
Abstract
Background:
Few studies investigated the long-term mental health outcome in culturally different post-conflict settings. This study considers two surveys conducted in Kosovo 8 years after the Balkans war and in Rwanda 14 years after the genocide.
Methods:
All participants (n = 864 in Kosovo; n = 962 in Rwanda) were interviewed using the posttraumatic stress disorder (PTSD) and major depressive episode (MDE) sections of the Mini International Neuropsychiatric Interview (MINI) and the Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36).
Results:
Proportions of participants who met diagnostic criteria for either PTSD or MDE were 33.0% in Kosovo and 31.0% in Rwanda, with co-occurrence of both disorders in 17.8% of the Rwandan sample and 9.5% of the Kosovan sample. Among patients with PTSD, patterns of symptoms significantly differed in the two settings, with avoidance and inability to recall less frequent and sense of a foreshortened future and increased startle response more common in Rwanda. Significant differences were also observed in patients with MDE, with loss of energy and difficulties concentrating less frequent and suicidal ideation more common in Rwanda. Comorbid PTSD and MDE were associated with decreased SF-36 subjective mental and physical health scores in both settings, but significantly larger effects in Kosovo than in Rwanda.
Conclusion:
Culturally different civilian populations exposed to mass trauma may differ with respect to their long-term mental health outcome, including comorbidity, symptom profile and health perception.
Introduction
Since the Second World War, at least 22 interstate conflicts and 240 civil conflicts occurred worldwide. Globally, it is estimated that 25 million non-combatant civilians were killed and 40 million forcefully displaced during this time period. Internal conflicts, which account for a large part of war-related human suffering, usually arise on the basis of lasting ethnic tensions in limited geographic territories (Esteban, Mayoral, & Ray, 2012). Such conflicts may involve the destruction of socioeconomic and health-care systems. These situations constitute complex emergencies in which mental health becomes an important public health issue (Mollica et al., 2004).
Many epidemiological studies reported prevalence rates of psychiatric disorders, such as posttraumatic stress disorder (PTSD) and depression, among civilian populations in different post-conflict countries, for example, Cambodia, former Yugoslavia or Sudan (Ayazi, Lien, Eide, Ruom, & Hauff, 2012; de Jong, Komproe, & Van Ommeren, 2003; Morina et al., 2013; Priebe et al., 2010). However, few studies compared the frequencies of specific symptoms and addressed comorbidity patterns across different settings. Psychological responses to collective traumatic events are complex phenomena and involve, among other factors, social and cultural dimensions (Kroll, 2003). Ethnocultural variables interact in shaping the perception, experience, clinical expressions and treatment responses to trauma (Marsella, 2010). The robustness of PTSD as a distinct diagnostic category has been questioned (Summerfield, 2001), and its cross-cultural validity has been debated as part of the revision process that led to the recently published Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5) (Friedman, Resick, Bryant, & Brewin, 2011; Hinton & Lewis-Fernandez, 2011). A better understanding of similarities and differences in symptom and comorbidity patterns in war-affected civilian populations might orient interventions in the post-conflict reconstruction phase. According to the guidelines for the treatment of PTSD, recommended therapeutic approaches indeed differ as a function of the most prominent symptoms, as well as psychiatric comorbidity (Foa, Davidson, & Frances, 1999).
Because methodological biases might limit the validity of cross-national comparisons, it is of paramount importance to use similar methods and measures across settings. In a systematic meta-analysis addressing the prevalence of PTSD and depression in the refugee and mental health field, not less than 21 different measures were reported for PTSD. Large inter-survey variability was associated with methodological factors, such as sample size, sampling method, diagnostic time frame and time elapsed since the conflict (Steel et al., 2009).
Kosovo and Rwanda share dramatic recent histories of collective violence and exposure of civilians to traumatic events. However, the Balkans region of Europe and Eastern Africa have little in common from an ethnocultural perspective. This study was based on two large surveys conducted in Kosovo 8 years after the war and in Rwanda 14 years after the genocide, using the same assessment tools. Whereas the prevalence of PTSD and major depressive episode (MDE) has been documented earlier (Eytan, Guthmiller, Durieux-Paillard, Loutan, & Gex-Fabry, 2011; Munyandamutsa, Mahoro Nkubamugisha, Gex-Fabry, & Eytan, 2012), this article focuses on similarities and differences between Kosovo and Rwanda regarding PTSD and MDE symptom presentation, comorbidity patterns and perceived health.
Methods
Setting and study design
Rwanda
In the spring of 1994, Rwandans endured a cataclysmic civil war and genocide. In 100 days, almost 1 million people perished and approximately 2 million people fled to neighboring countries, mainly Congo and Burundi. The genocide followed years of ethnic tensions and conflict between the Tutsi minority and the Hutu majority. Most of the country’s infrastructures and institutions were destroyed. Rwanda is a country of approximately 11 million inhabitants. Since 2006, the country is divided into five administrative provinces: Northern, Eastern, Southern, Western and Kigali Province (location of the capital) (Hagengimana, Hinton, Bird, Pollack, & Pitman, 2003).
Kosovo
In 1989, following decades of inter-ethnic tensions, the regional special autonomous status of Kosovo within the province of Serbia in the Federal Republic of Yugoslavia was drastically reduced. During the 1990s, the political situation worsened, with increasing cultural oppression and ethnic repression against the Albanian population. By 1998, the conflict turned into a guerrilla war, resulting in more than 1 million displaced civilians. On 17 February 2008, the parliament of Kosovo declared independence, provoking mixed international reactions. The population of Kosovo is about 2.2 million, with approximately 90% of ethnic Albanians (Eytan et al., 2011).
Rwanda and Kosovo surveys
The Rwanda survey was conducted 14 years after the genocide over a 3-month period in 2008 (Munyandamutsa et al., 2012). A total of 1000 subjects were interviewed, and 962 participants with complete data were included in this study. The Kosovo survey was conducted during a 2-month period in 2007, about 8 years after the peak of the conflict (Eytan et al., 2011). A total of 864 participants were interviewed and included in this study. Sampling procedures differed between the two surveys. For Rwanda, in each of the five provinces, two districts were selected: one urban district (the administrative center of the province) and one rural district (simple random sampling), except for the exclusively urban Kigali province. In each of the 10 districts, two sectors were randomly selected. A number of households proportional to the population in each sector were randomly selected. Interviews were conducted with a single member of each household, who was present at the time of the survey. When several household members were eligible, the participant was randomly selected. For Kosovo, households from eight municipalities were randomly selected from a list of families that included at least one person who had sought asylum in Switzerland and returned to Kosovo by April 2001. All adult household members, both returnees and people who had stayed in Kosovo during the war, were invited to participate.
None of the samples could be considered as representative of the country’s general population. However, conflict-exposed civilians aged 16 years or more, with no mental impairment and fluent in the local language (Kinyarwanda and Albanian, respectively) were interviewed in both Rwanda and Kosovo. Psychometric instruments and translation procedures were the same in the two settings, and surveyors received comparable training and instructions. The surveys were, respectively, supported by the Rwanda Ministry of Health and the International Organization for Migrations (IOM).
Ethics
The Rwanda project was approved by the National Ethics Committee of the Republic of Rwanda. In the absence of a research ethics committee in Kosovo at the time of the survey, the Kosovo project was approved by the Ethics Committee of the Geneva University Hospitals. On both sites, participants received oral and written information and gave informed consent for participation.
Instruments
PTSD and MDE diagnoses (categorical) were assessed with the appropriate sections of the Mini International Neuropsychiatric Interview (MINI). The Albanian version of the MINI was used in Kosovo (Morina & Ford, 2008). In Rwanda, the instrument was translated locally into the official language, Kinyarwanda. The MINI is a standardized, structured diagnostic interview designed conjointly in the United States and Europe to assess psychiatric diagnoses according to Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) and International Classification of Diseases, 10th Revision (ICD-10) criteria. It was tested against the Structured Clinical Interview for Diagnostic and Statistical Manual of Mental Disorders, Third Edition, Revised (DSM-III-R) (SCID) and the Composite International Diagnostic Interview for ICD-10 (CIDI) and found to be reliable and valid (Sheehan et al., 1998). It is short and can be administered by non-mental health professionals. The MINI is routinely used in a wide variety of cultures and settings, including for research purposes in Africa and the Balkans.
The PTSD section of the MINI starts with two screening questions investigating exposure to one or more potentially traumatic events and re-experience of these events in a distressing way: ‘Have you ever experienced or witnessed or had to deal with an extremely traumatic event that included actual or threatened death or serious injury to you or someone else?’ and ‘During the past month, have you re-experienced the event in a distressing way (i.e. dreams, intense recollections, flashbacks or physical reactions)?’ If answers are positive to these two questions, the instrument explores three clusters of PTSD symptoms (avoidance, hyperarousal, impaired functioning). For the first question, surveyors read a list of potentially traumatic events adapted from the first part of the Harvard Trauma Questionnaire (HTQ) (Mollica et al., 1992).
The MDE section of the MINI starts with two screening questions investigating depressed mood and loss of interest or pleasure: ‘Have you been consistently depressed or down, most of the day, nearly every day, for the past two weeks?’ and ‘In the past 2 weeks, have you been less interested in most things or less able to enjoy the things you used to enjoy most of the time?’ If the answer is positive to at least one question, the instrument explores seven other MDE symptoms.
Self-perceived physical and mental health was assessed using the Medical Outcomes Study 36-Item Short-Form Health Survey (SF-36), which considers a 4-week time frame for most questions (Ware & Sherbourne, 1992). The SF-36 was translated into several languages, including Albanian, and its cultural validity has been assessed in different countries. It was locally translated into Kinyarwanda for the purpose of this study, using a translation and back-translation method (as for the MINI) (Gjersing, Caplehorn, & Clausen, 2010). Some items pertaining to physical activities that are uncommon outside Western countries had to be adapted, as recommended in the literature (Wagner et al., 1998). SF-36 components were computed according to a three-step procedure (Leplège, 2001). Two continuous summary scores (physical component summary (PCS) score and mental component summary (MCS) score) were calculated as norm-based scores so that values 10 points below or above 50 represent differences of 1 standard deviation from average values in a US reference sample.
Both in Rwanda and in Kosovo, surveyors were recruited among psychologists, social workers and physicians with a special interest in mental health. All were trained during ad hoc workshops. Because of a high percentage of illiteracy, especially in rural areas, questionnaires were usually read aloud in both sites.
Statistics
Study samples were compared with the chi-squared test for categorical variables and the Mann–Whitney U test for continuous variables. The association of PTSD and MDE diagnoses was assessed with contingency tables and odds ratios (ORs). When testing PTSD and MDE symptoms for differences between samples, a Bonferroni correction for multiple tests was considered (i.e. significance level was divided by the number of tested symptoms). The Breslow–Day test was used to test the homogeneity of ORs in stratified 2 × 2 tables. Analysis of variance (ANOVA) models were used to investigate whether SF-36 dimensions (PCS and MCS) differed between studies (Kosovo vs Rwanda) and according to PTSD and/or MDE diagnoses (four categories), taking into account a possible interaction. Adjustment variables were sex, age group (10-year intervals), education (three levels) and their interactions with the study group. Planned contrast analyses considered the hypothesis that diagnosis effects would be independent of setting (e.g. differences between respondents with neither PTSD nor MDE and the ones with PTSD and comorbid MDE would be the same in Rwanda and Kosovo). Statistics were computed using SPSS version 20 (IBM Corporation, Armonk, NY, USA). All tests were two-tailed, with significance level at .05.
Results
Sample description
Sociodemographic characteristics of the Rwanda and Kosovo samples are provided in Table 1. Respondents were predominantly female (56.6% in Kosovo; 58.9% in Rwanda). They were significantly older in Kosovo than in Rwanda (median age 36 years, range 16–89 years in Kosovo; median age 33 years, range 16–108 years in Rwanda; p = .004), with a twofold higher proportion of subjects aged 65 years or more in Kosovo (11.7% vs 5.6%). Education level was significantly higher in the Kosovan than in the Rwandan sample (higher than primary level, 37.1% vs 20.3%).
Characteristics of respondents in the Kosovo and Rwanda surveys.
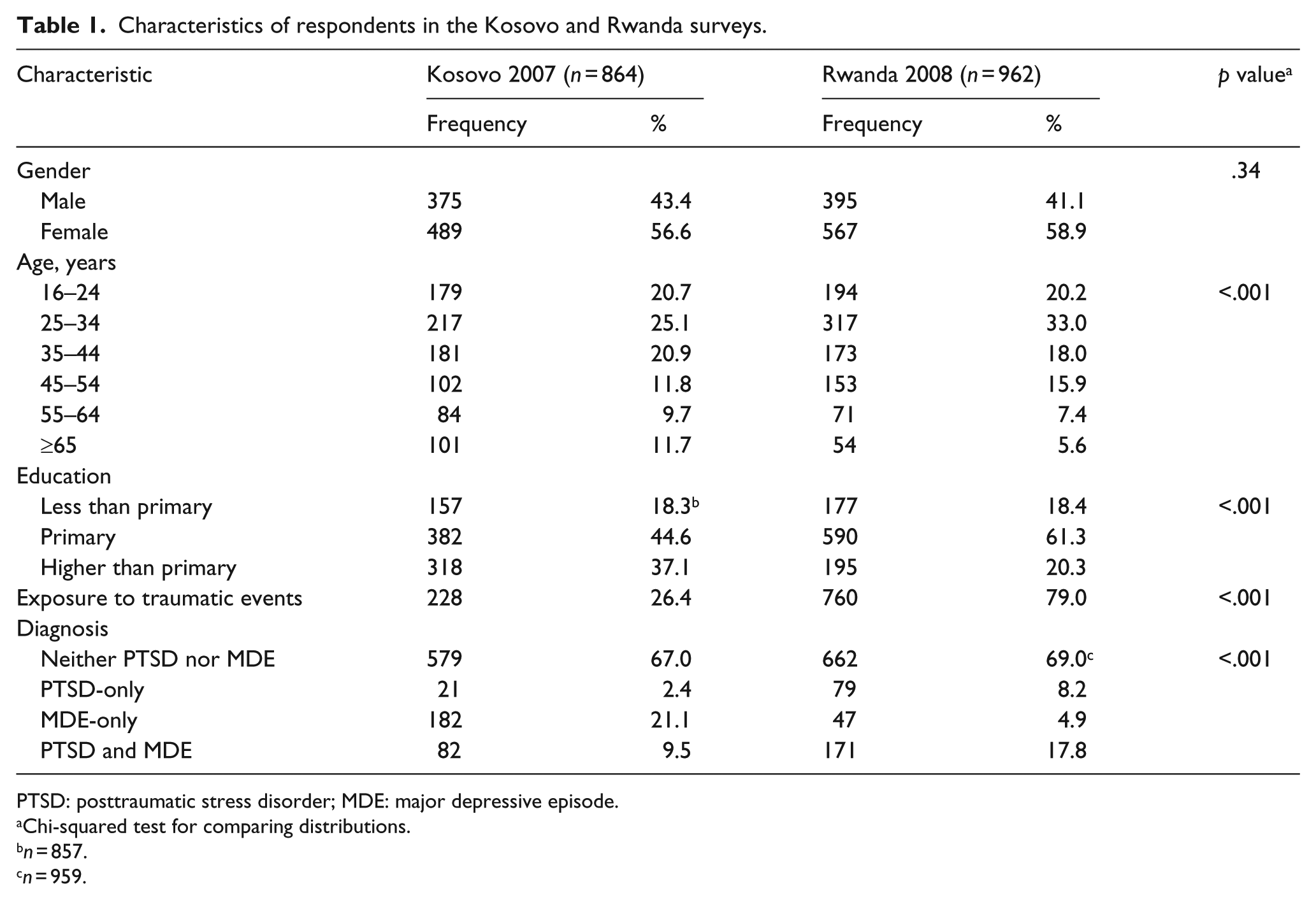
PTSD: posttraumatic stress disorder; MDE: major depressive episode.
Chi-squared test for comparing distributions.
n = 857.
n = 959.
PTSD and MDE diagnoses
Exposure to traumatic events (first necessary criterion for PTSD in the MINI) was significantly more frequent in Rwanda than in Kosovo (79.0% vs 26.4%). PTSD criteria were also more frequently met in Rwanda, where proportions of participants with PTSD-only (8.2% vs 2.4%) or comorbid PTSD and MDE (17.8% vs 9.5%) exceeded the ones in Kosovo. In contrast, MDE-only was more frequent in Kosovo than in Rwanda (21.1% vs 4.9%). About one-third of participants in each country met diagnostic criteria for either PTSD or MDE (33.0% in Kosovo; 31.0% in Rwanda).
A large majority of participants with PTSD had concurrent MDE in both settings (79.6% in Kosovo; 68.4% in Rwanda). The association of PTSD and MDE was significant in the two studies, but significantly stronger in Rwanda than in Kosovo (OR 30.5 in Rwanda vs 12.4 in Kosovo; Breslow–Day test of OR homogeneity p = .006), because of the low frequency of MDE-only in Rwanda. Exposure to traumatic events was not associated with MDE-only in subsamples that did not meet criteria for PTSD (Kosovo, p = .75; Rwanda, p = .11).
PTSD and MDE symptom profiles
Symptom profiles are presented in Table 2 for all subjects who met diagnostic criteria for PTSD. Two avoidance symptoms were significantly less frequent in Rwanda than in Kosovo (avoiding thoughts about the event, 74.1% vs 90.3%; trouble recalling, 37.8% vs 94.2%). Conversely, sense of a foreshortened future was significantly more frequent in Rwanda than in Kosovo (95.2% vs 71.8%), together with one symptom of increased arousal (exaggerated startle response, 90.0% vs 75.7%).
Components of current PTSD diagnosis according to the MINI.
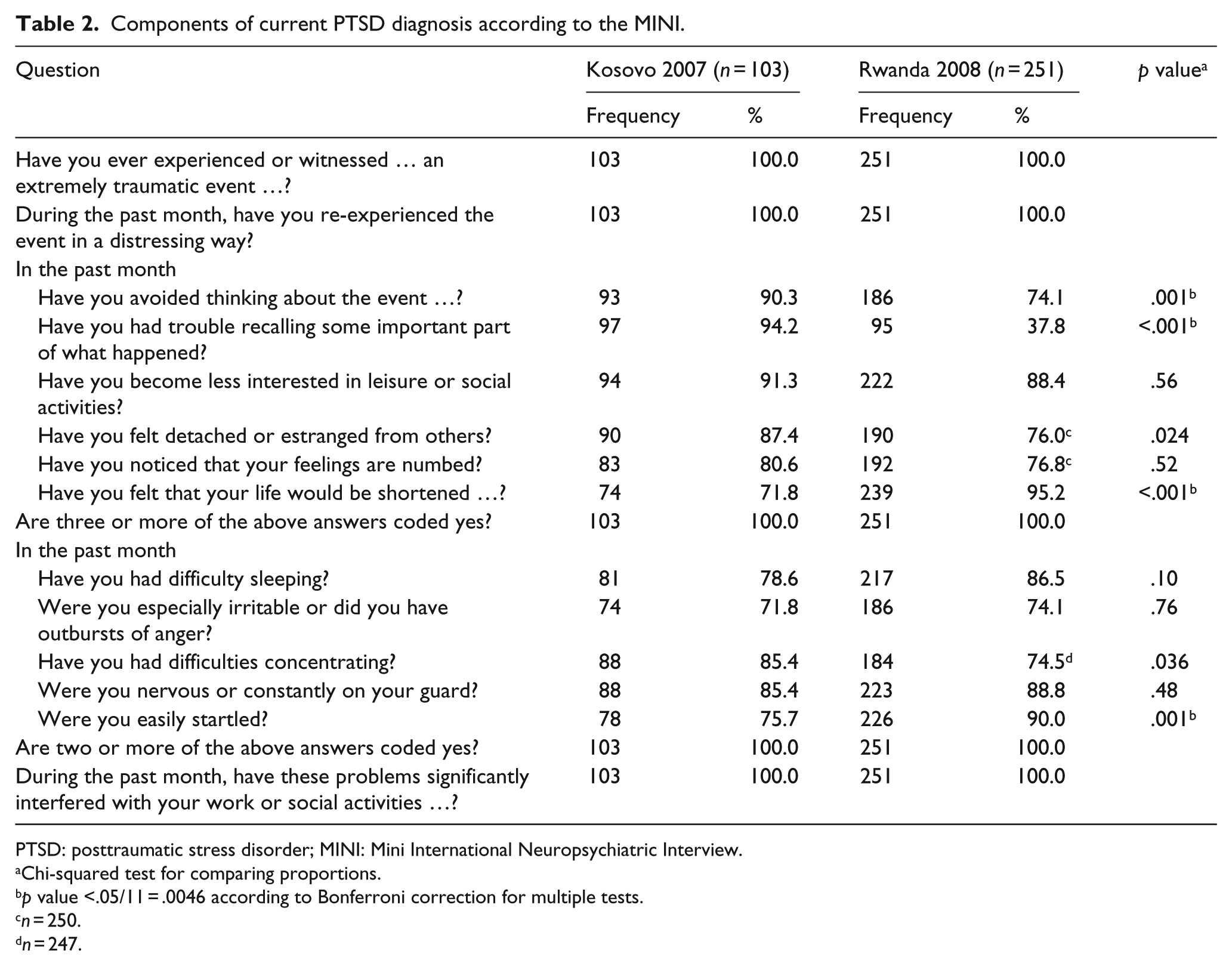
PTSD: posttraumatic stress disorder; MINI: Mini International Neuropsychiatric Interview.
Chi-squared test for comparing proportions.
p value <.05/11 = .0046 according to Bonferroni correction for multiple tests.
n = 250.
n = 247.
MDE symptoms are presented in Table 3 for all people who met the MINI criteria for MDE. Loss of energy (81.1% vs 92.8%) and difficulties concentrating (63.6% vs 79.9%) were less frequently endorsed in Rwanda than in Kosovo, while suicidal ideation was particularly rare in Kosovo (11.0% vs 68.7%). Suicidal ideation did not differ between MDE patients with and without comorbid PTSD in Kosovo (13.4% vs 9.9%, p = .53), but frequency of suicidality was increased among depressed Rwandan patients with PTSD (73.5% vs 51.1%, p = .006).
Components of current MDE diagnosis according to the MINI.
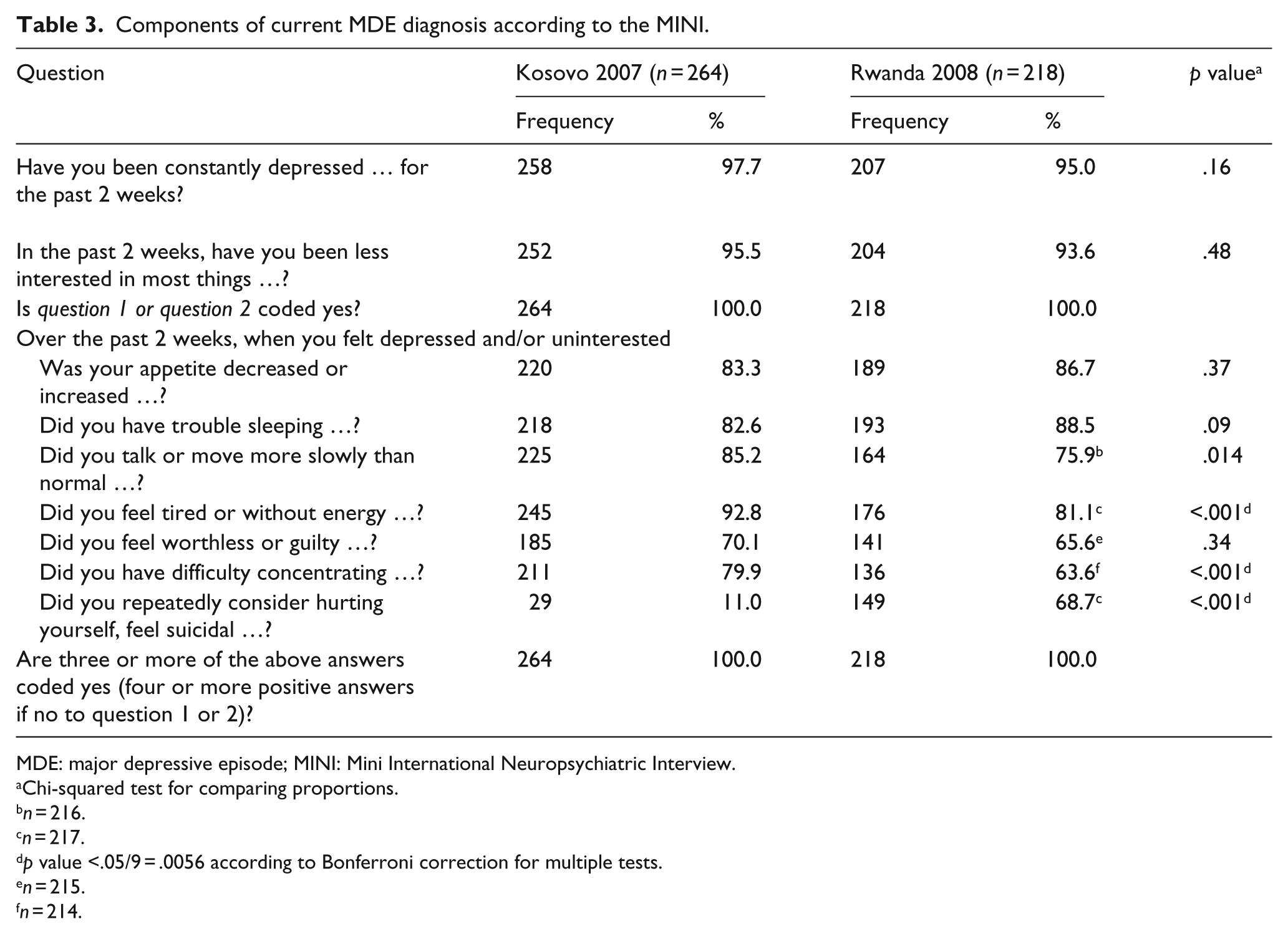
MDE: major depressive episode; MINI: Mini International Neuropsychiatric Interview.
Chi-squared test for comparing proportions.
n = 216.
n = 217.
p value <.05/9 = .0056 according to Bonferroni correction for multiple tests.
n = 215.
n = 214.
Because the Rwanda and Kosovo samples differed with respect to age and education, we re-examined symptom frequencies in the two studies after stratification for age and education. Effects did not show any significant inhomogeneity across age groups and education levels, except for two PTSD symptoms (sense of a foreshortened future and exaggerated startle response), for which differences between Rwanda and Kosovo were more pronounced among more educated participants (Breslow–Day test p < .01). Higher education was significantly associated with lower frequencies of these symptoms in Kosovo (p < .01) but not in Rwanda (p > .05).
Physical and mental health perception
SF-36 subjective health scores are presented in Table 4 for participants with neither PTSD nor MDE, PTSD-only, MDE-only and both PTSD and MDE. Respondents with neither PTSD nor MDE had the highest physical and mental health scores in both studies, while those with co-occurrence of PTSD and MDE had the lowest scores.
Subjective health scores (SF-36) according to PTSD and MDE diagnoses.
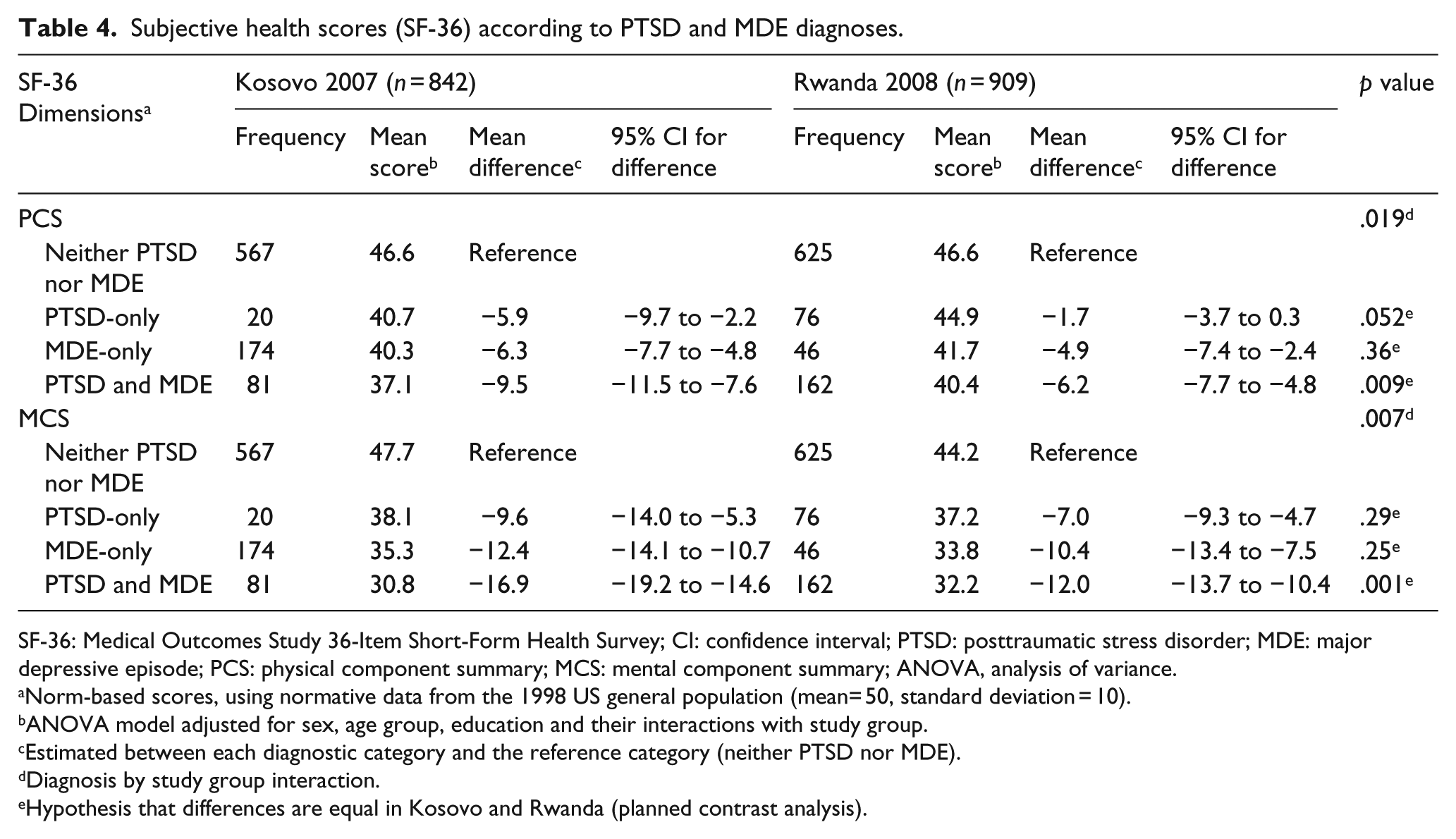
SF-36: Medical Outcomes Study 36-Item Short-Form Health Survey; CI: confidence interval; PTSD: posttraumatic stress disorder; MDE: major depressive episode; PCS: physical component summary; MCS: mental component summary; ANOVA, analysis of variance.
Norm-based scores, using normative data from the 1998 US general population (mean= 50, standard deviation = 10).
ANOVA model adjusted for sex, age group, education and their interactions with study group.
Estimated between each diagnostic category and the reference category (neither PTSD nor MDE).
Diagnosis by study group interaction.
Hypothesis that differences are equal in Kosovo and Rwanda (planned contrast analysis).
For PCS, we observed a significant diagnosis effect (F(3,1727) = 64.3, p < .001), study effect (F(1,1727) = 8.6, p = .003) and diagnosis by study interaction (F(3,1727) = 3.3, p = .019). The form of the interaction was further investigated by comparing the two studies with respect to the differences between participants with neither PTSD nor MDE and the ones in the other three diagnostic categories (Table 4). The effect of MDE-only did not differ in Kosovo and Rwanda (p = .36), whereas the effect of PTSD-only marginally differed (p = .052). Co-occurrence of PTSD and MDE was associated with a significantly larger impairment of perceived physical health in Kosovo than in Rwanda (mean PCS difference, −9.5 vs −6.2, p = .009).
For MCS, we observed a significant diagnosis effect (F(3,1727) = 173.6, p < .001), a non-significant study effect (F(1,1727) = 1.7, p = .20) and a significant diagnosis by study interaction (F(3,1727) = 4.1, p = .007). Contrast analyses revealed no significant difference between Kosovo and Rwanda for the effects of MDE-only (p = .25) and PTSD-only (p = .29). When both PTSD and MDE were present, impairment of perceived mental health was significantly larger in Kosovo than in Rwanda (mean MCS difference, −16.9 vs −12.0, p = .001).
Discussion
Few studies have examined the occurrence of psychiatric disorders in different post-conflict settings using an equivalent methodology, and even fewer have described the symptom profiles of posttraumatic reactions in different populations. A notable exception is the epidemiological survey conducted between 1997 and 1999 in four post-conflict regions (Algeria, Cambodia, Ethiopia and Gaza) (de Jong et al., 2001). The prevalence of lifetime PTSD varied from 15.8% in Ethiopia to 37.4% in Algeria, with intermediate rates in Cambodia (28.4%) and Gaza (17.8%). The relevance of contextual differences between countries was pointed out, with specific patterns of risk factors that included conflict-related events, elements of family history and ongoing adverse events (de Jong et al., 2001). Associations between PTSD and mood disorders, anxiety disorders and somatoform disorder were reported in a second article (de Jong et al., 2003). Comorbidity of PTSD and mood disorder within a 1-year interval varied from 1.8% in Ethiopia to 10.7% in Algeria.
In this study, proportions of participants who met diagnostic criteria for either PTSD or MDE were remarkably similar in Rwanda and Kosovo (about 30%), despite differences in MDE-only (more frequent in Kosovo) and PTSD alone or concomitant with MDE (both more frequent in Rwanda). On the one hand, the symptom overlap between PTSD and MDE has to be stressed. A recent study reported similar scores across all PTSD symptom scales in veterans with PTSD-only and major depressive disorder–only and suggested that differences might be fewer than expected from distinct diagnostic categories (Gros, Price, Magruder, & Frueh, 2012). On the other hand, the difficulty in comparing studies of different civilian populations exposed to war trauma has to be emphasized. Variability factors include trauma exposure, time elapsed between exposure and diagnosis, post-conflict events and cultural factors (Johnson & Thompson, 2008).
Experience of trauma most likely differed in the two studies, whether qualitatively or quantitatively. In the absence of detailed information about specific events, we observed that Kosovo participants less frequently reported exposure to trauma. They were thus less likely to meet diagnostic criteria for PTSD, which include experiencing or witnessing a traumatic event as a necessary condition. Because trauma has sometimes been considered as an independent risk factor for PTSD and MDE, we examined whether exposure to traumatic events was associated with MDE among participants without PTSD. No significant association was observed in line with a prospective study in Michigan, which showed that trauma did not increase the risk for first-onset major depression in people who did not develop PTSD. Both studies thus converge toward rejecting the hypothesis that PTSD and MDE might be two distinct responses to trauma (Breslau, Davis, Peterson, & Schultz, 2000). The Rwanda and Kosovo surveys also differed with respect to the time elapsed since the peak of the conflict, the political and socioeconomic conditions during that time and the availability and accessibility of health-care services. As it becomes more chronic, the psychopathology might also become less differentiated and characterized by mixed PTSD and depressive symptoms, as shown in a prospective study of injury survivors (O’Donnell, Creamer, & Pattison, 2004).
Association between PTSD and MDE
Whereas substantial comorbidity of PTSD and MDE has been largely documented (Brady, Killeen, Brewerton, & Lucerini, 2000; Kessler, Sonnega, Bromet, Hughes, & Nelson, 1995), we reported a long-lasting association of the two disorders about 14 years after the genocide in Rwanda and 8 years after the war in Kosovo. The strength of the association differed in the two settings. Comorbidity was observed in 9.5% of the Kosovo sample, in agreement with the figure of 9.1% in five countries of former Yugoslavia (Morina et al., 2013). PTSD and MDE co-occurred in 17.8% of the sample in Rwanda, where MDE alone was relatively rare (<5%). A large survey conducted in 2006 in four provinces of Rwanda similarly reported a strong association of PTSD and depression, which co-occurred in 21.8% of the sample (Brounéus, 2010). The high frequency of dual diagnoses in Rwanda might be attributed to more frequent exposure to traumatic events, as mentioned above. However, elements of post-conflict history might also be invoked. Participation as a witness in Rwandan village tribunals for truth and reconciliation (gacaca) was associated with increased levels of depression and PTSD, after adjusting for cumulative trauma exposure (Brounéus, 2010).
Differential presentation of PTSD symptoms
When focus was placed on respondents with PTSD, no between-sample difference was observed for symptoms such as diminished interest, concentration difficulties or sleeping problems, which are common to depression and PTSD. However, sense of a foreshortened future was significantly more frequent in Rwanda than in Kosovo, suggesting increased distress level. Two symptoms in cluster C (avoidance and numbing) were less frequent in Rwanda than in Kosovo, in line with numerous studies showing that these symptoms display considerable variability across cultures. They may represent coping mechanisms that depend more on cultural norms and societal processes than biology, in contrast to arousal and re-experiencing symptoms (Hinton & Lewis-Fernandez, 2011). Exaggerated startle response, a symptom in cluster D (hyperarousal), was more frequent in Rwanda. As part of a fear factor (Forbes et al., 2011), it might be relevant to the high comorbidity between PTSD and panic attacks, as observed in Rwandan widows (Hagengimana et al., 2003).
Differential presentation of MDE symptoms
MDE symptom patterns also differed in the two settings, with loss of energy and difficulty concentrating less frequent in Rwanda than in Kosovo. Historically, depression in Africa was characterized by a predominance of ideas of reference, persecutory delusions and psychosomatic symptoms. With globalization, this clinical presentation tends to change and resemble Western patterns of depression (Carta, 2013). The MINI investigates feelings of worthlessness and guilt with only one question. It is therefore not possible to make comparisons between these two cognitive symptoms of depression. In our study, we observed a major difference in suicidal ideation, which was endorsed by 68.7% of depressed participants in Rwanda, but only 11.0% in Kosovo. Since the MINI aggregates self-aggressive and suicidal ideations, this result should be interpreted with caution. A large study in five Balkan countries similarly reported a relatively low frequency of suicidal risk among participants with MDE alone (23.0%) (Morina et al., 2013), whereas thoughts of death or suicide had a prevalence >60% in seven of eight sites in cross-national epidemiologic studies of major depression (Weissman et al., 1996). Variable degrees of willingness to report about suicidal ideation might be invoked, in association with cultural factors and/or religious beliefs. In the Kosovo sample, we did not find increased suicidal ideation when MDE and PTSD co-occurred, in contrast to Morina et al. (2013). However, comorbidity was associated with increased suicidality in Rwanda. A large cross-sectional study in the United States showed that lifetime comorbidity of depression and PTSD was associated with much higher prevalence of suicidal ideation than either diagnosis alone (Cougle, Resnick, & Kilpatrick, 2009). A recent meta-analysis confirmed that comorbid depression increased suicidal risk among individuals with PTSD (Panagioti, Gooding, & Tarrier, 2012). As shown in Lebanon, exposure to war may increase the risk of suicide in individuals with prior impulse-control disorders, this effect being partly mediated by the emergence of mental disorders in the context of war (Karam et al., 2012).
Self-perceived mental and physical health
Either PTSD-only or MDE-only was associated with a poorer perception of physical and mental health in the two settings. Co-occurrence of PTSD and MDE led to further decreases in PCS and MCS scores, with significantly larger effects in Kosovo than in Rwanda. Poor physical health in patients with major depression is well documented, with a prevalence of unexplained somatic symptoms of about 50% throughout the world (Simon, VonKorff, Piccinelli, Fullerton, & Ormel, 1999). In Western countries, PTSD is similarly associated with elevated levels of somatic complaints (Weisberg et al., 2002) and increased risks of specific medical conditions, such as cardiovascular and pulmonary diseases (Spitzer et al., 2009). In Kosovo, PTSD and MDE were independently associated with somatic symptoms among bereaved young adults (Morina, von Lersner, & Prigerson, 2011). About 30% of respondents in our longitudinal Kosovo study reported about ill health without access to medical care in the post-war period, and this event was associated with both persistence and new occurrences of PTSD (Eytan et al., 2011). Unmet needs for medical care might have played a role with respect to the differential associations of PTSD, MDE and perceived physical health in the two settings. Another hypothesis might be related to culturally specific somatic complaints in reaction to trauma, which would not be taken into account with instruments such as the SF-36 (Hinton & Lewis-Fernandez, 2011). In Rwanda, such symptoms might include shortness of breath (Hagengimana et al., 2003), hiccups, fainting, hearing loss and loss of speech (Munyandamutsa et al., 2012).
Strengths and limitations of the study
Given the limited literature pertaining to the long-term mental health outcome in culturally different post-conflict settings, the strengths of this study are large sample sizes and use of similar study instruments in Rwanda and Kosovo. The study has limitations that also need to be acknowledged. First, the two studies were not designed with the a priori objective to compare the two settings so that the comparison should be considered as exploratory. Second, sampling methods differed and samples cannot be considered as representative of the populations in each country, as discussed in earlier publications (Eytan et al., 2011; Munyandamutsa et al., 2012). The relevance of different sampling schemes might nevertheless be limited in this work, which focuses on diagnostic groups that are homogeneous with respect to PTSD and MDE criteria. Third, information about the nature and amount of trauma exposure was not recorded. In both countries, participants mentioned traumatic events typically encountered during war and civil armed conflicts, such as torture, rape, murder of close relatives, forced isolation from others and lack of food or water. However, Kosovo and Rwanda most likely differed with respect to the type and cumulative amount of traumatic events known to influence PTSD severity through a ‘dose–effect’ relationship (Mollica et al., 1998). Recall bias is a fourth limitation since surveys were conducted 8–14 years after the conflicts. Differences between settings cannot be excluded in this respect because of distinct truth, justice and reconciliation processes. Fifth, the two surveys did not allow documenting post-conflict histories, which possibly included additional traumatic events, as well as non-traumatic stressors, such as familial difficulties, economical hardship and unmet needs for health care. They also did not address cultural factors, which might have contributed to shape the representation and adjustment to trauma in each country. Sixth, we focused on PTSD and MDE, while anxiety disorders such as panic disorders and generalized anxiety disorders may be part of the response to trauma in some cultures (Brady et al., 2000; Hagengimana et al., 2003). A seventh limitation arises from the use of the MINI as a diagnostic instrument. Algorithms for PTSD and MDE first consider two screening questions that determine whether other symptoms are to be investigated or skipped. Thus, full symptom patterns could only be described for participants who met diagnostic criteria for PTSD or MDE, but no complete picture was available for the ones with sub-threshold conditions.
Conclusion
This study has two main implications. First, it emphasizes that PTSD and/or MDE in post-conflict settings are long-lasting conditions associated with poor perception of physical and mental health. Concomitant PTSD and MDE have been associated with increased suicidality (Panagioti et al., 2012), low quality of life (Morina et al., 2013), socioeconomic disadvantage (Ayazi et al., 2012) and high frequency of health-care visits (Campbell et al., 2007) in different populations and settings. Taken together, these studies call for sustained efforts toward the implementation of integrative health-care systems in post-conflict countries, taking into account physical and mental health dimensions. Second, this study sheds light into some subtle differences between culturally different settings. Despite the difficulty to disentangle the specific role of cultural factors from the contribution of distinct conflict and post-conflict histories, integrating cultural and social components into our understanding of disparities in response to trauma remains a challenge.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.