
Abstract
Dental caries is considered a diet-mediated disease, as sugars are essential in the caries process. However, some gaps in knowledge about the sugars-caries relationship still need addressing. This longitudinal study aimed to explore 1) the shape of the dose-response association between sugars intake and caries in adults, 2) the relative contribution of frequency and amount of sugars intake to caries levels, and 3) whether the association between sugars intake and caries varies by exposure to fluoride toothpaste. We used data from 1,702 dentate adults who participated in at least 2 of 3 surveys in Finland (Health 2000, 2004/05 Follow-up Study of Adults’ Oral Health, and Health 2011). Frequency and amount of sugars intake were measured with a validated food frequency questionnaire. The DMFT index was the repeated outcome measure. Data were analyzed with fractional polynomials and linear mixed effects models. None of the 43 fractional polynomials tested provided a better fit to the data than the simpler linear model. In a mutually adjusted linear mixed effects model, the amount of, but not the frequency of, sugars intake was significantly associated with DMFT throughout the follow-up period. Furthermore, the longitudinal association between amount of sugars intake and DMFT was weaker in adults who used fluoride toothpaste daily than in those using it less often than daily. The findings of this longitudinal study among Finnish adults suggest a linear dose-response relationship between sugars and caries, with amount of intake being more important than frequency of ingestion. Also, daily use of fluoride toothpaste reduced but did not eliminate the association between amount of sugars intake and dental caries.
Introduction
Dental caries is considered a diet-mediated disease, as sugars are essential in the caries process (Burt and Pai 2001; Sheiham 2001; Moynihan and Petersen 2004; Zero 2004; Moynihan and Kelly 2014). A question that needs urgent attention is the shape of the dose-response relationship between sugars and caries, as it is central to decisions about the level of sugars compatible with low levels of dental caries (Moynihan and Kelly 2014). Studies in Japanese children during World War II reported a linear (ecologic) relationship between the log of annual caries incidence rate and national sugars consumption per capita per year (Takeuchi 1961; Koike 1962). Later, Newbrun (1982) suggested a sigmoid dose-response curve, based on evidence from animal studies, which became the accepted basis for establishing a limit on sugars intake (Sheiham 2001). A reappraisal of the Japanese ecologic data suggested a curvilinear dose-response relationship between annual per capita sugars consumption and annual caries incidence (Sheiham and James 2014a, 2014b).
Another question that needs addressing is the relative importance of frequency versus amount of sugars intake for caries development. The answer to that will influence health education advice on how to reduce caries. Some believe that the frequency of intake influences the sugars-caries relationship more than the amount (Touger-Decker and van Loveren 2003; Anderson et al. 2009). However, 2 longitudinal studies showed that caries increment in children was more strongly related to amount of sugars intake than to frequency (Rugg-Gunn et al. 1984; Burt et al. 1988; Rugg-Gunn 1993; Szpunar et al. 1995), although in both studies amount and frequency of sugars intake were modeled separately. A strong positive correlation (r = 0.77) between amount and frequency of sugars intake was also reported in 1 of those studies (Rugg-Gunn et al. 1984).
It has been suggested that the relationship between sugar intake and caries is much weaker in populations with widescale fluoride exposure than in those prior to fluoride toothpaste being widely available (Burt and Pai 2001; Touger-Decker and van Loveren 2003). Fluoride alters the dose-response relationship between sugars and caries, as it delays when cavitation occurs for a given level of sugars (Zero 2004). The use of fluoride toothpaste may reduce the strength of the association between frequency of sugars intake and caries incidence (Duggal et al. 2001; Bernabé et al. 2014), but nothing is known in terms of amount of sugars intake. Therefore, a third important question to address is whether the dose-response relationship between sugars and caries is affected by fluoride in adults. A recent review identified only 3 prospective studies in adults. All were conducted before fluoride toothpaste was widely available (Moynihan and Kelly 2014).
To fill these gaps in knowledge, this longitudinal study explored 1) the shape of the association of frequency and amount of sugars intake with caries in adults, 2) the relative contribution of frequency and amount of sugars intake to caries levels, and 3) whether the association of frequency and amount of sugars consumption with caries varies according to exposure to fluoride.
Methods
The present study adheres to the STROBE statement (Strengthening the Reporting of Observational Studies; Vandenbroucke et al. 2007).
Data Source
We used data from 3 surveys in Finland (Fig. 1). The Health 2000 Survey conducted in 2000–2001 was a national survey of the Finnish population that include 8,028 adults aged ≥30 y, recruited via stratified 2-stage cluster sampling (Aromaa and Koskinen 2004). A total of 6,335 subjects (79%) had clinical oral examinations. Of them, 5,389 (85%) were dentate, with complete data on dental status. A follow-up study in 2004–2005 included 2,000 adults randomly selected from the list of participants who had attended the oral examinations in the Health 2000 Survey. People who died or were edentate and, for logistic reasons, those in health center districts where <15 subjects had been sampled were excluded. The final sampling frame comprised 1,248 subjects who were invited to a clinical oral reexamination; 1,049 participated (84%). The Health 2011 Survey was a follow-up study of the Health 2000 Survey. All participants of the Health 2000 Survey alive and living in Finland were invited. The sample of those aged ≥30 y in 2011 consisted of 7,964 adults, of whom 5,806 (73%) participated in at least one part of the study and 4,221 (53%) in the health examination. Only those adults living in southern or northern Finland (2 of the 5 examination areas, n = 3,713) were invited to participate in a new oral examination, and 1,496 agreed (40%).
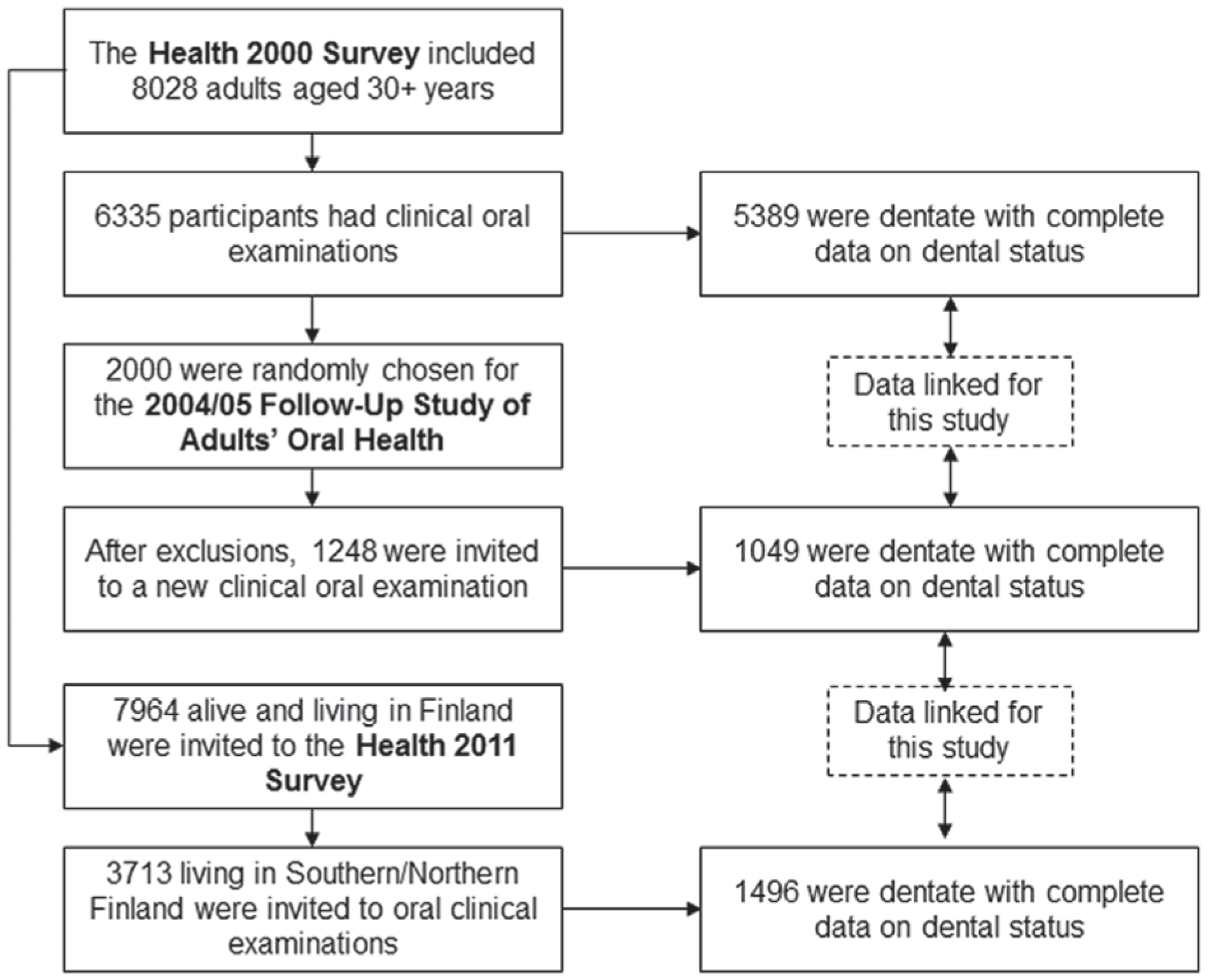
Flowchart of participation and data linkage for the 3 surveys: Health 2000, 2004/05 Follow-up Study of Adults’ Oral Health, and Health 2011.
There were 1,889 dentate adults (aged 30 to 89 y at baseline) who had caries data in at least 2 of 3 surveys (baseline plus 2004–2005 and/or 2011), of which 187 (10%) were excluded for missing data on covariates. Caries data were available for 1,702, 902, and 1,009 participants in 2000, 2004, and 2011, respectively. Furthermore, 1,493 (88%) contributed to 2 waves of caries data and 209 (12%) to all 3 waves.
Variable Selection
Food consumption was measured in the Health 2000 Survey (baseline data) with a validated food frequency questionnaire (FFQ), including 128 commonly used or nutritionally important food items and mixed dishes (Mannisto et al. 1996; Paalanen et al. 2006). Participants were asked to estimate the consumption frequency of each food item during the past 12 mo on a 9-point scale, from never or rarely to 6 times a day or more often. A standard portion size was assigned to each FFQ item and specified with natural units (piece, slice, glass, tablespoon, etc.). When returned, questionnaires were checked for unreliable answers by a nutritionist. The overall frequency of sugars intake (times/d) was estimated by adding the weighted responses (e.g., 0.143 for once a week, 2.5 for 2–3 times a day, and 6 for 6 times a day or more often) for 15 sugary items (coffee bread, Danish pastries, sweet pies, cakes, biscuits/cookies, fruit curd, pancakes, ice cream, chocolate, liquorice, candies, sugared coffee/tea, cocoa, fruit juices, and sweetened soft drinks). The amount of sugars intake (g/d) was estimated by multiplying the food consumption frequency by fixed portion sizes. The ingredients of mixed foods were broken down into their components as well as the contents of different nutrients via the Finnish Food Composition Database (Fineli; National Institute for Health and Welfare, Helsinki, Finland).
Demographic, socioeconomic, and behavioral factors at baseline were considered as potential confounders. Socioeconomic position was indicated by participants’ education (basic, secondary, or higher). Dental behaviors included dental attendance pattern reported on a 3-point scale (regularly for checkups, only for emergencies, or never), toothbrushing frequency on a 5-point scale (more often than twice a day, twice a day, once a day, less often than every day, or never), and use of fluoride toothpaste on a 4-point scale (daily, weekly, less often, or never).
Identical clinical oral examinations were conducted at baseline and follow-ups and were independent of participants’ completion of questionnaires. Clinical examinations were performed by dentists, with each participant seated on a dental chair and with the use of headlamps, fiber optic light, mouth mirror, and a World Health Organization periodontal probe. Teeth were blown dry before inspection and cotton rolls used to keep them dry while inspected. A tooth was recorded as decayed if there was evidence of a carious lesion clearly extending into dentine on any coronal or root surface. The carious lesion had to be cavitated, to have penetrated the fissure and undermined the enamel, or the dentine walls to be clearly softened. All the examiners (in 2000–2001, 2004–2005, and 2011) received similar training given by the same experienced dentists. The overall kappa value for inter- and intraexaminer reliability at the baseline survey was 0.87 and 0.95 at tooth level, respectively (Suominen-Taipale et al. 2004; Suominen-Taipale et al. 2008). The sum of decayed, missing, and filled teeth, or DMFT index, was estimated from each wave and used as a repeated outcome measure.
Statistical Analysis
Linear mixed effects models were used to estimate the longitudinal association between sugars intake at baseline and DMFT levels over 11 y. Linear mixed effects models use all available data over the follow-up, handle unequally spaced observations over time, and take into account the fact that repeated measures on the same individual are correlated (Singer and Willett 2003; Twisk 2013). We fitted both the intercept and the slope as random effects, allowing individual differences in DMFT level at baseline and rate of DMFT increment. All analyses were run in Stata 13 via the mixed command.
We first explored the shape of the dose-response relationship of frequency and amount of sugars intake with DMFT levels using fractional polynomials, a flexible family of parametric models that allows modeling curvilinear associations (Royston and Altman 1994; Royston et al. 1999). Briefly, the model deviance of each of 8 powers (–2, –1, –0.5, 0, 0.5, 1, 2, and 3, where a power of 0 is the log function and a power of 1 the straight line) was used to identify the best-fitting first-order polynomial. All 36 combinations of pairs of these powers were then examined, and again the model deviance was used to select the best-fitting second-order polynomial. Next, the best-fitting second-degree polynomial was compared with the linear model per the difference in model deviances. If the second-degree model provided a better fit to the data than the linear one (P < 0.05), the former was then compared with the best-fitting first-order model. Otherwise, the linear model was preferred (Sauerbrei et al. 2007). The method is similar with multilevel models (Long and Ryoo 2010).
We then explored the relative contribution of the frequency and amount of sugars intake to variations in DMFT levels. First, we estimated a model without any covariates (null model) to establish the rate of change in DMFT within the observed period. Survey years (2000, 2004, and 2011) were used as the underlying time scale in all models. Next, we tested the crude effects of frequency and amount of sugars intake on DMFT in model 1 and subsequently adjusted for sociodemographic factors (sex, age, and education) in model 2 and dental behaviors (toothbrushing frequency and dental attendance pattern and use of fluoride toothpaste) in model 3. Frequency and amount of sugars intake were mutually adjusted in model 4 to evaluate their relative contribution to explaining variations in DMFT levels conditional on each other.
Finally, the moderating role of use of fluoride toothpaste on the effects of frequency and amount of sugars intake was examined by testing the significance of the statistical interaction between use of fluoride toothpaste and each indicator of sugars intake in models also adjusted for confounders (model 3). We also tested the 3-way interactions among toothbrushing frequency, use of fluoride toothpaste, and each indicator of sugars intake. We set the significance level at 0.10 to increase power when testing interactions (Aiken and West 1991; Marshall 2007).
Results
We used data from 1,702 adults, with a mean age of 47.6 y (SD, 11.4). No differences in sociodemographic characteristics and DMFT levels were found between the study sample and those excluded for missing data on covariates. The mean amount of sugars intake was 110.9 g/d (SD, 47.8; range, 13.7 to 442.3) with significant differences by sex and age. The mean frequency of sugars intake was 3.2 times/d (SD, 2.4; range, 0 to 15.6) with significant differences by sex, education, toothbrushing frequency, and use of fluoride toothpaste (Table 1). The frequency and amount of sugars intake were positively correlated (r = 0.64, R2 = 0.41, P < 0.001). The mean DMFT at baseline was 21.91 (SD, 6.4; range, 0 to 32), with only 3 participants (0.2%) having no caries experience.
Frequency and Amount of Sugars Consumed According to Baseline Characteristics (n = 1,702 Adults).
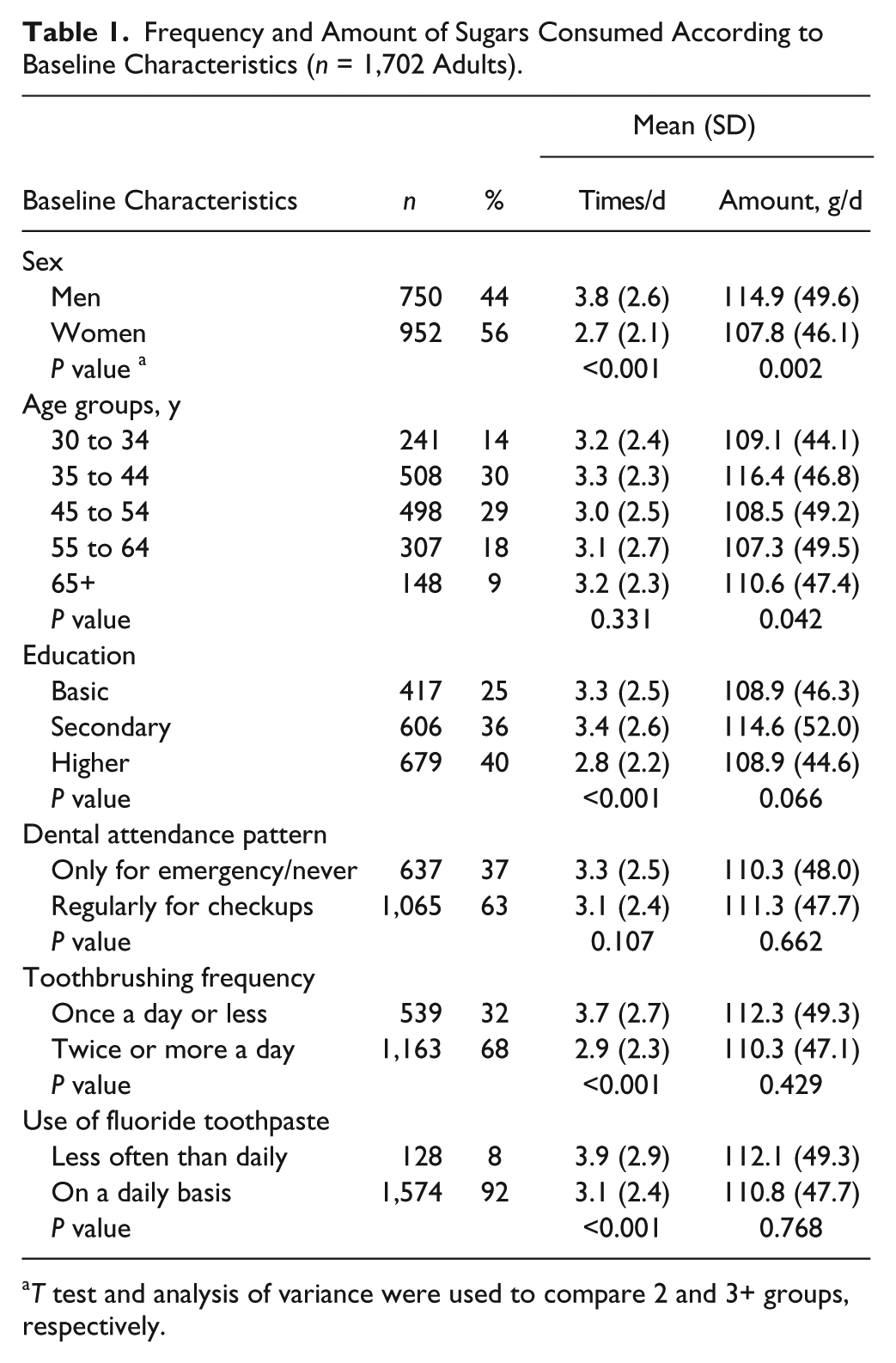
T test and analysis of variance were used to compare 2 and 3+ groups, respectively.
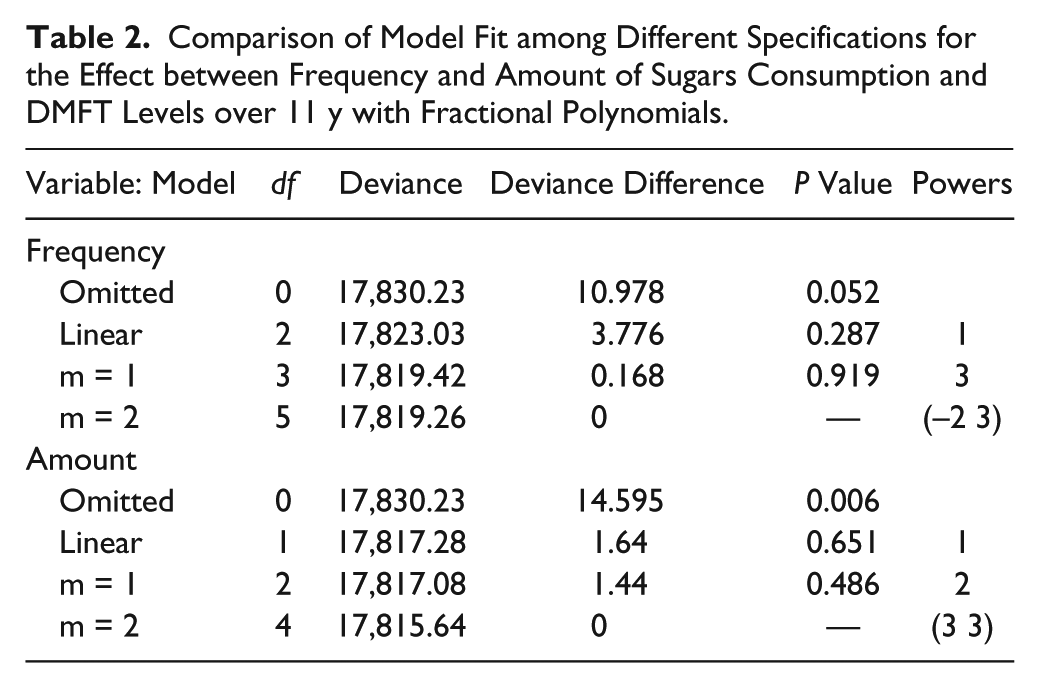
Table 2 shows the results from fitting first- and second-order polynomials to the data to test for curvilinear dose-response relationships between sugars intake and DMFT levels. The best-fitting first-order polynomial had a power 3, whereas the best-fitting second-order polynomial had powers (–2 3) in frequency of sugars intake. Neither model was significantly better in terms of model fit to data than the straight-line model. For amount of sugars intake, the best-fitting polynomials of degree 1 and 2 had powers 2 and (3 3), respectively. Again, the fit of those polynomials was not significantly better than that of the simpler linear model. Consequently, the associations of frequency and amount of sugars intake with DMFT levels were modeled as linear effects.
Comparison of Model Fit among Different Specifications for the Effect between Frequency and Amount of Sugars Consumption and DMFT Levels over 11 y with Fractional Polynomials.
The null linear mixed effects model showed that the mean DMFT increased by 0.47 units (95% confidence interval [95% CI]: 0.37 to 0.58) in 2004 and 0.74 units (95% CI: 0.64 to 0.84) in 2011. Neither the frequency nor the amount of sugars intake was significantly associated with DMFT in unadjusted models (Table 3). However, both indicators became and remained significant after adjustment for sociodemographic and behavioral factors. The DMFT throughout the follow-up period increased by 0.15 (95% CI: 0.04 to 0.25) and 0.10 units (95% CI: 0.04 to 0.15) for every additional occasion of sugars consumption and every 10 g of sugars consumed, respectively. In addition, only the amount of sugars intake remained significantly associated with DMFT levels in the mutually adjusted model (0.09 DMFT units; 95% CI: 0.02 to 0.15).
Linear Mixed Effects Models for the Associations of Frequency and Amount of Sugars Intake with DMFT Levels over 11 y (n = 1,702 Adults).
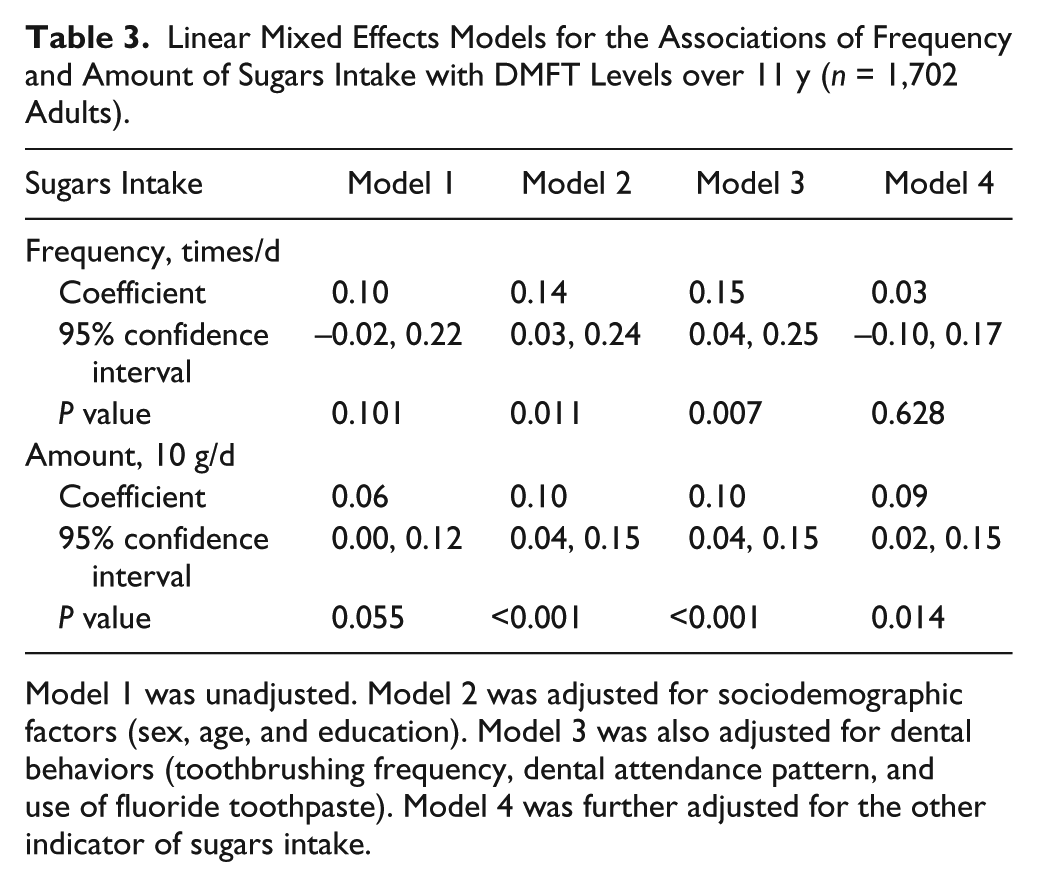
Model 1 was unadjusted. Model 2 was adjusted for sociodemographic factors (sex, age, and education). Model 3 was also adjusted for dental behaviors (toothbrushing frequency, dental attendance pattern, and use of fluoride toothpaste). Model 4 was further adjusted for the other indicator of sugars intake.
The use of fluoride toothpaste moderated the association between amount of sugars intake and DMFT levels (P = 0.064) but not that between frequency of sugars intake and DMFT levels (P = 0.129). The slope of the longitudinal association between amount of sugars intake and DMFT levels was less pronounced in adults using fluoride toothpaste on a daily basis (0.08, 95% CI: 0.03 to 0.14) than in those using it less often than daily (0.26, 95% CI: 0.07 to 0.45; Fig. 2). Although the same pattern was observed for frequency of sugars intake in adults using fluoride daily (0.12, 95% CI: 0.04 to 0.23) and less often than daily (0.43, 95% CI: 0.01 to 0.75), the 2 coefficients were not significantly different. The 3-way interactions of toothbrushing frequency and use of fluoride toothpaste with frequency and amount of sugars intake were not significant (P = 0.712 and 0.307, respectively).
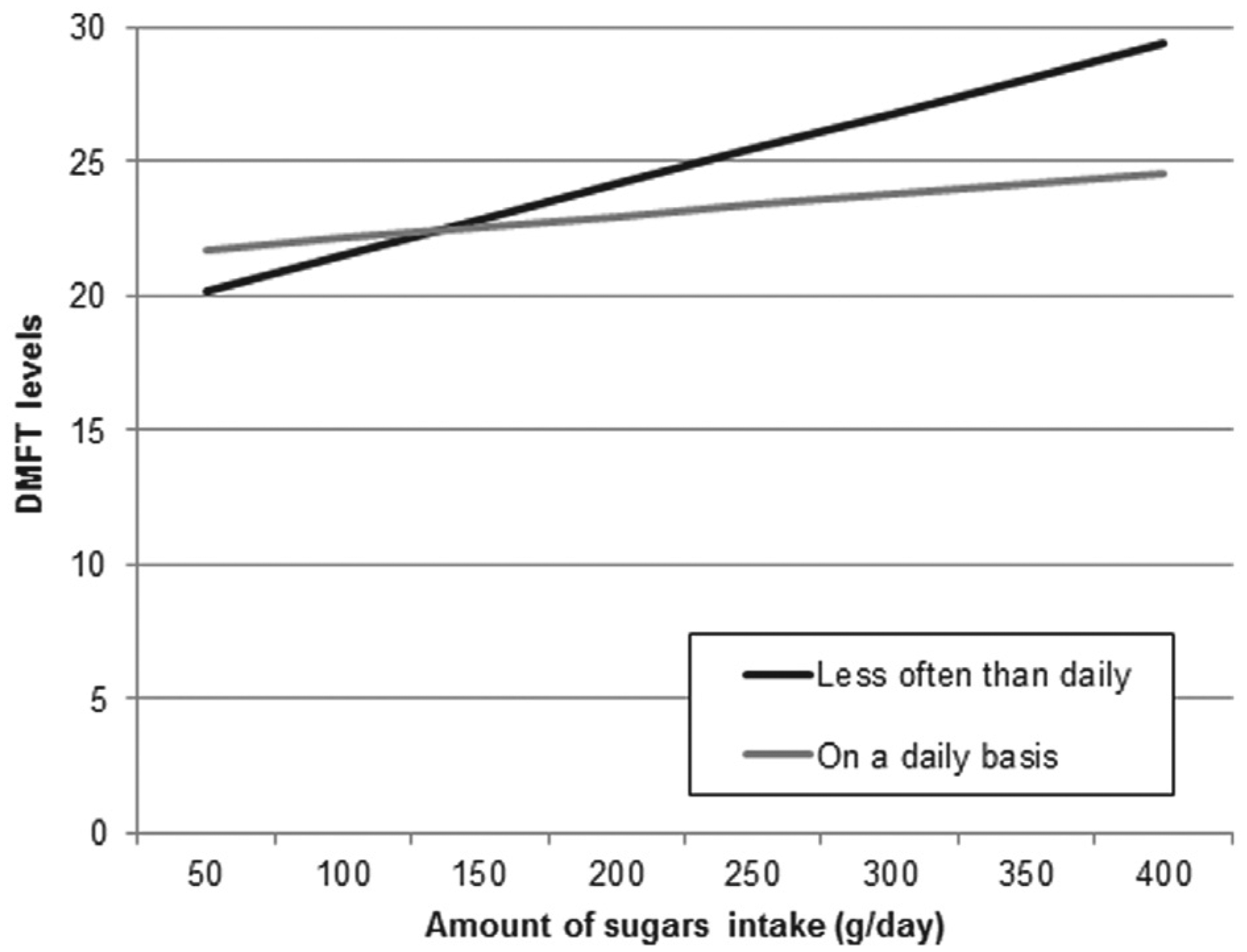
Association between the amount of sugars intake and DMFT levels over 11 y in adults with daily exposure to fluoride and those with exposure less often than daily. Estimates were derived from a linear mixed model regressing DMFT levels on sex, age, education, toothbrushing frequency, dental attendance pattern, use of fluoride toothpaste, amount of sugars intake, and the 2-way interaction between amount of sugars intake and use of fluoride toothpaste.
Discussion
This study first found that both the frequency and the amount of sugars consumption were linearly related to dental caries in adults. None of the 43 alternative curvilinear models—including the logarithmic, quadratic, and cubic transformations, among others—provided a significant improvement from the straight-line model. A linear dose-response relationship between sugars and caries implies that even the small amount of sugars will lead to caries development in adults. This finding challenges previously held assumptions on the shape of the sugars-caries relationship based on ecologic data from Japanese children. The difference between the original and reanalysis of the Japanese data is explained by the scale used to model caries incidence. While Takeuchi (1961) and Koike (1962) used the log of annual caries incidence, Sheiham and James (2014a, 2014b) used annual caries incidence. A curvilinear relationship in crude scale becomes linear when log-transformed.
Second, the amount of sugars consumed was more relevant to caries levels than the frequency of ingestion. In the mutually adjusted model, the DMFT increased by 0.09 units (95% CI: 0.02 to 0.15) for every additional 10 g of sugars consumed, while the coefficient for frequency of intake was not significant. The strongest evidence on the role of frequency of sugars intake in adults comes from the Vipeholm study (Gustafsson et al. 1954). However, our finding agrees with 2 prospective studies in children (Burt et al. 1988; Rugg-Gunn et al. 1984). Collinearity could not explain these findings, since amount of intake explained around only 40% of the variation in frequency and vice versa. This finding also implies that frequency cannot be used as a proxy for amount of sugars ingestion. Indeed, one could exceed the recommended energy intake from sugars in a single occasion. This finding supports the view that population nutrient goals should be set in terms of amount of sugars so as to monitor population’s diets and evaluate the outcomes of health promotion initiatives against clear milestones (Moynihan 2014). Focusing on amount of sugars intake will also be consistent with current guidelines to reduce the risk of other noncommunicable diseases related to excess sugars (World Health Organization 2015).
Third, the association between amount of sugars intake and dental caries varied depending on adults’ exposure to fluoride toothpaste. A weak, although significant, relationship between amount of sugars intake and dental caries persisted with regular exposure to fluoride toothpaste. Importantly, sugars were related to dental caries even in a population with slow caries progression (DMFT increment <1 tooth over 11 y), low levels of fluoride in water—in 98% of water from waterworks and 95% of single-well waters, the concentration of fluoride is <0.1 mg/L (Ahonen et al. 2008)—but high exposure to fluoride toothpaste (92% reported using fluoride toothpaste daily).
Some limitations need to be addressed. First, although the study sample was large and drawn from a national survey, those who participated in the follow-ups were younger and more educated and had more favorable dental behaviors and lower DMFT than did participants at the baseline survey. Thus, the present results reflect valid relationships between the variables of interest but are not generalizable to the entire Finnish adult population. Second, sugars consumption was collected with an FFQ with a 12-mo recall period and single average portion sizes. Thus, there can be some measurement error due to under- and overreporting (Thompson and Byers 1994; Shim et al. 2014). Furthermore, FFQs do not distinguish food items that are consumed together or on separate occasions during the day, which may overestimate the frequency of intake for some individuals. However, an advantage of FFQs is that they evaluate the usual long-term diet, which is conceptually more important in epidemiologic studies than absolute intake over a few days (as derived from food records). The FFQ used in this study was calibrated against a 16-d food record, and it was found to meet the requirements of epidemiologic studies (Paalanen et al. 2006). Third, we assessed sugars consumption at a single point in time (baseline). This is the simplest scenario in longitudinal research and unlikely to represent the complex interplay of factors influencing caries development (individuals’ diets may have changed during the follow-up period). Further studies, using alternative methods to assess sugars intake over multiple times, are therefore encouraged. Fourth, although caries was diagnosed for each tooth surface, it was recorded by tooth and reported with the DMFT, due to time constraints during comprehensive clinical examinations. The DMFT shows lower variation (and weaker associations) than the DMFS and is affected by the inclusion of teeth extracted for conditions other than caries, particularly among old groups. However, the DMFT is well established as the key measure of caries experience in dental epidemiology.
In conclusion, the association between sugars intake and dental caries in this group of Finnish adults was best described with a linear dose-response relationship. Second, the amount of sugars intake was more relevant to caries development than frequency. The effect of frequency on dental caries was fully attenuated after accounting for amount of sugars ingested. Third, sugars were related to caries in adults using and not using fluoride toothpaste daily, although the association was stronger in those using fluoride toothpaste less often than daily.
Author Contributions
E. Bernabé, contributed to conception, design, and data acquisition, drafted and critically revised the manuscript; M.M. Vehkalahti, A.L. Suominen, contributed to data acquisition and interpretation, critically revised the manuscript; A. Sheiham, contributed to data analysis and interpretation, drafted and critically revised the manuscript; A. Lundqvist, contributed to data acquisition and analysis, critically revised the manuscript. All authors gave final approval and agree to be accountable for all aspects of the work.
Footnotes
The Health 2000 (http://www.terveys2000.fi) and Health 2011 (![]() ) surveys were organized by the National Institute for Health and Welfare (THL), formerly the National Public Health Institute (KTL), of Finland and partly supported by the Finnish Dental Society Apollonia and the Finnish Dental Association. The 2004/05 Follow-up Study of Adults’ Oral Health was funded by the Social Insurance Institution of Finland (KELA) and organized by the National Institute for Health and Welfare (THL).
) surveys were organized by the National Institute for Health and Welfare (THL), formerly the National Public Health Institute (KTL), of Finland and partly supported by the Finnish Dental Society Apollonia and the Finnish Dental Association. The 2004/05 Follow-up Study of Adults’ Oral Health was funded by the Social Insurance Institution of Finland (KELA) and organized by the National Institute for Health and Welfare (THL).
The authors declare no potential conflicts of interest with respect to the authorship and/or publication of this article.