
Abstract
Aerobic exercises (AE) have been found to have short-term positive effects on certain aspects of cognitive functioning. Pilates exercises (PE) may have similar benefits. In this randomized controlled study, we compared the effectiveness of PE and AE on participants’ cognitive functions. We randomly assigned 52 physically inactive young adult volunteers into either a PE group (Mage = 20.85, SD = 2.11 years; 18 females and 8 males) or an AE group (Mage = 19.88, SD = 0.91 years; 18 females and 8 males). In both groups, participants engaged in a moderately intense exercise program three days a week for four weeks. We tested participants on cognitive measures of selective attention and inhibitory control (Stroop test), verbal fluency (verbal fluency tests (letter and category); VFTs), and speed of movement (Nelson’s Speed of Movement Test; NSMT). There were no group differences on the Stroop and the VFTs (p>0.05). However, there was a significant pre- to post-exercise difference for participants in both groups with a medium-large effect size (ES) on Stroop sections 1, 3, 4, and 5, respectively (PE: p < 0.001, ES = 0.58, p = 0.001, ES = 0.54, p < 0.001, ES = 0.88, p = 0.001, ES = 0.60; AE: p < 0.001, ES = 0.70, p < 0.001, ES = 0.89, p < 0.001, ES = 0.86, p = 0.006, ES = 0.65). There was a large effect size pre- to post-exercise detected for VFT sections labeled letter (PE: p < 0.001, ES = 1.45; AE: p < 0.001, ES = 1.11), and category (PE: p < 0.001, ES = 1.11; AE: p < 0.001, ES = 0.83), and there was a large ES for NSMT in the PE group (p < 0.001, ES = 1.07). Both PE and AE may lead to short-term improvements in selective attention, verbal fluency, and executive control in inactive young adults, and PE may benefit speed of movement.
Introduction
Young adults aged 18–25 years are often engaged in continued academic education to gain professional skills that demand concentration, attention, and rapid shifts between complex tasks. For these various skills to be acquired and developed, the dorsolateral prefrontal circuit in the prefrontal cortex must be active (Verburgh et al., 2014). The prefrontal cortex manages sensory input and motor output processes involving complex cognitive and emotional behaviors (Kane & Engle, 2002). Aside from its role in cognitive control, this cortical region seems to be related to executive functions such as decision-making, information processing, new learning (Hwang et al., 2016), attention, and working memory (Kane & Engle, 2002). Young adulthood is a critical period for frontal lobe brain growth (Sowell et al., 1999), and frontal lobe–mediated executive functions are important to these cognitive activities (Hillman et al., 2008). Others have described such additional executive functioning component skills as selective attention, inhibitory control, rapidly shifting mental sets, verbal fluency, and speed of movement, a psychomotor function in which cognitive and physical functions work together (Singh & Singh, 2016).
Other factors may impede or interfere with the smooth development and deployment of these components of executive functioning during this period of development. These may include inactivity, a sedentary lifestyle, and psychological factors, such as anxiety, stress, and depression (Marmeleira, 2013; Vancini et al., 2017). These factors may cause decreased academic achievement and self-esteem, focusing problems, and other cognitive concerns (Hillman et al., 2008; Khan & Hillman, 2014). Perhaps, particularly in this age group, strategies to maintain these cognitive skills should be developed to reduce and prevent these interfering factors from negatively affecting academic achievements and early career development. Exercise has been accepted as one such coping strategy for protecting executive functioning (Hillman et al., 2008). Specifically, regular aerobic exercise (AE) has shown benefits on aspects of cognitive functions such as psychomotor speed, reaction time, cognitive flexibility, memory, and attention in healthy adults (Guiney & Machado, 2013; Lin et al., 2018; Masley et al., 2009). These AE results have raised further questions as to whether other types of exercises might have similar benefits, perhaps particularly including exercises that encourage mental focus and attention.
Pilates-based exercises require practitioners to mentally focus on targeted body regions (García-Garro et al., 2020), and Pilates exercises (PE) are intended to improve the body–mind connection and the quality of human movement by directing attention to the moving body segment (Kim et al., 2019; Sorosky et al., 2008). Pilates aims to create new and controlled movement patterns, inhibit previous compensated movements, target muscle use, and provide self-control. Pilates contributes to neuronal development by increasing the amount of neurotrophin in brain areas related to learning, memory, and executive functions (Memmedova, 2015). Thus, Pilates appears to be an exercise method that might also positively affect cognitive functions. Indeed, past studies investigating the effect of PE in women aged 60 years and over (García-Garro et al., 2020), elderly people with cognitive impairment (Jurakic et al., 2017), and individuals with multiple sclerosis (Kucuk et al., 2016) have reported improvements on cognitive domains or cognitive functions. However, no prior studies have investigated the cognitive effects of Pilates for healthy young adults. Accordingly, we undertook this study to evaluate and compare the effects of PE and AE on participants' cognitive functions. We hypothesized that Pilates would improve selective attention, reaction speed, cognitive flexibility, and executive function control in young adults.
Method
Study Design
This was a randomized, controlled, and single-centered study with its database recorded at “clinicaltrials.gov.” Since there was no minimal effect size estimate for a change in the Stroop test available from past literature, we relied on a similar study by Chu et al. (2017) for calculating a minimum sample size estimate (η2 = 0.16; converted to Cohen’s d = 0.8729) (Chu et al., 2017). We then used G*Power 3.1.9.2 software (Cunningham & McCrum-Gardner, 2007) to determine the estimated required sample size per group, assuming 80% power (1–β) and α of 0.05, and we found this minimum sample size to be 22 for each group. We added five additional participants per group as a safeguard against a 10% attrition possibility. Thus, we evaluated a total of 54 participants at baseline, and, after two dropouts, 52 participants completed the study. We re-evaluated the participants at the end of the 4-week trainings (see Figure 1). We randomly assigned participants to either group PE (Pilates exercise) or group AE (aerobics exercise). Flow Diagram for Study Participants.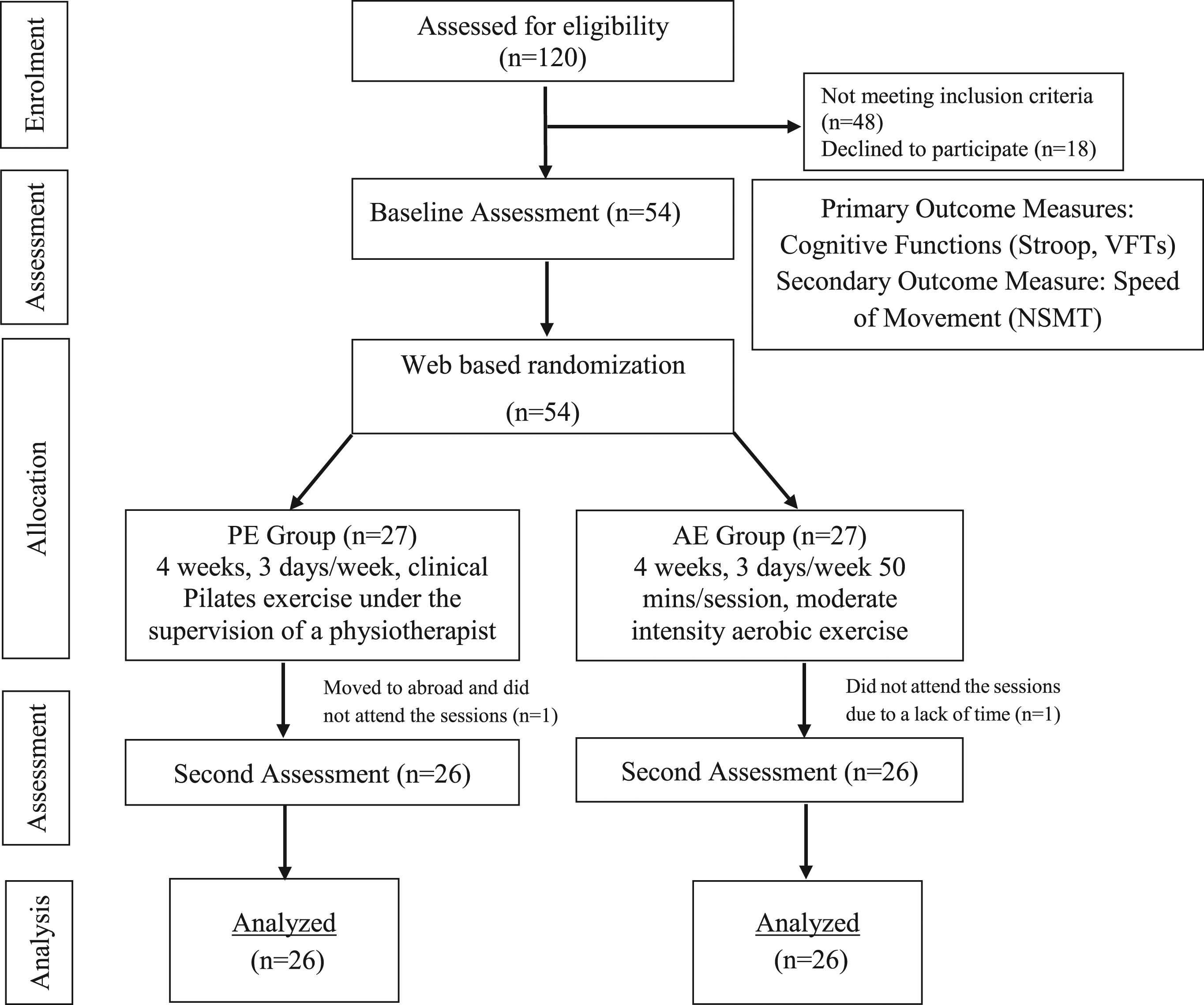
Participants
Volunteer participants were healthy individuals with no diagnosed diseases who were aged between 18 and 25 years. All participants were undergraduate students at a public university in Istanbul who responded to an announcement that PE and AE programs were available free of charge at the university campus. Volunteers were included if they self-reported less than 600 metabolic equivalent (MET) activity minutes/week on the International Physical Activity Questionnaire-Short Form (IPAQ-SF) (IPAQ Group, Online access August 19, 2020). Volunteers were excluded if they had musculoskeletal problems or cardiovascular disorders that limited their exercise capacity, neurological disorders, a diagnosis of any cognitive disease, pregnancy, a body mass index (BMI) over 35, or a Beck Depression Inventory (BDI) score of 17 or above. We also excluded smokers and medication users whose cognition might have been affected by these activities, and we excluded any volunteers with color blindness that might have affected their performance on the Stroop test. We included inactive individuals to detect the improvement of cognitive functions since better initial (pre-exercise) cognitive functions have been reported among the physically active than the physically inactive individuals (Khan & Hillman, 2014). In addition, we included participants with BMI values below 35 and BDI scores below 17 because obesity and depression have been shown to reduce cognitive performance (Dotson et al., 2014; Smith et al., 2011). We asked participants to avoid alcohol use for 24 hours and food or caffeine consumption two hours before the assessments. All participants gave informed written consent before any participation in the experiment. This research protocol was approved by the Clinical Research Ethics Committee of the author’s institution, and it was carried out in accordance with the Helsinki Declaration.
An initial assessment showed that prior to engagement in either AE or PE programs, participants in the two groups had the following descriptive characteristics: (a) age (PE: M = 20.85, SD = 2.11 years; AE: M = 19.88, SD = 0.91 years); (b) gender (18 female and 8 male in each group); (c) educational status (≥9 years in each group); (d) BMI (PE: M = 21.75, SD = 2.68 kg/m2; AE: M = 22.75, SD = 3.62 kg/ m2); (e) IPAQ-SF (PE: M = 446.10, SD = 124.33 MET min/week; AE: M = 369.90, SD = 155.35 MET min/week); and (f) BDI (PE: M = 8.50, SD = 5.04; AE: M = 10.12, SD = 4.56).
Outcome Measurements
All participants were assessed by the same researcher using outcome measurements at baseline (before the first training session) and after four weeks of the training programs. We used a separate form to collect descriptive participant data, and we questioned participants about the side effects of exercises verbally before and after each session (with no side effects reported). As noted above, we determined the participants’ physical activity levels with the IPAQ-SF (IPAQ Group, Online access August 19, 2020), which questioned respondents about the duration and frequency of their moderately intense physical activities, such as walking and sitting, performed for at least 10 minutes once a day over the previous seven days. In the total score calculation, we included data regarding walking, moderate and vigorous activity, but we did not include sitting data.
Regarding cognitive functions, we assessed selective attention with the Stroop test, which has been related to frontal lobe–mediated executive functioning (Lezak et al., 2004). The Stroop test has been reported as a gold standard tool within the field of neuropsychology (MacLeod, 1992), often used for evaluating information processing speed, working memory, inhibitory control, and selective attention. The Stroop test utilizes four stimulus cards and five sub-sections, with the critical part of this test in the fifth section in which there is an interference effect the respondent must master. Other sections are congruous control conditions in which basic levels of reading and color expression are determined. The participant’s initial task in section 1 is to read the black printed color names as fast as possible. In section 2, the participant is to read the names of the colors printed in red, blue, yellow, and green on the second card. In section 3, the participant says the names of the colored circles. In section 4, the participant says the color of the ink in which the following words are printed: “and,” “over,” “hard,” and “when.” In section 5, called “incongruent condition,” the participant’s task is to name the color of the ink (instead of reading) series of color words. Thus, in this condition, the participant must inhibit a tendency to read the color word. This difficulty inhibiting the reading of the colored word (the more automated process) is called the Stroop effect. The total score of the test is obtained by the total time taken to read these sections. The Turkish version of Stroop test was used in the current study (construct validity = 89.8% of total variance; test re-test = Section 1: r = 0.56, Section 2: r = 0.26, Section 3: r = 0.65, Section 4: r = 0.88, Section 5: r = 0.56; Karakas et al., 1999).
We also assessed verbal fluency as an executive control ability that is integrated with attention and related to frontal lobe–mediated executive functioning (Azuma, 2004). Verbal fluency tests (VFTs) have been used for letter (phonemic) and category (semantic) verbal fluency evaluations. The letter fluency test is a reliable test in healthy adults (internal consistency r = 0.83; Tombaugh et al., 1999, test re-test r = 0.82; Harrison et al., 2000). It is also known as the Controlled Oral Word Association Test (COWAT), and it has various versions and linguistic adaptations (Ponichtera-Kasprzykowska & Sobów, 2014; Spreen & Strauss, 1998). We used the Turkish version adapted with the letters K, A, and S in the current study (Oktem, 1994; Tumac, 1997, reliability coefficient: r = 0.90 for the letter K, r = 0.91 for the letter A, r = 0.89 for the letter S; Tumac, 1997, inter-rater reliability coefficient = 0.97; Tuncer, 2011).We asked participants to successively name as many words with each letter as possible in one minute, excluding proper nouns and derived words, starting first with the letter K and then with the letters A and S. Additionally, the category fluency test, in which respondents rapidly name nouns within categories, is often used with categories such as animals, fruits, vegetables, food, and supermarket items (Lezak et al., 2004). One or more categories can be used in the assessment of semantic fluency (Ponichtera-Kasprzykowska et al., 2019). Semantic fluency has been found to have construct validity for examining executive functions in healthy adults (construct validity = 61% of total variance; Aita et al., 2019, test–re-test r = 0.68; Harrison et al., 2000). Normative studies of category fluency have been carried out in various countries (Ponichtera-Kasprzykowska et al., 2019), and category fluency norms were also provided in the Turkish-speaking adult population (inter-rater reliability coefficient = 0.99; Mavis & Tuncer, 2016). In this study, we used the categories of animals, fruits, and supermarket items that have been most studied in prior research, and which have a potential role in human survival and ecological relevance for this age group (Caramazza & Shelton, 1998; Da Silva et al., 2004; Tombaugh et al., 1999). We asked participants to name as many animals, fruits, and supermarket items as possible in one minute for each category. The score for each test was based on the total words named minus any errors and repetitions. During the test, we recorded the participant’s voice with their permission to guarantee our scoring accuracy.
Finally, we used Nelson’s Speed of Movement Test (NSMT; reliability coefficient = 0.75; Johnson & Nelson, 1986) to evaluate speed of movement of the participants’ hand and arm movements, which has also been associated with the attention domain of neurocognitive functions (Smith et al., 2010). Participants performed the NSMT while sitting in a chair and placing each hand on the bar with palms facing each other while keeping the fifth digit of each hand in contact with the bar and 30 cm between them. The therapist then held a ruler at the midpoint of the hands and on the index fingers and, after the “Ready” command, dropped the ruler. The participant stopped the ruler as quickly as possible with a horizontal clapping movement of their hands, without shifting their hands upward or downward. We then measured the distance from the stopped ruler to the drop point. We conducted 20 trials, excluded the five best and the five worst trials, and averaged the remaining ten trials to derive a distance for this fall. We next calculated a reaction time, based on the constant acceleration of free-falling objects using this formula: Reaction Time = √2 x Distance (cm)/Gravity Acceleration (980 cm/sec2) (Johnson & Nelson, 1986). Finally, we calculated speed from this reaction time as follows: “Reaction Speed = 30 cm (Ruler’s length)/Reaction Time.” The numerical magnitude of the value obtained by the formula indicated the speed and final score for the test.
Training
Pilates Group (n = 26)
Before the first PE session, each participant was taught the five key elements (lateral breathing, centering, and placements of ribcage, scapula, head, and neck) of PE. Participants then performed PE under the supervision of an Australian Physiotherapy Pilates Institute–certified physiotherapist for 40–50 minutes three days per week over four weeks. Subgroups consisted of 6–10 individuals whose physical characteristics and suitability for the session schedules were similar. The sessions started with level 1 exercises, which require more support from the musculoskeletal system and less control. Each session consisted of about 10 minutes warm-up, 20–30 minutes mat exercises, and 10 minutes cool down exercises with 8–10 repetitions. Specific PE were “Hundreds,” “One Leg Stretch,” “Shoulder Bridge,” “Double Leg Stretch,” “Roll Up,” “Side Kick,” “One Leg Circle,” “One Leg Kick,” “Swimming,” “Swan Dive,” “Breaststroke Prep 1,” “Arm Opening,” “Spine Twist,” and “Roll Down” moves (see Appendix 1).
Aerobic Exercise Group (n = 26)
There have been prior studies of the effects of exercises with different intensities on cognitive functions (Hwang et al., 2016; Mekari et al., 2015; Susano, 2014; Wohlwend et al., 2017). A systematic review reported that the most effective exercise intensity for cognitive function effects was 50–70% (moderate intensity) of maximal heart rate (HRmax) with 150 minutes per week (Susano, 2014). Accordingly, in this study, participants performed moderate-intensity AE (WHO, 2010) by using an elliptical bike (15 minutes), static bicycle (15 minutes), and treadmill (20 minutes) under the supervision of a physiotherapist for over the length of this training (40–50 minute sessions 3 days per week over 4 weeks). We calculated HRmax with the “220-age” formula.
Data Analysis
We analyzed data using version 24.0 of the IBM Statistical Package for Social Sciences (SPSS). We considered p < 0.05 sufficient for statistical significance. Descriptive statistical analysis results were presented as means (Ms) and standard deviations (SDs). We analyzed data with the Kolmogorov–Smirnov normality test, and we compared differences between demographic characteristics/categorical and continuous variables of groups with the chi-squared and Mann–Whitney U tests, respectively. We analyzed intragroup changes before and after training with the Wilcoxon signed rank test. After the training, changes in the scores were shown in a 95% confidence interval (CI). We compared intragroup pre- and post-exercise changes using the Mann–Whitney U test. We calculated the effect sizes of the changes in the groups with the formula: “Effect size = difference between the means of the measurements/standard deviation of the first measurement.” Impact magnitude was interpreted as 0.2–0.5 “small,” 0.51–0.80 “medium,” and 0.81 and above as “large” (Sullivan & Feinn, 2012). Effect sizes were computed only for significant variables.
Results
Pre- and Post-4-Week Exercise Changes by Exercise Groups for Stroop, Verbal Fluency Test, and Speed of Movement Test Scores.
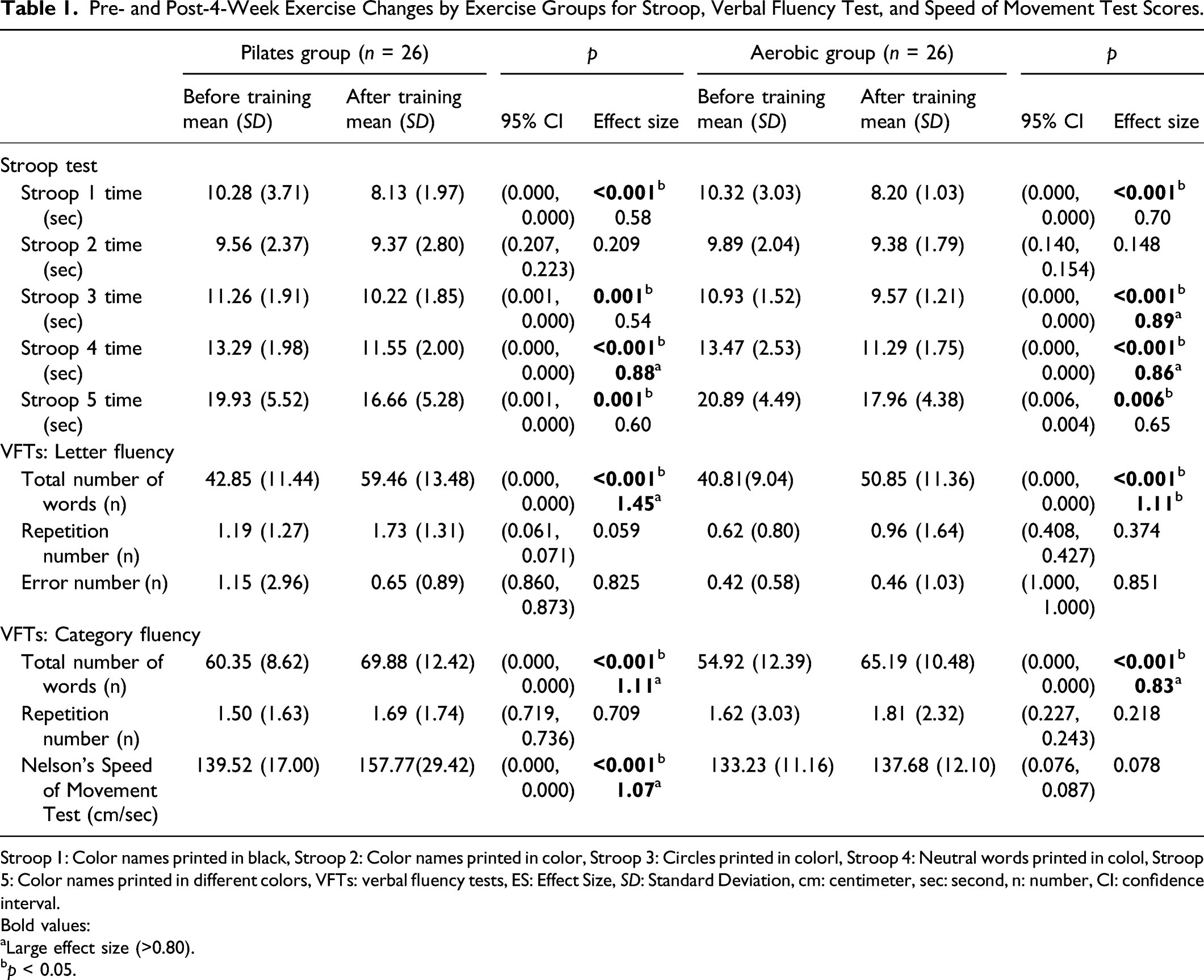
Stroop 1: Color names printed in black, Stroop 2: Color names printed in color, Stroop 3: Circles printed in colorl, Stroop 4: Neutral words printed in colol, Stroop 5: Color names printed in different colors, VFTs: verbal fluency tests, ES: Effect Size, SD: Standard Deviation, cm: centimeter, sec: second, n: number, CI: confidence interval.
Bold values:
aLarge effect size (>0.80).
bp < 0.05.
Comparison of Exercise Group Differences in Pre- and Post-4-Week Exercise Change Scores for All Outcome Measures.
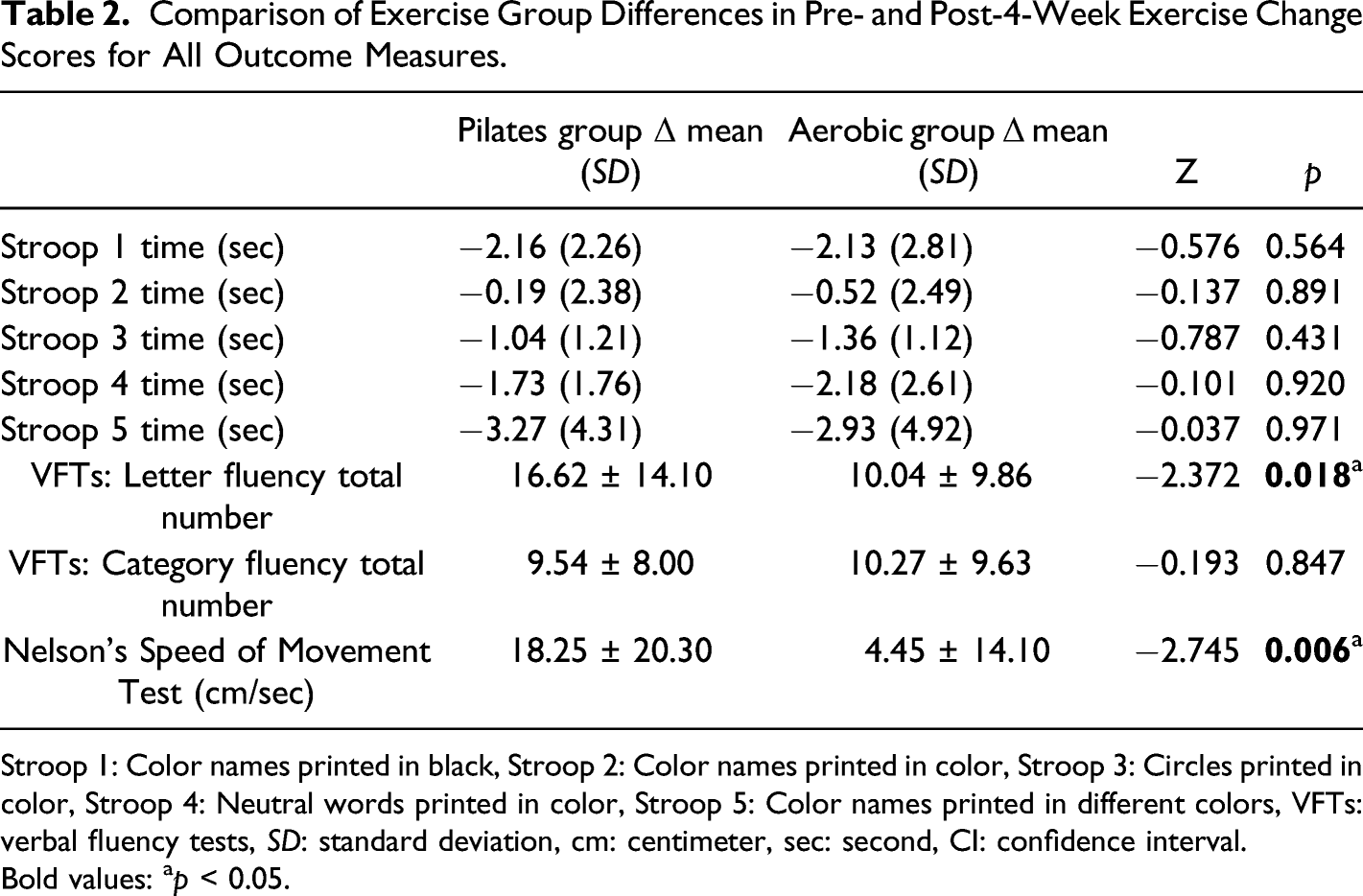
Stroop 1: Color names printed in black, Stroop 2: Color names printed in color, Stroop 3: Circles printed in color, Stroop 4: Neutral words printed in color, Stroop 5: Color names printed in different colors, VFTs: verbal fluency tests, SD: standard deviation, cm: centimeter, sec: second, CI: confidence interval.
Bold values: ap < 0.05.
Discussion
Results from the current study showed that participants who were engaged in PE and AE programs that were each applied for four weeks improved their cognitive functioning through Stroop and verbal fluency scores, with medium to large effect sizes. Speed of movement was increased for participants in the PE group, with a large effect size.
A meta-analysis revealed that exercise duration is an important factor for achieving adaptations and improvements in the musculoskeletal system through exercise (Clark, 2016). However, it has not been shown to be a significant factor for improving executive functions through exercise (Verburgh et al., 2014). In another review, the duration of exercises necessary to achieve a cognitive effect was determined to be short (1 day–16 weeks), medium (24–40 weeks), and long term (52 weeks and more) (Cabral et al., 2019). In the current study, we used a relatively short-term exercise duration of four weeks of training. While the number of repetitions and sessions increase progressively in these exercises, the requirement to engage executive functions such as attention and concentration within the exercises decreases over time, due to motor learning (Huber, 2012).
Past studies seeking to evaluate executive functions have relied upon different Stroop versions and score calculations. One of these versions is the Stroop Color and Word Test containing the following three parts: reading names colored with black ink, reading different color patches, and incongruent colors (Scarpina & Tagini, 2017). In the current study, we used the Stroop form that includes five sections (Karakas et al., 1999). In addition, we calculated the scores of the Stroop sections as reaction times in seconds. According to our results, there was a significant change in pre-exercise and post-exercise scores for Stroop sections 1, 3, 4, and 5, but not for section 2 for both PE and AE participant groups. Section 2 had the lowest internal consistency in the validation (Karakas et al., 1999). The first four sections of the test are generally used for control purposes and to assess attention (Smith et al., 2010). Section 5, which includes an incongruent color–word condition of the Stroop task, is related to inhibitory control called the Stroop effect, and it has been accepted as the most important section of the test.
In this study, we observed improvements on the Stroop after a 4-week exercise training program with inactive young adults. In past literature, Stroop performance has been improved after regular AE (Smith et al., 2010). While there have been many studies based on older adults, there is a paucity of research with young adults. Studies on youth and children have shown that increased physical fitness and regular AE have been associated with better inhibitory control (Ludyga et al., 2019) and improved cognitive flexibility, and working memory (Liu et al., 2020). Others found aerobic training with four weeks duration to be effective in decreasing the reaction times of responses to incongruent Stroop stimuli among children with Developmental Coordination Disorder (Alagesan & Brite Saghaya Rayna, 2020). In addition, a meta-analysis of the effects of AE on executive function determined that there was no difference in results between studies based only on AE and studies based on both aerobic and strengthening exercises (Smith et al., 2010). We also observed Stroop improvements among young adult participants in both AE and PE exercise groups, and, when these two types of exercise groups were compared, there was no significant relative difference favoring either group.
Verbal fluency is a complex skill that involves many cognitive processes, including attention, memory, and executive functions (Azuma, 2004). In a study investigating the effect of a 12-week aerobic training program on elderly participants’ letter and category verbal fluency, there were positive results attributed to increased aerobic capacity (Nocera et al., 2020). In our study, the baseline value on category fluency was consistent with the normative values on this task (Mavis & Tuncer, 2016). Four weeks of both aerobic (AE) and Pilates (PE) training positively affected the letter and category fluency of inactive young adults. There were no statistically significant changes in the number of errors and repetitions. Although the ratio of the total number of repetitions and errors were not reflected in the statistics, we presented in the Results section of this paper that there was a decrease for errors in the letter fluency section in the PE group, and a slight increase for repetitions in the letter and category fluency sections, compared to baseline performance for participants in both exercise groups. We found exercise to be more effective in terms of gains on tests of letter fluency than those of category fluency, and letter fluency has been described as more closely related to frontal lobe brain function than category fluency (Gourovitch et al., 2000). According to the differences between pre- and post-exercise assessments, Pilates training was superior to AE for enhancing letter fluency among our participants. Letter fluency has been said to involve frontal brain functions of working memory, information retrieval, attention allocation, strategic organization, planning, and response inhibition (Azuma, 2004). Due to the nature of Pilates, exercises, the key elements are taught to the participants in the first two sessions. In each following session, a correct application of Pilates principles requires the participant to plan and organize the movement by recalling this initially learned information. There is similar rapid planning associated with the letter fluency test in which respondents must say as many words beginning with a given letter as possible within a short one-minute time frame. Perhaps this task similarity is related to the higher letter fluency scores among PE participants in our study.
Psychomotor function is defined as the ability to demonstrate hand–eye coordination, balance, reaction time, and speed performed through the integration of physical, cognitive, and attention functions working together (Bhupinder Singh, 2016; Smith et al., 2010). Tasks associated with psychomotor functions require higher-level cognitive processes, related to changes in information processing, and cognitive tasks that demand attention and managing visual and spatial information (Zach & Shalom, 2016). In this study, we observed a statistically significant increase in speed of movement with a large ES for participants in the PE group (but not for participants in the AE group) when comparing their pre- and post-training test performances. Mohammadpour et al. (2012) had three groups of university students engage in either physical, mental, or combined mental–physical exercises. At the end of four training sessions, NSMT values were higher for participants in the combined exercise group compared to the other two groups; the authors concluded that both real and mental movements were important for reaction speed. A study of Gentili et al. (2006) proposed that physical exercise and related mental exercise share the similar neurocognitive networks which are useful for the sensorimotor and cognitive processes. Therefore, combining both mental and physical exercises may increase reaction speed/time more than physical tasks would alone, as mental–physical exercise involves and affects a wider range of cognitive functioning, including such specific cognitive functioning as learning, memory, and attention (Mohammadpour et al., 2012). In this context, our finding of improved speed among PE, but not AE, participants may be attributed to the greater role of mental focusing and even mental imagery in PE versus AE. Malhotra et al. (2015) reported significant improved reaction time to traffic light signals in young adults after they completed one session of mild to moderate AE. Researchers evaluated participants before and immediately after the exercise session. They attributed the cognitive effect to increased heart rate and cortical blood flow, which immediately occurs due to the “acute effect” of exercise. Yet, we were unable to produce a similar effect from four weeks of moderate instrumental AE. Assessments were not made immediately after exercise, as the acute effect was not targeted. We evaluated the participants at baseline and after the 4-week training period to investigate the “short-term effect” of exercise. AE, which does not require significant mental focus or attention, was performed at a moderate intensity in our study with a treadmill, elliptical bicycle, and bicycle ergometer. These exercises require lower limb motor performance, but the evaluation method used involves the motor performance of the upper extremities. For these several reasons, we may not have observed the positive cognitive benefits among participants in AE compared to participants in psychomotor functioning that included both physical and mental processes.
Limitations and Directions for Further Research
The current study has several limitations, including the absence of follow-up testing which would have provided important information regarding whether any PE- or AE-related improvements are maintained over time. Additionally, there was no control group. The presence of a control group who received no exercise training would have helped determine whether changes were due to exercise, testing practice effects, or some uncontrolled variable. Finally, the absence of any physiological brain measures (e.g., functional magnetic resonance imaging and/or other physiological brain–related markers such as brain-derived neurotrophic factor (BDNF) or insulin-like growth factor-1 (IGF-1)) means that we can only speculate regarding underlying brain mechanisms.
We evaluated participants with validated, easy-to-apply, and low-cost neuropsychological screening tests such as Stroop, verbal fluency tests (VFTs), and we used the NSMT to assess motor speed, consistent with prior investigators in this literature (Smith et al., 2010). A question arises whether our findings might be due to a practice effect on these neuropsychological tests rather than exercise benefits. In a meta-analysis by Scharfen et al. (2018), the learning effect on the Stroop and VFTs decreased as the time between testing and re-testing increased. Therefore, we believe that a practice effect was highly unlikely to occur within the 30-day re-testing interval in our study. It would be ideal to use both objective assessments and imaging methods in future studies to provide more reliable and accurate indications of brain-based changes from exercise engagement.
Conclusion
To the best of our knowledge, this was the first randomized controlled trial to (a) investigate the effect of PE on cognitive functions in inactive young adults and (b) compare those PE effects to AE effects. In the short term, both PE and AE improved selective attention, verbal fluency, and executive control. However, contrary to our expectation, PE, which includes mental focusing, was not superior to AE in its effects on cognitive functioning. PE seemed to be effective in increasing speed of movement associated with attention, and letter fluency associated with the executive function. Thus, PE can be used to enhance movement speed for athletes whose reaction speed is important, especially with the upper limbs, and PE can improve the attention that is important for academic success and activities of daily life.
Highlights
(1) Cognitive functions can be improved with short-term exercise training in inactive young adults. (2) Both clinical Pilates and aerobic exercises affect the selective attention, verbal fluency, and executive control ability. (3) Clinical Pilates exercises improve the speed of movement which is associated with attention.
Supplemental Material
sj-pdf-1-pms-10.1177_00315125211051178 – Supplemental Material for Comparing the Cognitive Functioning Effects of Aerobic and Pilates Exercises for Inactive Young Adults: A Randomized Controlled Trial
Supplemental Material, sj-pdf-1-pms-10.1177_00315125211051178 for Comparing the Cognitive Functioning Effects of Aerobic and Pilates Exercises for Inactive Young Adults: A Randomized Controlled Trial by Begum Kara Kaya and Ayse Zengin Alpozgen in Perceptual and Motor Skills
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Clinical Trial
Number: NCT03491566.
Data Availability Statement
The data that support the findings of this study are available upon request from the corresponding author. The data are not publicly available due to the restriction of the Ethics Committee, because it’s containing information that could compromise the privacy of research participants.
Institutional Review Board Approval
Clinical Research Ethics Committee of Istanbul University Faculty of Medicine, approval number 02 (26.01.2018 ).
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.