
Abstract
Keywords
Introduction
The preschool age is a crucial developmental period marking the transition to childhood, during which motor development significantly influences overall growth (Williams & Monsma, 2017). This process allows children to develop their coordination, balance, and agility, which helps them better control their bodies and interact more effectively with their environment (Adolph & Hoch, 2020). This development plays a central role in influencing not only physical growth but also cognitive and psychosocial aspects (Peyre, 2018). Furthermore, it is closely linked to socialization, which begins with early physical activities (Brian et al., 2020). A recent study has shown that advanced motor skills and a high level of physical activity promote broader social networks (Herrmann et al., 2021). Cognitively, mastering motor skills also contributes to the development of executive functions (Diamond & Lee, 2011) and predicts later academic progress (Cameron et al., 2016; Pitchford et al., 2016). Additionally, the development of fine motor skills is essential for preparing the child for school, particularly in tasks related to pre-writing (Nikitina & Bragina, 2024).
Motor skills progress rapidly during the preschool period and develop gradually through practice, alongside the child’s maturation (Kuzik et al., 2020), with the acquisition of these skills being facilitated from the age of 4 (Best & Miller, 2010). The school environment, particularly preschool where children spend a large part of their day, provides an ideal setting for implementing specific programs aimed at promoting their motor development and mental health (Matvienko & Ahrabi-Fard, 2010). Traditional physical and educational approaches, which emphasize the repetition of movements, play a key role in motor learning (Zeng et al., 2017). However, motor imagery (MI) has emerged as a complementary method, often more effective in improving motor skills (Guilbert & Fernandez, 2023). According to Jeannerod’s (2001) mental simulation approach, MI corresponds to a simulated motor action that engages the same neural structures involved in the action, but is inhibited before its execution. For Jeannerod, motor representations are internal models of the action’s goal. The theory of internal models of movement posits that the nervous system anticipates the sensory consequences of an action through an efference copy, even without physical execution (Lebon et al., 2013). Thus, MI can be defined as the ability to generate internal models of motor control (Puyjarinet, 2019). The development of MI abilities in children follows a well-defined trajectory. Guilbert et al. (2013) found that MI abilities begin to develop between ages 5 and 7 and continue to improve into adolescence. Furthermore, Butson et al. (2014) demonstrated that children aged 5 to 6 can already imagine movements accurately and perform mental rotation tasks. Thus, MI plays a crucial role in promoting motor learning and consolidation in children.
However, the effect of MI training on the improvement of motor skills has not yet been thoroughly studied in 5-year-old preschool children. Therefore, we based our analysis on studies conducted with the nearest age group available in the literature. Numerous recent studies have highlighted the positive impact of MI training on children’s motor skills. A meta-analysis conducted by Frank et al. (2024) revealed that MI has a positive effect on overall motor skills, with notable improvements in activities such as running, jumping, and throwing in children aged 6 to 18 years. In addition, other studies have demonstrated that children who practice MI show enhanced performance in fine motor activities, such as drawing or handling small objects (Frank et al., 2024; Guilbert & Fernandez, 2023). Furthermore, it has been shown that MI facilitates the retention and transfer of closed motor skills in primary school children (Taktek et al., 2008). Moreover, the combination of MI and balance training proves to be particularly effective in improving balance (Kulkarni & Rawal, 2022; Turan & Dişçeken, 2019).
Previous studies have shown that MI training improves motor skills in children. However, it is essential to consider individual differences, particularly those related to age and developmental stage. These factors significantly influence the effectiveness of imagery interventions, especially in the motor domain. Despite this, the literature on the benefits of MI in preschool settings remains limited. Within this population, 5-year-old children represent a critical period of development, during which MI abilities are emerging while motor patterns remain particularly malleable (Spruijt et al., 2015). Intervening at this early stage allows researchers and practitioners to act before the stabilization of these patterns, thereby maximizing the impact on both motor and cognitive maturation. Furthermore, targeting children before their entry into primary school offers a valuable opportunity to effectively guide educational and preventive practices. In this context, MI may serve as an effective complement to physical exercise, creating a synergy that fosters faster and more efficient motor skill development. Therefore, this study aims to assess, for the first time in preschool children aged 5, the impact of guided MI training on motor skills through a randomized controlled trial.
Method
Participants
Baseline Child Demographics (N = 46)
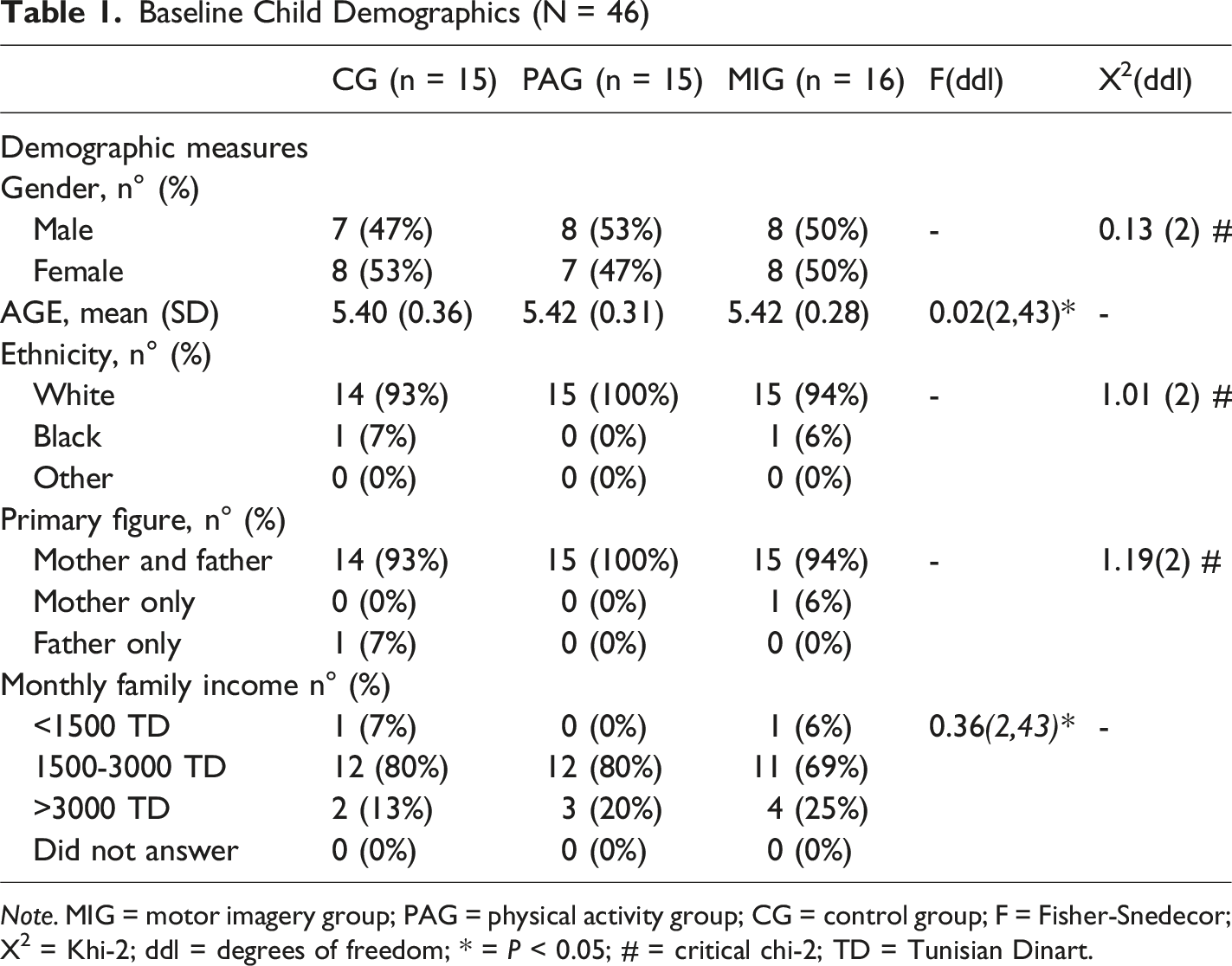
Note. MIG = motor imagery group; PAG = physical activity group; CG = control group; F = Fisher-Snedecor; X2 = Khi-2; ddl = degrees of freedom; * = P < 0.05; # = critical chi-2; TD = Tunisian Dinart.
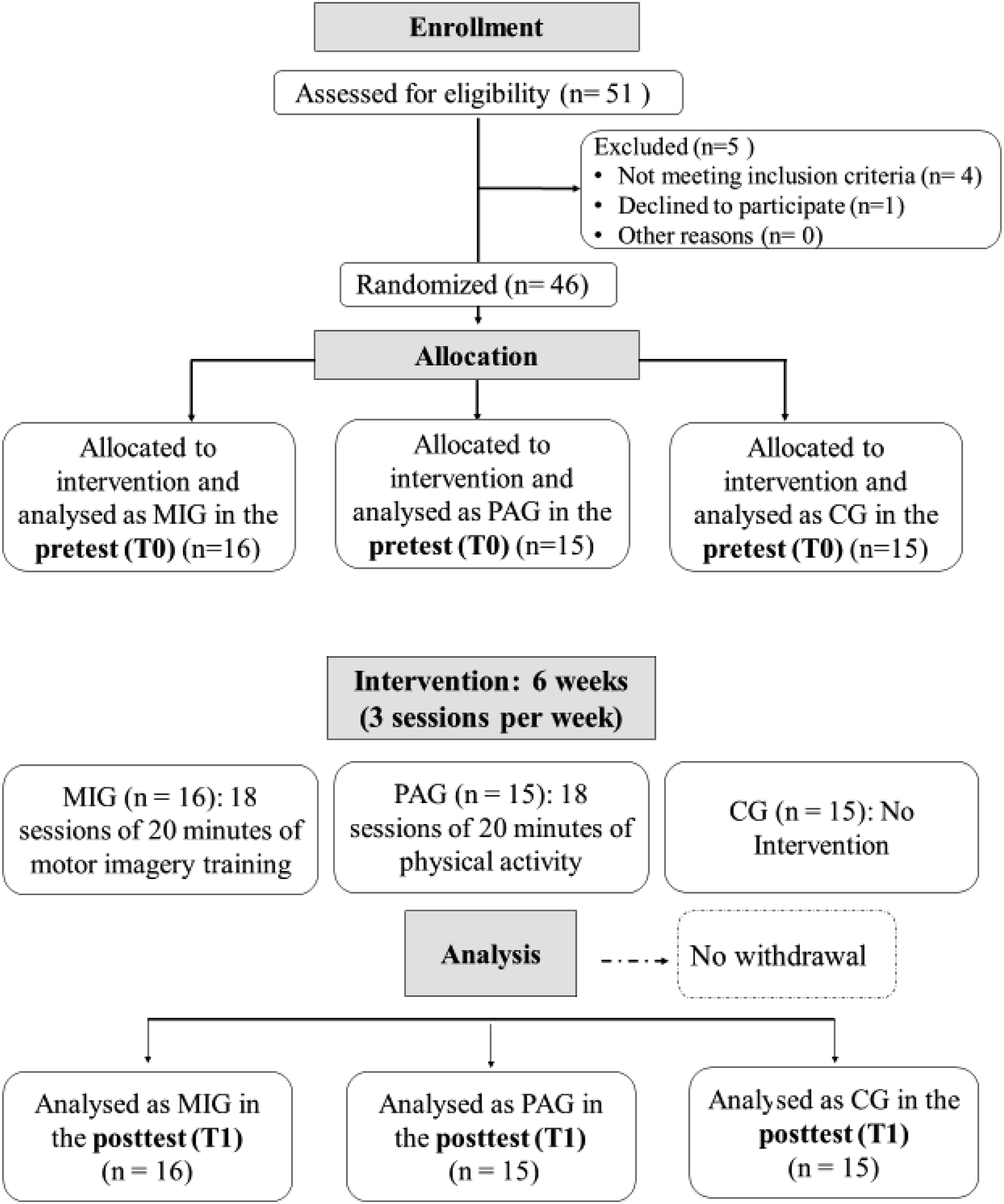
CONSORT Flow Diagram of the Study Protocol and Participant Flow.
Ethical Considerations
Written informed consent was obtained from the parents or legal guardians of all participating children. The preschool administration authorized the study to be conducted on its premises. All procedures were carried out primarily within the preschool environment, ensuring an appropriate, secure, and ethically supervised setting for the children. Participation was voluntary, and children could withdraw at any time without consequence. All procedures were conducted in accordance with the World Medical Association’s Code of Ethics for Human Experimentation and the Helsinki Declaration (World Medical Association, 2013). The experimental protocol was pre-approved by the ethical review board of the institute (Figure 2). Overview of the Study Protocols With Pre-and Post-tests.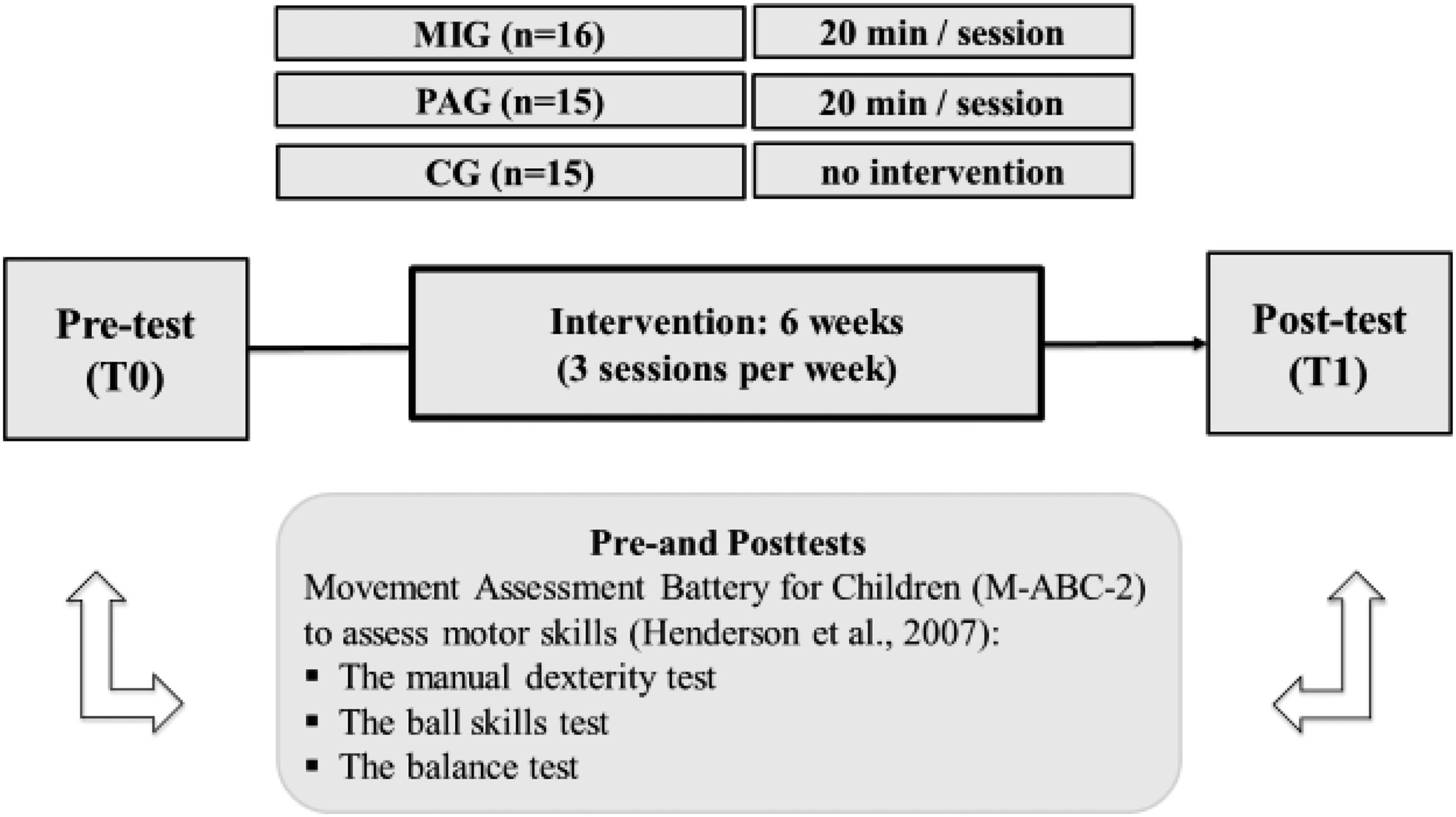
Determining Sample Size, Randomization and Allocation Concealment
We estimated the required sample size through a statistical power analysis using G*Power software (Faul et al., 2007), based on an alpha level (α) of 0.05, a statistical power (1-β) of 0.80, and an effect size of 0.25. This analysis indicated that a total of 42 participants would be required to achieve sufficient statistical power. Following recent recommendations, sample size estimation should be grounded in the smallest effect size of interest (SESOI) to ensure adequate power and to avoid relying on potentially inflated estimates from underpowered studies (Lakens, 2022).
To prevent selection bias and conceal participant group allocation, we employed a centralized randomization process. Participants were assigned to one of three groups based on a computer-generated list of random numbers, with block randomization ensuring an equal distribution across groups. Investigators were blinded to the group assignments, facilitating a double-blind, randomized controlled trial with baseline and post-intervention scores compared between groups.
Research Design
In the present study, we examined the effects of a 6-week MI training program in 5-year-old children, using a three-arm randomized controlled intervention study design. Participants were randomly assigned to three groups: (a) a MI training group (MIG, n = 16), which performed 3 MI training sessions of 20 minutes per week for 6 weeks; (b) a physical activity group (PAG, n = 15), which engaged in physical activity (6 weeks with 3 sessions of 20 minutes per week); and (c) a control group (CG, n = 15), which was more passive and did not participate in structured physical activity, instead engaging in self-chosen regular activities, such as free play during preschool hours. Activities for all three groups were conducted simultaneously at 10 a.m. To minimize potential confounding factors, children who participated in extracurricular physical or cognitive activities outside of preschool were excluded. Throughout the six-week intervention, all groups engaged exclusively in activities offered within the preschool setting, under regular school conditions. All participants completed the assessment measures at a similar time of day on two occasions: (a) at T0, before the 6-week MI, PP, or passive control condition; and (b) at T1, after the final scheduled session of MI or PP. There were two researchers in this study: one supervised the intervention process, while the other conducted the test sessions without knowing the group assignments to maintain blinding and avoid any assessment bias. At baseline (T0), the mental rotation test was used to assess MI ability, which helped select the children participating in the study. They were required to achieve at least 60% correct responses on this test to be included. This 60% cut-off, based on Funk et al. (2005), reflects a statistically significant mastery of mental imagery tasks in children around five years old, a population comparable to ours. At this age, MI abilities are still emerging and show considerable variability; thus, this threshold ensures that only participants capable of effectively engaging these processes are included (Spruijt et al., 2015). Furthermore, this criterion enhances the internal validity of the study by excluding children for whom the task would be too challenging, thereby avoiding bias related to insufficient abilities. The hand rotation task, a commonly used method for assessing MI, is a computerized task in which images of hands (left and right) are presented in different views and rotation angles. This task includes a total of 48 stimuli, consisting of 16 stimuli repeated three times. Participants must imagine their own hand moving towards the orientation presented in the stimulus in order to determine the laterality of the hand (Funk et al., 2005).
At T0 and T1, participants completed the eight subtests of the Movement Assessment Battery for Children (M-ABC-2) (Henderson et al., 2007) to assess their motor skills, including manual dexterity, ball skills, and balance.
Intervention
The MI intervention was conducted over a period of six weeks, with three 20-min sessions per week, for a total of 18 sessions. This frequency and duration were based, firstly, on the study by Smith et al. (2007), which examined the effects of MI training on improving a gymnastic movement in 7-year-old gymnasts, and secondly, on developmental considerations specific to preschool-aged children. Indeed, at this age, attention capacity is still limited and working memory capacity remains immature (López et al., 2005). According to the cognitive load theory, it is essential to adjust session length and frequency to avoid mental overload that could hinder learning (Gkintoni et al., 2025). Therefore, a protocol balancing stimulation and recovery optimizes intervention effectiveness while respecting the developmental characteristics of this age group. To structure these sessions, we adopted the protocol developed by Puyjarinet (2019), a reference for psychomotor therapists in the application of MI. This protocol is based on an alternation between the MI of motor tasks and their physical execution, ensuring a progressive reinforcement of motor skills. To date, no study has systematically implemented all six components of this protocol in preschool children, particularly around the age of five, as prior research has mainly focused on older children (from 7 years old). This gap underscores the originality and relevance of the present study, which evaluates the feasibility and effectiveness of a fully structured protocol. Each session followed the complete protocol to optimize the effects of MI on children’s motor development and to provide a robust foundation for future research tailored to developmental capacities.
Motor Imagery Guided Session Outline
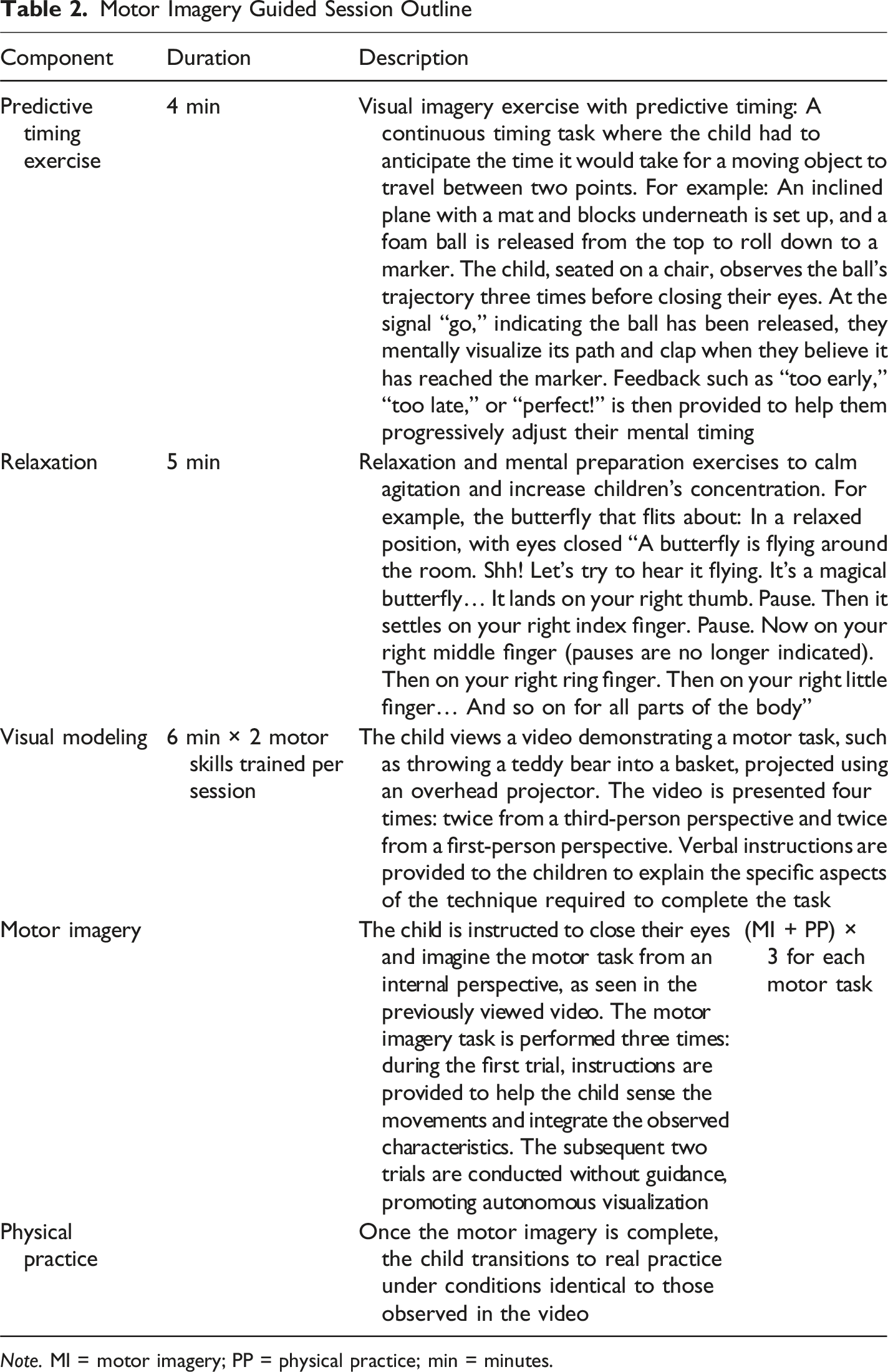
Note. MI = motor imagery; PP = physical practice; min = minutes.
The involvement of participants in our MI intervention was assessed through attendance, active engagement during the sessions, and self-reported evaluations. At the end of each session, participants rated the ease of visualizing and feeling the images on a 7-point Likert scale, allowing us to measure their specific imagery ability. The absence of dropouts throughout the intervention indicates a high level of involvement and motivation, reinforcing the validity of the protocol.
Participants in the physical activity group (PAG) completed 3 weekly sessions of 20 minutes each over 6 weeks. This involved the actual performance of the same motor tasks practiced in the MI group but without any instructions to imagine the movements. The periods corresponding to imagery time in the MI group were replaced with rest periods for the physical activity group to ensure identical session durations across groups. This protocol was designed to control for placebo effects and isolate the specific impact of MI, while preserving the potential effects of physical activity alone.
Participants randomized to the passive group (CG) did not participate in a systematically guided activity. Instead, they engaged in other typical preschool activities, such as free play and coloring. This group was included to control for potential confounding effects related to the natural maturation of motor skills and typical developmental progression in children in the absence of any targeted intervention.
Assessment Measures
Movement Assessment Battery for Children (M-ABC-2)
The M-ABC-2 (Henderson et al., 2007) is a standardized and normative test designed to assess fine motor skills (manual dexterity) and gross motor skills (static and dynamic balance, ball skills) in children aged 3 to 16 years. It includes three tests for each of the three age bands: 3-6 years, 7-10 years, and 11-16 years. In this study, we used the 3-6 years’ age band. The total administration time for the M-ABC-2 ranges from 20 to 40 minutes.
Manual Dexterity Tests
This test assesses the child’s ability to handle small objects with precision and to carry out fine motor tasks. The reliability of this subscale is considered moderate, with a coefficient of 0.59 (Najafabadi et al., 2022). It includes three tasks:
Unimanual Speed/Precision Task: In this task, the child was required to insert 12 tokens into a slot in a piggy bank while holding the piggy bank with one hand and performing the task with the other. Two trials were conducted for each hand, and the best performance was recorded (Henderson et al., 2007). This test demonstrated good reliability, with a coefficient of 0.80 (Najafabadi et al., 2022).
Bimanual Coordination Task: In this task, the child was required to thread 12 cubes onto a lace using both hands in a coordinated manner. Two trials were timed, and the best performance was recorded (Henderson et al., 2007). This test showed moderate reliability, with a coefficient of 0.68 (Najafabadi et al., 2022).
Unimanual Visuomotor Precision Task: In this task, the child was asked to trace a continuous line with their preferred hand without crossing the edges of the path. The score was based on the number of errors (Henderson et al., 2007). This test exhibited good reliability, with a coefficient of 0.80 (Najafabadi et al., 2022).
Ball Skills Tests
This test assesses gross motor coordination through tasks involving an object similar to a ball and demonstrates good reliability, with a coefficient of 0.79 (Najafabadi et al., 2022). It includes two tasks:
Catching Task. The child was required to catch a weighted bag thrown by the evaluator from a distance of 1.8 meters. The score was based on the number of successful catches out of 10 attempts (Henderson et al., 2007). This test demonstrated good reliability, with a coefficient of 0.78 (Najafabadi et al., 2022).
Throwing Task. The child was required to throw a weighted bag toward a target located 1.8 meters away. The score corresponded to the number of successful throws out of 10 attempts (Henderson et al., 2007). This test exhibited moderate reliability, with a coefficient of 0.70 (Najafabadi et al., 2022).
Balance Tests
This subscale assesses the child’s static and dynamic balance and demonstrates excellent reliability, with an intraclass correlation coefficient of 0.91 (Najafabadi et al., 2022). Three tasks are included:
Static Balance Task. The child was required to stand on one leg for a maximum of 30 seconds. The score corresponded to the time elapsed before losing balance (Henderson et al., 2007). This test has excellent reliability, with a coefficient of 0.89 (Najafabadi et al., 2022).
Dynamic Balance Task – Slow Movements. The child had to walk slowly along a straight line of 4.5 meters while keeping their heels raised. The score was based on the number of correct steps taken (Henderson et al., 2007). This test has good reliability, with a coefficient of 0.83 (Najafabadi et al., 2022).
Dynamic Balance Task – Fast Movements. The child had to perform five consecutive jumps on mats to reach a target. The score depended on the number of successful jumps performed without losing balance (Henderson et al., 2007). This test has moderate reliability, with a coefficient of 0.74 (Najafabadi et al., 2022).
The subtest scores were summed to obtain specific scores for manual dexterity, ball skills, and balance. These scores were then combined to calculate the total M-ABC-2 score, providing a comprehensive measure of general motor skills. The Raw scores were transformed into standard scores using age-appropriate normative tables. The M-ABC-2 demonstrates excellent inter-rater and test-retest reliability (>0.89), high internal consistency (Cronbach’s α = 0.83), and moderate to good validity (Najafabadi et al., 2022; Wuang et al., 2012).
Statistical Analysis
All statistical analyses were conducted using R software (version 4.4.3). Data are presented in tables as means ± standard deviations (SD) and in figures as boxplots showing medians (Q2), interquartile ranges (Q1–Q3), and extreme values. The normality of distributions was assessed using the Shapiro–Wilk test and quantile–quantile (Q–Q) plots.
For variables with a normal distribution (Ball Skills), a two-way mixed ANOVA (Group × Intervention) was performed using the rstatix package. Post hoc pairwise comparisons were adjusted using the Bonferroni correction to control for Type I error inflation. Effect sizes were reported as partial eta-squared (ηp2) for ANOVA effects and Cohen’s d for pairwise contrasts. Interpretation thresholds were as follows: ηp2 ≥ 0.14 (large), 0.06–0.13 (medium), and <0.06 (small); d ≥ 0.80 (large), 0.50–0.79 (medium), and 0.20–0.49 (small). For variables violating the normality assumption (Manual Dexterity, Balance, and Total M-ABC-2 score), a two-way mixed design was analyzed using the Aligned Rank Transform (ART) procedure, implemented via the ARTool package, to examine main effects and interactions. Bonferroni-adjusted post hoc tests were applied to significant effects, with Cohen’s d calculated for effect size estimation.
Results of Statistical Tests for M-ABC-2 Subtests and Total Score (Means ± Standard Deviations) in the Control Group (CG), Physical Activity Group (PAG), and Motor Imagery Group (MIG) Before (T0) and After (T1) the Intervention
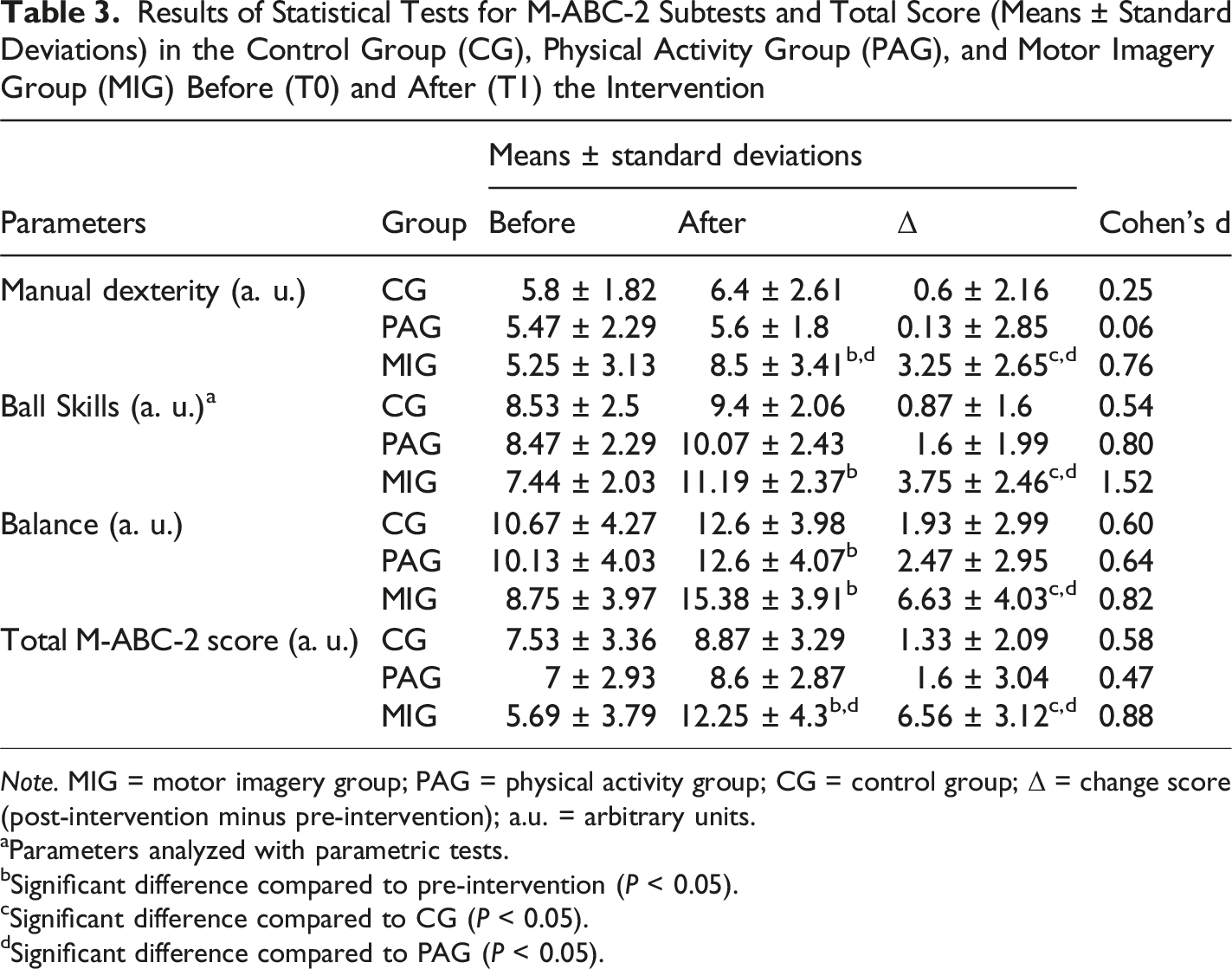
Note. MIG = motor imagery group; PAG = physical activity group; CG = control group; Δ = change score (post-intervention minus pre-intervention); a.u. = arbitrary units.
aParameters analyzed with parametric tests.
bSignificant difference compared to pre-intervention (P < 0.05).
cSignificant difference compared to CG (P < 0.05).
dSignificant difference compared to PAG (P < 0.05).
Results
Manual Dexterity
The ART analysis revealed a significant main effect of Intervention (F(1, 43) = 17.18, P < 0.001, ηp2 = 0.29), reflecting strong post-intervention gains. A Group × Intervention interaction (F(2, 43) = 6.65, P = 0.003, ηp2 = 0.24) indicated variability in responsiveness across groups, though no baseline differences were observed (Group: F(2, 43) = 1.11, P = 0.339, ηp2 = 0.05). Bonferroni-corrected post hoc tests confirmed baseline homogeneity (P > 0.05) and identified the MIG as the sole group with significant within-group improvement (P = 0.002). Furthermore, progress (Δ) comparisons demonstrated superior gains for the MIG over both the CG (P = 0.044) and the PAG (P = 0.010), with this improvement representing a large effect size (d = 0.76) and thus reflecting a developmentally meaningful enhancement in manual dexterity (Figure 3). Percentage Change (Δ%) in Manual Dexterity for the Three Experimental Groups.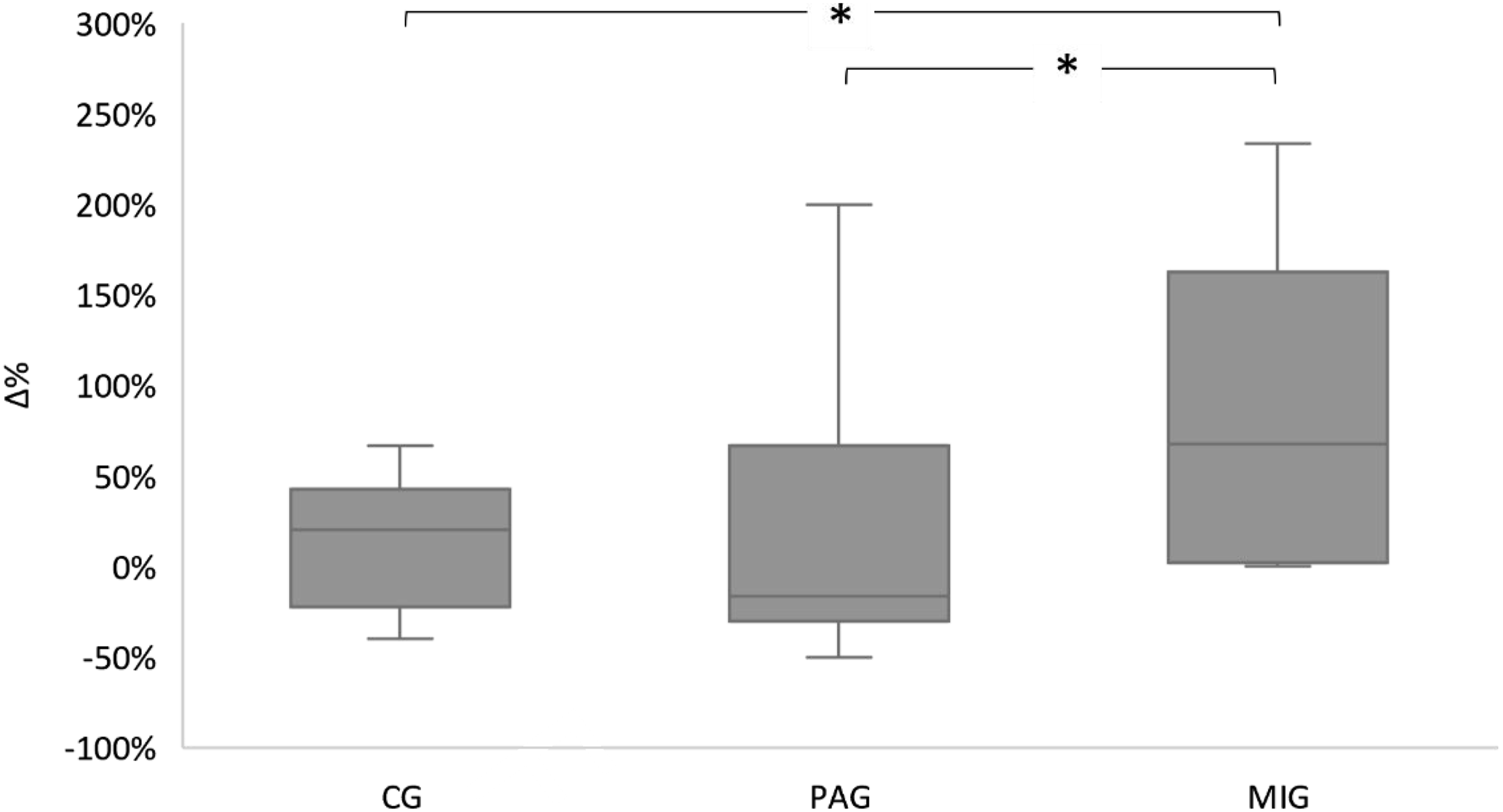
Ball Skills
A two-way mixed ANOVA showed a large main effect of Intervention (F(1, 43) = 46.54, P < 0.001, ηp2 = 0.52), with significant Group × Intervention interaction (F(2, 43) = 8.27, P < 0.001, ηp2 = 0.28), underscoring divergent trajectories among groups. Baseline equivalence was confirmed (Group: F(2, 43) = 0.13, P = 0.88, ηp2 = 0.006). Post hoc analyses revealed that only the MIG exhibited significant pre-post improvement (P < 0.001), alongside greater progress (Δ) relative to the CG (P = 0.001) and PAG (P = 0.017), with this progress representing a very large effect size (d = 1.52) and thus indicating a highly meaningful advancement in ball skills (Figure 4). Percentage Change (Δ%) in Ball Skills for the Three Experimental Groups.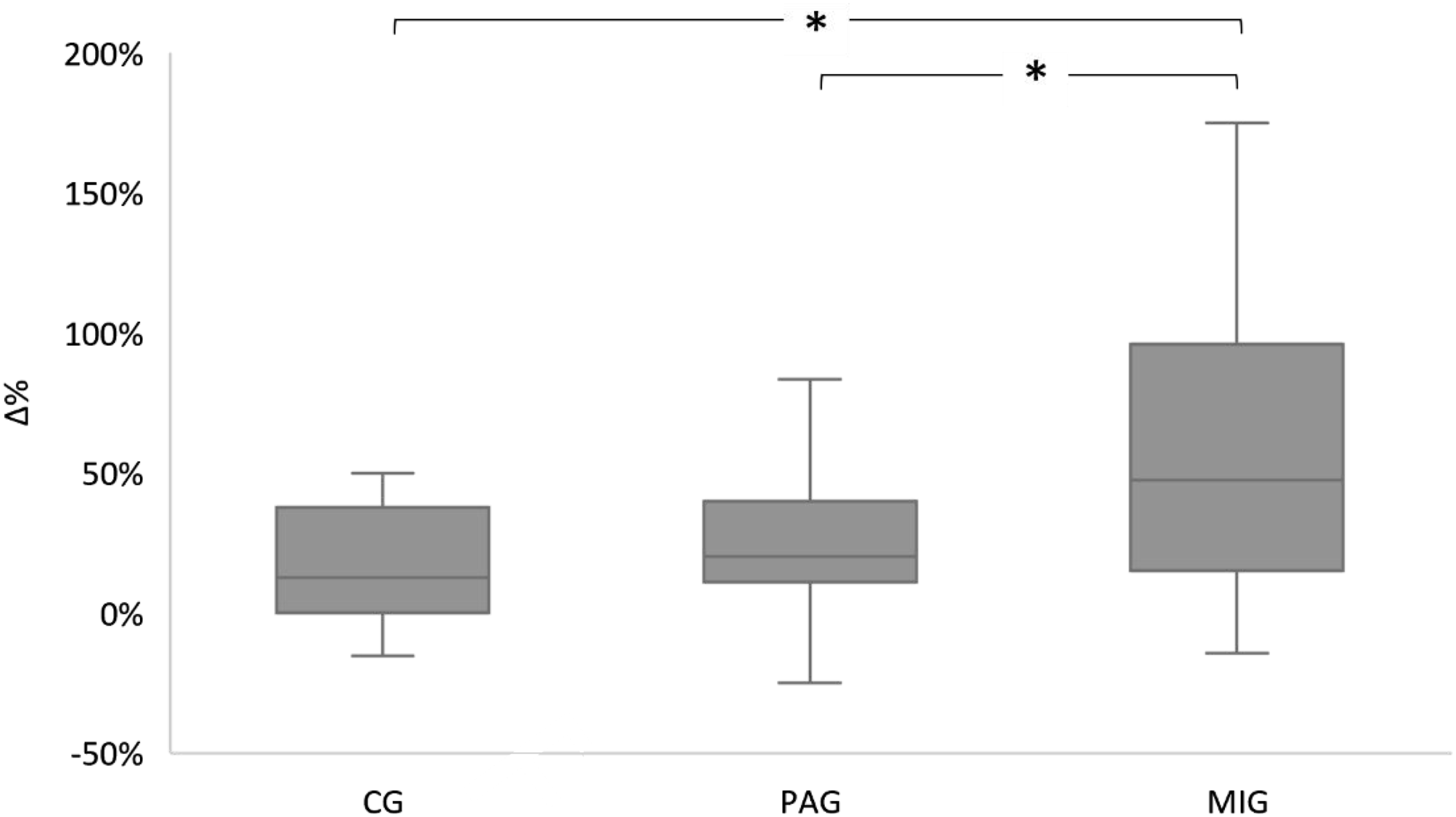
Balance
The ART analysis identified a substantial main effect of Intervention (F(1, 43) = 55.41, P < 0.001, ηp2 = 0.56) and a significant Group × Intervention interaction (F(2, 43) = 8.96, P < 0.001, ηp2 = 0.29), with no baseline group differences (Group: F(2, 43) = 0.17, P = 0.844, ηp2 = 0.008). Post hoc comparisons highlighted the MIG’s marked pre-post improvement (P < 0.001), surpassing both the CG (P = 0.003) and PAG (P = 0.026) in progress (Δ), while the PAG showed only marginal gains (P = 0.013), with this improvement corresponding to a large effect size (d = 0.82) and reflecting a substantial and developmentally significant enhancement of balance (Figure 5). Percentage Change (Δ%) in Balance for the Three Experimental Groups.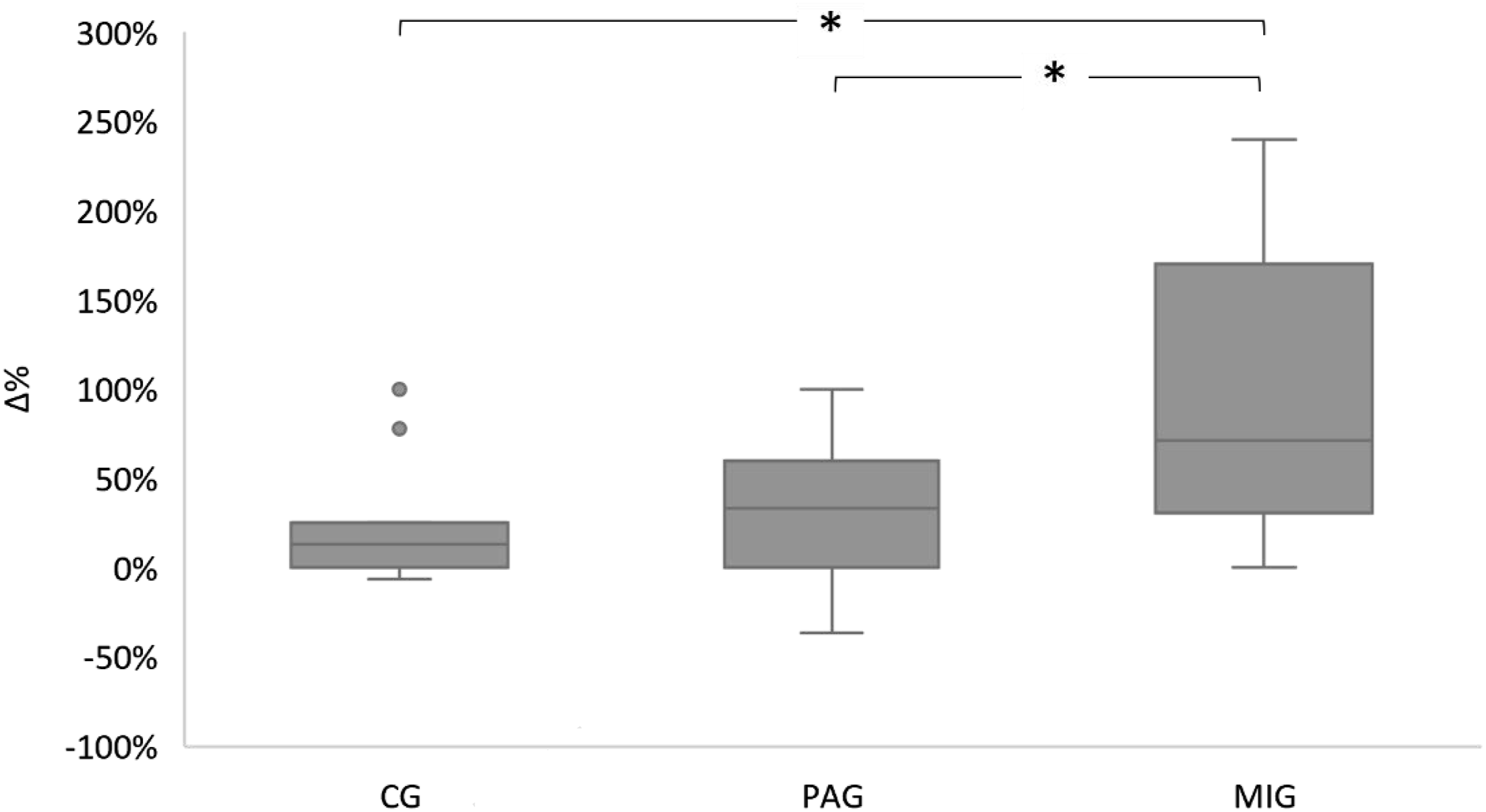
Total M-ABC-2 Score
The ART analysis demonstrated robust main effects of Intervention (F(1, 43) = 61.61, P < 0.001, ηp2 = 0.59) and a pronounced Group × Intervention interaction (F(2, 43) = 15.4, P < 0.001, ηp2 = 0.42), despite baseline equivalence (Group: F(2, 43) = 0.52, P = 0.596, ηp2 = 0.02). Bonferroni-adjusted analyses confirmed the MIG’s exceptional responsiveness, with significant pre-post gains (P < 0.001) and progress (Δ) exceeding both the CG and PAG (P < 0.001) for both), with this change reflecting a large effect size (d = 0.88) and thus underscoring a developmentally meaningful global enhancement in motor skills (Figure 6). Percentage Change (Δ%) in Total M-ABC-2 Score for the Three Experimental Groups.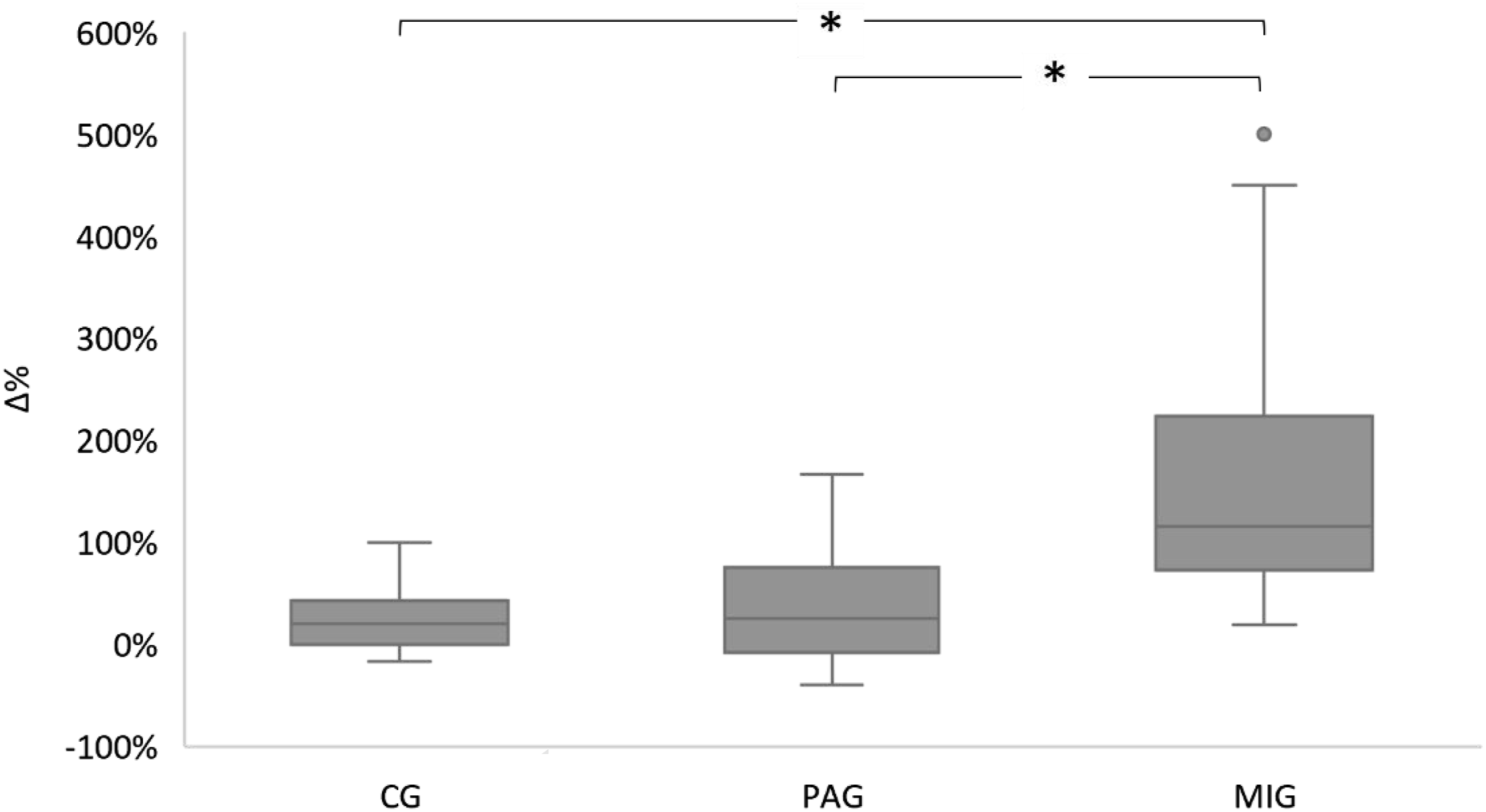
Analysis of M-ABC-2 Score Categories
McNemar–Bowker tests indicated no significant effect of the intervention on the distribution of M-ABC-2 categories within any group (P > 0.05). Similarly, Fisher’s exact tests comparing category distributions between groups at the pre- and post-intervention assessments revealed no significant differences (P > 0.05). In contrast, analysis of the binary variable “Improvement” (defined as improvement versus no improvement/regression) showed a statistically significant association with group membership (Fisher’s exact test, P = 0.006). The improvement rate was substantially higher in the MIG (100%) than in both the CG (60%) and the PAG (60%). Post hoc pairwise comparisons with Bonferroni adjustment demonstrated that the MIG achieved a significantly higher improvement rate than both the CG (P = 0.006) and the PAG (P = 0.006). No significant difference was found between the CG and PAG (P > 0.99).
Discussion
In our study, the aim was to evaluate the effect of MI training on motor skills such as manual dexterity, ball skills, and balance in preschool children, compared to a physical activity control condition and a passive condition. The main findings reveal that the 18 MI sessions led to a significant improvement in motor skills within the experimental group. These results are consistent with those of the study by Smith et al. (2007). Their study methodologically overlaps with ours, as it examines the effect of a six-week MI training program, consisting of three sessions per week, on improving motor performance in gymnastics in 7-year-old children. This methodological and result convergence strengthens the robustness and validity of our conclusions. However, it is important to recognize that the effect of MI training on motor skill development has not been extensively investigated in preschool children. In light of this limitation in the existing literature, our discussion is informed by studies conducted with the closest available age group, providing a relevant foundation for understanding the potential effects of MI on preschool-aged children. Although the specific neural pathways underlying these motor improvements remain largely unknown in this population, neuroscientific evidence from older children and adults provides a robust explanatory framework. The following discussion draws on these findings to propose plausible mechanisms underlying the observed gains in manual dexterity, ball-handling skills, and balance.
First, our statistical results revealed a significant effect of MI on manual dexterity in the experimental group compared to the PAG and CG. These findings align with the narrative review by Guilbert & Fernandez (2023), who demonstrated that MI improves performance in fine motor tasks such as drawing or object manipulation in children. However, it is important to note that this review is primarily based on descriptive studies, while our study uses a controlled experimental approach. This methodological difference strengthens the rigor and validity of our results, providing a more precise and reliable assessment of the impact of MI on manual dexterity. Positive effects of MI have also been reported in the studies by Asa et al. (2014) and Takazono & Teixeira (2018), who used similar manual tasks with 9-year-old children, with three groups comparable to those in our study. However, unlike these studies, which relied on a single training session, our study applied a protocol of 18 sessions, allowing for a more thorough evaluation of the effects of MI. The improvement in manual dexterity may be explained by several complementary mechanisms. In fact, MI is hypothesized to activate crucial brain regions such as the motor cortex, premotor cortex, posterior parietal cortex, basal ganglia, and cerebellum (Avanzino et al., 2015). These structures are directly involved in the planning, coordination, and execution of precise movements required for manual tasks (Glidden, 2009; Shadmehr & Krakauer, 2008). At the same time, MI promotes synaptic plasticity in the neural circuits involved in motor tasks (Avanzino et al., 2015). This adaptation could help refine brain connections, thereby improving movement coordination and precision (Ruffino et al., 2017). Moreover, MI may enhance sensorimotor feedback by optimizing the anticipation and integration of sensory information, which improves the precision and fluidity of fine motor movements (Guillot et al., 2012). This process is grounded in the internal models theory, which posits that the nervous system anticipates the sensory consequences of an action through an efference copy, even in the absence of movement, and compares this copy to internal predictions, thereby updating motor schemas (Lebon et al., 2013).
Secondly, our results highlighted an improvement in ball skills in the experimental group. This finding is consistent with the experimental work of Doussoulin & Rehbein (2011), who demonstrated improvements in the accuracy of ball throwing towards a target in children aged 9 to 10 after 6 sessions of MI training, despite methodological differences in the number of sessions and the age of the population. Furthermore, Taktek et al. (2008) demonstrated in a randomized controlled trial that MI combined with physical practice improves ball throwing accuracy in children aged 8 to 10 more than physical practice alone. This methodological approach is similar to ours and led to comparable results. Thus, experimental studies that used video observation in the visual imagery protocol, as in our study, have shown enhanced ball throwing and catching skills in children aged 7 to 10 (Zhang et al., 1992) and improved free throw performance in basketball in students aged 7 to 12 (Hatchi & Nicolas, 2023). MI has proven to be particularly effective in enhancing the accuracy and fluidity of ballistic movements in children. Its effectiveness may lie in its ability to activate neural circuits involved in motor coordination and execution, thereby strengthening synaptic connections and optimizing motor schemas (Guillot et al., 2008). This process is hypothesized to be supported by the internal models theory of movement, which suggests that the brain anticipates the sensory consequences of an action through internal representations even before the action is executed (Wolpert & Ghahramani, 2000). By engaging these representations, MI may enable children to mentally simulate the trajectories and postural adjustments required for successful completion of tasks such as aiming or catching (Cecchini et al., 2016). This mental simulation not only improves the execution of complex movements but also enhances anticipatory abilities and motor confidence, thereby significantly contributing to the overall development of motor skills (Behrendt et al., 2021).
Finally, regarding the improvement in balance observed in our study, our findings are consistent with those of Simonsmeier et al. (2021). Although their crossover experimental design differs from the methodology used in our study, they reported enhanced performance a standing balance task on bars among gymnasts aged 7 to 15 years following MI training. Furthermore, our results are in line with the randomized controlled trial conducted by Turan and Dişçeken (2019), which demonstrated the benefits of MI on both static and dynamic balance in adolescent handball players, despite methodological differences related to the age of the participants. Similarly, Mohamed et al. (2024) reported in a randomized controlled trial that MI is beneficial for children aged 7 to 10 with motor control issues. This improvement in balance may be attributed to the role of MI in activating key brain regions involved in postural control, including the parietal cortex, frontal cortex, vestibular system, basal ganglia, and cerebellum (Ferraye et al., 2014; Jeannerod, 2001). In particular, the cerebellum is thought to play a crucial role in compensatory and anticipatory postural adjustments by facilitating the integration of sensory feedback and anticipatory mechanisms necessary for maintaining balance (Yanagihara, 2014). Thus, MI could promote a better representation of postural adjustments, weight shifts, and stability strategies needed to maintain balance, resulting in reduced postural swaying and increased stability (Grangeon et al., 2011).
Beyond the neurophysiological and motor-specific explanations for each skill, additional factors may account for the observed superiority of MI over physical activity in our study. One key factor is attentional focus. During MI sessions, children can allocate their cognitive resources more efficiently to the critical aspects of the movement, which may enhance the encoding of motor representations and optimize both motor learning and performance (Bahmani et al., 2021). Another important factor is the novelty effect. As a novel and relatively unfamiliar activity for preschool-aged children, MI may have heightened their interest and intrinsic motivation, thereby facilitating engagement with the sessions, adherence to the protocol, and consolidation of motor learning (Mather & Plunkett, 2012). These factors may help explain why MI elicited larger improvements than conventional physical activity, although further research is needed to quantify their specific contributions.
Beyond attentional and motivational factors, MI may also support the development of executive functions, which are crucial during the preschool period. MI enables the representation of reality through multisensory mental images, whether of perceived or memorized objects (Guarnera et al., 2019). It also requires children to plan their actions, inhibit irrelevant responses, and manipulate internal representations, thereby engaging working memory, inhibitory control, and cognitive flexibility (Lebon et al., 2013). The literature indicates a positive correlation between imaginative abilities and executive functions, particularly visuospatial working memory and cognitive flexibility in children aged 6 to 7 years (Veraksa et al., 2022). Consequently, MI could not only enhance motor skills but also strengthen executive functions, providing a cognitive foundation conducive to learning, self-regulation, and adaptive behavior. This synergy between motor and executive development may partially explain the effectiveness of MI observed in our study.
Study Limitations and Directions for Further Research
Despite promising results, the study has some limitations. Conducting a follow-up was not feasible, which limits the assessment of the persistence of the observed effects. This constraint was mainly due to practical factors, including the limited availability of children and the challenges associated with obtaining repeated parental consent. Moreover, while six weeks allowed for the observation of initial changes, a longer period would have enabled the assessment of the long-term effects of MI. For future research, it would be relevant to use complementary instruments, such as neuropsychological measurements or brain imaging techniques, to better understand the mechanisms of the improvements observed. Another interesting avenue would be to assess the cognitive (memory, attention, executive functions) and emotional (emotional regulation, well-being) functions of participants. This would allow for examining the impact of MI on these aspects in addition to motor skills. It would also be useful to extend the study to children of different ages or populations with specific disorders. Finally, integrating MI with other approaches, such as internal dialogue, could enrich the results.
Practical Applications
The results of this study suggest that the MI protocol could be adapted for practical use by educators and therapists in school or rehabilitation settings. To facilitate its implementation, the protocol could be delivered as simplified guided sessions, including clear instructions and visual illustrations of the movements. The integration of digital tools, such as animated videos or interactive applications, would also allow children to practice MI independently or under supervision, while enhancing their motivation and engagement. Finally, providing practical worksheets or checklists would help professionals monitor children’s progress and adjust exercises according to their specific needs, making the protocol more accessible and operational in daily practice.
Conclusion
This study showed that an 18-session MI training program significantly improves the motor skills of preschool children. These results highlight the effectiveness of this approach, which is low-cost in terms of equipment and space, in promoting motor development during this crucial period. In this regard, integrating MI into school and educational programs, alongside physical activity, is a valuable strategy to support optimal motor development in children.
Footnotes
Acknowledgments
The authors would like to thank the preschool children and their families for their participation, as well as the teachers and the school principal for their valuable collaboration.
Ethical Considerations
The experimental protocol was previously approved by the ethics committee of the institute.
Consent to Participate
Written informed consent was obtained from the parents or legal guardians of all participating children prior to the start of the study.
Author Contributions
Conceptualization: Ichrak Abdelkefi, Sana Jarraya, and Jarraya Mohamed; Methodology: Ichrak Abdelkefi, Sana Jarraya, and Dorra Jallali; Software: Liwa Masmoudi; Data Collection: Liwa Masmoudi, Ichrak Abdelkefi, and Nesrine Ben Mansour; Writing—Original Draft: Ichrak Abdelkefi; Writing—Review & Editing: Ichrak Abdelkefi and Liwa Masmoudi.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.