
Abstract
There is a paucity of data for the effectiveness of reconstructive procedures in the treatment of peri-implantitis. The objective of this study was to compare reconstruction of peri-implant osseous defects with open flap debridement (OFD) plus porous titanium granules (PTGs) compared with OFD alone. Sixty-three patients (36 female, 27 male; mean age 58.4 y [SD 12.3]), contributing one circumferential peri-implant intraosseous defect, were included in a multinational, multicenter randomized trial using a parallel-group design. After OFD and surface decontamination using titanium brushes and hydrogen peroxide, 33 defects received PTGs. The implants were not submerged. All patients received adjunctive perioperative systemic antibiotics. The primary outcome variable (defect fill) was assessed on digitalized radiographs. Clinical measurements of probing depth (PPD), bleeding on probing (BoP), suppuration, and plaque were taken by blinded examiners. After 12 mo, the test group (OFD plus PTG) showed a mean radiographic defect fill (mesial/distal) of 3.6/3.6 mm compared with 1.1/1.0 in the control group (OFD). Differences were statistically significant in favor of the test group (P < 0.0001). The OFD plus PTG group showed a mean reduction in PPD of 2.8 mm compared with 2.6 mm in the OFD group. BoP was reduced from 89.4% to 33.3% and from 85.8% to 40.4% for the test and control groups, respectively. There was no significant difference in complete resolution of peri-implantitis (PPD ≤4 mm and no BoP at six implant sites and no further bone loss), because this finding was accomplished at 30% of implants in the test group and 23% of implants in the control group. Reconstructive surgery using PTGs resulted in significantly enhanced radiographic defect fill compared with OFD. However, limitations in the lack of ability to discern biomaterial from osseous tissue could not be verified to determine new bone formation. Similar improvements according to clinical measures were obtained after both surgical treatment modalities (ClinicalTrials.gov NCT02406001).
Keywords
Introduction
Peri-implant osseous defects are often the result of peri-implantitis defined as inflammation of peri-implant tissues accompanied by peri-implant bone loss with bleeding on probing (BoP) and/or suppuration (PuS), with or without concomitant deepening of peri-implant pockets (Lang and Berglundh 2011). According to recent reviews, this infectious condition has a prevalence of 20% in patients with implants (Klinge and Meyle 2012; Mombelli et al. 2012; Atieh et al. 2013; Derks and Tomasi 2015).
Various protocols, including mechanical debridement, the use of antiseptics and local or systemic antibiotics, as well as access and regenerative surgery, have been proposed for the treatment of peri-implantitis. There is currently no reliable evidence to identify the most effective intervention for treating peri-implantitis (Esposito et al. 2012).
Surgical methods are commonly applied for the management of moderate and advanced peri-implantitis (Aljateeli et al. 2012). One of the goals of surgical therapy is access for implant surface decontamination. An anti-infective protocol, incorporating surgical access, surface decontamination, and systemic antimicrobials was shown to be effective in a 12-mo follow-up (Heitz-Mayfield et al. 2011). Regenerative procedures, using bone grafts or bone substitutes, sometimes in combination with membranes, aimed at reconstructing peri-implant osseous defects have shown variable results (Khoury and Buchmann 2001; Roos-Jansåker et al. 2007a, 2007b; Schwarz et al. 2009; Schwarz et al. 2010; Roos-Jansåker et al. 2011; Aghazadeh et al. 2012; Wiltfang et al. 2012; Roos-Jansåker et al. 2014). However, there is only limited evidence available in the literature to compare the clinical effectiveness of reconstructive and nonreconstructive procedures (Khoshkam et al. 2013).
Porous titanium granules (PTGs) were recently introduced as an osteoconductive bone graft substitute for the treatment of peri-implant defects. A case report with human histology demonstrated that grafting of a peri-implant defect with PTGs could support reosseointegration of the implant with newly formed bone (Wohlfahrt et al. 2011). In a randomized controlled trial (RCT), Wohlfahrt et al. (2012) compared open flap debridement (OFD) (control group) with a surgical procedure placing PTGs (test group) for augmentation of peri-implant osseous defects in a submerged surgical technique, and they found significantly better radiographic peri-implant defect fill compared with the controls. In a case report, the reconstruction of a peri-implant defect with PTGs was preceded by implant surface debridement with a novel titanium brush and H2O2 (3%). Re-entry surgery after 6 mo revealed a complete integration of the bone replacement material in new bone, with no signs of loose particles (Wohlfahrt and Lyngstadaas 2012).
The objective of the present randomized trial was to compare reconstructive surgery of advanced peri-implant osseous defects with PTGs to OFD in a nonsubmerged technique, with the hypothesis of a significantly higher defect fill after 12 mo for the reconstructive procedure.
Materials and Methods
Study Design
This study was designed as a prospective multicenter, multinational, randomized parallel-group 12-mo clinical trial and is registered at ClinicalTrials.gov (NCT02406001). All investigators attended calibration meetings, in which preliminary cases were discussed and used to standardize case selection, clinical measurement techniques, and surgical procedures. On-site rules for the compilation of the data collection sheets for appropriate oversight were frequently reassured by a study monitor to ensure the validity of the data.
Study Population
Study participants were recruited consecutively from patients treated by experienced periodontists/implant dentists in Germany (University of Bonn), The Netherlands (Academic Centre for Dentistry Amsterdam), Italy (Rome University), Spain (Complutense University), and Sweden (Kristianstad University). After researchers provided a thorough explanation of the study procedure and its associated risks and benefits, each participant signed an informed consent form in accordance with the Declaration of Helsinki (1975, revised in 2008). The ethical committee for human subject trials at each institution approved the study protocol individually.
Seventy informed and consenting patients aged >18 y with a diagnosis of peri-implantitis were enrolled in the study and surgery was performed. Seven patients were withdrawn early at surgery, because the defect around the implants did not meet the inclusion criteria. After surgery, 63 patients (36 female and 27 male; mean age 58.4 y [SD 12.3] ; range, 26 to 88 y) remained in the study (n = 33, test group; n = 30, control group). A study flow chart is presented as Fig. 1.
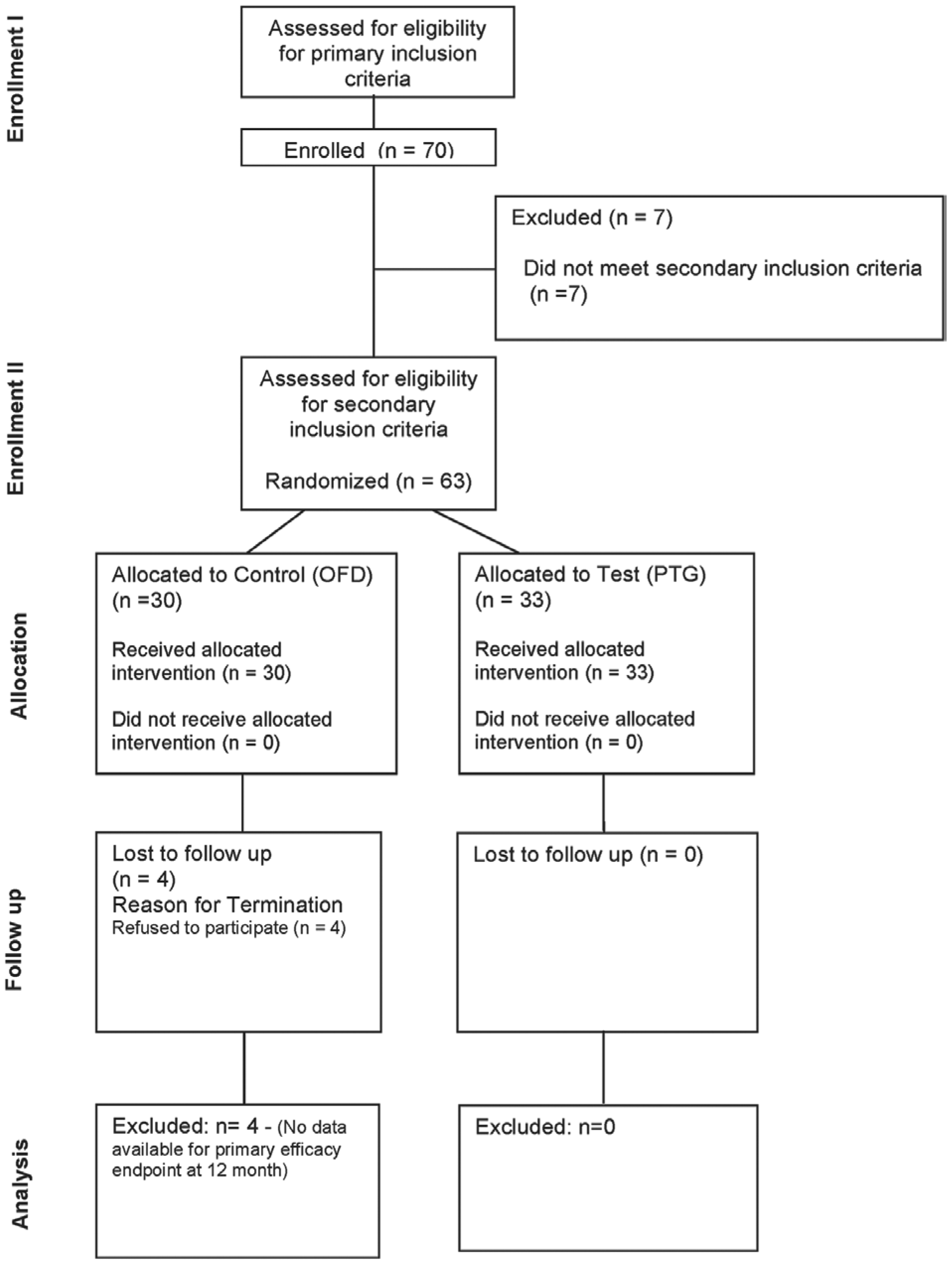
Study flowchart following CONSORT (Consolidated Standards of Reporting Trials) guidelines for clinical trials. Sixty-three patients met secondary inclusion criteria, 30 patients were allocated to the control group (OFD: open flap debridement), and 33 to the test group (PTG: porous titanium granules). Four patients in the control group were lost to follow-up.
Inclusion and Exclusion Criteria
All implants had to be in function for >12 mo. In patients with more than one peri-implant defect meeting the inclusion criteria, only one implant per patient was defined as the target (the most severe defect) and included in the study.
The primary inclusion criteria were as follows. An initial radiographic evaluation was performed and patients were included if they had an intraosseous defect ≥3 mm on a standard intraoral radiograph. Clinical evaluation was performed and patients were included if they met one of the following peri-implant probing depth (PD) ≥5 mm, BoP, and/or PuS. Using intraoperative exploration, patients were accessed for the following secondary inclusion criteria: intraosseous defect component ≥3 mm at the deepest point, three to four walls, defect with at least 270° (circumferential), and a defect angle ≤35° (from the axis of the implant).
The exclusion criteria were as follows: presence of diabetes mellitus (hemoglobin A1c ≥6.5), use of corticosteroids or other anti-inflammatory prescription drugs, use of medications known to induce gingival hyperplasia, a history of taking systemic antibiotics in the preceding month, pregnant or nursing, implants placed in grafted bone or previously augmented with bone/bone substitute, implants previously surgically treated for peri-implantitis, or a mobile implant.
Presurgical Treatment and Evaluation
All necessary periodontal treatments were finished as evaluated by a full periodontal examination with recording of pocket probing depth (PPD), full-mouth bleeding, and plaque scores at least 1 mo prior to the peri-implant surgical procedure and before entry into the study. Presurgical interventions included providing oral hygiene instructions according to the patients’ individual needs, nonsurgical periodontal/peri-implantation, and surgical periodontal therapy.
Patients who met all inclusion criteria, verified at surgery, underwent investigational procedures. Baseline measurements at the included implant were performed on the same day as the surgical procedure.
Radiographic Measurements
Intraoral periapical radiographs were obtained of implants in a standardized way using Eggen holders and long-cone–equipped dental X-ray units. All radiographs presenting study implants were digitalized, coded, and evaluated by MATLAB software (version R2013b for Mac OS 10.9; Mathworks, Natick, MA, USA).
Radiographs were studied by changing parameters in black and white modes as well as in color look-up tables. Measurements from a well-defined reference point at the coronal part of the implant body taken at the baseline, 6-mo, and 12-mo visits were as follows: vertical defect depth and width, marginal bone level, and horizontal bone level (Fig. 2, Appendix Fig.). Based on these measurements, changes in vertical defect depth, marginal bone level, percent defect fill, and percent defect resolution from baseline to 12 mo were calculated.
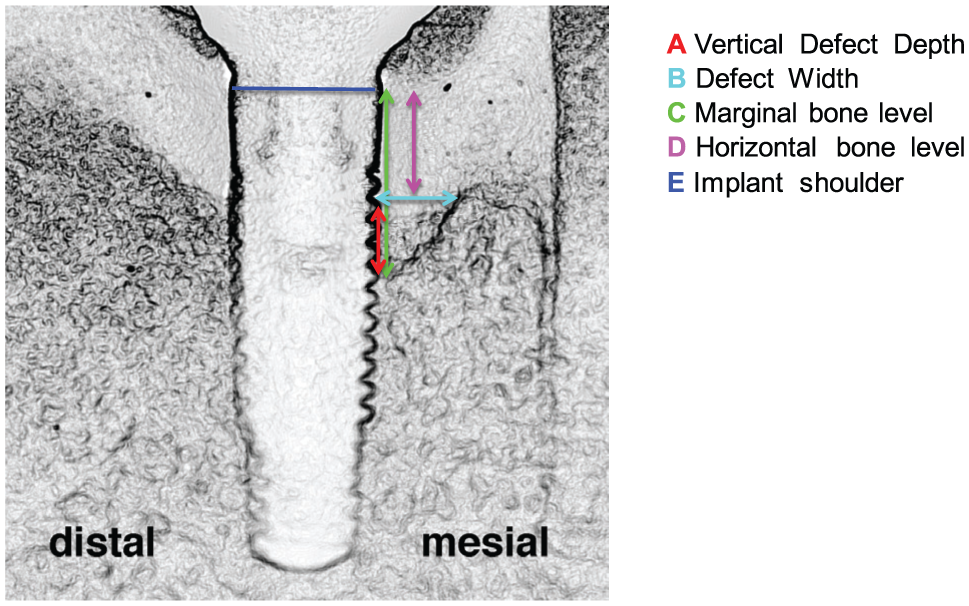
Radiographic measurements at baseline and after 12 mo.
The most coronal confluent aggregation of bone or bone with graft material was used to define marginal and horizontal bone levels. Titanium particles without visible mineralized tissue adjacent to the implant did not count as most coronal bone-to-implant contact. Likewise, single isles of bone or bone-like material were not considered.
Implant length and width or known dimensions of implant threads were used as reference for calibration of measurements. Radiographic evaluations were initially performed by an independent physicist (P.N.J.) with high expertise in image analysis, who was not involved in other aspects of the study. He had previously been extensively trained by a periodontist experienced in oral radiology on sample images on a LCD display with a resolution of 2560 × 1600 and a 32-bit color pixel depth. All measurements performed were saved as graphics placed on top of the corresponding image and were then independently confirmed by two periodontists. No double measurements of radiographs were performed. If differences were >0.1 mm, the three calibrated investigators reanalyzed the respective implant together to reach a consensus (Enkling, Jöhren, Klimberg, Bayer, et al. 2011; Enkling, Jöhren, Klimberg, Mericske-Stern, et al. 2011; Enkling et al. 2013).
Clinical Measurements
For proper standardization between baseline and re-evaluation data, only one examiner took all of the clinical measurements in each study center. All probing measurements were obtained with a pressure (0.20 to 0.25 N)–sensitive probe (Click-Probe, Kerr, Switzerland) to the nearest millimeter at six sites per implant (mesiobuccal, buccal, distobuccal, distopalatal, palatal, and mesiopalatal).
At the baseline and 12-mo visits, measurements of PPD, BoP, PuS, and plaque were taken. BoP and PuS at the affected implants were assessed within 30 s after probing. At surgery, intraoperative measurements included defect depth (in millimeters) at the deepest point, defect circumference (in degrees), defect walls (in numbers), and defect width (in millimeters).
Sample Size Calculation/Power Analysis
The calculation of the number of patients to be treated (sample size) was based on a previous proof-of-concept single-center RCT (Wohlfahrt et al. 2012) and the primary objective to detect a true mean difference of at least 2 mm between test and control treatment for radiographic defect fill after 12 mo. With a level of significance of alpha = 0.05 in a two-sided hypothesis and 90% power, the number of patients needed was 48. Assuming a dropout rate of approximately 30%, the total number of patients required was 60.
Patients were randomly assigned to the treatment modality by using a computerized randomization scheme prepared prior to study initiation, and they were randomly assigned to treatment in blocks of six individuals. The patients were allocated to either reconstruction of the defect with PTG (test) or closure of the flap after implant debridement (OFD/control). Documentation of treatment allocation for each patient was placed in separate, sealed opaque envelopes that were opened and revealed to the surgeon after the defect was debrided and the implant surface was finished. Clinical examiners and the statistician remained blinded to the treatment assigned.
Interventions
A nonsubmerged surgical technique was used for both the test and control sites. After administration of local anaesthesia, the flap elevation procedure included an intracrevicular incision around the implant. Full-thickness mucoperiosteal flaps were raised on the buccal and lingual aspects to gain access to the complete peri-implant defect and to the implant surface. The size of the flap was determined by supracrestal incisions extending mesial and distal of the implant site. Vertical incisions into the vestibule at a distance of at least one tooth/implant from the implant were performed as necessary for adequate access. Granulation tissue was removed using titanium curettes (HuFriedy, Chicago, IL, USA), and the exposed implant surfaces were cleaned mechanically by using a rotary titanium brush (Tigran PeriBrush; Tigran Technologies, Malmö, Sweden) and decontaminated chemically with 3% H2O2 for 1 min, followed by rinsing with saline for 60 s (2 × 20 ml).
After treatment allocation in accordance to randomization, Tigran titanium granules (Tigran Technologies) were applied into the intraosseous defects of the test sites. After insertion of the granules, excess material was carefully removed. Flaps were then repositioned and sutured back into position using monofilament nonresorbable sutures.
For the perioperative protocol, patients were prescribed a combination of amoxicillin 500 mg thrice daily and metronidazole 400 mg twice daily for 8 d, starting 1 d before surgery. Patients were then instructed to rinse twice daily with chlorhexidine mouth rinse (0.2%) for 1 mo. The patients used brushes as usual in other areas of the mouth. Anti-inflammatory and analgesic therapy was prescribed (ibuprofen 600 mg thrice daily) during the first 2 d and according to the patients’ individual needs thereafter.
The sutures were removed after 7 to 14 d and patients were instructed on the use of soft toothbrushes and soft interdental brushes (super soft Gentle/Implant Care; TePe, Malmö, Sweden) in the surgical area.
Patients were recalled at 6 wk and 3, 6, 9, and 12 mo after surgery for professional oral hygiene procedures with supragingival debridement and hygiene instructions provided as needed.
Predefined early withdrawal criteria were as follows: nonhealing infections, substantial exfoliation of graft material (rejection), local intolerance to graft material, recurrence of active peri-implantitis at the test site, loosening of the implant, or poor patient compliance (not returning for control visits).
Statistical Analysis
The primary outcome was defect fill, as assessed by changes in the radiographic marginal bone level and vertical defect depth. Secondary outcomes were changes in PPD, BoP, PuS, and plaque.
Analysis was performed using SAS software (version 9.2; SAS Institute Inc., Cary, NC, USA). All patients included in this study had surgery performed and were analyzed for side effects. Four patients were excluded from analysis because there were no data available at 12 mo (Fig. 1).
Statistical analysis of primary efficacy end point measures was performed using study center as the stratification variable. Because a significant interaction between baseline measurements and treatment was observed for vertical defect depth measures, a stratified Wilcoxon test (van Elteren 1960; Lehmann 1975) was applied.
Treatment intergroup comparisons of secondary efficacy end points were based on least-squares means obtained from the analysis of covariance model. Means for each treatment group and differences between treatment groups are presented, along with associated 95% confidence intervals (95% CIs) as well as P values for differences within treatment groups.
The statistical hypotheses for the defect fill (in millimeters) primary outcome were as follows: H0: Δ Marginal bone leveltest – Δ Marginal bone levelcontrol = 0 and H1: Δ Marginal bone leveltest – Δ Marginal bone levelcontrol ≠ 0; and H0: Δ Vertical defecttest – Δ Vertical defectcontrol = 0 and H1: Δ Vertical defecttest – Δ Vertical defectcontrol ≠ 0.
For percent changes, the statistical hypotheses were based on the following equations:


If the P value from this analysis fell below 0.05 in both mesial and distal measurements, it was concluded that there was a statistically significant difference in the average change between the two treatment groups.
Results
Between February 2010 and December 2013, a total of 105 patients were consecutively recruited at the five study centers (16 to 36 per center). Seventy patients fulfilled the primary inclusion criteria, and 63 fulfilled the secondary inclusion criteria and were randomized to the test (n = 33) and control (n = 30) groups. Four patients in the control group refused to participate at the 12-mo recall appointment and were lost to follow-up. The number of participants per center ranged from 10 to 13. Baseline characteristics and demographics for patients in the two study groups are presented in Table 1.
Patient Characteristics at Baseline.
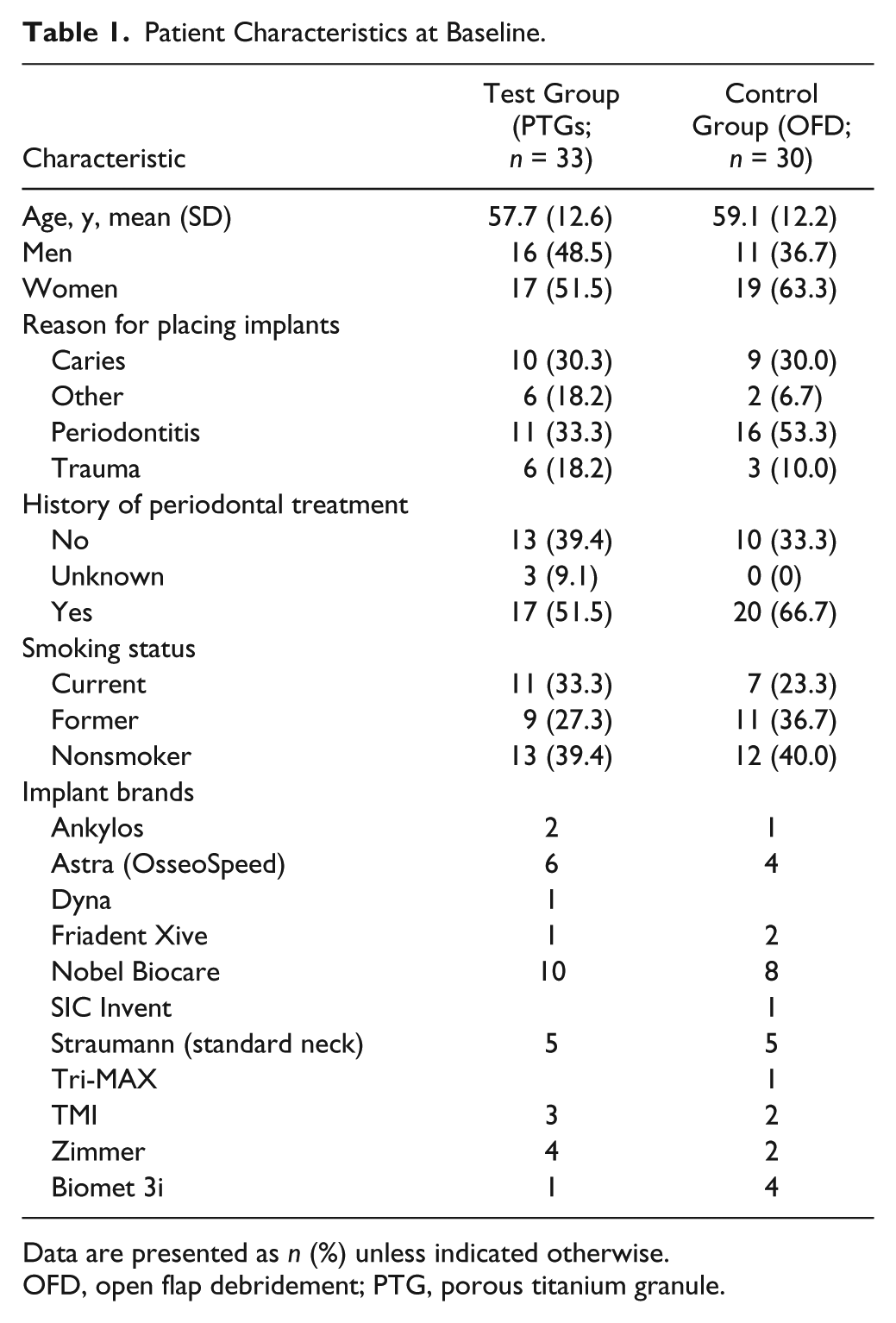
Data are presented as n (%) unless indicated otherwise.
OFD, open flap debridement; PTG, porous titanium granule.
Radiographic and clinical findings are presented in Table 2, and effects of treatment as shown by changes in radiographic and clinical parameters are presented in Table 3. Significantly higher reductions in vertical defect depth and gains in marginal bone level favored the PTG reconstructed group (P < 0.0001). After 12 mo, the mean gain of marginal bone level for the test group was 3.61/3.56 mm (mesial/distal) compared with 1.05/1.04 mm (mesial/distal) in the OFD group. This corresponded to a mean defect fill for the PTG-treated sites of 79.00%/74.22% (mesial/distal) compared with 23.11%/21.89% (mesial/distal).
Radiographic and Clinical Parameters at Baseline and 12 mo.
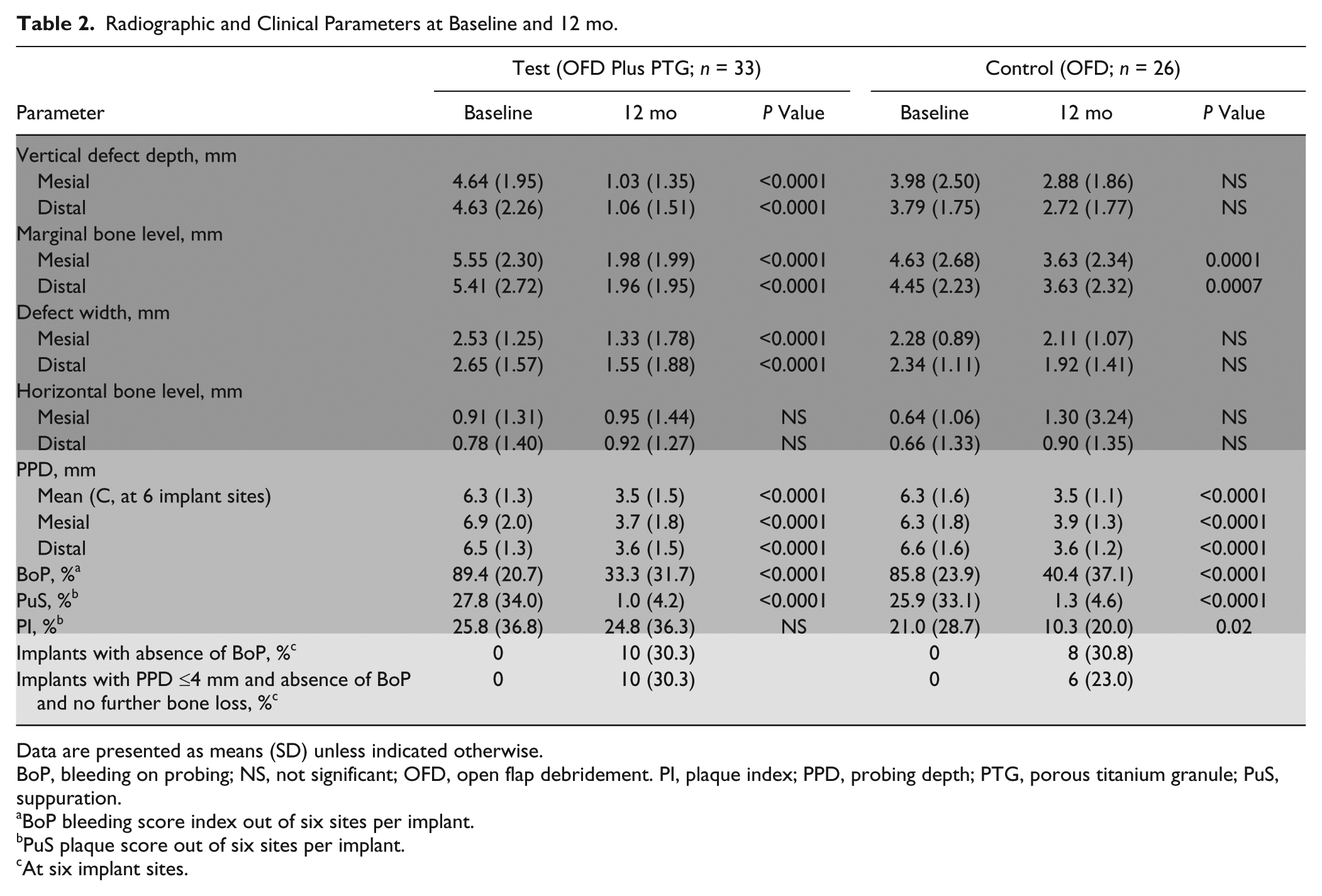
Data are presented as means (SD) unless indicated otherwise.
BoP, bleeding on probing; NS, not significant; OFD, open flap debridement. PI, plaque index; PPD, probing depth; PTG, porous titanium granule; PuS, suppuration.
BoP bleeding score index out of six sites per implant.
PuS plaque score out of six sites per implant.
At six implant sites.
Change in Radiographic and Clinical Parameters between Baseline and 12 mo.
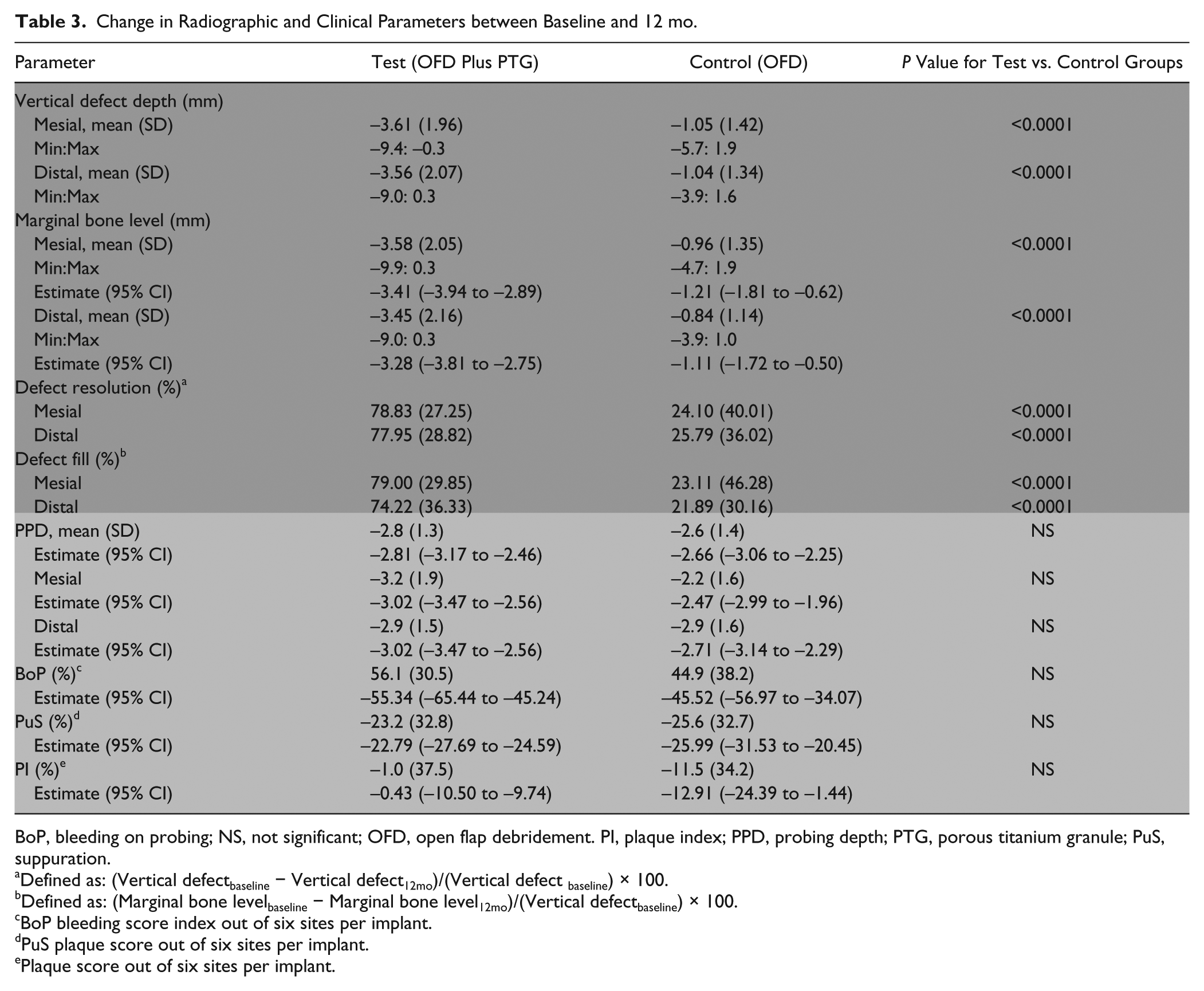
BoP, bleeding on probing; NS, not significant; OFD, open flap debridement. PI, plaque index; PPD, probing depth; PTG, porous titanium granule; PuS, suppuration.
Defined as: (Vertical defectbaseline − Vertical defect12mo)/(Vertical defect baseline) × 100.
Defined as: (Marginal bone levelbaseline − Marginal bone level12mo)/(Vertical defectbaseline) × 100.
BoP bleeding score index out of six sites per implant.
PuS plaque score out of six sites per implant.
Plaque score out of six sites per implant.
No differences in changes in defect width and horizontal bone level could be observed (Appendix Table).
The test group showed a mean reduction in PPD of 2.8 mm (SD 1.3) compared with 2.6 mm (SD 1.4) in the OFD group. Reductions for BoP amounted to 56.1% for the test group compared with 44.9% for the control group. Intergroup differences for PPD or BoP reduction were not significantly different.
In both treatment groups, 30% of implants showed disease resolution by absence of any BoP, whereas 30% (test) and 23% (control) of implants demonstrated successful peri-implantitis therapy by the use of a composite outcome that also included shallow pockets and no further bone loss (Table 2).
None of the patients treated demonstrated subjective or objective side effects, such as pronounced pain, manifest inflammatory reactions, discoloration of the surrounding mucosa, or patient morbidity, beyond what is normally expected for similar surgical procedures.
Discussion
This randomized multinational, multicenter trial demonstrated additional benefits after reconstructive surgery with application of PTGs in combination with an open flap nonsubmerged debridement procedure for the treatment of advanced peri-implant osseous defects compared with OFD alone. Mean radiographic defect fill, as the primary outcome, amounted to 3.6 mm, translating into a mean defect fill of approximately 79%, which was significantly higher than the 1.0 mm (22%) observed in the control group. Thus, the study null hypothesis assuming no difference in defect fill could be rejected.
With regard to secondary outcome measures, there were no statistically significant differences in the reduction of pocket depths and BoP. Both surgical treatment modalities resulted in marked improvements of the clinical conditions.
To our knowledge, this is the largest published randomized trial to evaluate the effectiveness of reconstructive peri-implant surgery and it is one of the very few studies that used OFD for comparison, as demanded by a recent systematic review (Khoshkam et al. 2013). This study adopted the current guidelines for quality of methods and reporting for studies of the efficacy of therapeutic approaches to peri-implant diseases (Graziani et al. 2012) from a recent consensus conference, in which multicenter approaches were encouraged (Sanz and Chapple 2012). The fact that different surgeons in a variety of settings treated a wide range of implant types enhances the generalizability of the obtained results.
There are also some limitations inherent in any study of the present design. First, a radiographic examiner cannot be blinded due to the use of a radiopaque bone substitute. We tried to compensate for this shortcoming by employing three independent calibrated examiners. Second, the amount of bone fill has to be interpreted with caution whenever radiopaque bone substitutes are used. In this regard, the choice of a distinctly visible material such as titanium granules may have advantages compared with other nonresorbable/slow-resorbable bone substitutes (e.g., natural bone mineral/deproteinized bone xenograft), because it can be more clearly distinguished from the surrounding bone. The possibility of pure “X-ray cosmetics” becomes less likely. Third, it has to be realized that reosseointegration/regeneration cannot be evaluated by a clinical study. Regarding the healing of PTG applied to peri-implant osseous defects, two case reports (one using human histology and the other using a re-entry procedure) can help to interpret the radiographic findings of our study. Human histology demonstrated that grafting of a peri-implant defect with PTGs could support reosseointegration of the implant with newly formed bone (Wohlfahrt et al. 2011), and re-entry surgery of a treated peri-implant defect after 6 mo revealed a complete integration of the bone replacement material in new bone, with no signs of loose particles (Wohlfahrt and Lyngstadaas 2012). Further evidence comes from recently published clinical studies on the use of PTGs for sinus augmentation, in which biopsies employing histological and micro–computed tomography analyses confirmed osteoconductive properties of porous titanium granules (Vandeweghe et al. 2013; Verket et al. 2013; Dursun et al. 2015; Lyngstadaas et al. 2015).
Another possible shortcoming in this study was the fact that the interexaminer agreement for the clinical parameters could not be assessed as a result of logistical and financial constraints. All clinical examiners were very experienced and had shown good intraexaminer reproducibility in the past, and measures were taken to standardize the probing assessment as much as possible. In particular, the use of a pressure-sensitive probe was considered to be very important for the reliable and reproducible assessment of peri-implant bleeding (Lang et al. 2000). Any bias resulting from a possible low interexaminer reproducibility would have affected, both the test and control groups, to a similar extent, and therefore most likely would have not affected the outcome of the efficacy analysis of this RCT.
Another possible confounder could be the distribution of different implant types in the test and control groups. Although there are currently no data from clinical studies on the influence of implant microstructure and other surface characteristics on the response to reconstructive treatment, the possible impact of such implant features on the outcomes cannot be ruled out.
All four of the patients who dropped out were from the control group. This could also have an effect on the results. We checked the baseline characteristics of these four individuals and were able to confirm that they were not outliers in any aspect.
The results of our study compare favorably with the weighted means of 2.17 mm (95% CI, 1.46 to 2.87 mm), 2.1 mm (95% CI, 1.47 to 2.72 mm), and 2.16 mm (95% CI, 1.36 to 2.96 mm), respectively, for radiographic defect fill reported in recent systematic reviews on the outcomes of reconstructive/regenerative procedures in the treatment of peri-implantitis (Khoshkam et al. 2013; Chan et al. 2014).
Comparing the results of the present multicenter RCT with the previous single-center RCT on the use of PTGs (Wohlfahrt et al. 2012), similar differences were seen. Wohlfahrt et al. (2012) used a submerged design for the healing phase, and their results showed that radiographic peri-implant defect fill was significantly increased with application of PTG (2.0 ± 1.7 mm) compared with the nongrafted control group (0.1 ± 1.9 mm). Although both studies used systemic antibiotics, differences in flap design and, in particular, characteristics of the peri-implant osseous defects treated might be responsible for the difference in the magnitude of the outcomes (Schwarz et al. 2010). Another contributing factor could be the implant decontamination procedure. Wohlfahrt et al. (2012) used titanium curettes and 24% ethylenediaminetetraacetic acid (EDTA), whereas a titanium brush in combination with 3% H2O2 was employed in this study. When comparing control groups of the two studies, differences in radiographic defect fill are obvious, because our control group showed an average defect reduction of 1 mm after 12 mo. By contrast, in the earlier investigation, the nongrafted control group did not improve at all after treatment (0.1 ± 1.9 mm). In our study, anti-infective OFD using a titanium brush with H2O2 decontamination of the implant surface even led to complete radiographic bone fill up to the implant shoulder in one implant. Finally, a retrospective cohort study using PTGs for peri-implantitis lesions in 18 implants in 16 patients reported a reduction of mean bone loss from 4.4 mm to 2.3 mm (Mijiritsky et al. 2013).
With regard to secondary outcomes, this study showed marked clinical improvements by reduction in inflammation (BoP and PuS) and reduction in mean PPD in both treatment groups. Mean BoP reductions of 56% in the test group compare favorably with the weighted mean of 45.8% in a recent systematic review (Koshkam et al. 2013). The proportion of implants with absence of any bleeding at six sites amounted to 30% in both groups. Likewise, mean PPD reductions of 2.8 mm in the test group are in concert with the weighted mean of 2.9 mm in a recent meta-analysis (Koshkam et al. 2013). PPD reductions in the control group are in agreement with a recent meta-analysis of studies using access flap and debridement (Chan et al. 2014). In interpreting these findings, a significantly improved full-mouth plaques score in the control group, which was not seen in the test group, should be kept in mind.
The use of composite therapeutic end points for the surgical management of peri-implantitis was recently recommended (Sanz and Chapple 2012), and these end points were applied in our study. Disease resolution by presence of shallow pockets without any bleeding at six sites of the implants and no further bone loss could be demonstrated for 30% of implants in the test group and 23% of implants in the control group. Although such an end point would be the ideal goal of peri-implantitis therapy and would be a measure of success, no other studies have yet reported such composite outcomes (Heitz-Mayfield and Mombelli 2014).
In this study, no barrier membrane was used to cover the bone substitute. For the contained defects, this additional measure would add more costs and was not felt to be necessary, although a recent meta-analysis demonstrated higher PD and BoP reduction after grafts and barrier membranes than after grafts alone (Chan et al. 2014). A long-term follow-up study showed a significantly better outcome after natural bone mineral in combination with a collagen membrane compared with a resorbable hydroxyapatite after 4 y (Schwarz et al. 2009). By contrast, Roos-Jansåker et al. (2014) found no additional effect from the application of a barrier membrane to a bone graft. Future studies will have to show whether membranes or the use of a nonresorbable/slow-resorbable bone substitute are of key importance to ensure long-term stability of the results of reconstructive peri-implant surgery.
Within the limitations of this study, it can be concluded that surgical treatment approaches that included the use of a titanium brush for implant surface decontamination and adjunctive systemic antibiotics have shown promising results for the treatment of advanced peri-implant osseous defects. No significant differences were observed regarding the clinical outcomes of bleeding and pocket reduction as well as for complete resolution of peri-implantitis between the test and control procedures. The radiographic findings must be interpreted with caution, because it is difficult to discern biomaterial and newly formed osseous tissue. Therefore, the relevance and potential benefit of an enhanced radiographic defect fill after application of PTGs into three- and four-wall defects must be evaluated by further histological studies and a long-term clinical follow-up.
Author Contributions
K. Jepsen, S. Jepsen, M. Sanz, contributed to conception, design, data acquisition, analysis, and interpretation, drafted and critically revised the manuscript; M.L. Laine, D. Anssari Moin, B. Zeza, contributed to data acquisition, analysis, and interpretation, critically revised the manuscript; A. Pilloni, contributed to conception and design, critically revised the manuscript; A. Ortiz-Vigon, A.M. Roos-Jansåker, contributed to data acquisition, critically revised the manuscript; S. Renvert, contributed to conception, design, data analysis, and interpretation, critically revised the manuscript.
Footnotes
Acknowledgements
The authors thank Professors B.G. Loos and D. Wismeyer (University of Amsterdam, The Netherlands) for contributing expertise and support, Paul Niklas Jepsen (Department of Physics, Massachusetts Institute of Technology, Cambridge, MA, USA) for expertise in performing MATLAB visual analysis on the radiographs, Pernilla Olausson for statistical analysis, and Eva Lundberg for study monitoring.
The clinical trial was supported by a research grant from Tigran Technologies AB. S.J. has institutional grant support from the German Research Foundation and in the past from Geistlich Pharma and Straumann. M.L.L. and D.A.M. have grant support from Biomet 3i. A.P. was previously a member of the scientific advisory board of Tigran Technologies. M.S. has grant support from Nobelbiocare, Straumann, Sweden & Martina, MIS, and Geistlich Pharma and fees from Nobelbiocare, Straumann, and Geistlich Pharma. S.R. is a shareholder and was previously a consultant and member of the scientific advisory board of Tigran Technologies and has grant support from Geistlich Pharma.
The authors declare no further potential conflicts of interest with respect to the authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.