
Abstract
The sixth edition of the United States Conference of Catholic Bishops’ (USCCB) Ethical and Religious Directives for Catholic Health Care Services (ERDs) provides ethical guidance for Catholic healthcare professionals and institutions for many moral issues. Presented here is a brief discussion of the main points contained in Part Five, which covers issues in care for the seriously ill and dying patient, and includes a focus on the challenges of promoting the essence of these Directives—without using religious arguments—to a secularized culture clamoring for physician-assisted suicide (PAS).
Keywords
Main Document
Death is an inevitable part of life, and it will come for us all. Of course, as that time does approach, decisions must be made about situations that may not have been discussed previously with family members. Advance directives may not be available or even exist—only about one-third of adults in the United States have any sort of advance directive (Yadav et al. 2017). Additionally, as physicians and healthcare professionals caring for patients at the end of their lives, conversations will likely include topics that tread into potential ethical dilemmas for Catholics: hemodialysis, intubation, medically assisted nutrition, hydration, and possibly even requests for assisted suicide as it becomes more heavily promoted as an acceptable medical “treatment.” The sixth edition of the United States Conference of Catholic Bishops’ (USCCB) Ethical and Religious Directives for Catholic Health Care Services (ERDs) provides ethical guidance for Catholic healthcare professionals and institutions for many moral issues (USCCB 2018). There are six parts contained within this document. Part Five—Issues in Care for the Seriously Ill and Dying—addresses these end-of-life challenges. Being able to properly defend human dignity when patients are at a vulnerable time, using the guidance and wisdom contained within Part Five of the ERDs, is essential. Yet, it must often now be done in a way to reach those who have no interest or respect for a faith-based perspective. Presented here is a brief discussion of the main points contained in Part Five, including a focus on the challenges of promoting the essence of these Directives—without using religious arguments—to a secularized culture clamoring for physician-assisted suicide (PAS).
Overview of Part Five of the ERDs
The fifth section of the ERDs begins with an introduction expounding on a Catholic institution’s need to provide a community of respect, love, and support as patients and families face the reality of death. Following that are twelve directives pertaining to situations patients face at the end of their life and what happens to them after death.
The first seven directives in Part Five address issues while the patient is still living, with the primary one being that Catholic institutions must offer adequate opportunities for those in danger of death to prepare for it by providing appropriate medical information to them and their families about their condition, the options available to them, spiritual support, and access to the sacraments. After that, the directives cover several important items. Mention is made of the obligation for a person to use ordinary or proportionate means to preserve his or her life, as well as the option to forego extraordinary or disproportionate means. Nutrition and hydration must be provided except when excessively burdensome, noting that those in a persistent vegetative state should not be excluded from receiving food and water even if assistance to receive it is needed. Free and informed judgment from competent adults about withdrawal of life-sustaining treatments should be respected unless their decision is contrary to Catholic teaching. Assisted suicide and euthanasia are not permitted; patients who request it should be offered compassionate care, spiritual and psychological support, and appropriate pain treatment. Patients should be made as comfortable as possible, and if they have suffering that cannot be alleviated, they should be guided towards an understanding of the Christian concept of redemptive suffering.
The final five directives pertain to situations after death has occurred. Stipulations as to whom should make the determination of death are covered. The desire of a person to donate organs or bodily tissue (or parents wishing to donate from their infant) should be respected if going towards ethically acceptable purposes and those organs or tissues are not removed until death has been determined. Tissue obtained by direct abortions should never be utilized, even for research or therapeutic applications.
Battling the Culture of Death
While the guidance offered by the ERDs is helpful for those patients and healthcare professionals who are practicing Catholics or at Catholic institutions, 1 much of the secular culture disagrees, or believes that they disagree, with Catholic teaching and rejects any arguments that are from a religious or faith-based perspective. This becomes especially pertinent when PAS is the topic at hand. How can the beliefs about the inherent dignity of each human life, and therefore that it is not morally acceptable to legalize suicide in any form, be adequately expressed when God is not permitted in the discussion?
An excellent article previously published in The Linacre Quarterly addressed the four most often cited arguments in favor of PAS and provided logical and reasonable rebuttals from a non–faith-based perspective (Sulmasy et al. 2016). The main arguments proponents of PAS offer are: (1) patient autonomy should not be thwarted, (2) there will be no slippery slope to broaden access to PAS, (3) some patients have unalleviated pain, and (4) it is a physician’s duty to provide the patient what they want. In answer to the patient autonomy argument, the authors state a response of “it [PAS] offends me” with four premises: life has infinite value, PAS devalues life, this devaluation of life is offensive, and human beings are relational and share in the value of life. Therefore, PAS is an offense to all human beings and that supersedes an individual’s autonomy. As to there not being a slippery slope, Sulmasy et al. argue that there are multiple cases where PAS in limited circumstances has led to PAS with markedly reduced restrictions (e.g. children, disabled people). In the United States, five of the eleven jurisdictions where PAS is currently authorized have proposed legislation to broaden access to it (Figure 1; Compassion & Choices 2021). Unalleviated pain is often cited by proponents as a reason PAS is needed, but pain can be treated; embracing excellent palliative care is the proper path to follow. Of note, pain is not even one of the top five reasons patients in Oregon list when using PAS to end their lives (Public Health Division 2020). Finally, regarding a physician’s duty, the authors state that PAS undermines the integrity of both physician and patient as it is a contradiction to the patient’s seeking to be well and a violation of the principled duty of the physician to help the patient become well. Undermined physician integrity leads to a loss of patient trust in physicians. Status of physician-assisted suicide (PAS) in the United States, 2021 (created with mapchart.net).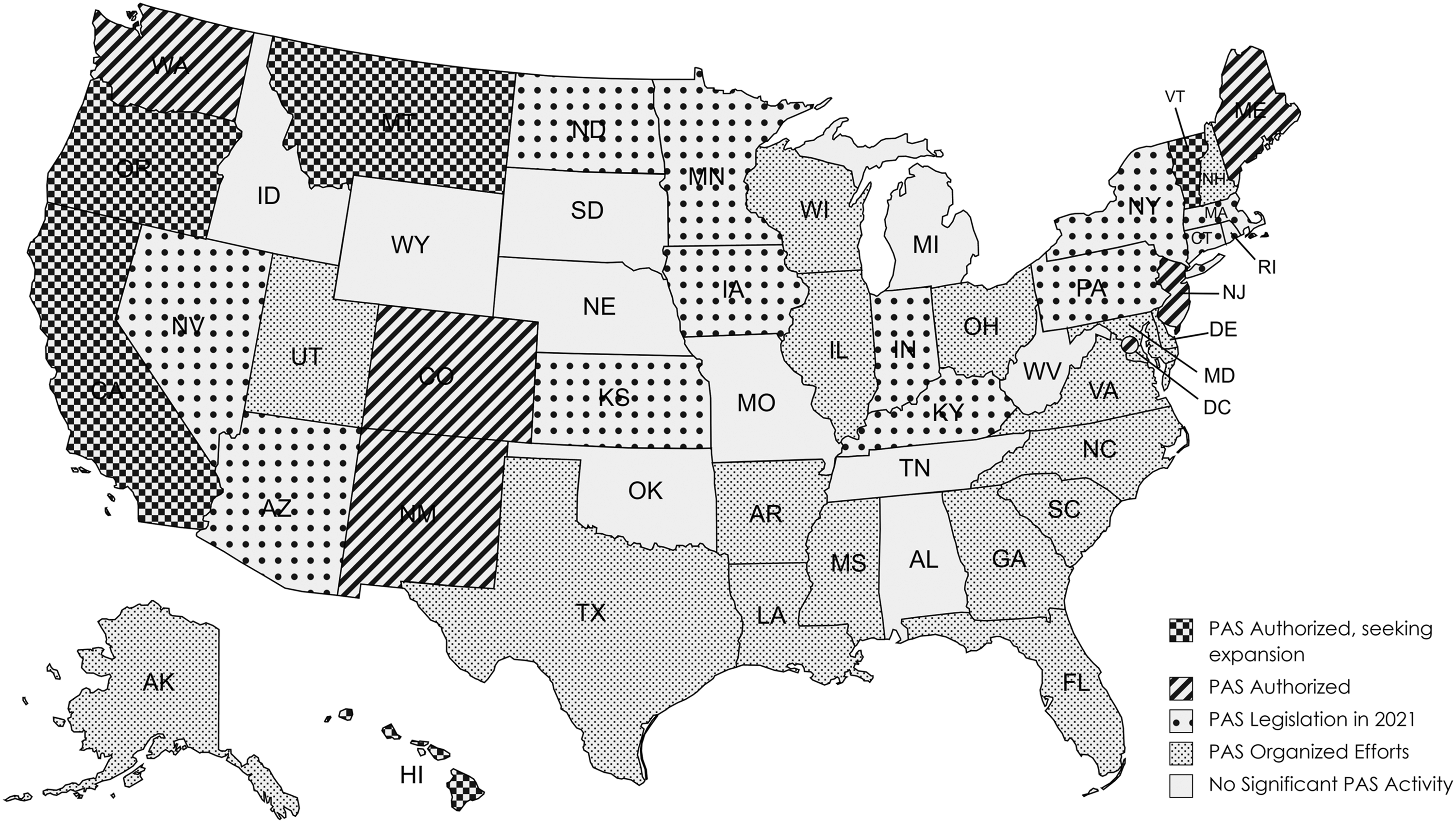
Other logical arguments against assisted suicide appeal to natural law. Since natural law is based in reason, not theism, it can be a route to argue against PAS. The American ideals of freedom were based on natural law, but freedom does not mean license; freedom comes with a responsibility to the common good and to society. “Similarly to how the three branches of the American government were created, three principles of medical ethics—autonomy, beneficence, and justice—were identified to keep one another in check. An executive branch ruling in isolation is recognized as tyranny. A scientist who clings to the virtue of truth but neglects love and mercy is heartless. The practice of autonomy in isolation reflects a society which has yielded to the reign of indifferent cruelty; indeed, to neglect the virtue of beneficence (to say nothing of justice) is a clear violation of the Hippocratic Oath: primum non nocere, first do no harm.” (Bloodworth et al., 2015). In a culture that values individualism over all else, the concept of the common good is lost in the push for autonomy. Yet, people need to be reminded that every act has consequences, and no suicide happens in a vacuum. We are creatures of relationship, and one suicide ripples its effects into an estimated one-hundred thirty-five other lives (Cerel et al., 2018). And what does it say to a young person suffering with depression and contemplating suicide? “It’s fine for your grandparent to commit suicide because he or she is old and no longer useful, but you are worth more because you are young and can be productive.” At some point, the youth will draw the quite logical conclusion that their life is no longer worth much if her grandparent’s life is not valued (or if the grandparent is even celebrated for killing himself or herself and relieving others of the burden of caring for them). Suicide rates have been shown to increase in jurisdictions that legalize PAS. 2 Drs. Jones and Paton evaluated the rates of suicide in the first four U.S. states that legalized PAS and compared the results to all other states. There was a significant increase in total suicides of 6.3% (95% confidence interval = 2.7%, 9.9%) and no reduction in the rates of nonassisted suicides. “The introduction of PAS seemingly induces more self-inflicted deaths than it inhibits…. This suggests either that PAS does not inhibit (nor acts as an alternative to) nonassisted suicide, or that it acts in this way in some individuals but is associated with an increased inclination to suicide in other individuals.” (Jones, Paton 2015) To say that assisted suicide is an individual person’s choice is a fallacy—everyone is affected by it, and the Church is correct to stand firm to defend the dignity of life until natural death.
Offering Hope and True Compassion
Within the Introduction of Part Five of the ERDs, there are some beautiful thoughts expressed. A few of them will be presented and briefly discussed here. “What is hardest to face is the process of dying itself, especially the dependency, the helplessness, and the pain that so often accompany terminal illness.” (USCCB 2018, 20)
This statement cuts to the heart of the matter for proponents of PAS. Of those who chose to die by assisted suicide in Oregon in 2020, the reasons for dying indicated by more than half of patients were: less able to engage in activities making life enjoyable (94.3%), losing autonomy (93.1%), loss of dignity (71.8%), and burden on family and friends/caregivers (53.1%) (Public Health Division 2020, 12). Fear of being dependent stems from the cultural idol of autonomy and is really an echo from the garden: you shall be like gods. Don’t tell us what to do with our bodies! If YOU don’t want PAS then don’t use it, but how dare you prevent others from choosing it? Supporters of PAS fail to realize that it is a slippery slope. Once the idea becomes mainstream, then everyone will be pressured to request PAS. Dr. T. Brian Callister testified in 2019 to the Nevada legislature that he had two patients, one from Oregon and one from California (both states where PAS is legal), who were denied life-saving treatments and offered lethal prescriptions instead. Neither he nor his patients had requested PAS, yet it was offered to them as a treatment option, and in a state where PAS was not legal. His conclusion was that “legalizing assisted suicide actually limits your choices and access to healthcare” (Callister 2019). Derek Humphry, founder of the Hemlock Society, a predecessor organization to what is now called Compassion & Choices, argues the same idea—it will be economics, not freedom or autonomy, that will ultimately push assisted suicide to become standard practice (Callister 2019). Furthermore, Humphry also predicts that “assisted suicide will remain ‘voluntary’ but elderly patients will know what would be ‘the morally correct thing to do for their family’ once they become a burden on others” (Doerflinger undated). Caring for those on the final leg of their earthly journey should include proper supportive care, to let them know they are valued and have dignity regardless of their functional status, not to tell them to end their life because they have lost utilitarian value. “The task of medicine is to care even when it cannot cure.” (USCCB 2018, 20)
Proponents for PAS say that offering a choice to commit suicide is the caring option, that it provides patients relief to know they can decide when to die. Yet, this is a hollow shell of comfort because PAS does not guarantee a peaceful death (Patients Rights Action Fund 2021). Euphemisms are also used to make it palatable: aid-in-dying, death with dignity, compassion and choices. Yet, dignity does not depend on functionality; dignity comes from being made in God’s image. And what is compassion? It means to be with someone in their suffering; PAS is about terminating the sufferer. Admittedly, it is difficult to be a witness to suffering, especially when we are often accustomed to having answers and solutions. However, there are other options that affirm human dignity: palliative and supportive care, attention to the spiritual needs of patients and family members, staying beside someone at the end of their life. These are ways to demonstrate true caring and compassion. When we cannot cure, we can still care. We do not need to kill. “In the face of death—for many, a time when hope seems lost—the Church witnesses to her belief that God has created each person for eternal life.” (USCCB 2018, 20)
As previously noted, the secular world often wants to exclude any mention of faith or religion from end-of-life conversations. Yet, having belief in Heaven—and hoping that we can go there—is the very idea that can bring true comfort when facing a terminal diagnosis. As Catholic physicians and healthcare professionals, we can begin the conversation with those supporting or seeking PAS by explaining our views on the grounds of natural law, and then hopefully we will be able to take the discussion to the higher ground of God’s law. Whether patients know it or not, the Christian view provides the true hope they are seeking when facing end-of-life decisions, and we should be knowledgeable about the supportive care options that are available for our patients while remaining compassionate and understanding when presenting those options.
Conclusion
When discussing end-of-life issues within a culture that admits only physical realities and seeks to be free from all suffering, we must be prepared to meet people where they are. And where they are is often a place that is indifferent or hostile to faith. As our Lord Himself told us, “Behold, I am sending you like sheep in the midst of wolves; so be shrewd as serpents and simple as doves” (Mt 10:16). We must be the voices that proclaim the truth of a spiritual realm and the power of uniting our suffering to Christ’s for our redemption. Shrewdly using natural law and the gems contained within these Directives, we can gain moral ground with those who view the world differently than us. In this manner, we can gently and compassionately advance them away from the culture of death and toward the culture of life. Thereby, we become witnesses to hope, a hope that the world desperately needs.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.