
Abstract
Aims:
New-type depression, which exhibits characteristics that are different from those of traditional depression, is thought to be associated with hikikomori. However, a causal relationship has yet to be established. Thus, this study examined the causal relationship between the psychological characteristics of new-type depression (interpersonal sensitivity and privileged self) and hikikomori.
Method:
The analysis included 393 male individuals with hikikomori, with longitudinal data collected from participants by asking them to respond 3 times at 3-month intervals. Participants responded to scales to measure the psychological characteristics of new-type depression and the severity of hikikomori symptoms. We analyzed the data using a random-intercept cross-lagged panel model.
Results:
Our results showed significant cross-lag effects. In particular, our findings revealed that the extent of hikikomori at Time 1 increased IS and PS at Time 2, whereas IS and PS at Time 2 increased the extent of hikikomori at Time 3. Our data fit the model. These results suggest a self-reinforcing pattern in which hikikomori tendencies intensify with increasing IPS over time.
Conclusion:
We propose that it is important to address both new types of depression and hikikomori rather than addressing one or the other in the treatment of these two disorders. However, this study focused exclusively on individuals who were hikikomori, men, unemployed, and non-disabled. Future studies should include individuals without hikikomori infections or new types of depression.
Keywords
Introduction
This study examined the causal relationship between Interpersonal Sensitivity (IS), the Privileged Self (PS), and hikikomori by analyzing longitudinal data. Recently, the incidence of depressions with characteristics that differ from those of Japanese traditional depression has been increasing (Kato et al., 2011; Sakamoto, 2022). For example, Modern-type depression (MTD) is characterized by a situation-dependent depressive state, blaming others, and strong avoidant tendencies (e.g. Kato et al., 2016). Other types of depression include dysthymia (Tarumi, 2005) and immature depression (Abe, 2011). Sakamoto et al. (2016, 2017) organized these subtypes of depression that differ from traditional depression and found common characteristics between them. Consequently, they proposed the concept of new-type depression (NTD) to comprehensively describe these subtypes. It is noted that Sakamoto et al. (2016, 2017) use the terminology “Modern type depression,” but recent papers have standardized on NTD (e.g. Sakamoto et al., 2024). In this study, we followed Sakamoto et al. (2024) and used the term NTD.
IS and PS are psychological features of NTD (Sakamoto et al., 2017). IS refers to the tendency to worry excessively about others’ negative evaluations and to overreact to them (Yamakawa et al., 2015). Individuals with high IS are often deeply affected by negative evaluations from influential others who frequently experience shock or depression (Sakamoto et al., 2017). For example, Sakamoto et al. (2017) reported that office workers with high IS tend to worry about negative evaluations from superiors and colleagues after making mistakes at work, which can result in depression. PS refers to the tendency to pursue pleasure and satisfaction at the expense of maintaining harmony with others (Yamakawa et al., 2015). Individuals with a high PS may avoid negative feedback, act defensively, or disregard others’ opinions. For example, Sakamoto et al. (2017) described high-PS office workers who, after making mistakes and feeling depressed, may blame superiors or colleagues for negative evaluations, or skip work to escape unpleasant feelings related to the situation.
IS and PS are concepts characterized by new-type depression (NTD). Muranaka et al. (2015) collected descriptions of NTD from 14 books authored by experts in psychiatry and related fields to organize their psychological features. They analyzed 105 descriptions using qualitative analysis and identified 2 primary labels, IS and PS (Muranaka et al., 2015). The combination of high IS and PS contributes to NTD development (Sakmaoto & Yamakawa, 2020). In this paper, IS and PS are collectively referred to as IS/PS.
Previous studies have demonstrated that the IS/PS can predict NTD characteristics. Several cross-sectional and longitudinal studies indicate that is/PS increases depression (Muranaka et al., 2019, 2023; Sakamoto et al., 2017). Reportedly, individuals with high IS/PS exhibit a more pronounced difference in their depressive states between workdays and holidays (Sakamoto & Yamakawa, 2022), as well as experience difficulty in suppressing anger and are more likely to express it (Sakamoto et al., 2022). Furthermore, IS/PS not only serves as a predictor of NTD, but may also be associated with several maladaptation’s. For example, IS/PS is associated with Internet addiction (Suzuki et al., 2023) and with seeking help from mental health professionals before and after the COVID-19 pandemic (Sakamoto et al., 2024).
One maladaptive condition anticipated to be related to IS/PS is hikikomori, a withdrawal from social participation (education, including compulsory education, employment, including part-time jobs, and other interactions outside the home), which continues under the condition of being housebound for over 6 months (this may include leaving the home while avoiding interactions; Saito, 2010). A Survey of hikikomori in Japan (Cabinet Office, Government of Japan, 2019) broadly defines hikikomori based on any of the following conditions lasting 6 months or longer: (a) staying at home but going out only for errands related to one’s hobbies, (b) staying at home but going out to a nearby convenience store, (c) leaving one’s room but never leaving the house, and (d) rarely leaving one’s room. Hikikomori is not limited to Japan and is now receiving international attention (Kato et al., 2012). Moreover, MTD, which is included in the NTD, is considered a gateway disorder for hikikomori (Kato & Kanba, 2017).
A hypothetical model of the occurrence of hikikomori in Japan and worldwide (Kato et al., 2019) asserts that emotional and cognitive reactions such as depression, decreased motivation, social phobia, distrust, anger (indirect), and amae (overdependence) cause hikikomori-related behaviors such as avoidance of social participation, escapism from life realities, and withdrawal from the Internet world (Kato et al., 2020). In this regard, IS/PS (a) includes hypersensitivity to other people’s evaluations and avoidant tendencies (Sakamoto et al., 2017), (b) increases interpersonal stress and depression (Muranaka et al., 2019, 2023; Sakamoto et al., 2017), (c) positively correlates with anger expression and is negatively associated with anger suppression (Sakamoto et al., 2022), and (d) increases Internet addiction (Sakamoto et al., 2024). Based on these findings, we hypothesized that the IS/PS predicts hikikomori.
This study examined the relationship between IS/PS, a psychological feature of NTD, and hikikomori. However, as most individuals are not hikikomori, measuring individual differences in hikikomori requires a specialized sample. Therefore, we conducted a longitudinal survey involving unemployed men and selected individuals with hikikomori. We focused on male participants because in Japanese society, unemployment has a particularly negative effect on men’s mental health (Kobayashi, 2021). In Japan, men are generally expected to work full-time as regular employees and serve as the primary breadwinners. Consequently, unemployment or nonregular employment is often viewed as a deviation from social norms that may negatively affect mental health. These gender differences in social evaluation may influence the psychological characteristics of new-type depression (NTD), the severity of hikikomori symptoms, and their relationship. Therefore, when examining maladaptive conditions such as NTD and hikikomori among unemployed individuals in Japan, it is necessary to consider the gendered effect of unemployment on mental health. Based on these considerations, this study focused on unemployed men, who are considered more vulnerable to maladaptation, to eliminate the confounding effects of sex. Using this sample, we examined the within-person causal relationship between IS/PS and hikikomori using a random-intercept cross-lagged panel model. This model enabled us to predict the impact of a decrease in IS/PS or improvement in hikikomori in an individual. The findings of this study provide valuable insights into the relationship between NTD and hikikomori.
Methods
Our Data and Participants
Longitudinal data were collected in March 2022 (T1), June 2022 (T2), and September 2022 (T3). We commissioned a Japanese research firm to collect data from unemployed men who were not disabled at T1. Specifically, we confirmed whether the participants were officially certified as having a disability and included only those who were not recognized in the survey sample. In total, 762 individuals participated in the survey at T1. All individuals who responded at T1 were asked to respond at T2 and T3. There were 162 participants in their 20s, and 200 each in their 30s and 50s.
We explained the study to the participants in writing and confirmed their consent to participate. Participants were informed that the survey would be anonymous, that no personal information would be collected, that the data would be used for research purposes only, and that they would receive rewards as determined by the research firm. The participants received this explanation at each time point and were asked to provide their consent to participate.
Although studies on specific populations, such as hikikomori, often conduct pre-screening before data collection, we did not implement a screening survey prior to the first wave of this study. Our approach aimed to reduce the number of survey waves required from each participant and maximize the number of valid cases for the time-series analysis. We included participants who responded to at least two of the three waves (i.e. all three waves or Wave 1 plus either Wave 2 or Wave 3) in the time series analysis. Conducting a pre-screening survey before the main three-wave survey would have required participants to complete the screening and at least two waves of the main survey, resulting in more stringent inclusion criteria and a higher number of cases excluded due to insufficient responses. Therefore, we did not include a prescreening procedure in our study design.
Measurements
Hikikomori Screening Components
Hikikomori screening included the following two components: (a) usual outgoing status and (b) time spent in that status. The usual outgoing status encompassed the following eight choices: (1) going out every weekday for work or school, (2) going out 3 to 4 days a week for work or school, (3) frequent outings for playing or other recreational activities, (4) occasional interactions with others outside home, (5) usually staying at home and going out only for errands related to one’s hobbies, (6) usually staying at home and going out to a nearby convenience store, (7) leaving one’s room but never leaving the house, or (8) rarely leaving one’s room. The participants selected an option that was optimally aligned with their condition. The second component, the time spent in that status, was evaluated on a five-point scale, as follows: (1) less than a month, (2) less than 3 months, (3) less than 6 months, (4) 6 months to a year, and (5) more than a year. Those who selected option (5) or above in the usual outgoing status, as well as selected 6 months or more, that is, options (4) or (5) in the duration of that status, are considered “hikikomori in the broad sense of the word” (Cabinet Office, Government of Japan, 2019). These components are adopted from a questionnaire administered by the Cabinet Office of the Government of Japan in 2018 (Cabinet Office, Government of Japan, 2019).
Interpersonal Sensitivity / Privileged Self Scale 2nd Version (IPS-2)
IPS-2 (Muranaka et al., 2021) measures psychological characteristics associated with NTD. The scale comprises 22 items rated on a five-point scale (1 = not applicable to 5 = applicable). It has two subscales, IS and PS, each of which is measured using 11 items. Some examples of IS items include “If I am criticized by those around me, I cannot forget about it,” and “I worry that those around me may complain about me or look at me strangely.” Examples of PS items include “I do not like to be given feedback about my ideas,” and ‘I think there are a lot of mean people around me.” In this study, the IPS-2 score was calculated based on the total score of all 22 items, which ranged from 22 to 110.
Hikikomori Questionnaire-25 One-Month Version (HQ-25M)
Notably, HQ-25M (Kato et al., 2023) is a 25-item Likert scale designed to measure hikikomori symptoms’ severity. Participants rated each item on a five-point scale ranging from not applicable (0 points) to applicable (4 points), based on their state during the past month. The HQ-25M has 3 subscales (isolation, socialization, and emotional support), and the total score obtained by summing the responses to all 25 items provides an overall hikikomori score ranging from 0 to 100. As the normal HQ-25 (Teo et al., 2018) assesses an individual’s status over 6 months, the response period overlapped in this study. Therefore, we used the HQ-25M, which captures information over a period of 1 month.
Demographic Variables
Participants responded to demographic items, including sex (all participants were men), age, employment status (all participants were unemployed at T1), disability status (all participants were non-disabled at T1), reason for unemployment, duration of unemployment, family and housemates, and past work experience. However, our analysis controls for the effects of time-invariant individual difference variables during the measurement period (6 months, from March to September 2022; see the analysis methodology below). The effects of the duration of unemployment, the existence of family members or housemates, and past work experience are unlikely to fluctuate over the 6-month measurement period. The aggregate results of the demographic variables for the subjects analyzed in T1 are presented in Supporting Information.
Analysis
Random Intercept Cross-Lagged Panel Model (RI-CLPM)
The RI-CLPM examines causality in within-person relationships (see Hamaker et al., 2015; Usami, 2022 for further details). It orthogonally decomposes the observed variables at each time point into a “stable trait factor,” which represents individual differences that remain stable over time, and within-person variability, which does not correlate with the stable trait factor at each measurement point. The stable trait factor was expressed as a random intercept. We then examined the causal effects of the variables on within-person variability by estimating the cross-lagged effects of within-person variability. This study examined the causal effects of within-person variability on the psychological features of NTD (i.e. the IPS-2 score) and hikikomori (i.e. HQ-25M score) using the RI-CLPM.
Ethical Considerations
The Ethics Committees of (omitted for blind review) approved our surveys (approval: [omitted for blind review]) between February 22 and May 10, 2022.
Results
Participants Analyzed
The participants were screened in three steps. First, we selected those who responded to at least two of the three questions. Consequently, 574 participants remained after 188 participants were excluded. Subsequently, we excluded 58 respondents who provided problematic answers at any of the 3 time points. Specifically, we excluded participants who (a) provided identical responses to all items, (b) offered false responses to trap items, and (c) changed their age by two or more years during the survey period (March–September, 2022). Of the 516 participants, 393 who had hikikomori in a broad sense at the time of the first survey (T1)were included in the analysis.
The analyzed participants’ (n = 393) mean age was 41.69 (SD = 10.09) years. Additional demographic information for the analyzed participants at T1 is provided in the Supplementary Material. There were 284 complete (T1, T2, and T3) and 109 two-point responses. Moreover, 73 participants answered T1 and T2, and 36 answered T1 and T3. Table 1 presents the descriptive statistics of the HQ-25M and IPS-2.
Mean, SD, ω Coefficient, and Correlation Matrix of the Interpersonal Sensitivity/Privileged Self Scale Second Version (IPS-2) and the Hikikomori Questionnaire-25 One-Month Version (HQ-25M) Scores at Three Time Points.
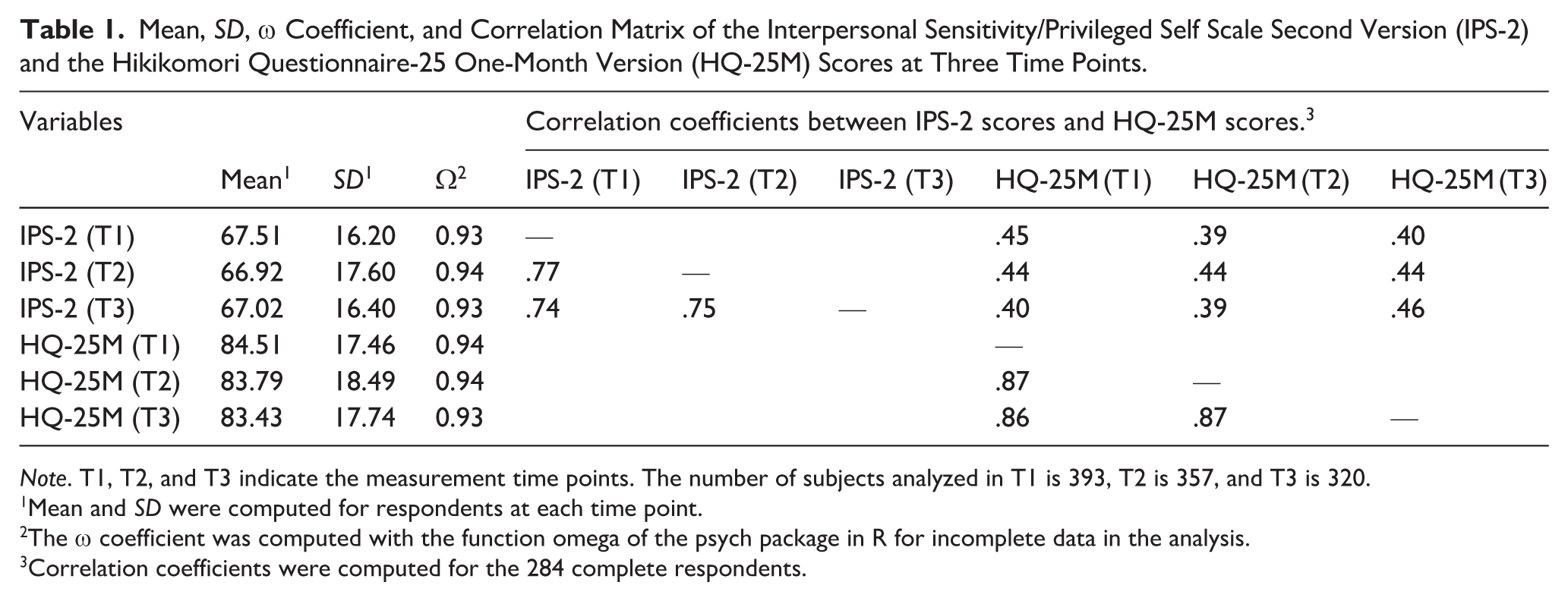
Note. T1, T2, and T3 indicate the measurement time points. The number of subjects analyzed in T1 is 393, T2 is 357, and T3 is 320.
Mean and SD were computed for respondents at each time point.
The ω coefficient was computed with the function omega of the psych package in R for incomplete data in the analysis.
Correlation coefficients were computed for the 284 complete respondents.
To better understand the participants’ backgrounds, we examined the reasons for unemployment and the severity of hikikomori. First, the reasons for unemployment were assessed at T1 using a five-point Likert scale. We calculated the mean and SD for each reason and counted the participants who selected a score of 4 or higher. The mean score for physical injury or illness was 1.87 (SD = 1.38), with 41 participants selecting 4 or higher. For mental health conditions, the mean was 2.31 (SD = 1.53), with 70 participants selecting 4 or higher. Additionally, 27 participants selected 4 or higher for both physical and mental health issues. Second, we analyzed the severity of hikikomori. Although the HQ-25M (1-month version) lacks an established cutoff, we used the HQ-25 (6-month version) cutoff of 44 points as a benchmark. Based on this reference, we counted the number of participants who exceeded the cutoff value. At T1, 369 of the 393 participants (93.9%) scored more than 44 points, indicating that the sample represented a high hikikomori population.
RI-CLPM
To examine the causal effect of within-person variability on IPS and HQ-25M scores, we analyzed longitudinal data using the RI-CLPM. As the measurement intervals were equally spaced and not as long as 3 months, we imposed equality constraints on the autoregressive coefficients of first-order lags from IPST1 to IPST2, IPST2 to IPST3, HQ-25MT1 to HQ-25MT2, and HQ-25MT2 to HQ-25MT3, as well as the error covariance at T2 and T3 for IPT-2 scores and HQ-25M scores in our model. For data analysis, we used R 4.0.3, and the Lavaan function from the Lavaan package to run the RI-CLPM. Because our model had a mean structure, we used the full information maximum likelihood method to estimate incomplete data.
The analysis revealed significant autoregressive coefficients for IPS-2 and HQ-25m scores. The autoregressive coefficients for the equality-constrained IPS-2 were β = .225 (SE = 0.101, p = .025, 95% CI[0.028, 0.423]), while those for HQ-25M were β = .325 (SE = 0.104, p = .002, 95% CI[0.120, 0.530]). Additionally, we found significant cross-lagged effects from HQ-25MT1 to IPS-2T2 (β = .450, SE = 0.192, p = .019, 95% CI[0.075, 0.826]), and from IPS-2T2 to HQ-25MT3 (β = .156, SE = 0.076, p = .041, 95% CI[0.006, 0.306]). Other cross-lagged paths, including IPS-2 T1 to HQ-25M T2 (β = −.082, SE = 0.122, p = .500, 95% CI[−0.322, 0.157]) and HQ-25M T2 to IPS-2 T3 (β = −.016, SE = 0.123, p = .895, 95% CI[−0.257, 0.225]), were not significant. The percentage of variance of the stable trait factor (i.e. random intercepts) to the variance of the measured values at T1 was 76.2% for the IPS-2 score and 86.0% for the HQ-25M score. The correlation between IPS-2RI and HQ-25MRI was significant (r = 524, p < .001). Our data were a good fit to the model (χ2(4) = 0.193, p = .996, CFI = 1.000, RMSEA = 0.000, SRMR = 0.003, GFI = 0.999, AGFI = 0.991). Figure 1 shows the RI-CLPM results.
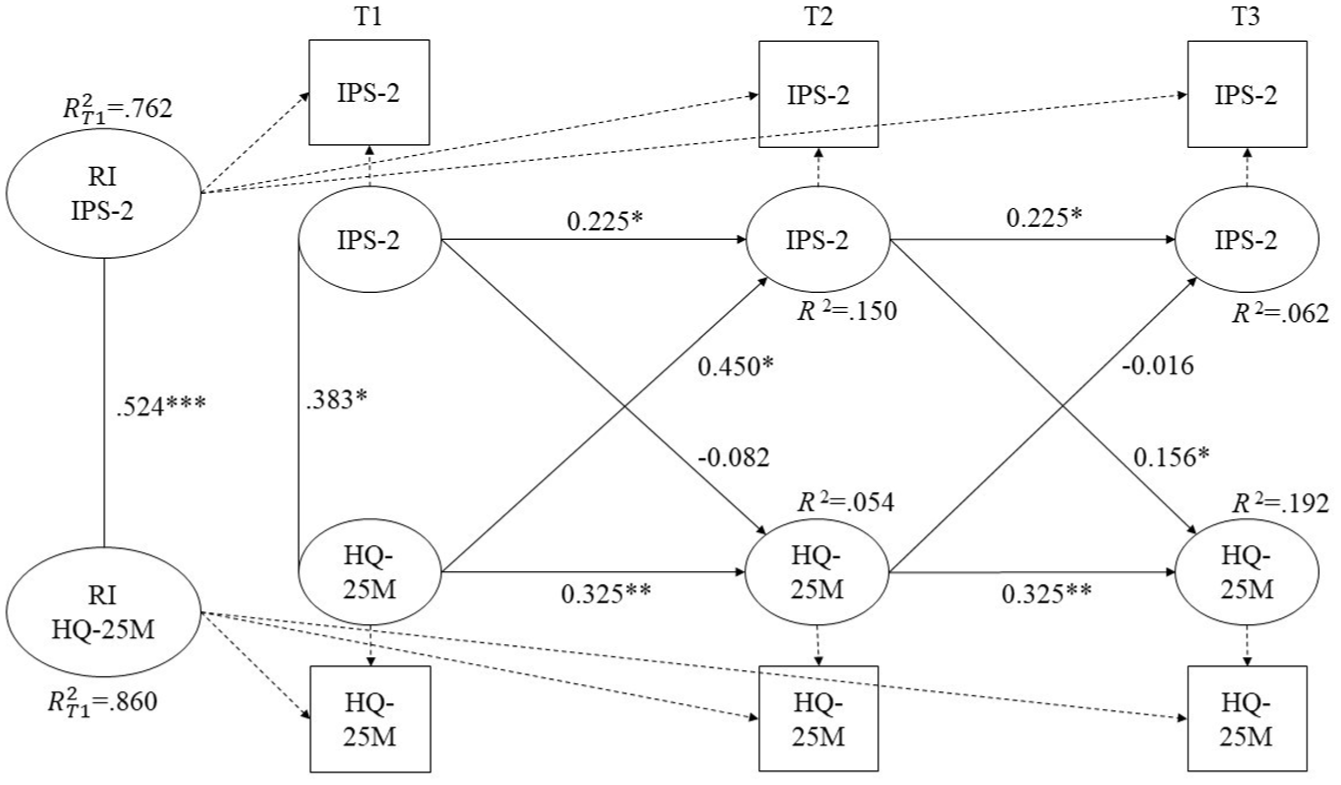
RI-CLPM for IPS-2 and HQ-25M scores.
This figure shows the result analyzed using the Random Intercept Cross-Lagged Panel Model (RI-CLPM) of analyzing the scores of the Interpersonal Sensitivity/Privileged Self Scale second version (IPS-2) and the Hikikomori Questionnaire-25 One-month version (HQ-25M) measured at three time points. The covariances between the random intercepts of the IPS-2 (RI IPS-2) and HQ-25M (RI HQ-25M) and between the latent variables of the IPS-2 and HQ-25M at T1 were standardized. The coefficient of the dashed path is constrained to 1.00. The results of the errors are omitted.
Discussion
We examined the causal relationship between IS/PS and the psychological features characterized by new types of depression and hikikomori. The participants were unemployed, non-disabled, hikikomori, and male. Our study revealed two major findings. First, autoregressions were significant for both the IPS-2 and HQ-25M scores. Thus, an increase in IS/PS and hikikomori enhanced the same trend over the months. Second, cross-lagged effects from the HQ-25M score at T1 to the IPS-2 score at T2 and from the IPS-2 score at T2 to the HQ-25M score at T3 were significant. However, other cross-lagged paths (i.e. IPS-2 at T1 to HQ-25M at T2 and HQ-25M at T2 to IPS-2 at T3) were not significant, indicating that the bidirectional and temporal effects were not consistently supported.
These results suggest that is/PS may mediate self-reinforcement of hikikomori tendencies and contribute to their worsening. From T1 to T2, the cross-lag effect from the HQ-25M to the IPS-2 was significant, indicating that hikikomori characteristics, such as social isolation, may increase IS/PS. Additionally, from T2 to T3, the cross-lag effect from the IPS to the HQ-25M was significant. Individuals with higher IS/PS levels are more likely to experience interpersonal stress (e.g. Muranaka et al., 2019) and express anger (Sakamoto et al., 2022). Overall, IS/PS appear to negatively affect social relationships and may exacerbate hikikomori by making it more difficult to establish and maintain these relationships. This relationship between the IS/PS and hikikomori tendencies likely leads to hikikomori self-reinforcement. Considering this self-reinforcing process, we propose a simultaneous approach targeting both hikikomori and IS/PS for the treatment of hikikomori and NTD. For example, combining standard hikikomori interventions, such as drop-in centers and day programs, with counseling aimed at reducing IS/PS among individuals with hikikomori may be highly effective in improving both hikikomori and NTD.
When interpreting the findings of this study, attention should be paid to the definition of hikikomori. Individuals meeting the criteria for hikikomori were identified according to the definition and measurements of the Cabinet Office, Government of Japan (2019). Specifically, those who reported going out for work or school 3 to 4 days per week were not classified as having hikikomori. In contrast, Kato et al. (2019) proposed a more recent definition that considers going out 3 days or fewer per week as a criterion for hikikomori; however, individuals who attend work or school are not regarded as having hikikomori, even with a low outing frequency. Although the two definitions differ slightly in their outing frequency thresholds, both agree that regular attendance at work or school excludes individuals from being classified as having hikikomori. Therefore, we considered that the actual responses leading to the hikikomori classification would not differ substantially between the two definitions. The Cabinet Office, Government of Japan (2019) definition was adopted in this study because it was not feasible to use the criteria proposed by Kato et al. (2019) at the time of data collection. A self-report scale consistent with Kato’s definition (HiDE-S) will not be published until 2025 (Reina et al., 2025), whereas our survey will be conducted in 2022. Thus, we used the definition of the Cabinet Office of the Government of Japan, which has an established measurement method. In future research, the use of an HiDE-based definition and measurement is expected to become the standard.
Limitations
This study focused on unemployed and undisabled men. We analyzed the responses of participants who were considered to have hikikomori in the broadest sense. Therefore, caution must be exercised when applying the findings of this study to employed, disabled, and non-hikikomori individuals of other sexes. Particularly, the participants had high scores on the HQ-25M (M T1 = 84.51), and stable trait factors accounted for 86.0% of the variance. Our findings should be carefully adapted to non-hikikomori patients with unstable hikikomori symptoms. As a social problem, hikikomori is not limited to unemployed adult men. Future research should focus on non-hikikomori individuals and other target groups, such as women and students. Specifically, we believe that future research should focus on non-hikikomori individuals and those with NTD to demonstrate that NTD is a gateway disorder for hikikomori.
Conclusion
The findings of this study suggest the self-reinforcement of hikikomori through IS/PS. We propose the use of both hikikomori symptoms and IS/PS to treat hikikomori and NTD. However, the participants in this study were male, unemployed, non-disabled, and hikikomori. To demonstrate that NTD is a gateway disorder for hikikomori, it is desirable to focus on both NTD and non-hikikomori individuals.
Supplemental Material
sj-docx-1-isp-10.1177_00207640261456745 – Supplemental material for Examining the Causal Relationship Between Hikikomori and Psychological Features of New-Type Depression: A Longitudinal Study on Male Individuals With Hikikomori Condition
Supplemental material, sj-docx-1-isp-10.1177_00207640261456745 for Examining the Causal Relationship Between Hikikomori and Psychological Features of New-Type Depression: A Longitudinal Study on Male Individuals With Hikikomori Condition by Yudai Suzuki, Takahiro A. Kato and Shinji Sakamoto in International Journal of Social Psychiatry
Footnotes
Acknowledgements
The online surveys were administered by Cross Marketing, Inc., Tokyo. This manuscript has been edited by Editage.
Ethical Considerations
The Ethics Committees of Nihon University approved our surveys (approval: 03-77 and 04-01) on February 22, and May 10, 2022.
Consent to Participate
Respondents gave written consent for review and indicated their consent before answering the online questionnaire.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by JSPS KAKENHI (Grant Number 20H01773).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
It is not possible to share our data, as this study has not been approved by the Ethics Committee or the respondents to share the data.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.