
Abstract
Volatile substance abuse (VSA) continues to cause preventable deaths worldwide. In Australia, petrol sniffing has historically been the main form of misuse in remote Indigenous communities. However, coronial and surveillance data suggest an increasing role of gas fuels and aerosol propellants. Twenty-five VSA-related deaths reported to the Northern Territory (NT) coroner over a 21-year period (2002–2022) were reviewed. In the 22 cases where acute volatile substance inhalation was the direct cause of death, the decedents were all male, and predominantly young Aboriginal individuals aged between 12 and 29 years. Furthermore, petrol vapor inhalation was responsible for most fatalities up to 2018, after which no further petrol sniffing-related deaths occurred. Deaths that occurred after 2018 were associated with the use of propane or butane from aerosol cans, such as those used for deodorants. A public health initiative that resulted from this was the keeping of aerosol deodorants in supermarkets within locked cabinets. In conclusion, public health interventions, such as the introduction of Opal fuel in remote communities in the NT, have been effective, with a sharp decrease in petrol sniffing-related fatalities. However, this seemed to have led to a shift towards the use of other inhalants, most commonly butane and/or propane inhaled from aerosol canisters. Forensic practitioners should be alert to non-petrol volatiles, and public health strategies need to broaden beyond petrol substitution to include regulatory and community-level measures addressing gas fuels and aerosols.
Keywords
Introduction
The deliberate inhalation of volatile substances is an enduring public health and forensic concern.1,2 These substances—ranging from fuels such as petrol, butane, and propane to solvents, aerosols, and gases—are inexpensive and widely available. Their appeal lies in their accessibility and their capacity to produce rapid intoxication. On occasion, inhalation may augment sexual asphyxia. 3 Unfortunately, the physiological effects of volatile substances can be unpredictable and often fatal. Mechanisms of death may include, but are not limited to, oxygen displacement leading to asphyxia, aspiration of gastric contents, and the arrhythmogenic effects of hydrocarbons on the myocardium, a phenomenon sometimes described as “sudden sniffing death.” Sporadically, deaths may be due to accidental asphyxiation from nose and mouth occlusion if petrol is inhaled from a metal can. 4
The current study examined Volatile substance abuse (VSA)-related deaths in the Northern Territory (NT) of Australia over a 21-year period to determine whether there had been any changes in methods used over time.
Methods
A retrospective review of coronial cases in the NT between 2002 and 2022 was undertaken, where VSA was identified as the direct or contributory cause of death, as per the standardized coronial framework. Cases were identified using coronial cause-of-death coding and keyword searches (“volatile substance abuse,” “volatile substance misuse,” “volatile substance inhalation,” “petrol,” “butane,” “propane,” and “organic vapour”) of coronial databases. Each case file typically included police reports, autopsy findings, toxicology results, and coronial findings. Data were extracted on demographic characteristics, location and circumstances, substances involved, co-intoxicants, mechanisms of death, and autopsy features.
The local findings were compared with larger datasets: (i) national NCIS data covering 2000–2021, (ii) a South Australian autopsy study (1983–2002), (iii) Office for National Statistics mortality data from England and Wales, (iv) poison center surveillance in the United States, and (v) reviews of volatile substance use in Indigenous communities.1,5–10 Relevant forensic case reports were also considered to highlight specific mechanistic risks.
Ethics approval was obtained from the Human Research Ethics Committee of the Northern Territory Department of Health and Menzies School of Health Research (HREC 2025–5228), and permission for this research was granted by the NT coroners’ office.
Results
Demographic profile
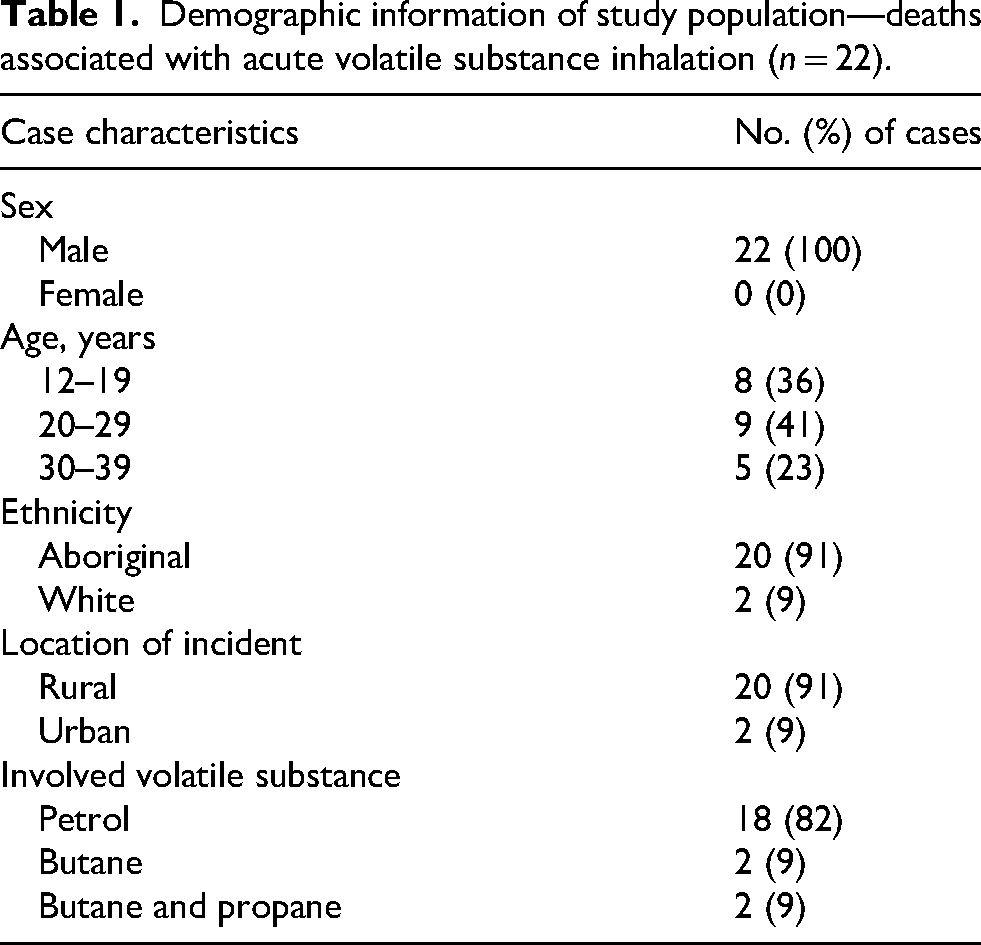
Twenty-five deaths were identified where volatile substance inhalation caused or contributed to death. Acute volatile substance inhalation was the direct cause of death in 22 of the identified cases (see Table 1). In these 22 cases, the individuals were all male, the majority were Aboriginal (20, 91%), with most deaths occurring at rural locations (20, 91%). The age range was 12–37 years, with a median age of 22.5 years and an average age of 22.7 years. The age distribution was heavily weighted towards teenagers and young adults. The highest number of cases in one year was recorded in 2004, when six deaths were recorded (see Figure 1).
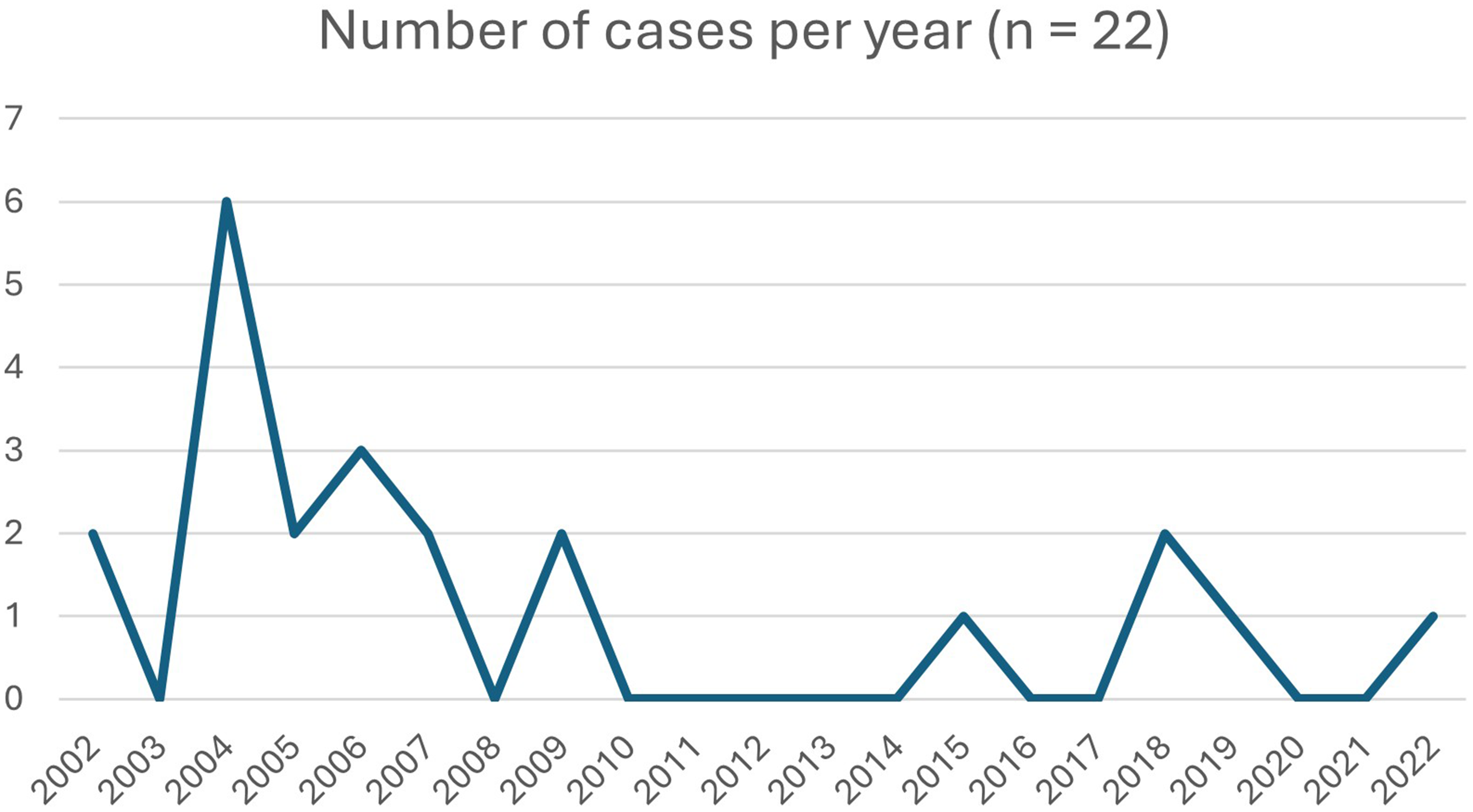
Distribution of cases over the study period.
Demographic information of study population—deaths associated with acute volatile substance inhalation (n = 22).
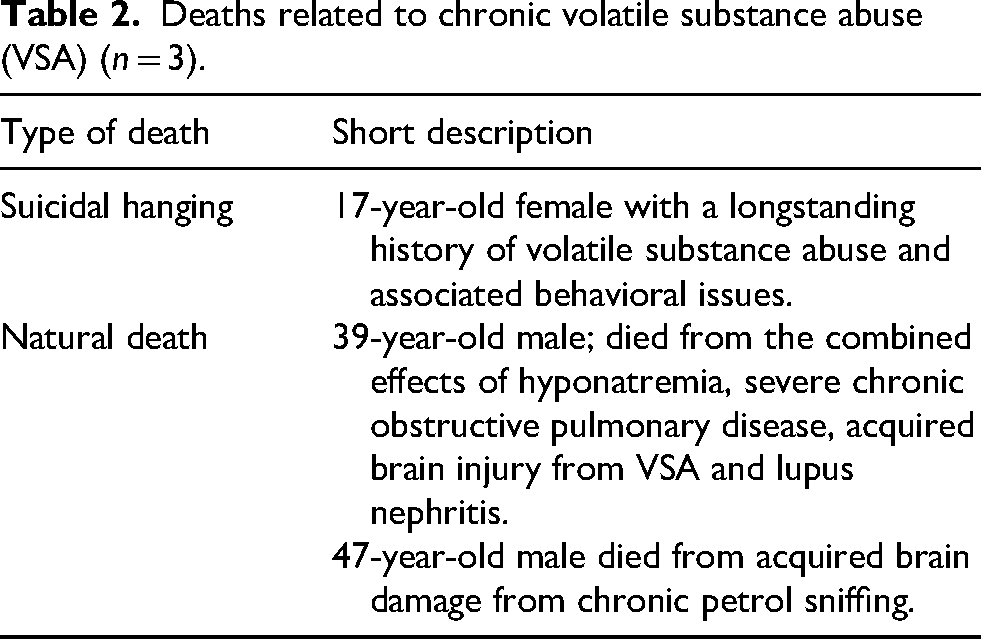
Chronic volatile substance abuse was listed as a contributing factor in death in three cases, involving one female and two male Aboriginal individuals (see Table 2).
Deaths related to chronic volatile substance abuse (VSA) (n = 3).
Substances, environments, and toxicological analyses
Toxicological analyses, including screening for volatile organic compounds (VOCs), were performed in all but two cases (n = 20, 91%) at the Forensic Science South Australia toxicology laboratory. Headspace analysis for the detection of VOCs is not included in the standard scope of analysis and is usually undertaken on request from the pathologist when there are suggestive circumstantial findings or a relevant history indicating possible exposure. The analyses were most commonly performed on post-mortem blood samples (n = 18); in some cases, body cavity fluid, urine, lung, liver, and/or brain tissue were also submitted. The presence of volatile substances was confirmed in 18 of these 20 analyses. In two cases, toxicological analyses were not performed, and in another two cases, toxicological analyses failed to confirm the presence of volatile organic compounds. In these four cases, the cause of death was determined by strong circumstantial evidence and the absence of any other organic or traumatic death at autopsy (see Table 3).
Deaths related to acute volatile substance inhalation—relevant circumstantial information, autopsy findings and toxicology results.
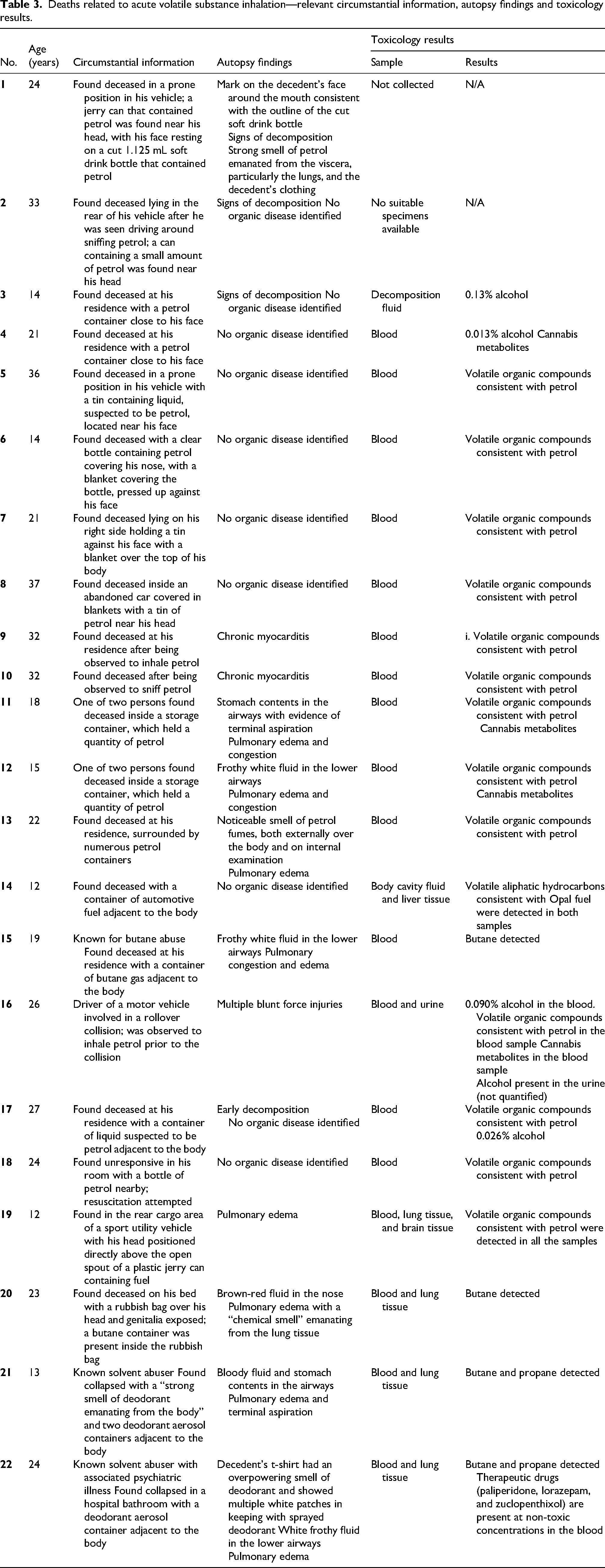
Petrol was implicated in 82% (n = 18) of deaths, with the last petrol-sniffing-related death recorded in 2018. One fatality in 2007 was related to the inhalation of Opal fuel. Gas fuels (primarily butane and propane) accounted for 18% (n = 4), with deodorant canisters found in close proximity to the bodies in two cases, and butane gas containers in the other two cases.
Petrol sniffing deaths often occurred in outdoor locations or abandoned dwellings, with several incidents linked to enclosed spaces or the use of plastic bags to concentrate fumes. The manner of death was deemed accidental in all 22 cases.
There was a known history of VSA present in all cases except in the case of possible auto-erotic asphyxia. The single case of possible auto-erotic asphyxia was included for completeness and represents a distinct behavioral category, not considered to influence the observed VSA trends.
Mechanisms and autopsy findings
The dominant mechanisms of death were asphyxia and sudden cardiac events. Witness reports of abrupt collapse supported arrhythmic mechanisms. Autopsy commonly revealed pulmonary edema and cerebral edema; aspiration and chronic myocarditis were documented in some cases. Associated alcohol and/or cannabis use featured in some cases (n = 6, 27%), but at levels suggesting secondary rather than primary roles in the cause of death. In one case, the cause of death was multiple injuries in the context of acute organic vapor toxicity, as the decedent was involved in a motor vehicle collision shortly after being observed to inhale petrol.
Discussion
In Australia, petrol sniffing was entrenched in some remote Aboriginal communities during the latter part of the twentieth century. The devastating impact on individuals, families, and communities has been well-documented and the subject of several coronial inquests.1,10,11
The introduction of government-subsidized low-aromatic Opal fuel (a variety of low-aromatic 91 RON petrol developed in the mid-2000s by BP Australia as a deterrent to petrol sniffing) and the Volatile Substance Abuse Prevention Act 2005 marked a major policy success, substantially reducing petrol sniffing in targeted regions.12–14 This temporal association has been demonstrated in the current case series, with a peak in the number of cases reported in 2004, followed by a sharp reduction, and the last recorded petrol sniffing-related death occurring in 2018.
However, reductions in petrol misuse did not eliminate volatile misuse altogether in the NT. With petrol being less accessible or less psychoactive, it seems that users are displaying substitution behavior, turning to butane and propane, products that are inexpensive, highly intoxicating, and widely sold and available. There is no general prohibition on the sale of all aerosols in the NT, but specific products, like aerosol paints, are restricted, and others, such as deodorants, have been moved to locked cabinets in many stores to prevent misuse. 12
National and international experience mirrors this trajectory. National NCIS data (n = 164) showed that gas fuels were the most frequent substances in fatal incidents (35%), with petrol and adhesives/paints contributing around 20% each.14,15 Sudden collapse was frequently described, and pneumonia was uncommon, consistent with very rapid death. Similar to what was seen in a South Australian study on inhalant deaths, there were no deaths in this case series from paint and glue inhalation. 6
In the United Kingdom (UK), adhesive inhalation, which had previously dominated mortality figures until the mid-1980s, has been replaced by fuels such as butane and propane, which are now responsible for the majority of deaths.7,16 Similarly, poison center data from the United States from the 1990s and 2000s reveal high rates of adolescent misuse and particularly lethal outcomes with butane and difluoroethane. 8
The mechanisms of death underline the challenges for forensic practice. The syndrome of sudden sniffing death, with fatal arrhythmias occurring within minutes of inhalation, is well described in the toxicological literature and was consistent with several of our witnessed cases. Asphyxial mechanisms were also common, especially in situations involving bags or enclosed spaces. Autopsy findings, by themselves, are rarely diagnostic, although, in some cases, inhaled material may be detected in the lungs if paint has been sniffed. 9 Usually, however, the combination of scene investigation, toxicology, and witness evidence is required to reach a reliable conclusion. Chronic VSA is associated with impairments of cognition and neurological damage 1 ; three cases were identified in the study period where chronic VSA contributed to death, as described earlier.
Sociodemographic themes run through the data. The overwhelming male predominance is consistent across jurisdictions. Indigenous Australians at remote locations bear a disproportionate burden of VSA-related deaths, while data from the UK link mortality to social deprivation. Adolescent vulnerability is universal, with experimentation often beginning in early teenage years.7,8,15
The introduction of low-aromatic fuel has been a significant success story13,14; however, the rise of gas fuels and aerosols necessitates a new or revised policy response. Measures that may be introduced include restrictions on the sale of lighter refills, modifications to packaging, community-driven education programs, and enhanced surveillance through coronial databases. Interventions would have to be culturally informed and community-led to have a lasting impact.
Although this study was limited by its modest sample size and the inherent challenges of toxicology (volatiles will only be tested for if suspected), the findings are consistent with those from larger datasets nationally and internationally. They highlight the urgent need for broadened strategies to reduce deaths from VSA.
Conclusions
VSA remains a cause of preventable death in the NT; however, a shift has occurred from historical petrol sniffing to non-petroleum volatiles, typically involving the inhalation of gases from aerosol cans. Forensic practitioners should anticipate involvement of non-petroleum volatiles and consider the possibility of sudden arrhythmic death even when toxicology is limited. Public health efforts that have successfully addressed petrol sniffing must now be adapted to include the realities of butane, propane, and aerosol misuse. Method substitution is an ever-present problem in dealing with substances of abuse.
Footnotes
Ethical considerations
Ethics approval was obtained from the Human Research Ethics Committee of the Northern Territory Department of Health and Menzies School of Health Research (HREC 2025–5228), and permission for this research was granted by the NT coroners’ office.
Author contributions
MT and SP collated study data and prepared the original draft. MT, SP, and RWB provided input on subsequent drafts.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.