
Abstract
Policing demands are widely acknowledged to negatively impact on the physical and mental health of police officers and staff. Research has documented the need for greater insight into the stressors and trauma that impact police officers, with a current national drive towards enhancing the police wellbeing agenda: namely, Oscar Kilo and the National Wellbeing Service. To understand the current wellbeing strategies in place, 34 Blue Light Wellbeing Frameworks were analysed. A mixed methods approach was adopted: quantitative data was descriptively examined, with thematic analyses employed to explore the qualitative data. Findings from the review highlight developments in police wellbeing, as well as areas for future development.
Literature review
Policing responsibilities and demands are widely acknowledged to negatively impact on the physical and mental health of police officers and staff (Clements et al., 2020). Following the 2017 launch of Oscar Kilo 1 (OK) and the Blue Light Wellbeing Framework 2 (BLWF; Hesketh and Williams, 2017), the Front Line Review was conducted (Home Office, 2019) and the National Police Wellbeing Service 3 (NPWS) was launched in 2019. During this time, a range of national wellbeing activities have been promoted, with ongoing work to continue to support the delivery of the wellbeing agenda. Police Federation of England and Wales (2020) recently emphasised the importance of mental health in policing and launched a Hear ‘Man Up’, Think ‘Man Down’ campaign, urging police officers and staff to look out for colleagues who may be in need of support. Despite the significant focus and improvements in police wellbeing, the Police Federation of England and Wales (2020) argue that efforts must continue ‘to provide earlier, better and more consistent support’. Concerns have been raised in terms of management capacity to proactively share the wellbeing message, the consistency of its implementation and the sustainability of its impact (Knight, 2019; Ordon et al., 2019). Furthermore, a recent review by Syed et al., (2020) cautioned that the prevalence of mental health problems may be an inaccurate reflection of the true picture, with further consideration of risk factors and the diversity of issues required.
Recent developments in police wellbeing
Extensive academic research has documented the need for greater insight into the multifaceted stressors and traumas that impact police officers; not only to ensure individual and collective wellbeing of officers and forces, but also as it is a pressing public health issue that needs addressing (Miller et al., 2019). In the UK, several recent campaigns and evaluations that reinforce these concerns have occurred. As noted above, the past few years has seen the launch of OK, the BLWF (Hesketh & Williams, 2017) and the NPWS. The Front Line Review captured evidence from police forces across England and Wales and documented the variety of issues affecting the working lives of both officers and staff – with wellbeing being one of the key themes evaluated (Home Office, 2019; Knight, 2019). The findings of the review are echoed in other research, highlighting increased demand but increasingly limited capacity, persistent organisational and operational stressors, a lack of time and commitment by management in enabling individuals to focus on activities which positively promote wellbeing, the complexity of evaluating and seeking ways to improve wellbeing, and the prevailing scepticism about the wellbeing agenda being put forward – particularly relating to its consistency in implementation, and ability to have a lasting impact (Knight, 2019; Ordon et al., 2019; Phythian et al., 2021).
As well as their Hear ‘Man Up’, Think ‘Man Down’ campaign, PFEW have also launched a video providing practical advice for police officers on mental wellbeing in light of the recent coronavirus pandemic (Police Federation of England and Wales, 2020) and several forces promote mental health action days via hashtags such as #TimetoTalk and #WorldMentalHealthDay on their websites and social media (e.g. see Essex Police, 2019). In December 2019, an online booking system went live on OK to enable forces across the UK to request a visit from a Wellbeing Van, provided by the NPWS; the vans offer ‘physical, psychological and financial health checks to officers and staff’ and are ‘supported and staffed by Occupational Health staff or Occupational Health providers from each force area’ (Oscar Kilo, 2019). Similarly, localised initiatives include a welfare van introduced by Hampshire Police to support police officers at crime scenes and wellbeing wagons offering psychological and physical screenings (The Telegraph, 2019a). Police Scotland also gained funding from Police Care UK to conduct a 3-year workplace action plan focussing on mental health and wellbeing, in partnership with See Me (Police Scotland, 2020). Despite the significant focus given to police wellbeing via such strategies, the Police Federation of England and Wales, 2020 argue that efforts must continue ‘to provide earlier, better and more consistent support’. While there is a notable increase in recognition that mental health is as important to prioritise as physical health in the police force via such visible promotional strategies, Edwards and Kotera (2020) argue that trends in the status of mental wellbeing in UK police forces still indicate a ‘significant mental health crisis’ is imminent.
Academic studies continue to document the ‘high-risk’ nature of the profession and the unique physical and mental challenges the work presents (Kamkar et al., 2020). Considerable emphasis is placed on the extensive mental health burdens that ensue for current individual officers, in addition to wider personal circles such as friends and family (Edwards and Kotera, 2020; Knaak et al., 2019). Recent studies have especially centred on: the importance of understanding, monitoring and preventing psychological work injuries from exposure to trauma, such as post-traumatic stress disorder (PTSD) (Foley and Massey, 2019; Grupe et al., 2019; Miller et al., 2019); the lack of emphasis on understanding the ‘moral injuries’ that arise from the conflicts that occur when officers try to uphold the law, but also adhere to personal moral and spiritual values (Papazoglou, 2019; Papazoglou et al., 2020; Wagner et al., 2019); and tackling mental health stigma, which is argued to remain embedded in police culture (Edwards and Kotera, 2020).
Psychological work injuries
Police officers are regularly exposed to threats to their, or others’, physical safety from dealing with routine criminal activity, in addition to risks which come from more extraordinary or extreme events such as natural disasters (Kerswell et al., 2019; Regehr et al., 2019). Persistent exposure to ‘violence, aggression, environmental stressors and traumatic events’ has resulted in poor physical and mental health in the police force (Liakopoulou et al., 2020: 1). Specific and pronounced concerns surrounding psychological work injuries such as PTSD, depression, anxiety and suicide have been evidenced recently across a variety of geographical contexts (see Clements et al., 2020; Foley and Massey, 2019; Mona et al., 2019; Sheard et al., 2019; Soomro and Yanos, 2019).
In the UK, there have been several studies and media articles that have detailed some of the tangible effects of the psychological injuries being experienced by officers. Currently, the Trauma Resilience in the UK Policing project (2019) is utilising a series of qualitative and quantitative methods to explore the prevalence of trauma exposure in operational policing and find ways to support trauma processing and maintain resilience. Preliminary findings from their online survey of 16857 officers and operational staff, conducted in 2018, show that 20 per cent of participants who had experienced trauma had symptoms of some form of PTSD (BBC, 2019, Policing: The Job & the Life, 2019). Furthermore, ‘66 percent of all respondents reported a psychological or mental health issue which they felt was a direct result of police work’ (Policing: The Job & the Life, 2019). Foley and Massey (2019: 24) highlight a steady increase in police officer illness in the preceding 3 years to their study due to ‘psychological disorders’ in the Metropolitan Police Service. Moreover, in 2019, it was also reported that numbers of police officers being signed off sick with stress and anxiety had doubled in the prior 5 years following a Freedom of Information request of 40 forces across the UK (The Telegraph, 2019b).
However, as Sheard et al. (2019) argue, recent studies do not always assess the prevalence of such psychological injuries according to the role that officers have. Their survey of 602 officers in North East England found that, while most questionnaire respondents reported having experienced mental health difficulties, the role held had a significant effect on levels of certain psychological difficulties. For example, ‘resolution without deployment officers reported higher levels of secondary traumatic stress and lower compassion satisfaction than individuals in a number of other roles’ (Sheard et al., 2019: 273). In Syed et al.’s (2020) systematic review of 16 databases and over 11000 publications on mental health problems in police personnel spanning the last 40 years, they emphasise the need for studies to centre on the variety of mental health problems, and subsequent secondary conditions, experienced. This is to complement the disproportionate (although important) centring of research on PTSD. They found that officers demonstrate a considerable range of conditions; for example, one in 10 across their dataset met the criteria for an anxiety disorder or suicidal ideation, with potentially damaging coping mechanisms also noted, such as the hazardous drinking that approximately ‘one in four police officers’ screened positive for (Syed et al., 2020: 3).
Police culture and mental health stigma
A prevailing barrier to police wellbeing that continues to feature in recent research is that of police culture, especially regarding mental health stigma (see Demou et al., 2020; Purba and Demou, 2019). Contreras-Negretti (2019) argue that hegemonic masculinity still pervades the police, normalising the ‘silencing of distress’ (p. 11) and causing the suffering individuals to be emotionally alienated. Edwards and Kotera (2020) state that the UK-based police officers they interviewed experienced discrimination and stigmatising attitudes from colleagues upon developing mental health issues. Cohen et al. (2019) highlight that traditional police culture restricts the creation and implementation of appropriate wellness agendas, as there is a lack of investment from leaders due to persistent notions of ‘toughness’ being required for the job. This, they argue, in turn generates reluctance from individuals to speak out (Bell and Eski, 2016). Mental health stigma filters into decision-making to manage symptoms by the individual, such as refraining from taking time off (Stamatakis, 2019), which generates perceived devaluation of skills and abilities (Knaak et al., 2019), and causes delays in pursuing treatment (Velazquez and Hernandez, 2019). Velazquez and Hernandez (2019) also allude to the need for more research centring on endorsement (conscious or otherwise) of negative stereotypes about people with mental health issues by police officers. Syed et al. (2020) argue that effective preventative mechanisms for mental health problems should be focused on tackling negative police cultures via stigma reduction strategies to promote more positive peer and leader attitudes towards mental health.
Summary
Recent literature highlights the need for police forces globally to be adapting to new technological, socio-economic and political contexts which consistently bring new physical and mental challenges. These include: austerity and other financial or resource constraints (Hesketh et al., 2019; Miller et al., 2019); technological advances which have generated new, or adaptations of pre-existing, crimes; and increased prevalence of crimes that typically present traumatic experiences for officers (such as child sexual exploitation [CSE], see Gray & Rydon-Grange, 2020). Whilst there are encouraging developments through the implementation of both national and local wellbeing initiatives, literature indicates that more work is needed to reduce stigma and to develop a positive police culture to ensure appropriate support is available to police staff and officers who continue to work in a developing and increasingly complex society. What is more, amongst the plethora of interventions and training that have arose over the past few years, it is critical to ensure progress and efficacy is regularly reviewed and evaluated. This study proposes to review BLWFs to understand the current wellbeing strategies in place, in addition to the areas of wellbeing that UK forces deem to require development.
Method
Blue light wellbeing framework
The BLWF consists of six sections within wellbeing and policing: Leadership (L); Absence Management (AM); Creating the Environment (CE); Mental Health (MH); Personal Resilience (PR); and Protecting the Workforce (PW). Each section within the framework contains a number of statements about particular subthemes relating to the section theme, with a total of 94 statements in the framework. For each statement, the force records various measures, including: the self-assessed level of development in regard to a particular aspect within a theme (fully developed [FD], in development [ID], or underdeveloped [UD]); notes to support their self-assessment level; and the overall, self-assessed level of development for each of the six sections (FD, ID, UD).
Research design
The research used a mixed methods approach incorporating both qualitative and quantitative methodologies. Put simply, quantitative approaches use statistical methods to measure and analyse numerical data, which is often associated with greater accuracy, validity and reliability of data, allowing for comparison and replicability. However, whilst quantitative methods are adept in illustrating straightforward information and trends, they do not explain the nuances as to why a particular outcome is taking place. This is why qualitative approaches are illuminating as they provide meaning as well as providing contextual information to enhance the quantitative data. Furthermore, Clements et al. (2020) highlight the dearth of qualitative studies that have examined the social context of wellbeing, with quantitative studies having previously dominated.
Procedure and analysis
Each of the frameworks were individually extracted from the Oscar Kilo website (a cut-off date of 23rd March 2020 was applied) and imported into MS Excel. During the compiling of data, each framework was pseudo-anonymised by the researchers by assigning an ID number to each framework. A total of 34 frameworks were available for analysis (a further four frameworks were excluded from analysis due to missing data).
Both quantitative and qualitative analyses were conducted on data collected using the BLWF. Self-assessment scores (UD, ID, FD) were collected and quantitatively coded for each of the framework’s six sections (i.e. 1 = UD; 2 = ID; 3 = FD). Upon completion of data cleaning, the dataset was then imported into SPSS IBM v.26 for descriptive analysis. As each of the six theme scores were summed to create the total development score, Cronbach’s alpha was used to test the internal consistency of the total development score. The test found that the total development score had an almost excellent internal consistency, α = .895. Qualitative data was collected from completed ‘notes and evidence’ sections. The completed notes sections 4 were transferred into NVivo (QSR International) for thematic analysis; responses were collated for each statement for all forces.
Results
Quantitative overview of the BLWF
To first understand the extent to which each framework was complete, the number of answers to each was examined. The average total number of questions answered was 86.53 (SD = 15.40), out of the total 93 possible questions. This average involved 18 frameworks that completed all of the questions, with only three frameworks appearing as outliers and the remaining 13 frameworks failing to complete the questions in full. In understanding the answers across each theme, the number of frameworks that provided full sets of answers were totalled. Overall, full answers were present in: 28 (82.35%) frameworks for AM; 26 (76.47%) frameworks for CE; 27 (79.41%) frameworks in L; 30 (88.24%) frameworks in MH; 27 (79.41%) frameworks in PR; and 21 (61.76%) frameworks in PW. The totalling highlighted how MH and AM were the themes that provided the most completed questions, with PW providing the most incomplete answers across the sample of frameworks.
Development self-assessment: total development score
Each question in the six themes were scored (1 = UD; 2 = ID; 3 = FD); this score was totalled across each theme to generate total theme scores, and further summed to form an overall ‘total development score’ across all 34 frameworks. The total development score ranged between 93 (if a force was UD across all 93 questions) and 279 (if a force was FD across all 93 questions), meaning a higher total score reflected greater development of the overall organisation. The average total development score was 220.65 (SD = 29.70), meaning that forces as a whole were just verging into ‘fully developed’. To understand how well developed each of the six themes were in relation to the total score, each of the theme scores were compared to their possible maximum. This involved the actual score of each theme being compared to the total possible maximum if all 34 frameworks in that theme were fully developed. This was then presented as a percentage to standardise the scoring across each of the themes (see Figure 1). Proportion of development across each of the six themes, using the total development score as a benchmark for comparison.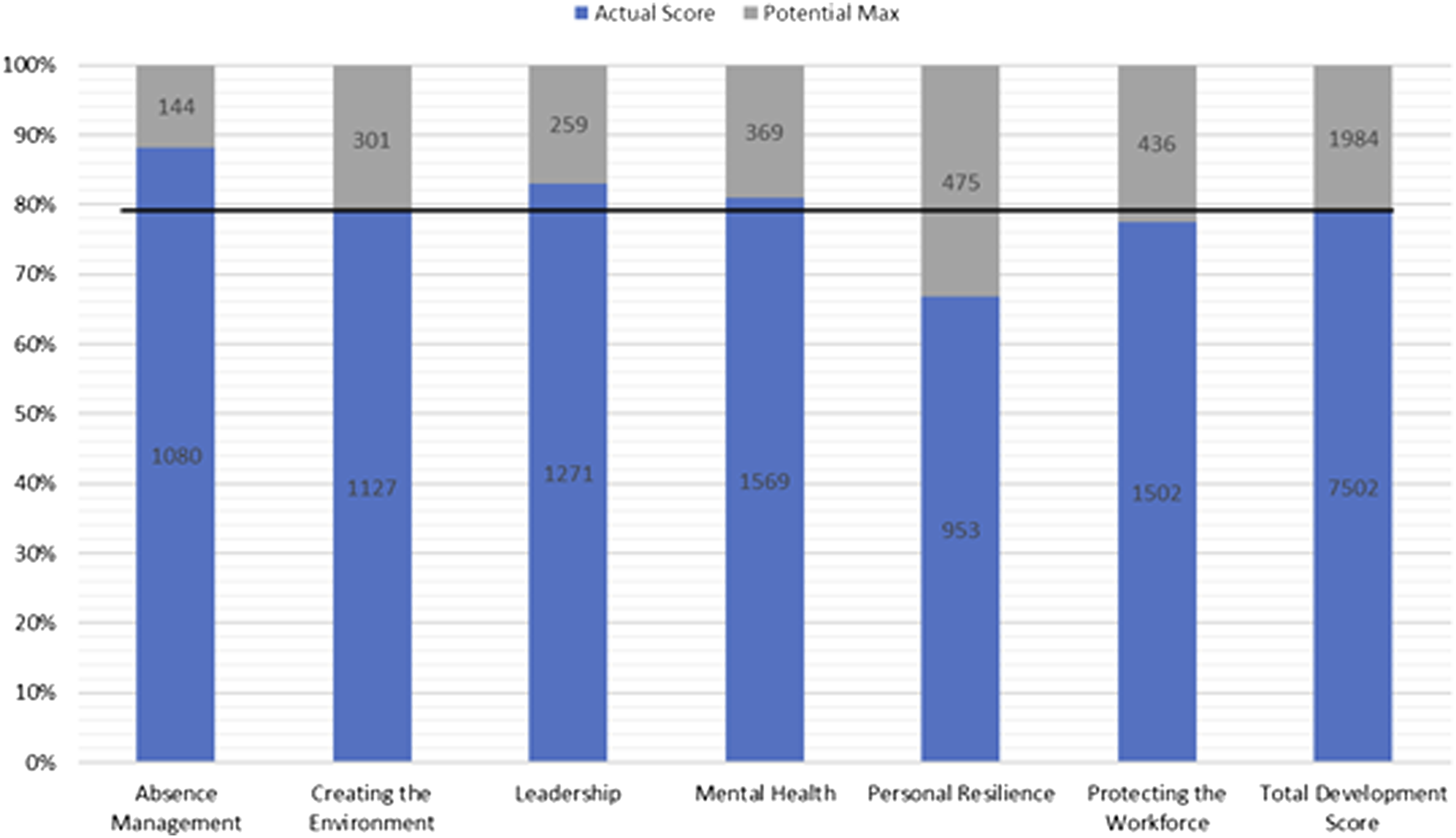
As seen within Figure 1, AM appeared to be more developed in comparison to all other themes with 88.2% of the score potential achieved by all forces. Conversely, PR appeared to be less developed in comparison to all other themes, with 66.7% of the score being achieved by all forces. Furthermore, this trend did not relate to the number of answered questions in each theme, as PW had the least completed questions and MH had the most comprehensively answered sections. This suggested that the greater development of AM and the lesser development of PR was based upon the actual reported scoring of the forces within each framework.
Qualitative overview of the BLWF
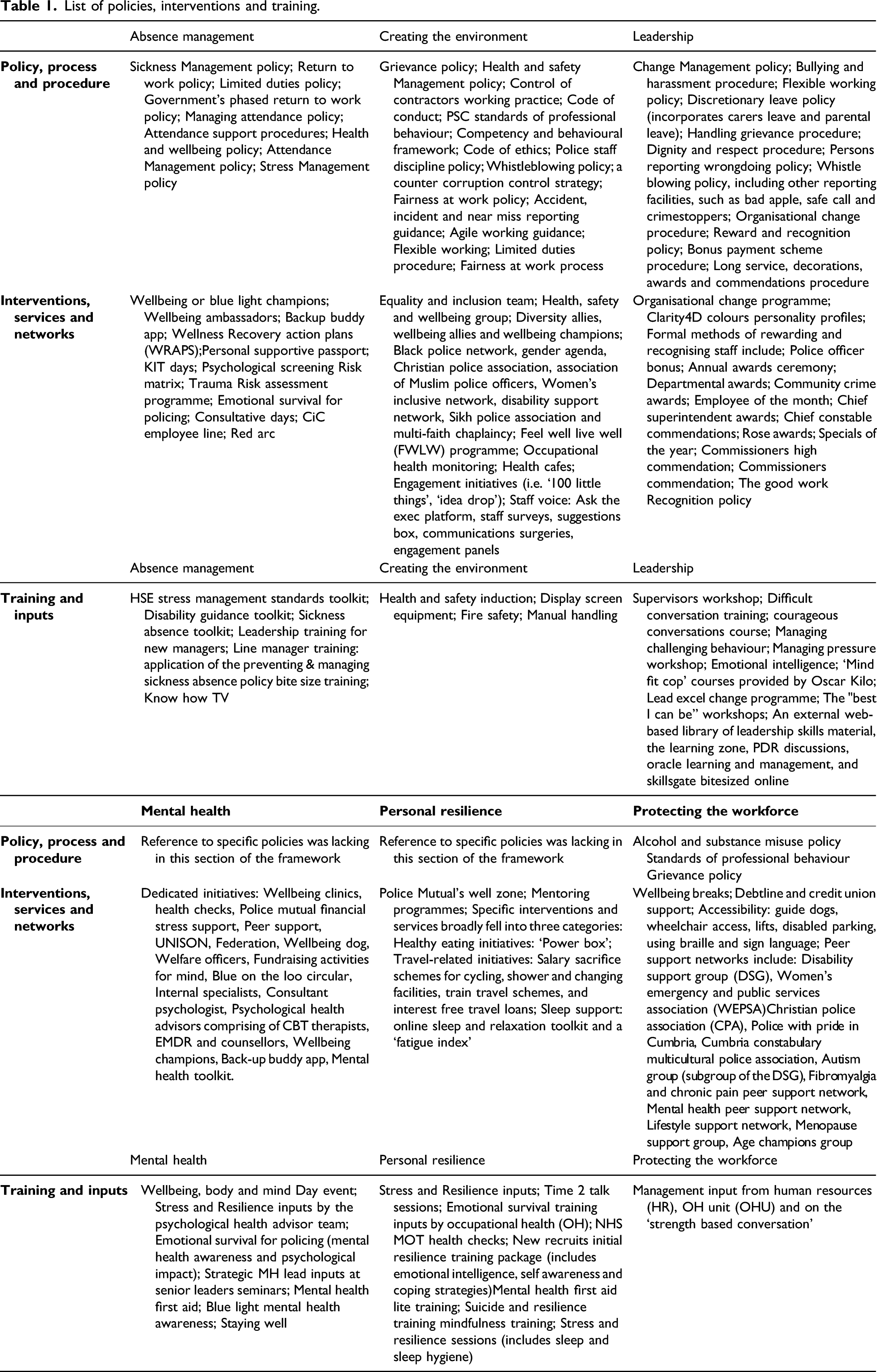
Numerous policies, interventions and training were reported across the frameworks (see Table 1 for a full list). Thematic analyses identified three themes: 1. Risk assessments and psychological monitoring; 2. Empowering and supporting staff; 3. The role and responsibility of management. List of policies, interventions and training.
Risk assessments and psychological monitoring
To support staff in an appropriate and meaningful way, forces utilise various forms of data (i.e. sickness, assault, occupational health [OH] data) to understand the needs specific of their staff; data is broken down ‘across each Local Policing Area and Department as to the types of absence, length, staff type etc’. The use of dashboards was noted as a way to streamline and automate this process, with the ability to highlight ‘trends in the number of cases, reasons for absence and areas of absence’. Trends identified are then discussed at various committees (i.e. the Engagement and Wellbeing Board, Gold Absence Management meetings) to enable a ‘strategic overview’ to be taken, which in turn supports the ability to intervene early and in a targeted manner (AM). Three subthemes were identified: i.) targeted support; ii.) high-risk roles; and iii.) Bradford Index. i. Targeted support: Monitoring trends in absence and sickness assists the ability to intervene early and respond to staff needs in a proactive way; this also enabled forces ‘to target wellbeing interventions to groups who are identified as needing extra support to maintain their health and wellbeing’ (AM). Targeted support was also apparent for the aging workforce: in addition to reasonable adjustments, ‘retirement inputs… take place twice a year’ with reports of a ‘menopause support group that supports females who are menopausal, males that live with those that are coping with menopause and line managers to understand what the symptoms are’ (PW). ii. High-risk roles: Whilst the use of risk assessments was evident within generic roles, it was prominently linked with those in vulnerable or high-risk roles. Inconsistencies were subsequently observed, with some forces implementing psychological monitoring for high-risk roles only, compared to others with a more flexible approach to identifying police officers and staff who need such support: ‘Risk assessments as such are not provided for specific roles but proactive psychological support is in place for those roles with exposure to distressing work e.g. child protection’(AM). Further comments reported how sickness trends were also monitored to determine ‘where the high stress departments are’ (MH). iii. Bradford Index: There were inconsistencies observed in the methods of monitoring data and the use of trigger points. Forces who identified as using the Bradford Index clarified that it was used as an ‘indicator’, as opposed to being ‘used in isolation when reviewing any absence issues’ or leading ‘to performance sanctioning’. On the other hand, concerns were raised in relation to adhering to the score and failing to consider the context: ‘There is empirical evidence that any member of staff triggering Bradford factors is often subject of sanctions no matter what the circumstances’ (AM).
Empowering and supporting staff
Methods are in place to support the individual and meet their working needs, as it was recognised that the organisation ‘has a responsibility to do all that it reasonably can to assist all individuals with a long-term health problem’ (AM). Moreover, approaches to empower staff in their roles and to ‘engage all staff in decisions’ to support their working environment were reported. Generally, active engagement of staff was highlighted in relation to promoting a ‘positive environment’ (CE). The value of rewarding and motivating employees was acknowledged: “Policing is a 24-7 operation. The demands on our people are therefore significant and the public expects its police officers to step forward in situations where everyone else is running the other way. This takes courage and great commitment and that should never be taken for granted, neither should the complexity of the crucial work undertaken by our police staff.”
Four subthemes were reported: i.) a holistic approach; ii.) an inclusive working environment; iii.) psychological and physical wellbeing; and iv.) personal responsibility and accountability. i. A holistic approach: To be effective in the support provided to police officers and staff, ‘a holistic approach to workplace health’ is encouraged. The importance of aligning ‘the physical and psychological capabilities of the employees, along with the needs of the organisation’ is acknowledged. Management work with, and are supported by, other services, such as OH and human resources (HR). Organisations including the Police Federation and Unison ‘are invited to individual case conferences to discuss actions, outcomes, expectations in partnership to ensure a fair and equitable outcome’. This unified approach of various agencies, services and departments aims to provide an informed, appropriate and consistent response to employees (AM). ii. An inclusive working environment: Efforts to take ‘special care’ to ‘create a pleasant and safe working environment’ for all staff are evident. This ranged from an ‘investment in decor, noise reducing tech, ergonomically safe rising desks and chairs, enlarged canteen facilities, [to] a dedicated quiet room with subdued lighting, massage chair and relaxation music’. Staff are ‘encouraged to raise environmental issues’; changes to the working environment based on employee feedback were noted, with reports that one police station was ‘completely re-decorated as staff rightly complained about their working environment’ (CE). iii. Psychological and physical wellbeing: Forces acknowledged that to support personal resilience, work and personal circumstances must be considered to ‘enable a sustainable balance to be attained’. The ‘links between psychological wellbeing and physical wellbeing, productivity and engagement’ are evident. Numerous resources to support physical health were reported in the BLWFs. Online resources are accessible to ‘assist in weight loss and healthy living initiatives’, with ‘informal exercise packages available through Officer Safety Training colleagues’. However, a combination of existing facilities, space and funding impact on the range and type of initiatives available; so, whilst ‘physical activity is encouraged’ it is ‘not supported by the physical environment … [and] it may depend on where you work as to whether you have access to facilities’. In terms of psychological health, more general responses were provided (i.e. compared to the specific physical health-related initiatives). Yet, forces appeared cognisant of this issue, with one force detailing their action plan to ‘evaluate investment in psychological health resources [and] develop specific initiatives to support the workforce’ (PR). iv. Personal responsibility and accountability: All police officers and staff are ‘made aware of the need to create an environment that is conducive to wellbeing’. To ensure: health and wellbeing are promoted; policies and processes are fit for purpose; and, management is held to account, various groups meet at ‘strategic, tactical and local levels’ with ‘representatives from Federation, Unison and Supts Association’ and ‘Occupational Health, HR, Estates [and] Corporate Communications’ (CE). Individual accountability was also noted in terms of maintaining ‘health and fitness’ levels, and developing personal resilience and self-efficacy, such as ‘staff demonstrating that they take initiative in problem solving and making decisions, and asking for feedback to improve their personal effectiveness’ (PR).
The role and responsibility of management
There was a clear responsibility on management to ensure their staff received consistent and continuous support. Attendance management training is provided to managers, so they fully understand ‘their responsibilities in identifying and addressing issues relating to the health and wellbeing of staff members’. Processes placed the ‘emphasis on the line manager to ensure they support their staff whilst understanding and meeting their specific needs’, including the need for management to take ‘the initiative’ to ensure appropriate adjustments are appropriately implemented (AM). Whilst the ‘pivotal role’ senior management ‘play in ensuring the legal obligations in relation to health, safety and welfare in the workplace are met’, the need for management to be available and accessible to staff was also noted (CE). What’s more, the importance of leaders ‘in linking wellbeing to both the organisations corporate strategy and workforce needs’ was recognised, with the common responsibilities of leaders including ‘role modelling, having the right conversations and creating the time and space for these conversations to discuss wellbeing’ (L). Four subthemes were highlighted: i.) support for management; ii.) supporting staff development; iii.) visibility and accessibility; and iv.) reinforcing a positive culture and driving the agenda. i.) Support for management: To subsequently support managers in delivering clear and consistent support to staff, assistance is provided, such as ‘policies, procedures and `how to guides' on dealing with wellbeing issues’, as well as general and ongoing help for line managers and supervisors (AM). There was also evidence of supporting the development of soft skills in line managers. Management ‘receive training prior to promotion which includes an input from HR, OHU and on the Strength Based Conversation to enable them to start these difficult conversations’ whilst creating an environment in which ‘staff can self-disclose any issues they may have’ (PW). ii.) Supporting staff development: A core responsibility of leaders is to support the development of their staff appropriately and effectively. This requires a ‘first-hand’ understanding of ‘how their staff are coping’. Working together closely fosters ‘greater trust between staff and supervisors which only makes the team stronger and more resilient’. To support their staff, managers are expected to: ‘Provide regular and continuous feedback both informally and formally via performance reviews … therefore developing staff and managing unsatisfactory performance’. It was also deemed important for line managers to ‘manage the expectations of individuals taking into account personal ability, development needs and likely opportunities within their role or another role’ (L). iii.) Visibility and accessibility: It is evident that processes are being implemented to support the visibility and approachability of senior management, such as ‘Chief officers blog regularly’, ‘supervisors are encouraged to take time and speak to employees’, and ‘regular meetings with line manager/supervisor’. Networks, forums, working groups and ‘communication surgeries’ offer an opportunity to feedback communication from senior management, whilst also providing staff with a ‘voice’ (AM). Moreover, ongoing work was noted ‘to embed a better 1-2-1 culture’ between management and their staff (MH). iv.) Reinforcing a positive culture and driving the agenda: Multiple forces commented on members of senior management engaging with wellbeing boards and acting as Wellbeing Champions ‘to support wellbeing on a wider basis’. The strengths of management ‘leading by example’ were thought to assist in reinforcing a positive culture throughout the organisation (AM). A ‘significant drive from Senior leaders to put wellbeing at [the] forefront’ was also reported, although concerns were raised in relation to the consistency of the message (L).
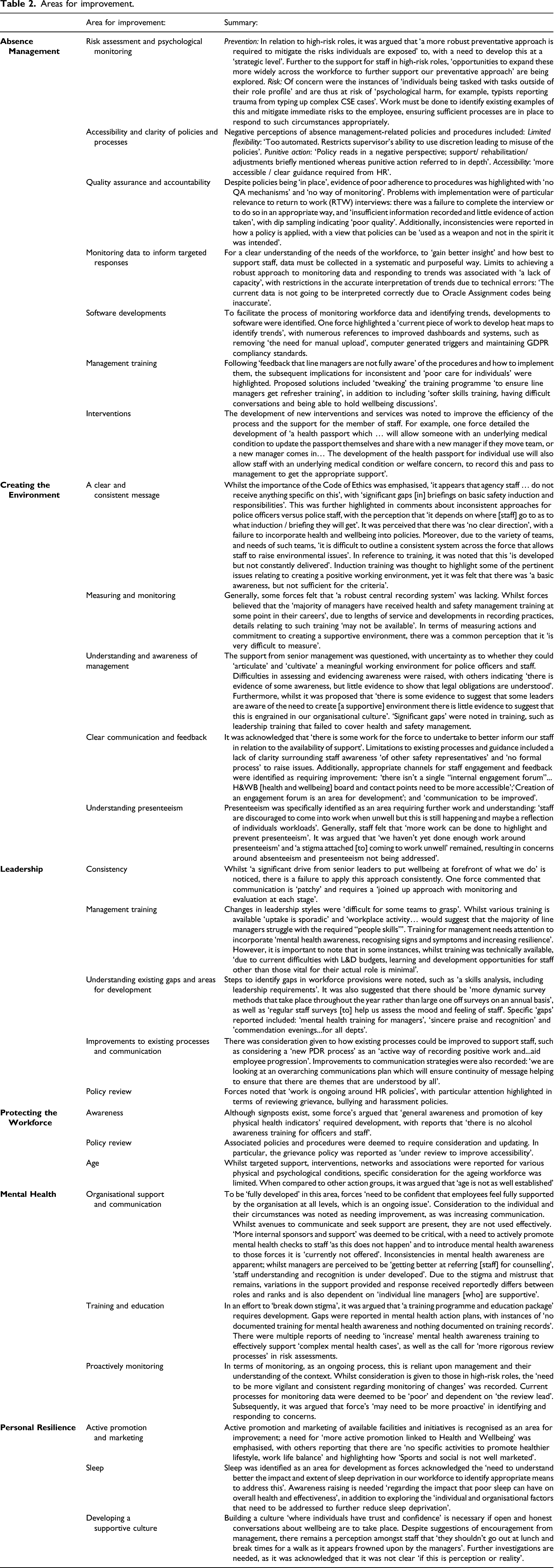
Areas for improvement
Areas for improvement.
Discussion
To understand the current wellbeing strategies in place, the progress that has been made nationally and the areas of wellbeing that UK forces deem to require development, a total of 34 BLWFs were analysed. Findings from the review indicated developments in police wellbeing; based on the development score of the overall sample, forces were perceived to be ‘fully developed’ with the levels of development of sections within the framework falling within the expected development levels: absence management was the most developed section of the framework and personal resilience remained to be the most underdeveloped (see analysis of earlier BLWF data, Phythian et al., 2021). Whilst methodological limitations prevent a statistical comparison between the 2018 and 2020 BLWF data, descriptive statistics indicate a development in national police wellbeing (i.e. total development score mdn = 212.50 and = 221.00, respectively).
The qualitative analysis reflected the overall development levels presented in the quantitative analysis; absence management and leadership contained detailed accounts of multiple policies, procedures, initiatives and services, yet this is much more limited when reviewing the personal resilience and protecting the workforce sections. Moreover, physical health appeared to be better understood with a wealth of provisions in place; whilst psychological support was evident, this was somewhat sporadic. In comparison to the BLWF data explored in 2018 (Phythian et al., 2021), references to using an evidence-base and adopting research-informed approaches were evident, with forces engaging in self-assessment to identify areas for improvement. Whilst developments are in progress, inhibitors to a positive wellbeing environment remain, such as culture, management support and awareness, and negative perceptions, as well as sporadic adherence to and application of organisational processes (i.e. RTW interviews).
Progress is promising. Yet, in a constantly evolving and increasingly complex society, it is imperative that the support in place for police wellbeing continues to develop in a way that can be sustained nationally. As discussed in the literature review, culture and stigma constitute barriers to care and recovery from psychological work injuries for the police (Bell and Eski, 2016; Velazquez and Hernandez, 2019); it is critical to value staff and ensure they are fully supported when fulfilling their roles. Therefore, it is essential that management have the necessary awareness and emotional intelligence in response to wellbeing (e.g. Houdmont et al., 2020). Areas for improvement include consistency in the application and delivery of policy and processes, management training, developing a supporting culture and clear signposting; generally, uncertainties remained in how to achieve some elements set out in the frameworks in practice. There was also a need for: increased attention to quality assurance, improved understanding of management (compared to staff more generally), and more consideration given to sleep and the ageing workforce.
Recommendations and implications for practice
Evidence-based and targeted approaches
During the short time period since the launch of OK and the NPWS, developments in activities and the promotion of national conversations surrounding police wellbeing are evident. Whilst there are increasing examples of evidence bases being consulted and used to inform future actions, there is still limited clarity on which initiatives are informed by research and which have undergone evaluation. Such resources and evidence on ‘what works’ are available via OK. Measures of engagement with OK and the various guidance should be collected; this would assist in understanding the ongoing awareness of UK policing, as well as identifying trends and implementing an appropriate response (i.e. does an increase in engagement with personal resilience resources align with force perceptions of being underdeveloped? Could additional evidence-based guidance assist?).
With the increasing body of knowledge available, ‘recommended’ approaches (i.e. interventions, strategies) and ‘good practice’ should be actively shared with forces, with the view to achieving a consistent and informed national stance, saving valuable funding, time and resources. Consequently, this would support in clarifying the inconsistencies in the policies and interventions that are reported. It is currently difficult (without further scrutiny) to determine if the policy in one force is the same as that in another force, albeit with a different policy name. However, whilst national consistency supports sharing best practice and the development of a unified approach, force-specific nuances and needs are acknowledged.
A consistent approach to completing the BLWF
Inconsistencies in the use and completion of the BLWF were observed. To evaluate and compare progress, and to identify and share best practice, consistency in the data collected would be useful. For example, clarification as to the desired type of response would reduce the variations in the data, such as one force leaving the response blank, another responding with a ‘yes as per policy and process’ and another going into detail surrounding the procedures in place. Differences in individual force interpretations were also evident in terms of defining ‘underdeveloped’, ‘in development’ or ‘overdeveloped’, as well as variations in the evidence that was appropriate and supportive. Repeated responses were also observed in multiple statements and across sections. Whilst it is understandable that there will be a degree of crossover in relevant processes, for example, ensuring the expected responses are clear with a distinction between the statements and sections would reduce repetition and support in the provision of relevant content. Additionally, when completing the frameworks, uncertainty in how to answer the question and how to evidence it was noted: the provision of practical guidance may aid in clarifying to practitioners what is required. A consistent and guided approach to completing the framework would enable more robust measures for peer assessment and inferential analyses to be applied.
Organisational and individual perspectives of wellbeing
As recommended previously (see Phythian et al., 2021), it is critical to align organisational and individual perspectives to achieve a shared understanding of wellbeing and success. Whilst improvements to the development levels across multiple forces were apparent, there are indications that individual-based wellbeing remains less developed (e.g. personal resilience), compared to institutional processes that are seemingly better developed (e.g. absence management). This questions the wider implications, as to whether the organisation’s priority is an accountable workforce rather than staff wellbeing. If the organisation deems the presence of policy to represent development, despite the adverse impact of the policy on the employee, there will be difficulties in effectively supporting the workforce. This is evident in the completion of the BLWFs, with some responses identifying a policy and others detailing specific staff support.
Limitations
Inconsistencies in the frameworks and challenges to evaluating progress persist, such as missing data and variations in the level of detail provided. Some forces failed to provide a self-assessed level of development for individual statements within the framework; for analytical purposes, the current research categorised forces with missing levels of development as ‘underdeveloped’, yet caution must be taken as the reason for failing to select a level of development is unknown. Additionally, due to the specificity of the statements within the framework, much of the content surrounding the themes was descriptive. This resulted in descriptive, as opposed to analytical, content. Additionally, the variations in level of detail provided resulted in difficulties identifying specific elements, and themes, of wellbeing applied and acknowledged by forces. There was a degree of overlap in the content provided in each of the six sections; it was not clear which overlap represented a ‘natural overlap’ or ‘relationship’ in the data, and which was indicative of a lack of a clear understanding of how one section is distinct to another (i.e. between personal resilience and protecting the workforce).
Conclusion
Recent national developments have supported in driving the wellbeing agenda forward. Whilst awareness of wellbeing is increasing, and open and honest conversations are taking place, progress is still to be made. Developments in national police wellbeing should be mindful of existing initiatives and training that may be available, as well as those which have undergone evaluation, whilst also being cognisant of individual employee needs and perspectives to ensure they are aligned to the organisation. Considering the areas of improvement identified by forces, future developments of police wellbeing should consider: how to support the implementation of evidence-based, targeted approaches; how to guide practitioners in completing the BLWF, in a consistent way that would be conducive to supporting peer review, development of wellbeing and analysis of progress; and how to align the perspectives of the individual to the organisation, and to capture this data in the BLWFs.
Footnotes
Acknowledgements
Special thanks to academics and practitioners who have supported and provided data for this study, particularly the National Police Wellbeing Service team and Oscar Kilo.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research was commissioned by the National Police Wellbeing Service.