
Abstract
Introduction
Lumbar decompression surgery has been a frequently preferred and clinically efficient surgical procedure for many years. Surgeons mainly prefer decompression surgery to reduce pain, improve functionality, and increase quality of life, specifically in cases requiring decompression procedures in the lumbar region (Sunderland et al., 2021). Patient education and rehabilitation practices before and after lumbar decompression surgery can improve the quality and quantity of clinical gains (Mannion et al., 2007). According to the current clinical guidelines, post-operative rehabilitation, including remote home exercise, clinical consultation, and patient education, is required due to the accelerated discharge procedures (Williamson et al., 2007).
In recent years, telerehabilitation procedures have become widespread, making it efficient to follow rehabilitation programs and home exercise prescriptions remotely (Seron et al., 2021). Comprehensive meta-analyses have emphasized the effectiveness of telerehabilitation, physiotherapy, and rehabilitation in chronic low back pain and other spinal lumbar pathologies (Fiani et al., 2020; Lara-Palomo et al., 2022). Nevertheless, the number of studies emphasizing telerehabilitation after lumbar surgeries is limited.
A recent feasibility study stated that combining telerehabilitation with wearable technologies may be a suitable protocol for rehabilitation after lumbar surgery (Master et al., 2024). One randomized controlled trial focused on the effectiveness of telephone-based rehabilitation after lumbar spinal surgery. The results of this trial, which included a total of 24 months of long-term follow-up, emphasized the advantage of telerehabilitation in terms of pain, disability, and quality of life, with particular emphasis on the patient’s compliance with the exercise program (Hou et al., 2019).
Nevertheless, the results of these limited number of studies do not provide a clear finding on the effectiveness of telerehabilitation in specific lumbar spinal surgery. Focusing on the effectiveness of telerehabilitation in particular patient groups may provide more pragmatic clinical outcomes, particularly considering that the clinical outcomes of fusion, decompression, or combination surgeries and the efficiency of rehabilitation after surgery may differ (Chang et al., 2017; Liang et al., 2017). Furthermore, the content of the rehabilitation program is also essential. Exercise training based on the biopsychosocial model and providing vertebral stability may be more advantageous after lumbar spinal surgery (Özden, 2022a, 2022b). Taking into account psychological parameters such as pain management and kinesiophobia may increase the effectiveness of core stabilization training (Ogunniran et al., 2023). Conversely, telerehabilitation offered in this context may provide more specific clinical outcomes.
Another crucial point in terms of the use of telemedicine is its more common preference for teleconsultation and teleassessment procedures (Craig et al., 2022; Iyer et al., 2021; Satin & Lieberman, 2021). Feasibility and field studies show that virtual spine consultation and surgical plan examinations are practical regarding patient and clinician satisfaction and cost-effectiveness (Hobson et al., 2021; Iyer, Bovonratwet, et al., 2022). Clinical guidelines on teleconsultation are available, and comprehensive reviews emphasize the importance of telemedicine visits (Goyal et al., 2020; Iyer et al., 2022). On the other hand, it has also been noticed that telemedicine assessment protocols have been developed, and feasibility studies have been carried out recently (Goyal et al., 2020; Hobson et al., 2021; Master et al., 2024).
Nevertheless, current studies do not provide evident data to produce meta-analyses and, therefore, clinical guidelines at a high level of evidence due to limited randomized controlled trials on telerehabilitation applications and insufficient clinical outputs on specific sampling. Thus, considering this lack of literature, we planned to conduct an interventional telerehabilitation efficacy study with patients undergoing lumbar decompression surgery. This study aimed to investigate the effect of post-operative telerehabilitation on pain and mobility in patients undergoing lumbar spinal decompression surgery.
Methods
Patients and Recruitment
A randomized controlled trial was conducted between June 2023 and March 2024 with individuals who were followed up after surgery by the Department of Neurosurgery at Bursa Çekirge State Hospital. Individuals were assigned to two groups: Usual Rehabilitation (UR) (n = 11) and Telerehabilitation (TR) (n = 11). Information about the study was given to 26 patients who were followed up in the Physiotherapy and Rehabilitation Unit in the second month after decompression surgery. Two of the individuals did not agree to participate in the study. One patient was excluded from the study because of malignancy, and the other was excluded because of a neurological comorbidity. The study was completed with 22 patients after decompression surgery, 11 in each group. The flow chart of the patient recruitment process of the study is presented in Figure 1. The Recruitment Flowchart of the Research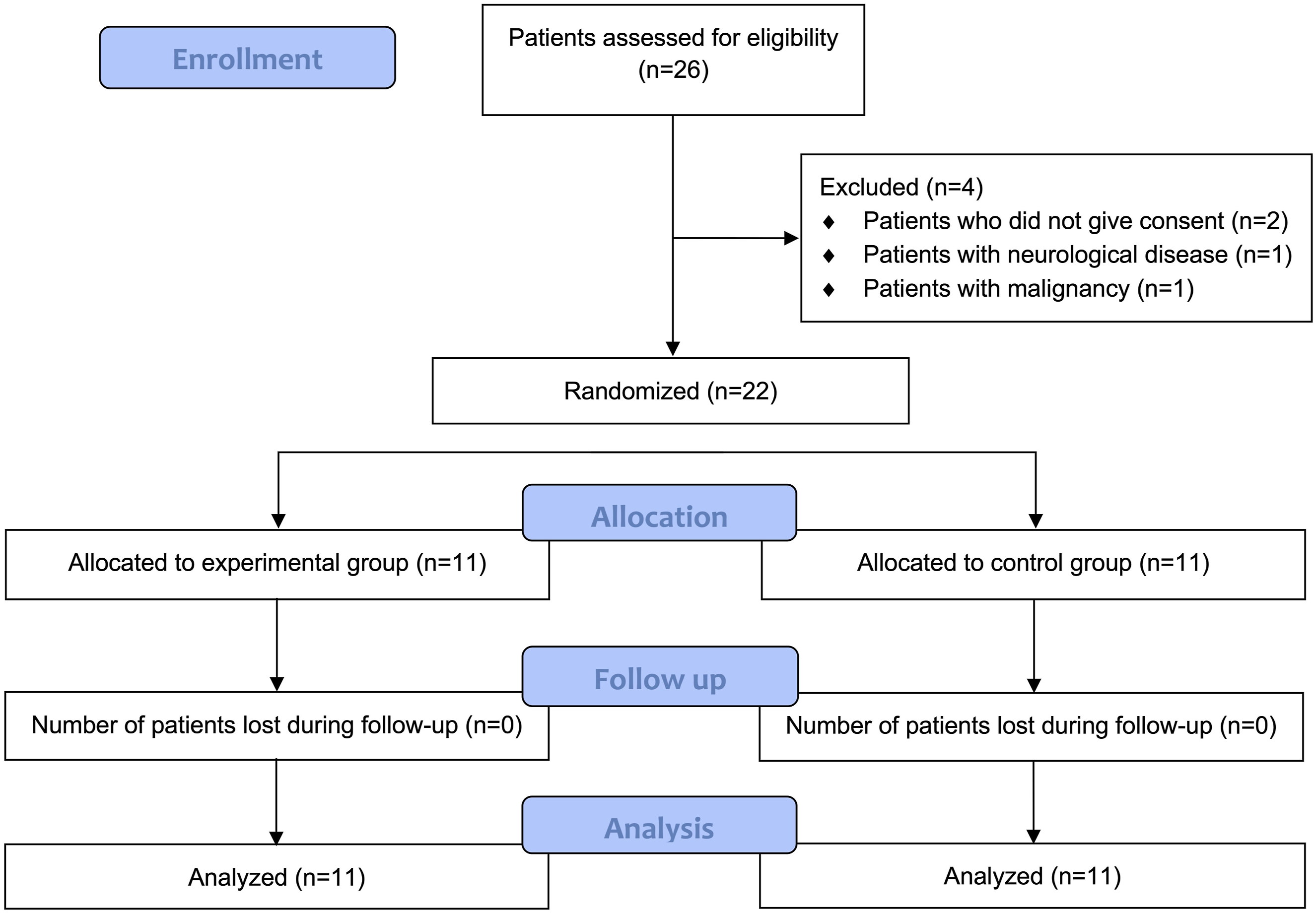
Eligibility Criteria
Inclusion criteria were: (1) individuals who were two months post lumbar decompression surgery, (2) patients aged between 18 and 65 years, and (3) no communication problems. Exclusion criteria were (1) individuals who underwent combined surgical procedures such as fusion or instrumentation in addition to decompression, (2) participation in all follow-up evaluations, (3) patients with malignancy, (4) individuals with a history of previous spinal surgery, (5) patients with poor co-operation during the study, (6) patients with other comorbidities.
Sample Size Calculation
Considering the effect size (1.65) obtained from the reference study with a similar design and subject matter (Hou et al., 2019), the sample size calculation calculated with G-Power 3 revealed that a total of 20 individuals, 10 in each group, would be sufficient (95% power and 95% confidence level).
Ethical Consideration
The present study was conducted in accordance with ethical principles and the Declaration of Helsinki. The written consent of the patients was obtained before the start of the first assessment of the study. The study protocol was approved by the ethics committee of Muğla Sıtkı Koçman University (No: 90, Date: 12.06.2023). The trial protocol was registered to clinicaltrial.gov (No: NCT06014645).
Randomization and Blinding
The National Institutes of Health National Cancer Institute Clinical Trial Randomisation Tool was preferred for the randomization procedures of the study. This software automatically generates the table required for randomly assigning individuals to groups. The working principle of this randomization tool is based on the randomization method for the asymptomatic maximal procedure (Zhao et al., 2018). This study did not include any blinding procedure.
Interventions
Individuals in both groups started rehabilitation within the study’s scope in the second month after lumbar decompression surgery. Conventional rehabilitation procedures had been applied in the previous two months. After one session of face-to-face exercise training, individuals in the UR group continued their treatment individually within a home program, while individuals in the TR group continued their treatment with video exercises.
Usual Rehabilitation Group: The control group received post-operative cognitive training and routine exercise therapy as described by Moseley et al. and was encouraged to be physically active (Moseley et al., 2004). These individuals were also offered strengthening, stretching, balance, coordination, and walking exercises, which included core stabilization.
Telerehabilitation Group: The intervention given to the study group was presented with a video exercise within the scope of telerehabilitation. This program included core stabilization (transversus abdominus, oblique abdominals, and multifidus lumborum muscles), strengthening, balance, coordination, and walking exercises for other extremities. Similar to UR, individuals in TR were encouraged to be physically active.
Outcome Measures
Characteristics of all study subjects were recorded before starting treatment. The first evaluation was performed two months post-operatively, and the second was performed two months after treatment. In these two evaluation sessions, Visual Analogue Scale (VAS), Tampa Kinesiophobia Scale (TSK), Pain Catastrophizing Scale (PCS), Roland Morris Disability Questionnaire (RMDQ), lumbar region flexibility in flexion-extension and lateral flexion directions, lumbar region endurance for flexor-extensor muscles, Functional Reach Test (FRT) and Stair Climbing Test (SCT) were evaluated.
Visual Analog Scale
Participants’ pain levels were measured on an analog scale, on which they could mark their pain level using a 10-cm straight line. The pain level increases from 0 to 10. The VAS is a valid and reliable assessment tool for lumbar spinal conditions (Vishwanathan & Braithwaite, 2019).
Tampa Scale of Kinesiophobia
The assessment of individuals’ fear of movement due to pain was performed with a 17-item TSK. In this questionnaire, movement phobias related to tasks involving movement in the individual’s daily life are addressed. The validity and reliability of the Turkish version of the questionnaire were performed by Tunca Yılmaz et al. (Yilmaz et al., 2011).
Pain Catastrophizing Scale
The PCS is a 13-item patient-reported outcome measure assessing participants’ psychological perceptions of pain. The questionnaire has 0-4 Likert-type answers. Turkish validity and reliability of the questionnaire have been demonstrated (Süren et al., 2014).
Roland Morris Disability Questionnaire
The RMDQ is a gold-standard questionnaire that assesses the functional status of individuals with spinal disability. RMDQ has 24 items. It is frequently used in the post-operative period of lumbar surgery. Turkish validity and reliability of the questionnaire are available (Küçükdeveci et al., 2001).
Lumbar Joint Flexibility (Flexion-Extension-Lateral Flexion)
For flexion the participant stands on a high block. The participant then leans forward with waist flexion without flexing the knees. At the end point of the movement, according to the distance of the finger approaching the block, the distance between the finger and the block is measured and recorded with a negative symbol and the distance between the finger and the block is measured and recorded with a positive symbol. For extension, the participant stands in front of a wall, facing the wall. The participant’s pelvis and torso are in contact with the wall. The participant is asked to perform lumbar extension. At the end point of the movement, the distance between the sternal notch and the wall is measured. For lateral flexion, the participant stands in front of a wall with their hands by their trunk. The participant is asked to perform lumbar lateral flexion. Based on the third hand finger, the distance between the end point of the movement and the beginning of the movement is measured and noted (Robinson & Mengshoel, 2014).
Lumbar Muscle Endurance (Flexor-Extensor)
For flexor endurance, participants are placed in a supine position with their hips and knees flexed 90 degrees and their trunk flexed 60 degrees on a wedge. Stabilization is provided by placing support behind their feet. After the wedge is moved back 10 cm, the participants try to maintain their body position for as long as possible. The time after the wedge is retrieved and until the participant re-establishes contact with the wedge is measured and recorded. For extensor endurance, the participant is placed prone with the upper edge of the iliac crests in line with the upper edge of the bed. The lower parts of the body in contact with the bed are strapped to the bed. Participants cross their arms across their chest and try to maintain a neutral position for as long as possible. The time between the start of the test and the moment when the neutral position is disturbed is recorded (Reiman et al., 2012).
Functional Reach Test
FRT is a physical performance test in which static balance is assessed. The participant stands upright on both feet in a comfortable position. The support surface is adjusted so that the feet are approximately shoulder-width apart. The arm is extended parallel to the wall with 90° flexion. Reach forward as far as possible to maintain normal physiological curvatures of the lumbar and cervical spine. Measure the distance between the fingertip in the initial position and the distance in the final position (Vachalathiti et al., 2020).
Stair Climbing Test
A 9-step ladder with a handrail with a step height of 20 cm is used for the test. The participant is instructed to ascend and descend the staircase as quickly but safely as possible. Handrails and walking aids are allowed if necessary. The time starts with the start command and ends when the participant has both feet in contact with the ground. During the test, the participant can stop and rest if necessary, but the timing continues. The time taken to ascend and descend the stairs is recorded (Ljungquist et al., 2003).
Statistical Analysis
The research data were analyzed using SPSS v25 for Mac. The significance level for all analyses was p < .05. Pearson Chi-square test for categorical variables and Mann-Whitney U test for continuous variables were used to determine the homogeneity of baseline values between UR and TR. The Shapiro-Wilks test checked the homogeneity of clinical evaluations. Wilcoxon and Mann-Whitney U tests were used to determine statistically significant differences between and within groups for VAS, TAF, PCS, RMDQ, lumbar region flexibility in flexion-extension-lateral flexion directions, lumbar region endurance flexor-extensor, FRT, and SCT, respectively. All data are presented with per-protocol analyses.
Results
The Individual Characteristics of the Patients in the TR and UR
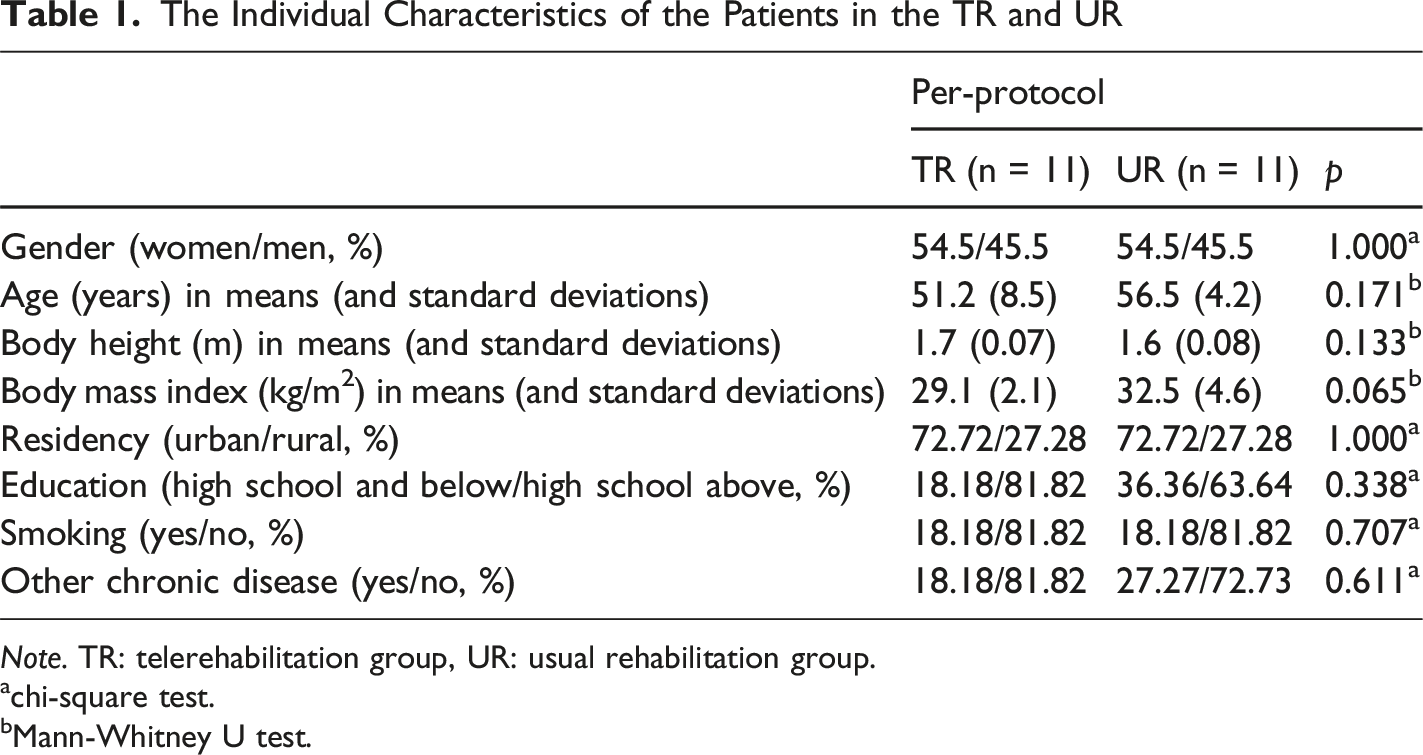
Note. TR: telerehabilitation group, UR: usual rehabilitation group.
achi-square test.
bMann-Whitney U test.
The Comparison of the Groups in Terms of Patient-Reported Outcome Measures
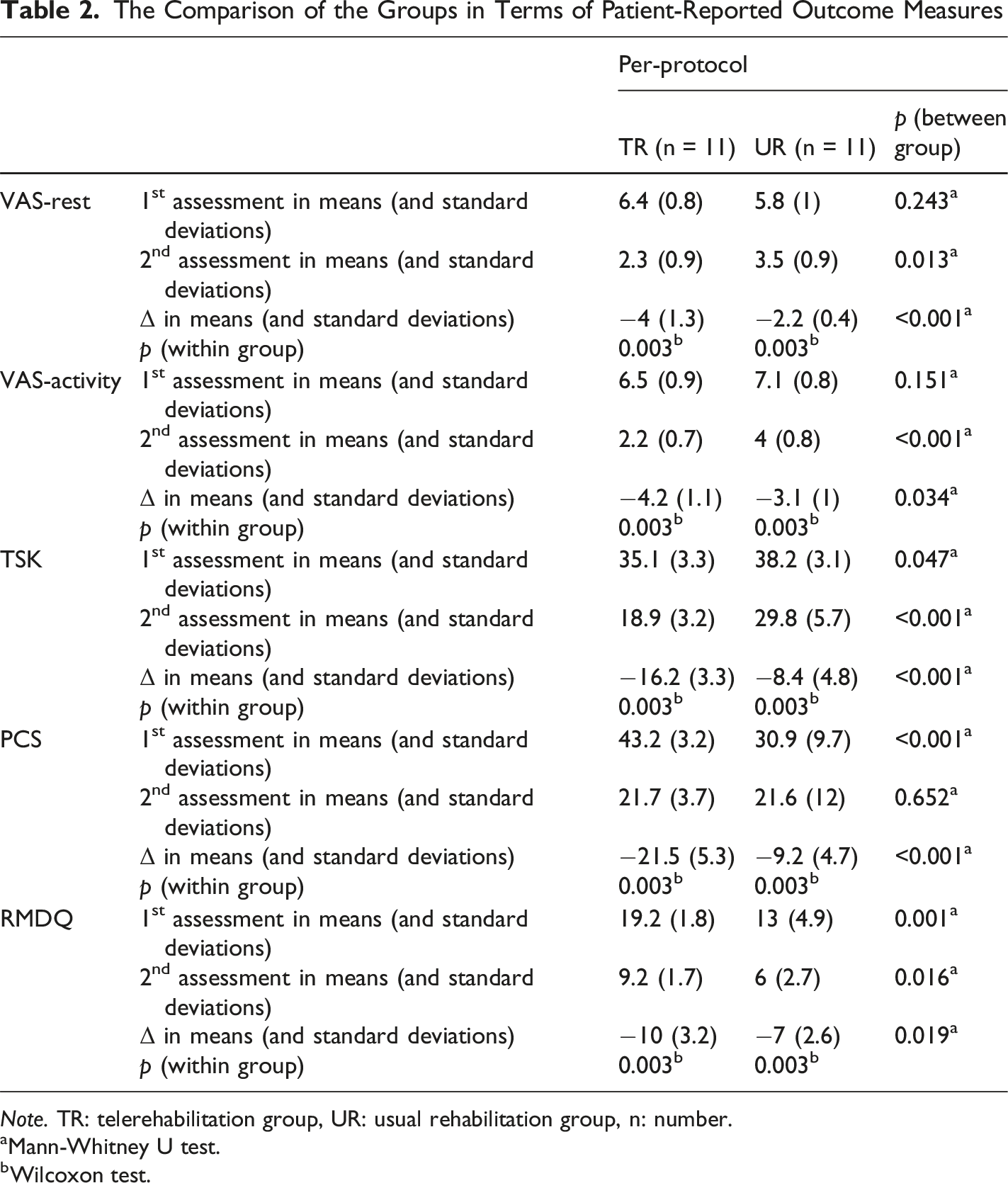
Note. TR: telerehabilitation group, UR: usual rehabilitation group, n: number.
aMann-Whitney U test.
bWilcoxon test.
The Comparison of the Groups in Terms of Performance Tests
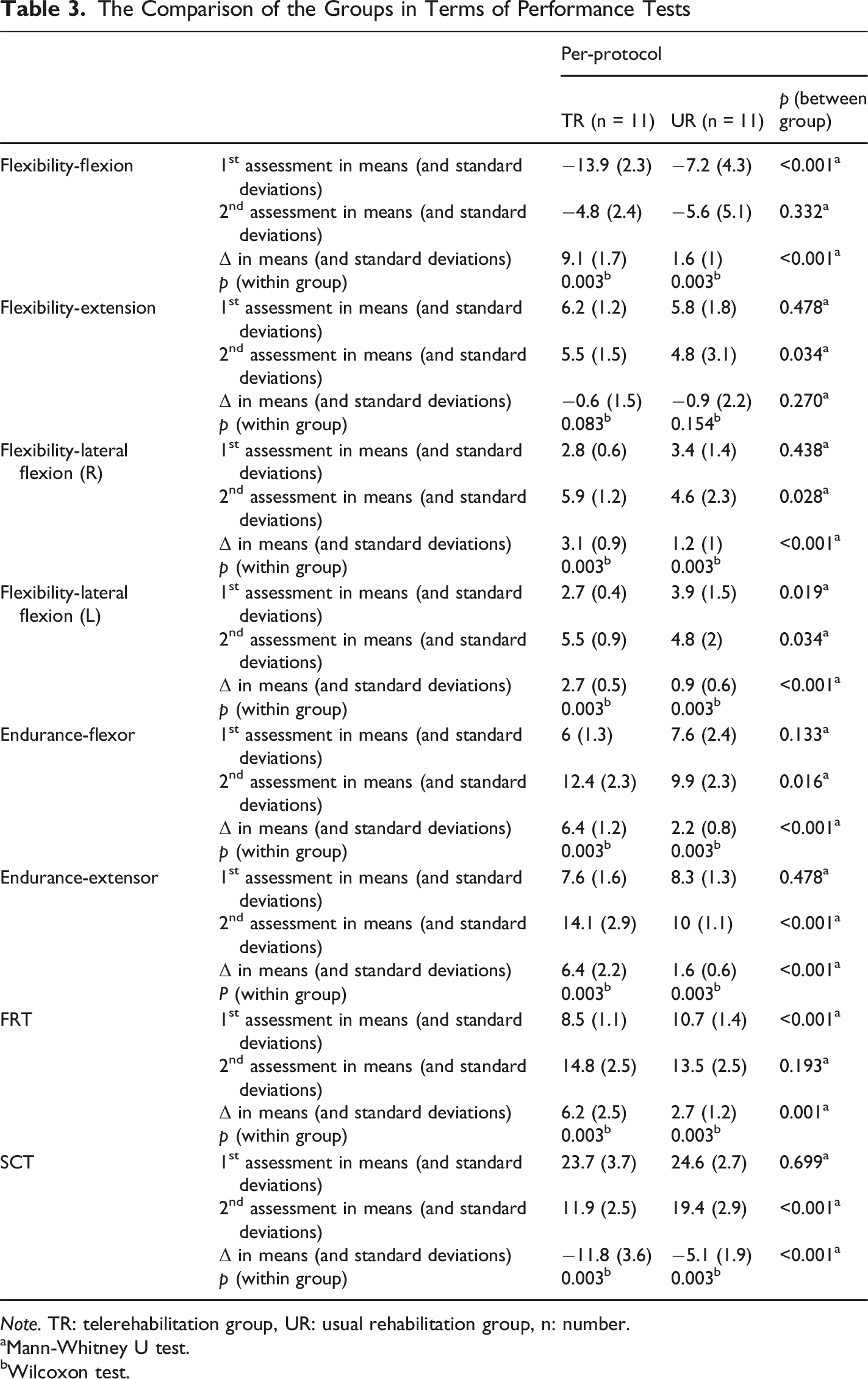
Note. TR: telerehabilitation group, UR: usual rehabilitation group, n: number.
aMann-Whitney U test.
bWilcoxon test.
Discussion
This study focused on the effectiveness of physiotherapy and rehabilitation programs delivered via telerehabilitation on pain, function, kinesiophobia, pain catastrophizing, flexibility, endurance, and physical performance in individuals after lumbar decompression surgery. The result provided the superiority of post-operative physiotherapy via telerehabilitation in patients undergoing lumbar decompression surgery. Considering the limited number of interventional studies focusing on the effectiveness of telerehabilitation after lumbar surgery, neurosurgery clinicians should consider telerehabilitation in further studies and in post-operative terms for the patients in clinical practice.
Telerehabilitation has become very popular in recent years (Seron et al., 2021), and it is recognized as an effective health service and an important cost-effective procedure (Nizeyimana et al., 2022). The effectiveness of telerehabilitation in chronic low back pain has been demonstrated (Lara-Palomo et al., 2022). Telemedicine methods are frequently used before and after lumbar surgeries (Craig et al., 2022; Goyal et al., 2020; Iyer, Bovonratwet, et al., 2022; Master et al., 2024). However, a limited number of studies have addressed rehabilitation follow-up with video exercises within the scope of telerehabilitation. The lack of studies addressing the effectiveness of telerehabilitation after lumbar decompression surgery reveals the originality of our study.
A recent feasibility study tested the combination of wearable technologies and telehealth services for applicability after lumbar spinal surgery. In this study by Master et al. with 16 patients, patient follow-up was provided with physical activity monitoring. According to the study results, while the gain in pain and disability parameters was emphasized, the usefulness of patient follow-up with wearable technologies in physical activity was correspondingly mentioned (Master et al., 2024). In our study, we planned a randomized controlled trial of video exercise rehabilitation protocol within the scope of telerehabilitation. Our telerehabilitation method provided effective clinical outcomes in pain and function compared to standard rehabilitation procedures. Although the design of the two studies differed, it is clear that telerehabilitation after lumbar spinal surgery has positive effects on physical parameters such as pain and disability. With the increase in the number of similarly designed studies on telerehabilitation in future studies, the outputs of meta-analyses may provide more apparent implications for clinical guidelines after lumbar spinal surgeries.
In our study, in addition to pain and disability gains, we also focused on flexibility and endurance. Especially flexibility and muscle strength gains after lumbar decompression surgery should be addressed more in clinical studies. Our exercise protocol, which includes core stabilization and stretching exercises (Ogunniran et al., 2023), has important implications for flexibility and muscle strength after decompression surgery. Another randomized controlled trial of a mobile application focused on pain, disability, and quality of life. However, as can be seen from many reviews, clinical outcomes based on flexibility and muscle strength measurements are not sufficiently focused. In this study, Hou et al. emphasized the importance of telerehabilitation in terms of pain and function in a 24-month long-term follow-up (Hou et al., 2019). The fact that these results are similar to the clinical outcomes of our study emphasizes the importance of telerehabilitation in both short-term and long-term follow-up.
In our study, we also focused on kinesiophobia and pain catastrophizing, which are psychological aspects of pain (Picavet et al., 2002). Recent reviews show that rehabilitation with a biopsychosocial model provides more effective results after lumbar surgeries (Özden, 2022a; 2022b). Therefore, our study shows that holistic rehabilitation services can be provided within the scope of telerehabilitation to improve the psychological parameters of pain.
Another momentous clinical outcome that should be emphasized in our study is the evaluations performed with physical performance tests. It is comprehended that the gains in individuals’ daily living activities after lumbar surgery are also evaluated through RMDQ (Burbridge et al., 2020). However, more objective evaluations can be made with measurements that represent real life more clearly, such as stair climbing, climbing stairs, and reaching forward. In our study, the telerehabilitation group provided more effective clinical outcomes in the reaching forward and stair climbing tests. In this respect, we have emphasized our results on the effectiveness of telerehabilitation through more actual clinical outcomes.
Clinical Implications
According to our clinical telerehabilitation experience, we think that telerehabilitation can provide effective results considering early discharge after lumbar surgery, accelerated comprehensive rehabilitation protocols (Nielsen et al., 2008; Oosterhuis et al., 2017), and the patient group in the working population due to the relatively young population. Since it is known that technology literacy is high, especially among post-surgical individuals under 65 years of age (Vujkovic et al., 2024), the use of telerehabilitation after lumbar decompression will provide efficient clinical outcomes. However, mobile apps or other telehealth software should be designed with user-friendly design in order to improve its comprehensibility regarding the remote design of this procedure. In particular, monitoring patients’ participation in exercise with manual methods or automated systems may increase the efficiency of clinical outcomes. Finally, progressive revision of the exercise programs offered to the patients may make the gains in the clinical parameters of the patients more efficient.
Limitations
Some limitations related to the methodological design of the study should be mentioned. First, in this randomized controlled trial, a single or double-anonymized design could not be used for the evaluators, treatment providers, or group individuals. International guidelines strongly recommend binding procedures to reduce bias (Sherrington et al., 2000). However, in our study, we were able to provide an evaluation by a single therapist with a pragmatic design due to the currently available conditions. In this way, we aimed to reduce the risk of bias by standardizing evaluation protocols. Secondly, due to its specific design and specificity, our study focused only on individuals with lumbar decompression surgery. The generalizability of our results in other populations, specifically in older individuals after decompression surgery combined with fusion, is still being determined. Thirdly, the fact that telerehabilitation was offered to patients within a standardized program and did not include specific modifications due to its nature may have masked the successes in individual treatment outcomes. However, due to the randomized controlled design, we aimed to achieve a high-level control mechanism with a stable rehabilitation protocol. Future studies may provide up-to-date clinical implications on different control groups by including different techniques in telerehabilitation protocols as part of rehabilitation.
Conclusions
The result provided the superiority of post-operative physiotherapy via telerehabilitation in patients undergoing lumbar decompression surgery. Considering the limited number of interventional studies focusing on the effectiveness of telerehabilitation after lumbar surgery, neurosurgery clinicians and rehabilitation professionals should consider telerehabilitation in further studies and in post-operative terms for the patients in clinical practice.
Footnotes
Ethical Considerations
Consent to Participate
Informed consent of the patients was obtained.
Author Contributions
Fatih Özden: Conceptualization, Data curation, Formal analysis, Methodology, Project administration, Writing – original draft, Writing – review & editing. Mustafa Yalçın: Data curation, Investigation, Writing – review & editing. İsmet Tümtürk: Data curation, Methodology, Writing – original draft, Writing – review & editing. Ferdi Başkurt: Formal analysis, Methodology, Writing – review & editing. Baki Umut Tuğay: Formal analysis, Methodology, Supervision, Writing – review & editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.