
Abstract
Dental caries is the most prevalent chronic disease affecting human populations worldwide. The diverse disease patterns across and within countries are related to socio-behavioral determinants, demographic factors, environmental conditions, and the availability and accessibility of oral health services, in particular, exposure to disease prevention programs (Petersen, 2003, 2008a). Benefits of fluoride for caries prevention have been substantiated in many countries (Petersen and Lennon, 2004; Jones et al., 2005). In the second half of the 20th century, this focus shifted to the development and evaluation of fluoride toothpastes and rinses and, to a lesser extent, to alternatives to water fluoridation, such as salt and milk fluoridation. Most recently, efforts have been made to summarize this extensive database through systematic reviews of fluoride administration (McDonagh et al., 2000; Marinho et al., 2003; Australian Government, 2007). The Asian workshop held in Phan-Nga, Thailand, during March 22-24, 2011, aimed to discuss current information on fluoride and dental caries, as well as to try identifying barriers and opportunities that countries of Asia may have for implementing such programs. In addition, the intention was to give recommendations for including fluoride schemes within national public health programs.
Fluoride for Public Health
According to the World Health Organization (WHO), the automatic administration of fluoride, such as water fluoridation, salt fluoridation, and milk fluoridation, plays a major role in public health (Petersen, 2008b). In addition, the use of affordable fluoride toothpaste is recommended; however, toothpastes must have sufficient fluoride content to be effective (e.g., 1500 ppm F). The WHO policy on effective use of fluoride is reflected in four World Health Assembly Resolutions: WHA22.30 (1969) and WHA28.64 (1975) on fluoridation and dental health; WHA31.50 (1978) on fluoride for prevention of dental caries; and, most recently, WHA60.17 (2007), “Oral Health: Action Plan for Promotion and Integrated Disease Prevention". The 2007 Resolution urges Member States to ensure that populations and segments benefit from the appropriate use of fluoride.
Dental Caries
Two mechanisms of dental caries were described during the meeting: the ionic “see-saw” and Stephan’s curve. The first component emphasizes the exchange of calcium and phosphate ions between the enamel surface and plaque. The second component describes the fall in plaque pH following the ingestion of or rinsing with sucrose solutions. There are four key elements: the resting plaque at around pH = 7; the rapid fall in plaque pH within 2 to 5 min of a sucrose (2-10%) rinse; the critical pH at around pH 5.5, below which we see loss of calcium and phosphate ions from the enamel surface; and the slow increase in plaque pH back to the resting level over a period of 15 up to 120 min. These components are useful for an understanding of disease mechanisms and the role of fluoride in the caries process, particularly in promoting formation of hydroxyapatite, reducing breakdown of dietary sugars, and promoting remineralization of enamel.
Early Detection of Initial Caries
Recommendations are to focus on sound teeth and protect them from caries; methods for detecting early stages, such as quantitative light-induced fluorescence (QLF), have been developed. Differentiating definitions for caries, lesion, process, detection, assessment, and diagnosis have been developed. The QLF methodology has also been used for studying the effect of fluoride on remineralization of incipient caries.
Scientific Rationale of Fluoride in Caries Prevention and Control
Fluoride action is predominantly post-eruptive; fluoride in the oral fluids is interchanged with soft tissues, dental hard tissues, and dental plaque, expectorated or swallowed, and recycled via saliva. Key to the effective use of fluoride is using the appropriate amount and the appropriate method of delivery: either community-based, professionally administered, or self-applied by the individual. The prospects for fluoride in caries prevention depend on establishment of the best public health intervention, correct topical combinations, methods for optimizing delivery of free ionic fluoride and retention in the oral cavity (minimizing ingestion), targeting fluoride intervention with eruption patterns, and use in combination with other remineralizing agents, such as calcium compounds.
Fluoride Research—Unfinished Tasks
The meeting highlighted the need for continuous research. Improvement in the anti-caries effect of fluoride may be explored by enhancement of the physicochemical effect of fluoride and association with anti-biofilm agents, and possible interaction with non-fluoride anti-caries agents. The ultimate goal is the optimization of oral health in a most efficient manner, and with minimum risks (World Health Organization, 2010). Some level of slight enamel fluorosis has been the trade-off for effective caries prevention depending on fluorides. The mild or very mild level of fluorosis is often related to multiple uses of caries-preventive fluorides. Reducing the risk of enamel fluorosis would require a clear understanding of the effects of different fluoride applications.
Dental caries is a multi-factorial disease. In addition to the biological mechanisms, population risks involve social determinants (e.g., personal income, education), behavioral factors, and the accessibility of fluoride at the community or individual level (Kwan and Petersen, 2010). Meanwhile, the role of socio-environmental factors in disease prevention and health promotion should be studied, particularly in developing countries.
Community Fluoride Administration
Fluoride is available to the population via community methods, professional applications, or self-administration (World Health Organization, 1994). Three vehicles (water, salt, and milk) have been successfully used in community approaches for providing fluoride to people for caries prevention. The success of fluoridation programs for the prevention of dental caries has been demonstrated in several countries. Water-based administration requires a centralized distribution system, and levels of 0.6 to 0.8 ppm F in drinking water are recommended (Australian Government, 2007). Particle size and humidity are critical to the successful fluoridation of salt; the recommended concentration is 250 ppm F (Marthaler and Petersen, 2005). Milk fluoridation requires the existence of a school milk program and administration of milk (0.65 mg/L/day) for the recommended 200 days per year (Bánóczy et al., 2009). All three systems require preliminary studies of fluoride exposure, strict epidemiological surveillance, and adequate occupational health practices. Since no special effort is required from the individual for ingesting fluoridated water, salt, or milk, these methods have been designated for automatic dental caries prevention relevant to public health (Petersen et al., 2012).
Professional Administration of Fluoride
Fluoride is administered topically as gels or varnishes. Gels contain 1.23% fluoride, and reports indicate significant caries reduction. Varnishes contain about 5% fluoride, and reviews indicate important reductions in caries in permanent and primary teeth. Silver fluoride or silver diamine fluoride at a concentration of 40% has been effective in preventing new caries and arresting active caries lesions in children. Frequency of application of topical fluoride depends on assessed caries risk and may not be justified in low caries risk or when populations are exposed to other sources of fluoride (Lo et al., 2012).
Self-Administered Fluoride
These include fluoride mouthrinses and fluoride toothpaste, which has been recognized as a main contributor to caries reduction. The effect of self-applied supervised use of fluoride mouthrinse (e.g., school-based) and fluoridated toothpaste can be greater than that of operator-applied and unsupervised home use. The effect of fluoridated toothpaste may increase with higher initial levels of caries. It increases when a higher fluoride concentration is used in the formulation (dose-response); health benefit for adults is significant only for concentrations of 1000 ppm and above. Higher-concentration fluoride toothpaste (> 1500 ppm F) may be associated with an increase in enamel fluorosis. Fluoride toothpaste has high acceptability. Fluoride mouthrinsing used in addition to fluoride toothpaste achieves a larger reduction in caries compared with that achieved by the use of toothpaste alone (Zero et al., 2012).
Fluoride Programs in Asia
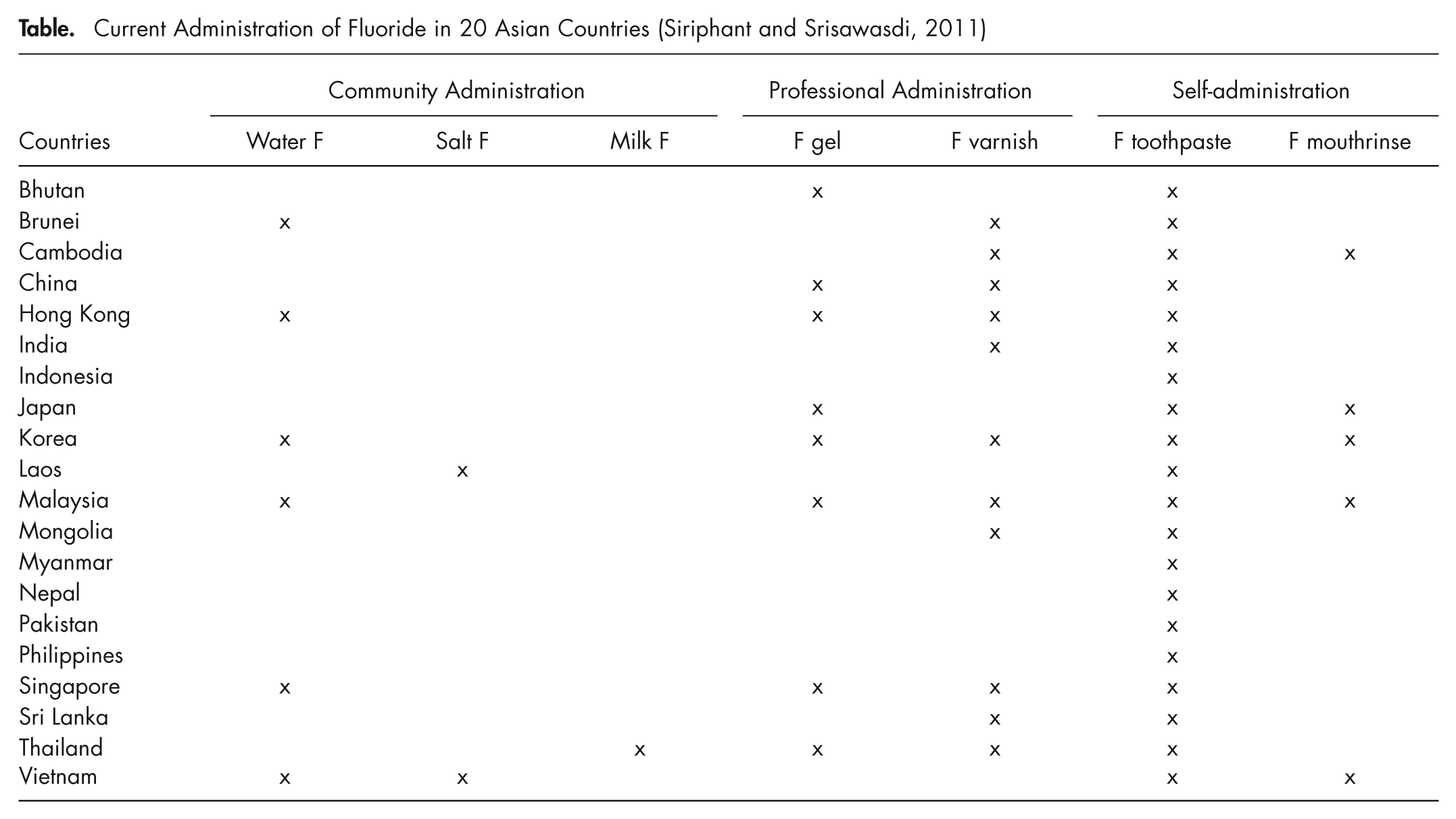
Traditionally, the burden of dental caries has been low in Asia, but during recent years the prevalence rates have grown markedly among children, adults, and older people. Much of the disease still remains untreated, or teeth are being extracted because of caries. This is particularly the case in low- and middle-income countries and among poor and disadvantaged population groups. Unfortunately, many countries in Asia have not been able to implement national health programs including fluoride (see Table), and the Phan-Nga meeting disclosed important barriers and opportunities to incorporating the use of fluoride (Siriphant and Srisawasdi, 2011). Prevention by the use of fluoride is most cost-effective and the only realistic way of reducing this public health burden. Taking account of the scientific evidence and the 2007 WHO World Health Assembly Resolution 60.17, participants confirmed that universal access to fluoride for dental health is a part of the basic human right to health. The statement is strongly supported by the International Association for Dental Research, the World Dental Federation FDI, and the World Health Organization, co-sponsors of the meeting.
Current Administration of Fluoride in 20 Asian Countries (Siriphant and Srisawasdi, 2011)
Footnotes
Acknowledgements
The authors are grateful for the valuable support to the workshop provided by Dr. Maria Fidela Navarro (IADR President), Dr. Roberto Vianna (FDI President), Dr. Adirek S. Wongsa (Dental Association of Thailand President), and Dr. Arunee Laiteerapong (J&J). The WHO Global Oral Health Programme is grateful to the Borrow Foundation for its continuous support of the work for oral health.
The authors received no financial support and declare no potential conflicts of interest with respect to the authorship and/or publication of this article.