
Abstract
Arts-based creative interventions have demonstrated positive psychological effects, including creativity, self-efficacy, and social connectivity, an approach deeply rooted in a humanistic framework that emphasizes the intrinsic value of every individual and the transformative power of creative expression. This study explored the feasibility and acceptability of a web-based music composition intervention to support survivors of serious illness hospitalized during the COVID-19 pandemic. Inspired by the New York Philharmonic Very Young Composers (VYC) program, trauma-informed care-trained teaching artists guided participants through four web-based sessions to develop unique compositions, culminating in a live, online performance. Feasibility data were based on adherence to intervention components. Acceptability data on resilience-related traits were self-reported via pre–post surveys. Fourteen participants enrolled, 12 completed all intervention sessions, and 10 attended the optional final performance. Qualitative analysis revealed five themes that contributed to participants’ positive experience: (I) Novelty, (II) Skill/Perspective Gained, (III) Pleasure, (IV) Self-Efficacy, and (V) Connection to others. Results suggest that the VYC-inspired music composition intervention is a feasible and highly acceptable method for fostering resilience-associated traits in patients impacted by serious illness.
Background
The relationship between engagement in arts-based experiences and overall health and well-being has received significant attention from researchers, policymakers, practitioners, and the general public. This approach is deeply rooted in a humanistic framework that emphasizes the intrinsic value of every individual and the transformative power of creative expression. Across the continuum of health services, community arts, arts in medicine, and creative/expressive arts therapy practices all contribute to the growing evidence base of the use of arts-based experiences for health-related outcomes. This pilot study was established as a feasibility and acceptability study, exploring the ways in which a music composition program developed for those without musical training can provide an outlet for creativity to support resilience in those who required hospitalization during the COVID pandemic.
Trauma-informed care (TIC) is a resilience-supporting framework that recognizes the prevalence of trauma and adversity, the various ways it manifests in patients, and its effects on healthcare staff (SAMHSA, 2014). A trauma-informed approach integrates knowledge about trauma into policies, procedures, and practices to optimize engagement and resist re-traumatization (SAMHSA, 2014). The intention is not to provide trauma-focused treatment, but rather to encourage “universal trauma precautions,” assuming that most individuals have experienced trauma or adversity in their lifetime that impacts their experiences and relationships throughout their lives. This provides a crucial framework to address actual and potential impacts of trauma with resilience-building strategies and interventions devised and delivered beyond healthcare settings.
Resilience has been characterized as “the process of, capacity for, or outcome of successful adaptation despite challenging and threatening circumstances” (Masten et al., 1990). Resilience also serves as an umbrella term, capturing a range of resilience-associated traits that contribute to one’s capacity to maintain or regain a sense of self-efficacy and meaning amidst adversity. The six guiding principles of TIC align with this perspective: psychological and physical safety; transparency and trustworthiness; collaboration; empowerment; attention to culture, race and gender; and appreciation of the unique value of peer support (Centers for Disease Control and Prevention, 2022). Resilience can be cultivated in many ways, including through engagement with the arts.
A musical composition is a complete work for any number of instruments or vocalists in any genre or musical style, of any duration and scope. It can be notated, learned aurally (not written down), or improvised. There is limited research investigating the potential therapeutic benefits of musical composition. Published case examples include the use of musical composition as a means for communication, self-expression, agency, and creativity among hospitalized children, in pediatric rehabilitation, among abused children, among caregivers, and in addiction recovery (Bradt, 2013; Davidson & Almeida, 2014; Gleeson & Tomlinson, 2019; Gottesman, 2016; LaVerdiere, 2007; O’Callaghan et al., 2007; Viega, 2015). Finally, through arts-based research methods, Habron explored the benefits of a community music collaboration between a chamber orchestra and a small group of older adults (Habron, 2013). The findings demonstrated that individual and group music composition contributed to a sense of well-being through control over musical materials, opportunities for creativity and identity making, validation of life experience, and social engagement.
Literature Review
Arts-based approaches to healing have gained increasing recognition over the past decade. As medical treatments advance, many healthcare systems are developing arts-based outreach programs to enhance well-being and provide support for individuals adapting to changes and survivorship (Lambert et al., 2017). These arts in public health programs are community-based and designed to promote well-being, strengthen social connections, facilitate arts-based message and communication, and enhance resilience (Albright & Carytsas, 2021). Resilience is a core theoretical construct underlying trauma-informed approaches and is indirectly targeted by our intervention through fostering resilience-related traits such as self-efficacy, creativity, social connection, and agency. Although resilience itself is not directly measured as a singular construct in this pilot study, understanding resilience is essential to interpreting our intervention’s intended impacts and contextualizing our approach within existing resilience-promoting frameworks.
The Substance Abuse and Mental Health Services Administration (SAMHSA) has defined trauma as an event or series of events that an individual experiences as physically or emotionally harmful or life threatening, and that has lasting adverse effects on functioning and well-being (SAMHSA, 2014). The COVID-19 pandemic amplified awareness of the ubiquity of trauma and adversity across the general population, particularly in healthcare. The negative and lasting psychological impact of illnesses requiring hospitalization were well recognized prior to the COVID pandemic (Alzahrani, 2021; Davydow et al., 2008; Righy et al., 2019). Unprecedented COVID-19-related restrictions, uncertainties, and isolation disrupted crucial sources of support and resilience during periods of hospitalization and afterward, compounding the negative psychological impacts of admission (Ju et al., 2021; Tarsitani et al., 2021; Vlake et al., 2021).
There is growing research evidence on the possible benefits of arts in public health programs to foster resilience while facing multiple challenges, including recovery from illness. For example, Fancourt and colleagues demonstrated that a 10-week group drumming program could increase social resilience and decrease depression. Gallagher et al. (2024) conducted a randomized controlled trial demonstrating that an 8-week arts-based program enhanced mood, resilience, and well-being of individuals with chronic health conditions. And a 2020 systematic review identified impact of participatory music engagement on well-being identified managing and expressing emotions, facilitating self-development, providing respite, and facilitating connections (Perkins et al., 2020).
Within trauma-informed practices, music experiences can create opportunities to exercise choice, remain curious, have agency; increase self-efficacy; and safely explore, experience, and connect with self and others through music while providing a sense of control (Sokira et al., 2023). Participation in therapeutic music and music therapy programs have been cited in the literature as providing an opportunity not only to foster individual-level resilience but also to provide a safe and enjoyable outlet to counter the negative feelings associated with traumatic life events (Landis-Shack et al., 2017). This includes key factors associated with resilience such as self-efficacy, social support, optimism, emotional regulation, and meaning making (Haase et al., 2020; Myers-Coffman et al., 2020; Ribeiro et al., 2021; Saarikallio et al., 2019; Southcott & Nethsinghe, 2019). Therapeutic music experiences may involve creating, improvising, listening to music, and/or performing music. Creating music, whether through songs or musical composition, often serves as a symbolic representation of an experience. Therapeutically, creative music experiences can provide opportunities for the following: self-expression without the need to elaborate through words; strengthening of communication of emotions; providing opportunities for creative problem-solving; allowing choice and decision-making; and highlighting patterns that play a significant role in an individual’s daily life (Moore & Elliott, 2018). Certain models of resilience even include creativity as an inherent component (Metzl & Morrell, 2008), and there is growing evidence of the connection between arts participation (including music and creative expression) and psychological resilience and neurological health (Fancourt et al., 2019) .
Through adaptive programs, it is possible for individuals without a musical background to actively participate in the compositional process. The New York Philharmonic Very Young Composers (VYC) program offers a unique opportunity to utilize the role of creativity to build resilience in individuals without previous music training (Menard, 2013). Created by Jon Deak, with the mission to empower participants and celebrate their creative potential, VYC provides individuals with the opportunity to transform their musical ideas into finished compositions. The VYC model utilizes Teaching Artists, professional composers who serve as mentors to program participants. These participants attend a series of in-person sessions in which they engage in musical activities fostering the development of a participant’s unique musical composition. The program has been expanded to a range of ages, countries, and cultures since its launch in 1997, aligned with the manner in which a trauma-informed framework honors the diversity, equity, inclusion, and belonging dimensions of healing and well-being programs (Very Young Composers, 2024).
Research Questions
This pilot study aimed to develop and evaluate the feasibility and acceptability of an online music composition program, characterizing the impact on self-efficacy and resilience of individuals who were hospitalized during the COVID pandemic. More specifically:
Is it feasible to adapt a Teaching Artist-facilitated music composition program to an online four-session program for patients who had been hospitalized during the COVID pandemic?
How do post-hospitalized patients respond to an online music composition program designed for individuals with little or no musical training, including on self-reported levels of resilience-associated traits?
Ethical Approval and Informed Consent Statements
This study was registered with ClinicalTrials.gov (NCT05727514). Ethics approval was obtained from the Brigham and Women’s Hospital institutional review board (IRB; 2021P000904) and the Berklee College of Music IRB (04222021-F-E-S1) (ClinicalTrials.gov NCT05727514).
This study made use of implied consent. In accordance with the Partner’s Human Research Committee policy, a participant is considered enrolled when providing implied consent by completing a questionnaire. Prior to enrollment, all potential participants were given a study information sheet which detailed the study procedures and any risks involved in this study. Participants were informed that by clicking into Zoom links for sessions and links for questionnaires, they were giving their implied consent to participate, informed that they could withdraw from the study at any time, and given the option “choose not to answer” on each questionnaire.
Design and Methods
A mixed-methods design was used to elicit a fuller understanding of participant experience, both with validated measures and direct feedback. Validated instruments were used to measure resilience and self-efficacy. A qualitative questionnaire was included, given the lack of specificity of the instruments to the nature of this music composition-based intervention, in order to develop a specific understanding of the subjects’ experience of the program, including whether and how it was impactful. Feasibility outcome measures included recruitment and retention, including questionnaire and program completion (Low et al., 2020). Acceptability data on resilience-related traits were assessed through two methods: (1) quantitative analysis of self-report responses to the Brief Resilience Scale (BRS) and New General Self-Efficacy (NGSE) Scale pre- and post-intervention and post-performance and (2) thematic analysis of participant feedback post-intervention and post-performance. Qualitative data were included to capture participants’ nuanced experiences of creativity, emotional resonance, sense of agency, and the processes underlying the development of resilience-related traits—insights that quantitative measures alone could not fully convey.
Participants
Participants were recruited from an urban city hospital using a centralized clinical data registry (Research Patient Data Registry [RPDR]) consisting of records of patients across hospitals. Identified patients were sent research invitations via an encrypted patient portal for secure communication between healthcare professionals and patients. This study also utilized physician key informants to recruit potential study participants. Participants were eligible if they: (1) were between the ages of 18 and 60 years, (2) were in-state residents, (3) exhibited English fluency, (4) were in care with an in-network provider, (5) were an inpatient for at least 3 days to an in-network hospital for any serious illness warranting admission between March 15, 2020 and July 21, 2022, (6) were not hospitalized within the month before starting the study, (7) had access to adequate video-based technology such as a computer, laptop, smartphone, or iPad with a webcam, and an email address, and (8) did not have any acute neuropsychiatric illness (including suicidality, psychosis, active substance abuse, or dementia) that may impede ability to participate in this 4-week program. They did not require any prior musical training.
This study made use of implied consent. Eligible participants underwent a two-part screening process: first, asked questions via phone call; second, asked to consent to a chart review, in which the study Principal Investigator assessed the participant’s clinical eligibility based on study inclusion criteria. Prior to enrollment, all potential participants were given a study information sheet which detailed the study procedures and any risks involved in this study. Participants were informed that by clicking into Zoom links for sessions and links for questionnaires, they were giving their implied consent to participate; informed that they could withdraw from the study at any time; and given the option “choose not to answer” on each questionnaire.
The RPDR identified 1,040 individuals matching study criteria; this cohort was sent research invitations through Patient Gateway. Of those, 62 completed the REDCap screening form. Key informants referred 6 patients who filled out the online form, for a total 68 completed online screenings. A total of 14 individuals who had at least one 3-day inpatient hospital stay (3/15/2020-7/22/2022) and meeting inclusion criteria detailed above participated in this study.
Measures
Data for this study were collected using: (1) researcher-developed intake forms to record demographic and background information on each participant; (2) the BRS; (3) the NGSE Scale; (4) researcher-developed post-intervention survey; and (5) researcher-developed post-performance survey. Resilience associated factors were assessed through online questionnaires via REDCap at three time points in the study: pre-intervention (before session 1), post-intervention (after session 4), and post-performance (after the post-intervention final performance).
The BRS is used to assess ability to recover after stress (Smith et al., 2008). It includes six items to which participants rate the extent to which they agree (from 1 = “Strongly Disagree” to 5 = “Strongly Agree”). Responses were scored by averaging the ratings across statements.
The NGSE scale evaluates one’s perception of their overall ability to perform successfully in a variety of common scenarios by rating each item from 1 = “Strongly Disagree” to 5 = “Strongly Agree” (Chen et al., 2001).
Post-intervention survey consisted of three open-ended questions: (1) What did you enjoy about this program? (2) What did you find challenging about this program? (3) What did you learn about yourself through this program? and a fourth regarding acceptability: (4) Would you recommend this program to other survivors of serious illness?
Post-performance survey consisted of three open-ended questions: (1) What was it like to hear your composition performed by professional musicians? (2) How did participating in this performance increase the impact of this program overall? (3) Does this program make you feel more confident about being able to be creative in the future? and a fourth regarding acceptability: (4) Would you recommend attending the performance as part of this program to other survivors of serious illness?
Procedures
Five composers on faculty at a local performing arts college in the northeast were recruited to serve as Teaching Artists. Prior to working with study participants, Teaching Artists were provided three training videos: introduction to TIC developed by a physician (NCLC) with expertise in trauma-informed perspectives across care domains; an introduction to the music composition program developed for individuals with no prior musical training; and tips to inspire music creation developed by a composer (RDC) with a decade of international experience training Teaching Artists in the VYC protocol. Opportunities for follow-up discussion and support throughout the study period were offered. Additionally, Teaching Artists were informed of all study protocols, including safety and confidentiality practices.
All intervention sessions were facilitated online, via zoom. Participants were paired with a Teaching Artist who was responsible for implementing the study protocol. Each of the four intervention sessions lasted for 1 hr and included one Teaching Artist and one participant. The same Teaching Artist/participant dyads remained over the course of the four-session protocol. Prior to the first session, and after the last session, participants were directed to complete the BRS and the NGSE scale.
Intervention Sessions
The VYC-inspired music composition intervention consisted of four 1-hr sessions over four consecutive weeks. These occurred over Zoom. Each Teaching Artist was equipped with several warmup exercises designed to foster musical expression. The Teaching Artists were encouraged to tailor lesson plans to each participant based on which approaches seemed most engaging. The Teaching Artist played the participant ideas on their own instrument and took notes during the intervention session to prepare a final score of each participant’s musical composition. The general session structures were as follows:
Session 1: Introduction and listening, vocal, and drawing-based warmup exercises (15 min); introduction to string instruments (10 min); writing first melody (15 min); brainstorming titles (10 min); writing a 1-min piece (10 min).
Session 2: Listening and visualization-based warmup exercise (10 min); writing musical melodies (15 min); conduct and vocalize the music (10 min); composing the middle of a piece (15 min).
Session 3: Choice of warmup exercises (5 min); extending the music (10 min); developing the title (15 min); reviewing the musical form (15 min); writing additional lines (15 min).
Session 4: Choice of warmup exercises (5 min); adding harmonies (15 min); finalize orchestration (30 min); review complete piece (15 min).
Following the participants’ fourth and final intervention session, participants were sent an email with a request to complete the post-intervention questionnaires (BRS, NGSE, and the post-intervention survey). Finally, each participant was provided with a copy of their final score in a PDF format along with an audio recording of their composition.
Final Performance
Once all participant sessions were completed, a collective final online performance of all participant compositions was scheduled. The music compositions were performed by a music college-affiliated string quartet. The performance was live-streamed, and a recording was made available to those who could not attend. Participants who viewed the performance were invited to complete the post-performance survey. A total of 12 compositions were performed during the final performance.
Participants were compensated at multiple points throughout the study. Participants received a $25 online gift card for completing online surveys (for a total up to $75) and received a $25 online gift card for each intervention session they attended (up to $100 total).
Data Analysis
To assess changes in self-efficacy and resilience, aggregate scores of the NGSE and BRS were computed at three intervals: pre-intervention, post-intervention, and post-performance. Data were analyzed in IBM SPSS (version 28).
Qualitative thematic analysis was carried out on the open-ended questions at the post-intervention and post-performance surveys. Four researchers independently completed inductive thematic analysis of the qualitative open responses (Brown et al., 2022). First, researchers familiarized themselves with the data by discussing the questions and the participants’ responses. Next, researchers independently went through each response and generated words or phrases that captured the key point(s) of each statement. These words and phrases were then compiled to assess consistency amongst researchers. Once it was clear that certain themes were emerging, researchers went back and reclassified the responses into new codes. These new codes were discussed, and differences were reconciled by discussion among members of the research team. Once no repetitive data emerged, the themes were finalized.
Results
Feasibility
Fourteen participants enrolled in this study by completing the pre-intervention measures, of whom 12 completed the post-intervention measures, and 10 completed the post-performance measures. This represents a retention rate of 85.7% (n = 12) and 71.4% (n = 10) for the optional final performance. Participants were predominantly female (n = 8; 57%), white (n = 9; 64.3%), and non-Hispanic (n = 10; 71.4%), with a mean age of 44 ± 12 years (range: 21–59 years; Table 1).
Demographic Characteristics of Enrolled Study Participants.
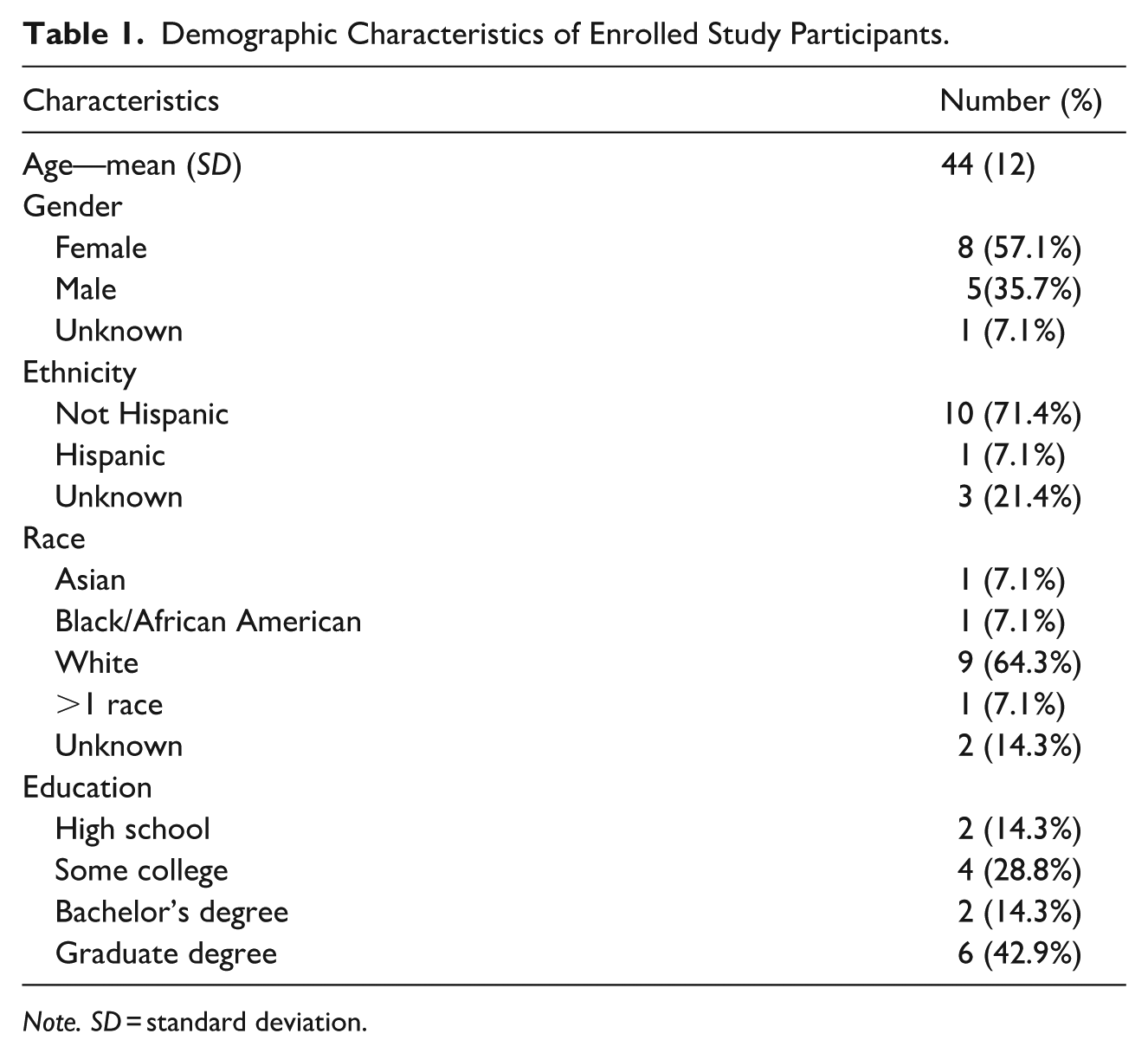
Note. SD = standard deviation.
Resilience-Related Measures
Outcome measures were assessed using paired t-tests between each time point: pre-intervention, post-intervention, and post-performance. All measures were normally distributed. Resilience-related measures displayed a modest increase after intervention but not following the performance (Table 2). The data lacked power to explore other differences due to sample size.
Resilience-Related Scores Based on the BRS and NGSE.
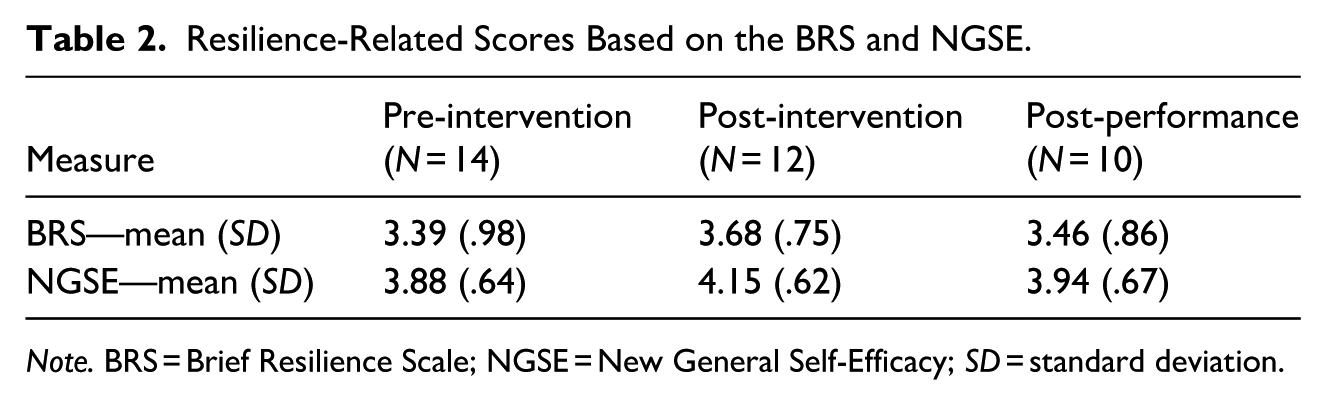
Note. BRS = Brief Resilience Scale; NGSE = New General Self-Efficacy; SD = standard deviation.
Qualitative Results
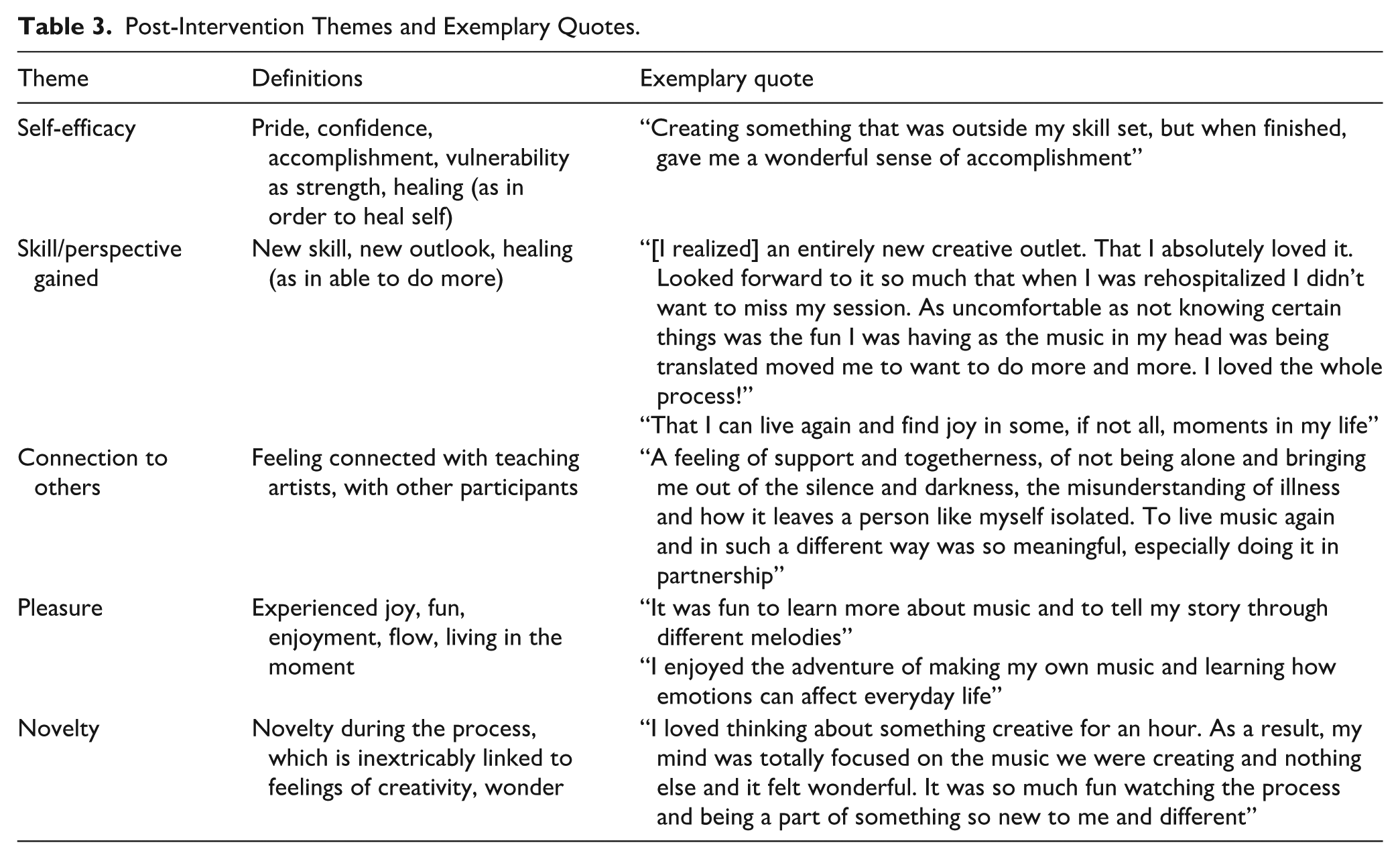
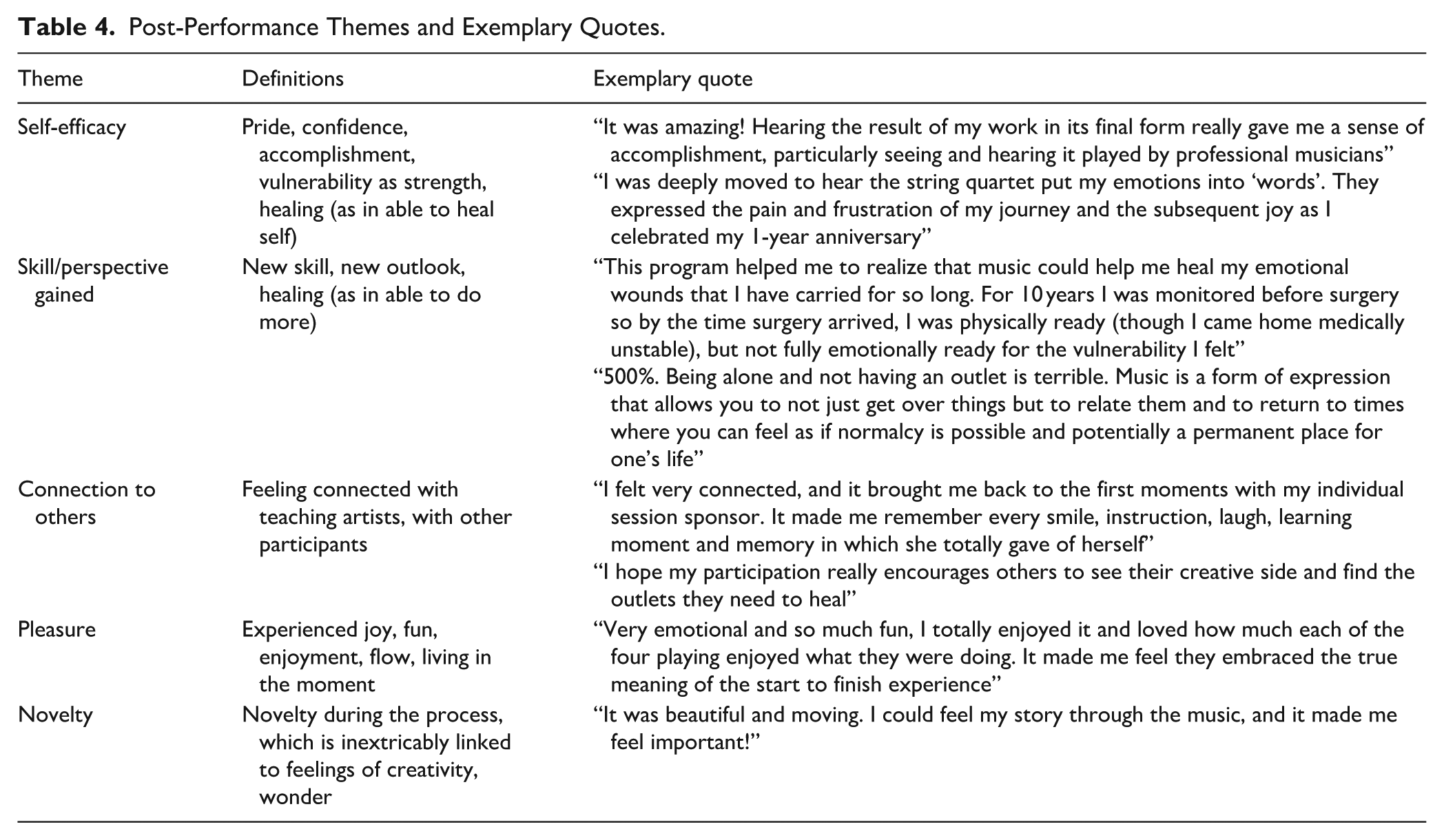
Participants responded to qualitative questionnaires at the conclusion of the intervention (N = 12; Table 3) and performance (N = 10; Table 4). Researchers identified five overarching themes from the participants’ open-ended responses to the post-intervention and post-performance questions: (1) Self-Efficacy, (2) New Skill or Perspective Gained, (3) Connection, (4) Pleasure, and (5) Novelty.
Post-Intervention Themes and Exemplary Quotes.
Post-Performance Themes and Exemplary Quotes.
Both series of questions asked if participants would recommend the intervention and performance, respectively, to other people who experienced a serious illness. Eleven of the 12 participants reported that they would recommend this program to others. One participant remarked: “Yes, I definitely would [recommend]. I think it provides a welcome distraction and produces a confidence-boosting result.” Of note, the one participant who indicated reservations about recommending this program was the only one who had worked as a professional musician, reporting, “I wouldn’t unless they already have a history in music or are interested in composing music.” (See Table 3 for post-intervention themes and exemplary quotes.)
Participants were asked what they found challenging about this program. Common responses included being creative and developing confidence using an unfamiliar medium (music) and vulnerability tied to being creative in an unfamiliar modality. It is notable that despite these challenges, the overwhelming majority of participants enjoyed the experience and would recommend it to others.
When asked if they would recommend attending the final performance as a part of this program all 10 of the responders said they would. One example: “Absolutely! Think it was an integral part of the experience as it made me even prouder of what I had accomplished. It also gave me a feeling that it was a shared experience with the others in the study, both in our original traumas and musical compositions.” (See Table 4 for post-performance themes and exemplary quotes.)
Discussion
The role of therapeutic arts and arts in health programs for fostering resilience is widely recognized. The COVID pandemic had a significant impact on care delivery, including greater isolation during hospitalization, and expanded access to web-based therapies and activities in other settings. It also highlighted the importance of identifying impactful approaches to respond to community-wide traumatic events with healing-focused interventions that cultivate creativity to support resilience.
This study assessed the feasibility and acceptability of a VYC-inspired music composition program as a trauma-informed means of fostering resilience in individuals who experienced hospitalization in the COVID-19 era. This innovative program was (1) developed as an entirely virtual intervention and included teacher-training on the principles of TIC, and (2) utilized in individuals identified by their medical experience. Study results demonstrated that the implementation of this online music composition program was feasible, as 86% of enrolled participants completed the core program. Additionally, Teaching Artists trained in trauma-informed practices and core principles of teaching composition to non-professional musicians successfully facilitated sessions that resulted in fully composed instrumental works. Scheduling flexibility due to remote sessions may have contributed to the high retention rate of intervention. The goal was to have one session per week for four consecutive weeks. Due to participant scheduling conflicts, 5 out of the 12 who completed the intervention did not follow this timeline exactly.
By recognizing the synergies of this Teaching Artist-supported composition process with the principles of TIC, the study extends the application of a creative musical program for arts in health programming to intentionally support self-efficacy and resilience in post-hospitalized participants. When asked what was most challenging about this program, participants of all education categories reported a lack of musical ability and difficulty navigating a new modality in the process of creativity. Overcoming these challenges was cited by most participants as contributing to feelings of accomplishment at the final product. Quantitative analysis revealed a trend toward increased resilience-related traits and self-efficacy after the intervention. Future studies with larger samples are required to effectively power an analysis to identify whether there is a causal relationship between increases in self-efficacy and resilience and the musical intervention itself. Thematic analysis evidenced a robust positive impact of the intervention and performance. Specifically, participants reported that this program strengthened their feelings of self-efficacy, equipped them with new skills and/or perspective, and provided a sense of connection, all key criteria for building resilience.
The neurobiological underpinnings of this impact have been well described. Music activates several areas of the brain, often simultaneously. These include modulation of stress reactivity pathways; the somatosensory cortices (auditory, visual, motor); the cerebellum (rhythm, timing, and fine-tuning movement); as well as the deeper limbic structures that regulate our emotions (amygdala, orbitofrontal, anterior cingulate cortex), memory (hippocampus), and desires (nucleus accumbens and mesolimbic rewards pathways; Raglio et al., 2016; Salimpoor et al., 2013; Trost et al., 2014).
Patterns of activation across these areas change in response to the type of music or by the emotional response or memory invoked by a particular piece of music (Koelsch et al., 2005). Patterns of brain activation also change depending on whether we are listening to music or playing or improvising new music, both independently as well as in dyads (Beaty, 2015). These interbrain networks contain the mirror neuron system and are also associated with various aspects of social cognition, including empathy and trust (Sänger et al., 2012). As empathy and trust are cornerstones for social cooperation, music may provide a tool for building greater collaboration, engendering greater cross-cultural understanding through shared empathy, and engaging in more meaningful peer to peer collaboration and support.
Music not only exerts an effect on our brain and bodies during the time in which it is heard or played but may also provide more lasting and far-reaching changes in brain structure and function. Music can activate, or modulate, the signaling in several areas of the brain involved in emotional processing, cognitive flexibility (or abstract thinking), attention, reward, and motivation. Over time, it may also create lasting structural changes within these same key areas, addressing the potential of both functional and structural changes that result from trauma exposure. More research into the specific ways in which non-lyrical music composition impacts this neurocircuitry is warranted.
Limitations
This pilot study is limited by participant size, the absence of a control group, and no analysis of varying levels of education or music training by participants on outcomes. Recruitment was primarily through a passive patient-portal approach, and the participants thus self-selected if motivated to participate. To minimize the burden of questionnaires on participants for this pilot study, we did not request information on sexual orientation, disability status, socio-economic status, or mental health service use. While the current pilot study did not specifically quantify resilience as a standalone variable, resilience-related traits (e.g., self-efficacy, social connectedness, and perceived creativity) were directly assessed. In addition, as hospitalization during the COVID pandemic was considered the sentinel “exposure,” indicating a serious degree of illness amplified by isolation from visitors, we did not collect information about the type of hospitalization.
Conclusion
This pilot demonstrated the feasibility and acceptability of a trauma-informed music composition program in participants who were hospitalized with serious medical illness, utilizing both active (composing) and passive (attending composition concert) musicality. The findings demonstrate that this is a feasible and effective framework to use for future research deeply rooted in a humanistic framework that emphasizes the intrinsic value of every individual and the transformative power of creative expression in supporting resilience-related traits. Opportunities to expand on the findings of this study include consideration of different patient populations and representation of different cultural contexts and instruments used in composition, with more detailed characterization of the participant population to understand how factors such as level of musical education are related to impact and experience. In addition, there are opportunities to incorporate biometrics and neuroimaging that explore and explain the ways in which creativity, nurtured through an active music composition intervention, supports resilience-associated traits.
Footnotes
Acknowledgements
The authors thank the Berklee College of Music Teaching Artist team of Brian Sears, Anne Goldberg-Baldwin, Brian Buch, Joo Park, Ryan Suleiman, Victoria Cheah, as well as the New Composer String Quartet: Gabriela Díaz, Lilit Hartunian, Sam Kelder, and Rafael Popper-Keizer, for their partnership. For assistance in project development, the authors thank Derek Nelson and in article preparation, Maranatha Hampson and Grace Guo.
Ethical Considerations
This study was registered with ClinicalTrials.gov (NCT05727514). Ethics approval was obtained from the Brigham and Women’s Hospital institutional review board (IRB; 2021P000904) and the Berklee College of Music IRB (04222021-F-E-S1).
Consent to Participate
This study made use of implied consent. In accordance with the Partner’s Human Research Committee policy (“Informed Consent of Research Subjects,” 2020), a participant is considered enrolled when providing implied consent by completing a questionnaire. Prior to enrollment, all potential participants were given a study information sheet which detailed the study procedures and any risks involved in this study. Participants were informed that by clicking into Zoom links for sessions and links for questionnaires, they were giving their implied consent to participate, informed they could withdraw from the study at any time, and given the option “choose not to answer” on each questionnaire.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by internal funds from the Brigham and Women’s Hospital Department of Psychiatry.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
IRB approval did not include data sharing for this study.