
Abstract
Introduction
The healthcare system has been threatened by the COVID-19 pandemic caused by SARS-CoV-2. Although over 80% of the total cases are asymptomatic or minimally symptomatic, they can still transmit the virus as easily as symptomatic patients (Oran & Topol, 2021). This makes people in exposed areas highly vulnerable to infection, including healthcare workers who are at high risk of contracting COVID-19 (Mushtaque, Dasti, et al., 2021). Additionally, pandemic-related factors, such as burnout (Mushtaque, Raza, et al., 2021), Corona anxiety (Sarfraz, Hafeez, et al., 2022), social loneliness, suicidal thoughts (Ashraf et al., 2021; Hosen et al., 2021), and PTSD (Liu et al., 2021), have significant effects on mental health. Therefore, more mental health research needs to be conducted, along with commensurate changes in healthcare services and regulations (Holmes et al., 2020). Vaccination is the only option for the development of cost-efficient, effective, and safe treatment (Khuroo et al., 2020).
Immunization willingness has been observed to increase due to fear of COVID-19. For instance, healthcare workers (HCWs) have reported increased acceptance of vaccines due to fear of being infected, spreading the virus to others, and dying from COVID-19 (Sarfraz, Ji, et al., 2022). However, in developing countries like Pakistan, insufficient budget schemes and religious perspectives can hinder vaccine acceptance, especially among rural populations. Educated people have an optimistic belief about vaccines, whereas superstitious beliefs about COVID-19 vaccines are predominantly found in rural areas (Mushtaque, Dasti, et al., 2021). Nevertheless, a study shows that over half of the participants have reservations about the vaccine’s safety and efficacy, and 42% are concerned about its side effects. Around 72% planned to get vaccinated, while 28% did not as reported by the same study (Yasmin et al., 2021). Vaccinations have been found to benefit mental health and reduce death anxiety symptoms. Although there is less evidence that vaccinations improve mental health (Nur et al., 2022), a survey of over 8000 people showed that their stress levels decreased after the first dosage of the COVID vaccination (Perez-Arce et al., 2021). However, there is evidence that vaccinations benefit mental health and reduce death anxiety symptoms (Singh & Jaswal, 2022).
Religion is an integral component of human culture and has a significant impact on social interactions and work. Across the globe, people follow various religions, which can both connect and separate individuals. Religion’s effects on coping are complex, as it has both beneficial and detrimental impacts (Pargament & Brant, 1998). According to Taghiabadi et al. (2017), religion, spirituality, and happiness in life reduce death anxiety and existential depression. Additionally, spirituality and enjoying life are coping mechanisms (Taghiabadi et al., 2017). Research on religious fundamentalism has grown in the past two decades (Phillips & Kitchens, 2021), particularly as HCWs confront critical situations and must make difficult decisions for their survival (Abdulkareem et al., 2020). Patients with COVID-19 experience high levels of death anxiety, with helplessness, insecurity, anxiety, and worry being primary factors (Brooks et al., 2020). Özer et al., 2021b found that higher levels of spirituality are associated with lower death anxiety. A survey of nurses revealed that 53.5% had a significant fear of death due to COVID-19, with death anxiety negatively impacting their mental health (Farhadi et al., 2021). The presence of an intrinsic religious orientation reduced death anxiety and increased mental wellness (Farhadi et al., 2021).
In a study on the Pakistani population, listening to religious lectures during COVID-19 was associated with a negative correlation between religiosity and death anxiety (Saleem & Saleem, 2019). A review of 84 studies on religiosity and death anxiety found a positive correlation in 27 studies, no correlation in 41 studies, and a negative correlation in 40 studies (Pandya & Kathuria, 2021; Zhang et al., 2019). Coping mechanisms are shaped by early socialization, belief systems, and ideology (Zhao et al., 2015). Negative religious coping can reduce the connection between COVID-19 fear and depression, death anxiety, and distress (Kızılgeçit & Yıldırım, 2022).
Positive religious coping mechanisms have been shown to improve mental health states, such as COVID-19 anxiety (DeRossett et al., 2021). However, Warner et al. (2021) found that only individuals with high degrees of religiosity demonstrated negative religious coping, which mediated the relationship between stress and depression. Positive religious coping was negatively associated with psychiatric problems, depression, and mental illnesses in Muslims (Mosqueiro et al., 2015). During infectious disease epidemics, constructive religious coping strategies may help individuals avoid grief (Thomas & Barbato, 2020a, 2020b). Religious beliefs can also aid in coping with despair and suicide ideation (Mosqueiro et al., 2015) and promote trust and resilience through positive religious beliefs (Teismann et al., 2017). Positive religious coping strategies have been found to have a widespread impact, with lower levels of anxiety and depression reported among HCWs who use such strategies during the pandemic (Chow et al., 2021). In addition, Thomas and Barbato (2020a, 2020b) observed a negative correlation between positive religious coping and general mental health in a sample of Muslims from the United Arab Emirates during the pandemic. Similarly, the effect of positive religious coping on stress levels among American Orthodox Jews has also been observed (Pirutinsky et al., 2020). Positive religious coping impacts have appeared to be more widespread than negative ones (Fatima et al., 2022), and the levels of anxiety and depression of HCWs have been reported to be lower among those maintaining positive religious coping strategies during the pandemic (Chow et al., 2021).
Although evidence suggests that the COVID-19 pandemic has led to an increase in mental health problems (Hosen et al., 2021), many individuals have engaged with and relied on religious activities. Religious and spiritual rituals are being used to mitigate the social isolation impacts of the pandemic (Lucchetti et al., 2021) and have been shown to have a positive effect on mental health (Zacher & Rudolph, 2021). According to Carvalho et al. (2021), numerous COVID-19 vaccines have been approved for emergency use to prevent the acquisition and spread of the virus and the occurrence of severe cases, hospitalization, and mortality; whereas medical professionals have a crucial role in promoting the importance of COVID-19 vaccination to the public. In Pakistan, the government has made the Sinopharm vaccine mandatory for medical personnel and adults over 55 years old (Mushtaque, Dasti, et al., 2021). In the Western world, legislation is being enforced that prioritizes high-risk groups and HCW vaccination. It is also important to understand healthcare workers' attitudes towards vaccination and communicate accurate information to the public (Mushtaque, Dasti, et al., 2021). Vaccination may help reduce anxiety among those at high risk of infection, including healthcare workers (Othman et al., 2022). Additionally, vaccination may improve quality of life, economic prospects, and social engagement (Rajabimajd et al., 2021).
Studies show that death anxiety is associated with diseases with high mortality rates, such as COVID-19 (Guner et al., 2021). Death anxiety is defined by preoccupations, concerns, and feelings regarding one’s final moments, related to having overpowering thoughts and feelings about mortality (Sarıkaya & Baloğlu, 2016). Fear, threat, and discomfort are also linked to death anxiety (Neimeyer et al., 2003). In the context of the COVID-19 pandemic, a limited number of studies have been conducted investigating the fear of death. Özer et al., 2021b found that nurses and other HCWs working with sick, stressed, or violent patients may experience death anxiety, an unpleasant emotion that occurs when people think about death. In addition to self-reported health anxiety and overall psychological distress, the findings revealed a significant positive correlation between death anxiety and anxious beliefs and behaviors related to COVID-19 (Othman et al., 2022).
In Pakistan, religion plays a significant role in the lives of the population, with 98% of the population being Muslim. Religion is often used as a coping mechanism, especially when dealing with health issues (Shafiq, 2020). As aforementioned, many Pakistani people are unwilling to accept the COVID-19 vaccine, and religious beliefs appear to be one of the factors leading to this unwillingness. This might lead to higher death anxiety levels in HCWs. In addition, as per the analysis of COVID-19-related suicide among HCWs, it has been found that being positive for COVID-19 was the prominent reason for suicide, followed by fear related to COVID-19 infection or transmission (Jahan et al., 2021); this reflects the notion that death anxiety might be higher among HCWs. However, the present study aims to look at the effects of positive religious coping strategies and the acceptability of the COVID-19 vaccination on death anxiety among HCWs engaging with COVID-19 patients in Pakistan.
Material and Methods
Study Design
The current study utilized a cross-sectional survey design to collect data between October 2021 and January 2022. The sample consisted of HCWs employed in public and private hospitals in Pakistan. 10 hospitals from different regions of the country were selected using convenience sampling, including Jinnah Hospital Lahore, Services Hospital Lahore, Govt Said Metha Hospital Lahore, District Hospital Layyah, City Hospital Multan, Nishtar Hospital Multan, Combined Military Hospital Mianwali, Sirati Hospital Layyah, Thal Hospital Layyah, and Fatima Hospital Multan. The hospitals were chosen based on their treatment and care of COVID-19 patients. All participants were vaccinated at the time of data collection.
Data Collection Approach
To be eligible for the study, HCWs had to be working with COVID-19 patients and at least 20 years of age. The self-administered questionnaire was distributed using the convenience sampling technique, and the research team utilized their professional contacts to approach the selected hospitals. The required sample size was calculated using G-power software with a 5% margin of error at the 95% confidence level, resulting in a sample size of 320. A total of 500 participants were approached, and 389 completed responses were received, resulting in a response rate of 77.8%. The collected data were screened for completeness, quality, and consistency, and incomplete or missing responses were excluded from the analysis.
Data Collection Tools
In addition to basic socio-demographic information, the data collection tools included several scales. The entire questionnaire was in English, given that all participants were HCWs and were assumed to be proficient in English. A description of the scales utilized in the study was also provided.
Positive Religious Coping Strategy
The Brief Religious Coping Scale, developed by Pargament and Brant (1998), measures two kinds of religious coping: negative religious coping and positive religious coping. It is a self-administered scale. The current study assessed only positive religious coping techniques using 12 elements of positive religious coping (i.e., “looked to have a stronger relationship to GOD”). The positive religious coping scale was assessed on a five-point Likert scale ranging from 1 (not at all) to 5 (a lot). The reliability value of the scale was 0.935.
Vaccine Acceptance
The Vaccine Acceptance scale, developed by Sarathchandra et al. (2018), consists of a total of 15 items (i.e., “COVID-19 vaccines are safe”). It is a self-administered questionnaire used to assess vaccine acceptancy. The scale has four subscales (positive attitude towards vaccine, vaccine effectiveness, vaccine schedule, and legitimacy of authorities). The vaccine acceptance scale was assessed using an eight-point Likert scale. In this study, the reliability of the scale was 0.895.
Death Anxiety
The Death Anxiety scale was developed by Templer (1970) and consists of 15 items. It is a self-administered questionnaire. The scale questions depict death-related thoughts (i.e., “when I heard of someone’s death, it disturbed me for several days”). The death anxiety was assessed using a five-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). The reliability of the scale was 0.973 in this study.
Ethical Consideration
This study was conceived and conducted in accordance with the Government Said Metha Teaching Hospital Lahore, Pakistan’s ethical norms. Accordingly, the Faculty of Medical, Government Said Metha Teaching Hospital, granted ethical approval (reference number 123–21). Informed consent was taken from the participants before enrolling in this study. It was guaranteed to the participants that the collected data did not lead to the identification of the survey respondents, ensuring the respondents' confidentiality and anonymity to keep the results unbiased.
Data Analysis
The data were analyzed by employing SPSS-25 statistical software tool. The categorical variables were measured by frequency. The readability of the scales was determined by using Cronbach’s alpha. The Pearson product-moment correlation was utilized to evaluate the relationship between the independent and dependent variables. Further associations and effects were measured using a PLS-SEM.
The study framework is presented in Figure 1, which shows independent variables (Vaccine acceptance and positive religious coping strategy) and dependent variable (Death Anxiety). Study framework.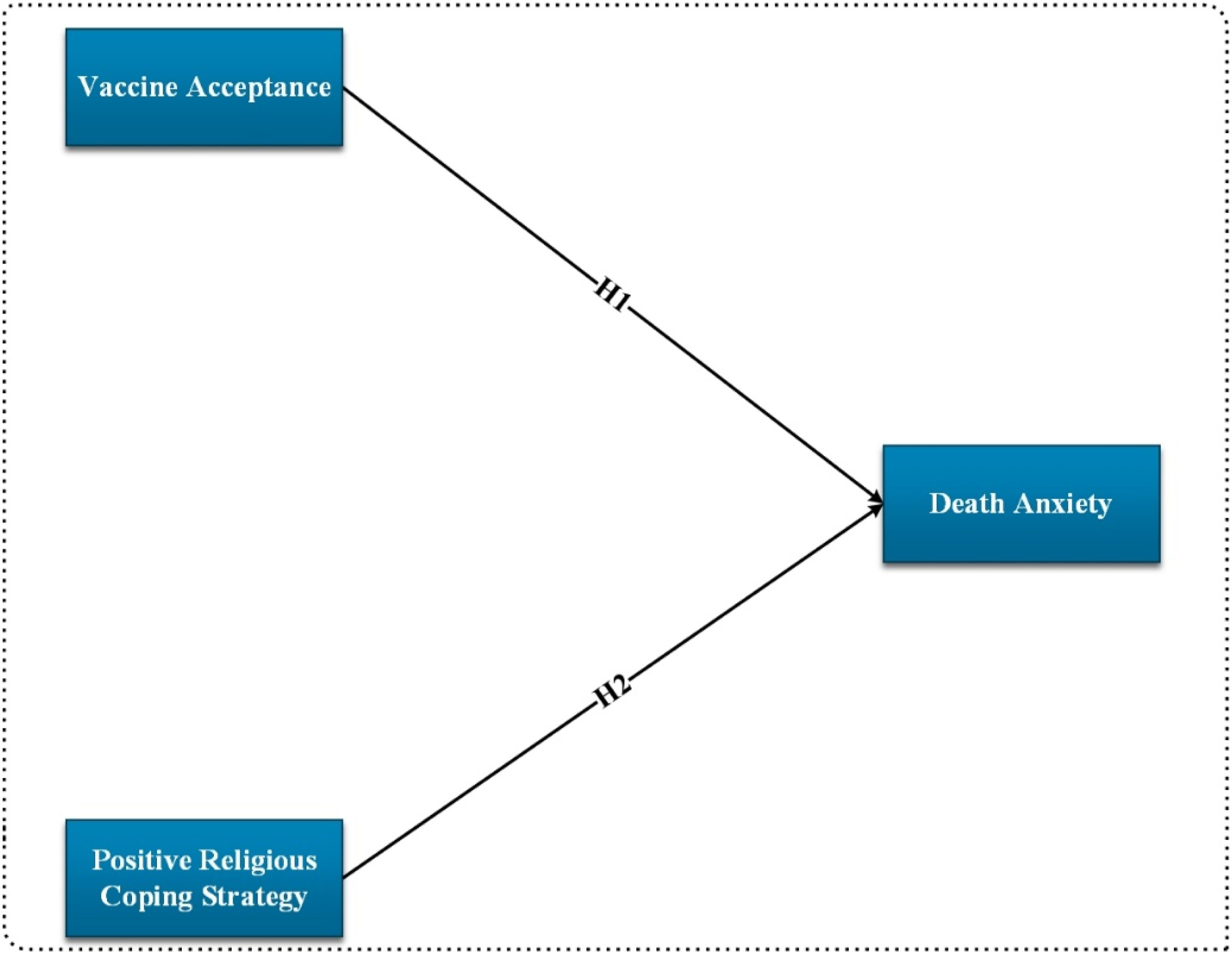
Results
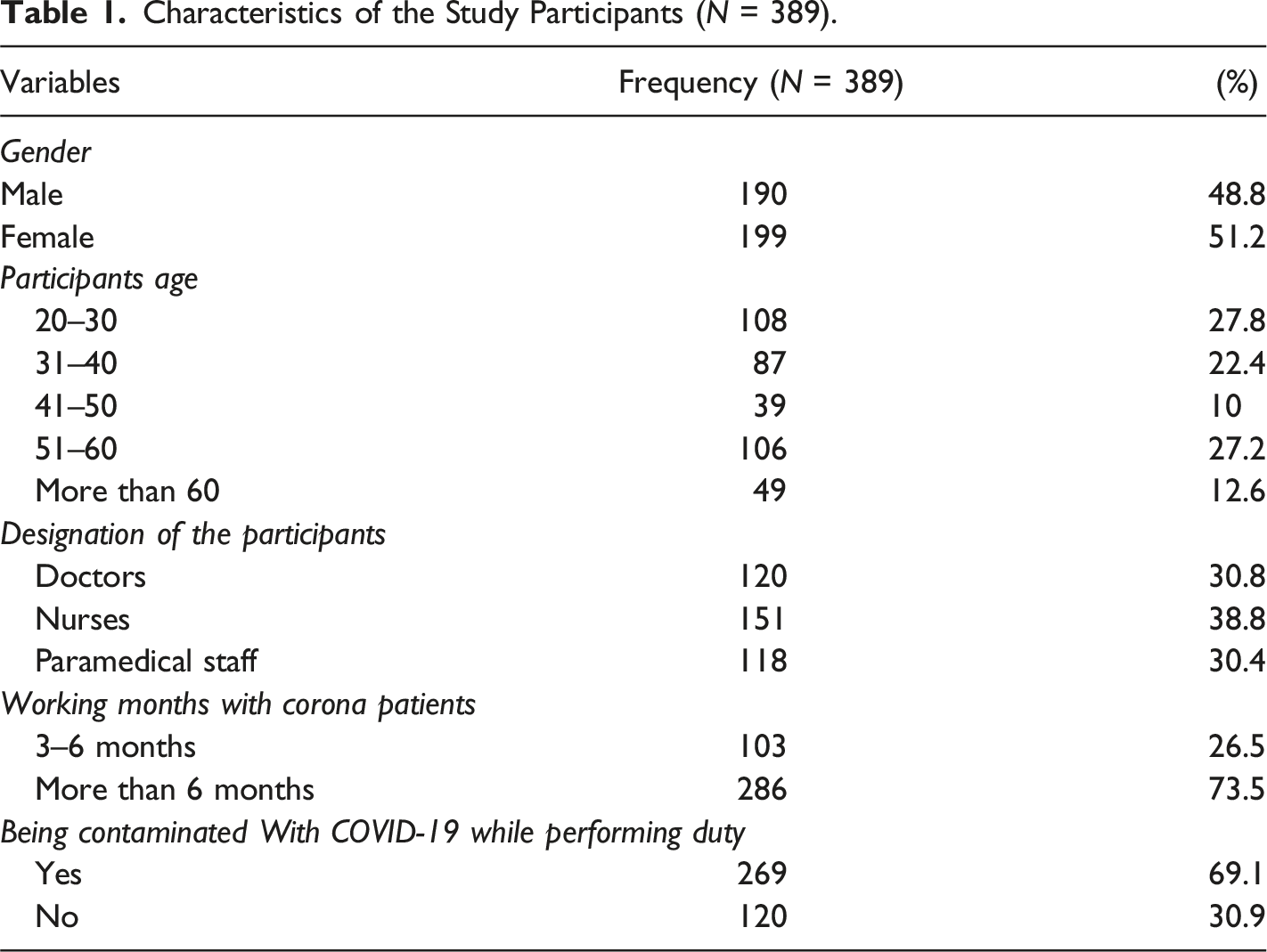
Characteristics of the Study Participants (N = 389).
Reliability of the Scales.
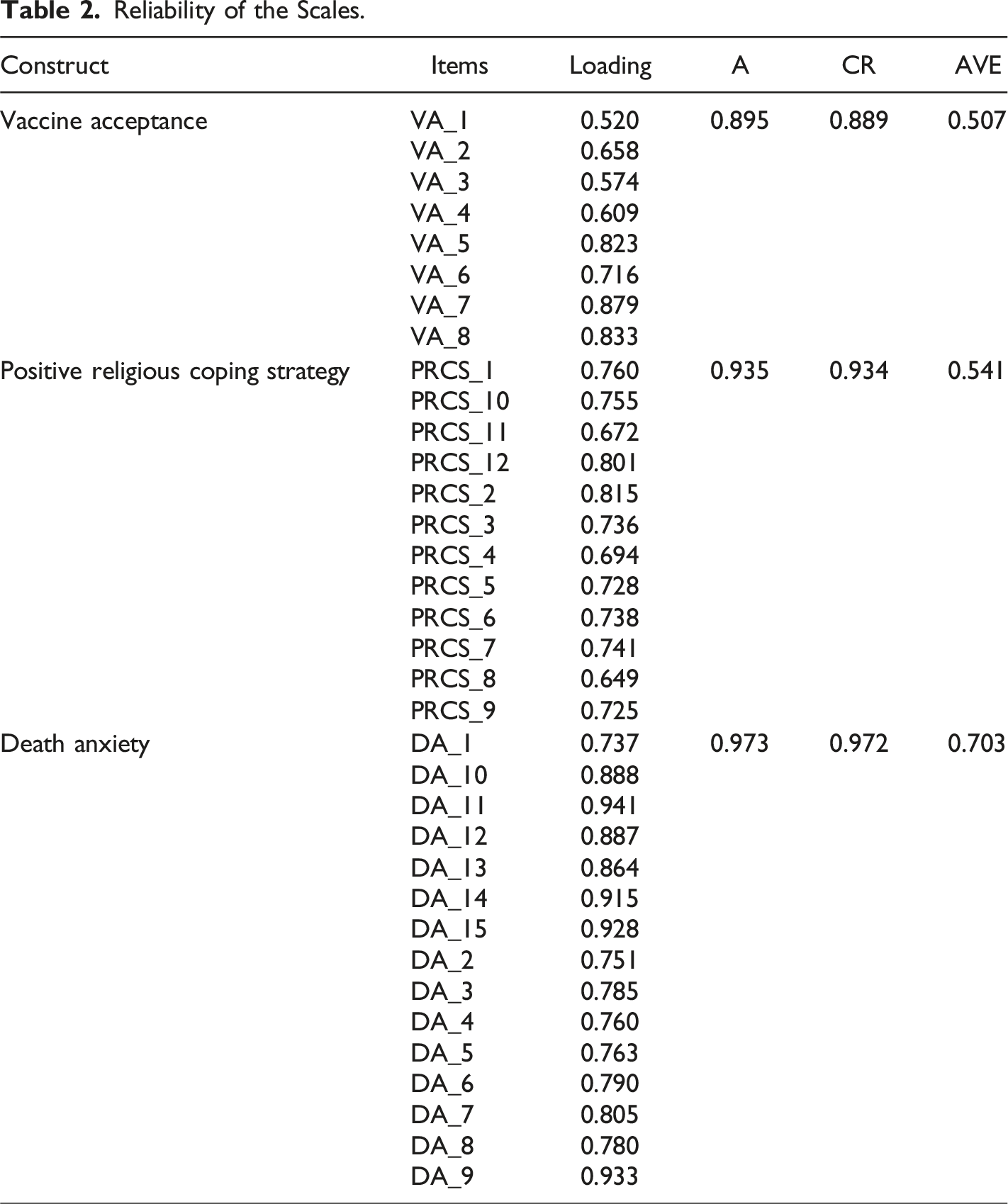
Figure 2 is a graphical representation of the study measurement model while Figure 3 shows the results of structural model. Factor loadings are presented in the figure and all 35 items values are within the suggested range, which should be greater than 0.5 (Hair et al., 2010 2010). Measurement model. Structural model.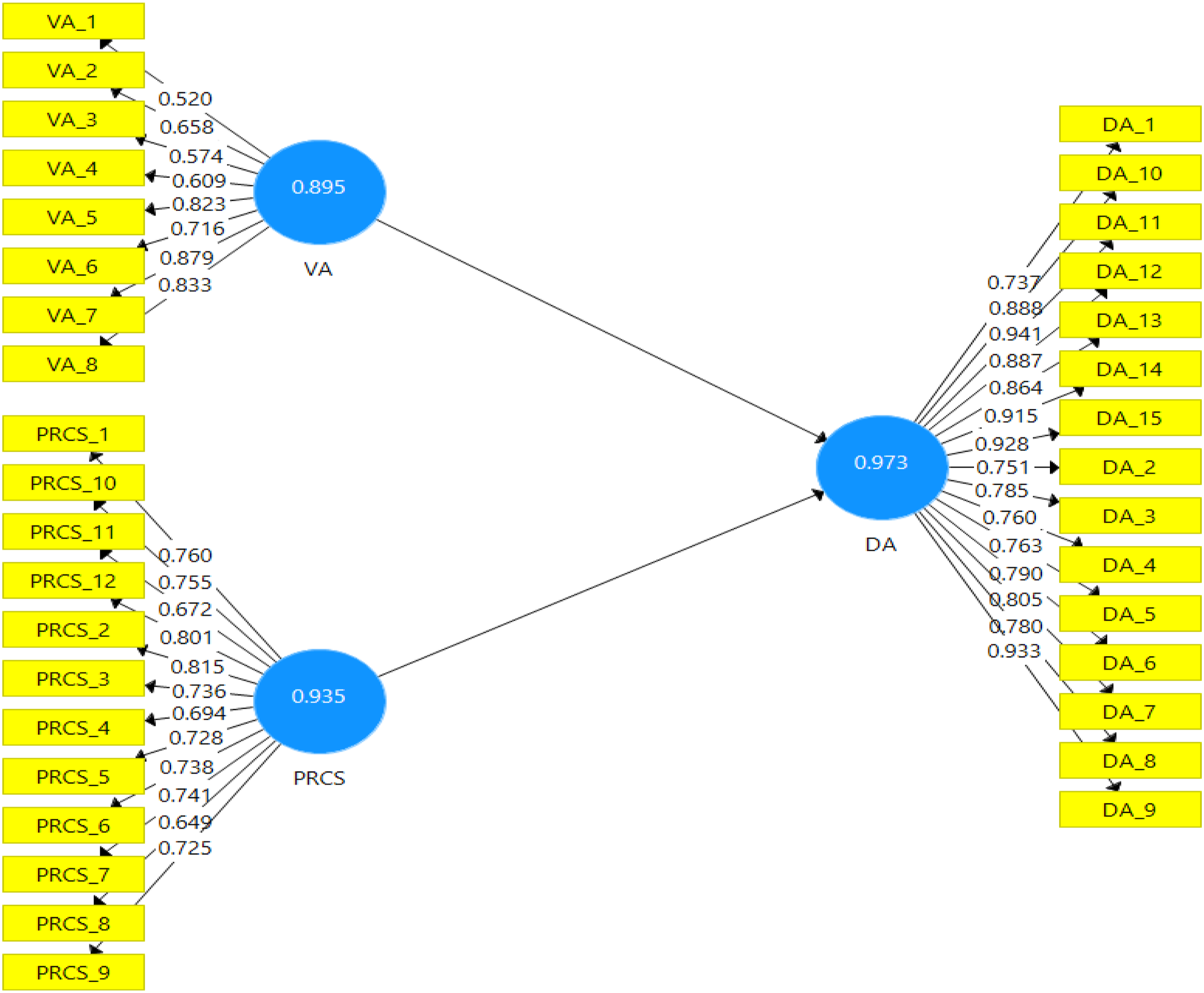
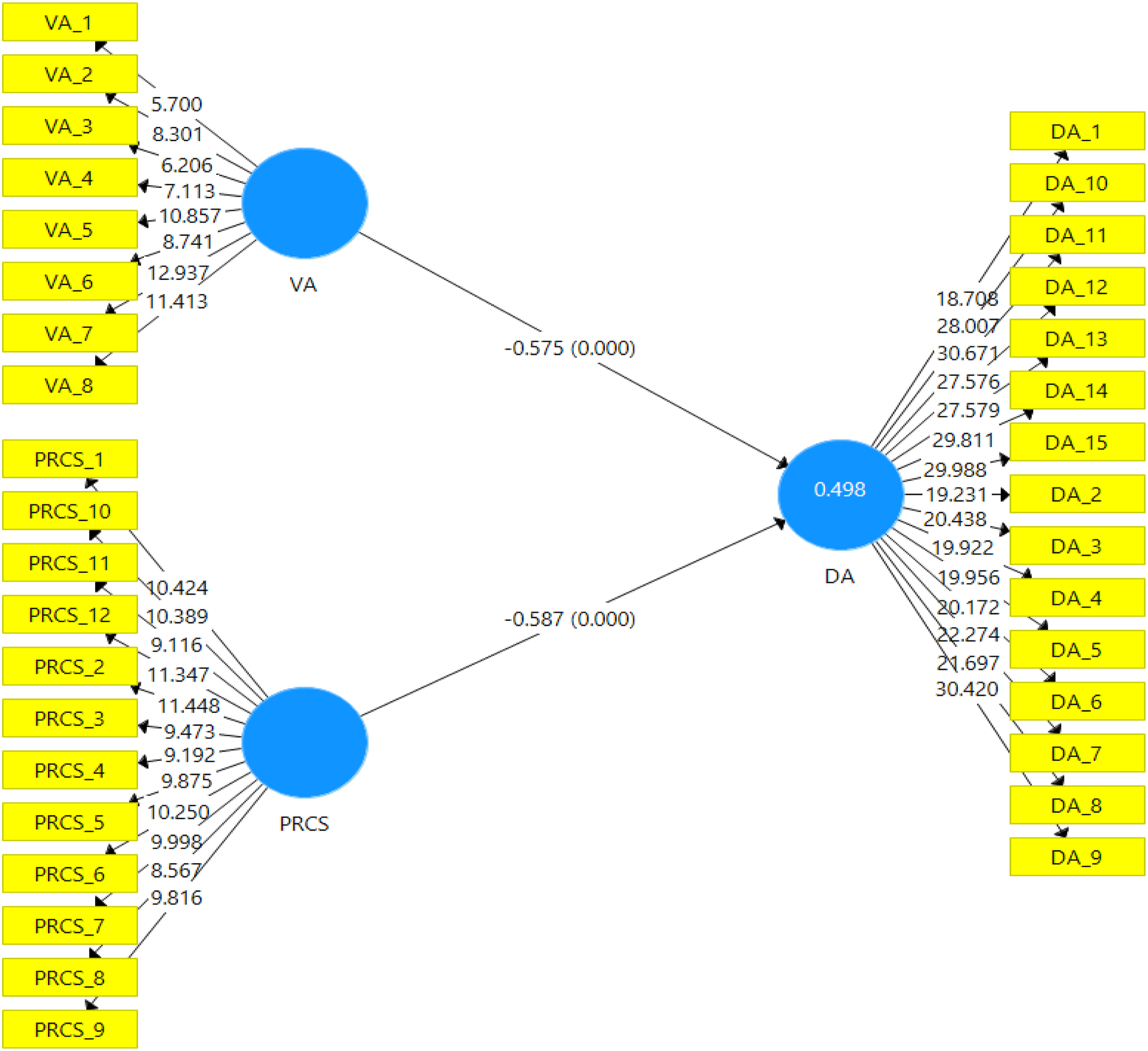
Hypotheses Testing Direct Effect.
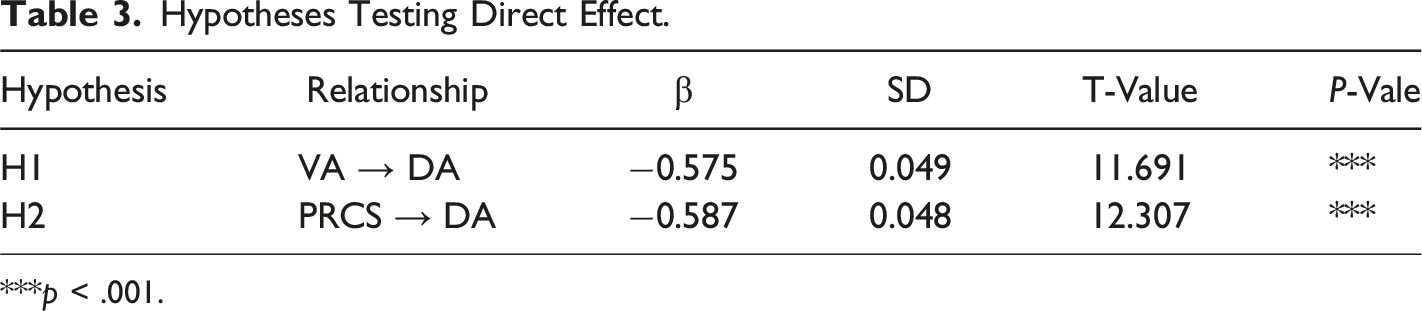
***p < .001.
Quality Criteria.
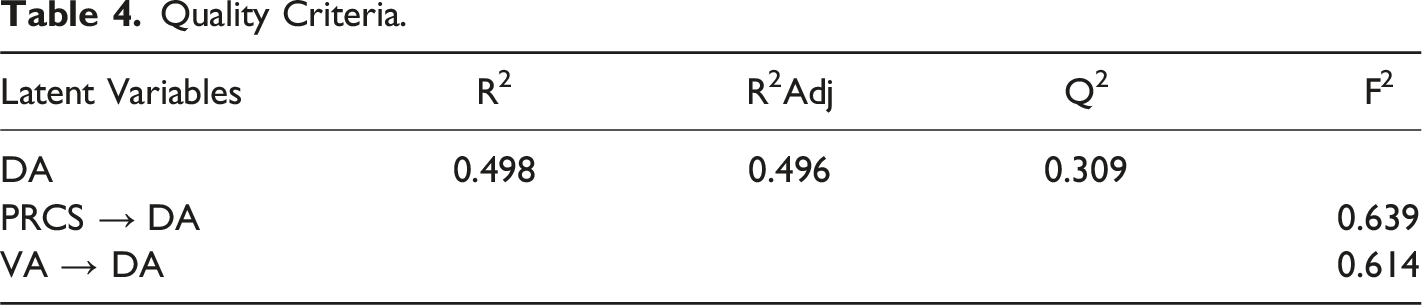
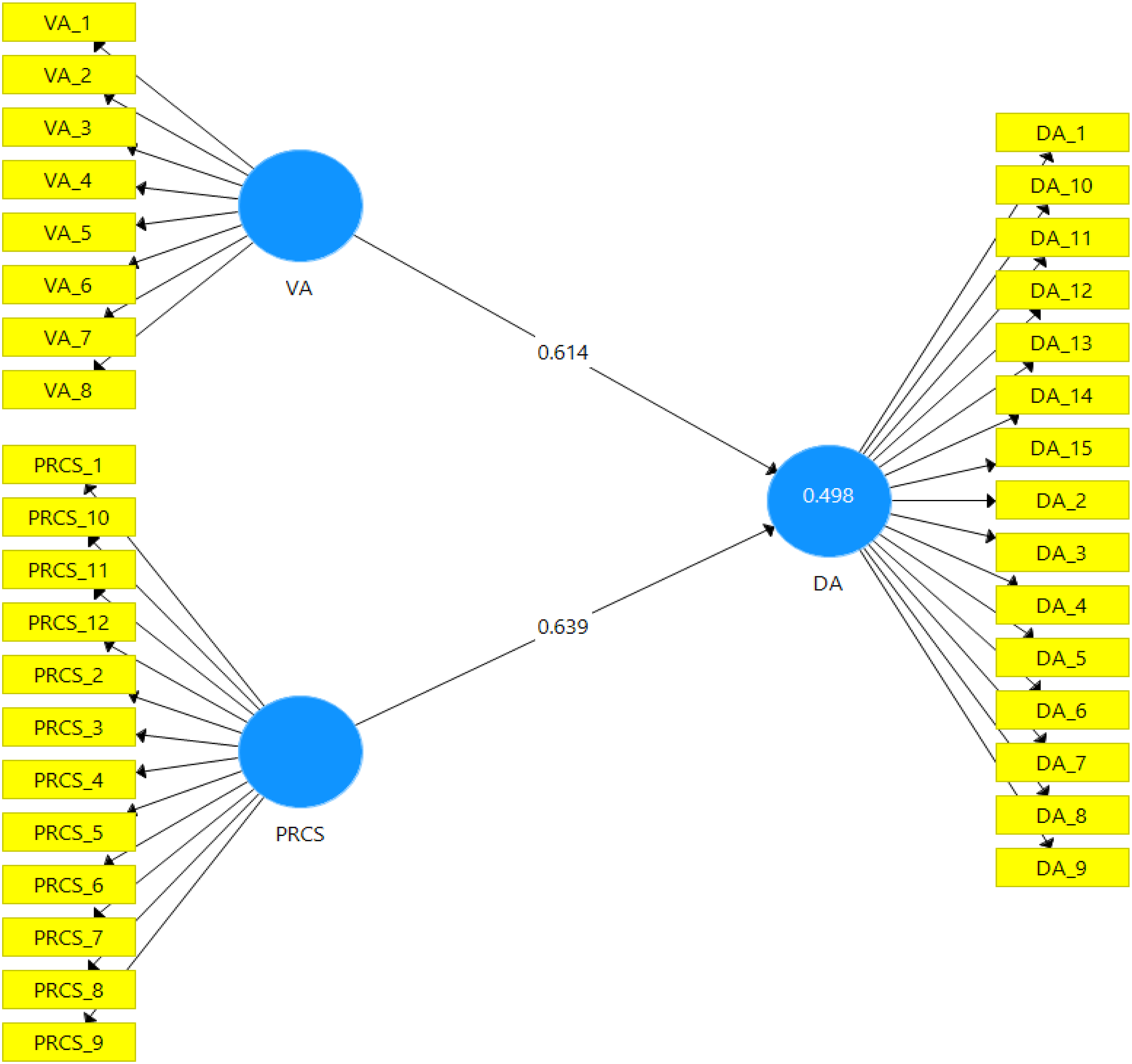
Graphical representation of R2 and F2.
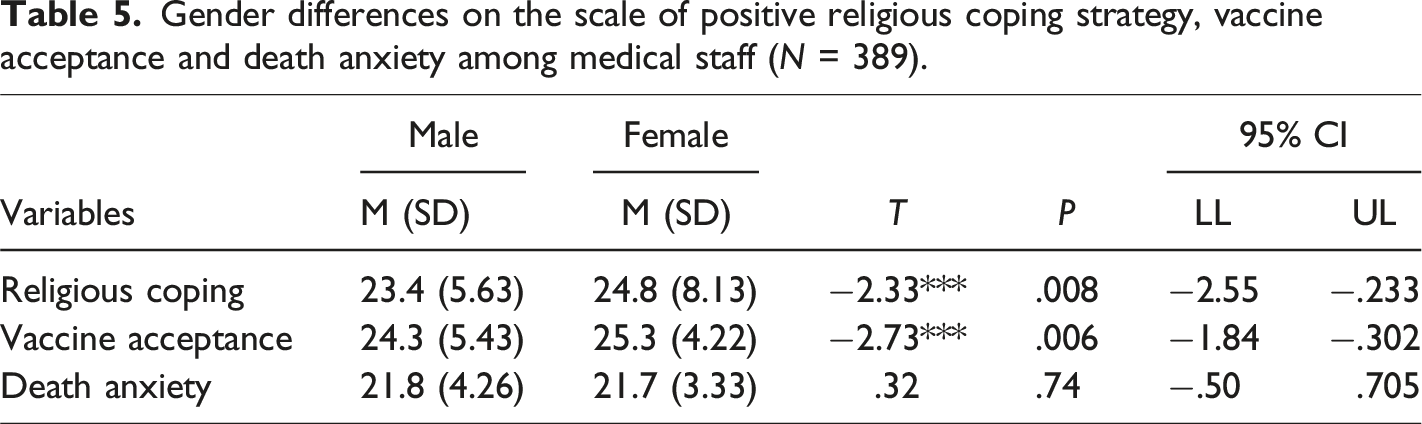
Gender differences on the scale of positive religious coping strategy, vaccine acceptance and death anxiety among medical staff (N = 389).
Discussion
This study explores the relationship between religious coping strategies, COVID-19 vaccine acceptance, and death anxiety among Pakistani HCWs working in COVID-19 wards. The results show that a positive religious coping strategy and vaccine acceptance have a significant impact on reducing death anxiety. These findings support previous research that has demonstrated the benefits of practicing religiosity coping during the pandemic (Mahmood et al., 2021). Due to their increased risk of exposure to COVID-19, HCWs are vulnerable to infection and death. Physicians play a critical role in controlling the spread of the virus, and non-clinical HCWs are also at high risk of infection due to their frequent contact with medical personnel and COVID-19 patients (Jain et al., 2020; Shreffler et al., 2020). Research has shown that HCWs experience high levels of death anxiety due to the possibility of their patients' or their own death from COVID-19 (Lázaro-Pérez et al., 2020).
Vaccination is an effective means of controlling the spread of COVID-19, and this study examines the relationship between vaccine acceptance and death anxiety among HCWs. The results of this study demonstrate that most HCWs have a positive attitude towards the COVID-19 vaccine and that vaccine acceptance significantly reduces death anxiety. The high vaccine acceptance rate may be due to HCWs' increased risk of contracting COVID-19, which highlights the perceived advantages of vaccination and decreases vaccine safety concerns (Pogue et al., 2020). The higher vaccine acceptance may be due to the COVID-19 mortality rate of HCWs. In this study, 69% of the participants reported being contaminated with COVID-19; perhaps this could be a reason for the high vaccine acceptance. This can be explained by the Health Belief Model, whereby the perceived advantage of vaccination includes a large reduction in COVID-19 infection fear, increasing worried individuals' intention to take the vaccine. With respect to gender, there was no significant difference in death anxiety scores; while female HCWs had a higher mean score of vaccine acceptance, this could be because females were more concerned about the adverse effects of the pandemic (Hosen et al., 2021). The participants knowing more about COVID-19, and working in the medical area, likely made them more likely to get the vaccination than those working in other fields (Malik et al., 2021). Comparable to a study that monitored the mental health of Lebanese HCWs at the medical facility 6 months after getting the COVID-19 immunization and found that only 23% of them exhibited indicators of anxiety, the participants' levels of death anxiety were low (Msheik El Khoury et al., 2021). Another study involving the same cohort of largely immunized HCWs caring for COVID-19 patients identified a correlation between low anxiety and high levels of resilience. The participants' lack of anxiety may be explained by the high vaccination rate and the availability of personal protection equipment (Sakr et al., 2022).
According to Bentzen (2021), religiosity is thought to provide individuals with cognitive and emotional resources that help them overcome uncertainty and hardship. However, Chen et al. (2020) found a link between religiosity and mental health difficulties, such as the belief that COVID-19 is a punishment from God. Nonetheless, the current study revealed that a more positive religious coping style was associated with a lower level of death anxiety, and participants with higher scores on the spirituality scale reported less death anxiety. Rajandram et al. (2011) suggest that medical professionals facing anxiety may use hope and positive expectations to alleviate symptoms. In addition, the high levels of work-related burnout observed in Pakistani HCWs during the pandemic (Mushtaque, Raza, et al., 2021) may have influenced the use of religion as a coping technique, given the favorable effects of religion on mental health. Mahmood et al. (2021) also found that people with health anxiety frequently turn to religion for refuge, highlighting the need to study the role of religion and spirituality in pandemic-induced anxiety. Furthermore, the Terror Management Theory suggests that religion can help people cope with anxiety (Vail et al., 2010), which may have been it may have influenced religious attitudes and intensified the levels of death anxiety in the COVID-19 context (Rigoli, 2021). For example, individuals with a higher level of religiosity may believe in God as a helper, whereas those with a lesser level of religiosity may believe in God as a punisher (Chen et al., 2020). This is because of the fact that good religious coping, intrinsic religiosity, and trust in God were associated with less stress and more positive impact, but negative religious coping and mistrust in God were not, as per a study among American Orthodox Jews (Pirutinsky et al., 2020). Therefore, it can be said that faith can help people overcome adversity (Pirutinsky et al., 2020). With respect to gender, in this study, female HCWs were found to practice the positive religious coping strategy to a higher level compared to male ones, although there was no significant difference observed for death anxiety.
It is important to note several limitations of this study. First, the cross-sectional design precludes definitive assertions about causes and effects. Furthermore, the data were collected only from one province in Pakistan, which may limit generalizability to other provinces with different cultural and linguistic backgrounds. In addition, the fact that all participants were already vaccinated may have impacted their scores on the vaccine acceptance scale. Self-report surveys may also suffer from social desirability bias. Moreover, this study only included Muslims, making it difficult to compare results across different religious groups. Future research should consider using experimental methods to investigate religious coping strategies, and should also include participants from different geographic and ethnic backgrounds, with varying spiritual perspectives, social backgrounds, or levels of spirituality.
Implications
It is crucial to consider religion and spirituality in mental health treatments during social and health crises, as per the present study, which shows that positive religious coping mechanisms reduce death anxiety. In order to integrate religion and spirituality into mental health treatments during the pandemic and beyond, healthcare professionals such as physicians, counselors, and social workers must collaborate across various societal institutions. The findings highlight the essential role of healthcare workers in providing emotional support to patients and ensuring vaccine safety at the community level.
Conclusion
During the COVID-19 pandemic, frontline healthcare workers (HCWs) have reported increased psychological distress as they directly deal with COVID-19 patients. However, according to the current study, COVID-19 immunization has a positive impact on individual mental health. This is because vaccines offer protection from COVID-19 infection, reducing the risk of death anxiety among HCWs caring for COVID-19 patients. Additionally, the study found that HCWs who adopt positive religious coping strategies tend to experience better mental health outcomes, higher levels of hope, and lower levels of dread, concern, and depression. This information confirms the importance of continuing religious and spiritual practices during the pandemic. Consequently, healthcare providers should be aware of patients' and their families' spiritual and religious beliefs to provide the most comprehensive care possible, taking into account the beneficial and harmful uses of such beliefs.
Footnotes
Ethical Approval
This study was conceived and conducted in accordance with the Government Said Metha Teaching Hospital Lahore, Pakistan's ethical norms. Accordingly, the Faculty of Medical, Government Said Metha Teaching Hospital, granted ethical approval (reference number 123–21). Informed consent was taken from the participants before enrolling in this study. It was guaranteed to the participants that the collected data did not lead to the identification of the survey respondents, ensuring the respondents' confidentiality and anonymity to keep the results unbiased.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This study is supported by the Scientific Research Start-up Fund of Zhejiang Shuren University, PR China (KXJ0122604).