p < 0.05, **p < 0.01, ***p < 0.001.
Acknowledgements
We wish to thank the UC–Riverside Political Economy Seminar participants for their helpful feedback on an earlier draft.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.