
Abstract
To understand how resilient adolescents adapt to adverse situations, this study examined resilient adolescents and their coping strategies. Resilience is the phenomenon characterized by good outcomes despite serious threats to adaptation and/or development. The current study aimed to identify the coping strategy profiles that distinguish a resilient group from three other groups—struggling, competent, and vulnerable—specifically to differentiate the resilient group from the competent group. Descriptive discriminant analysis results indicated that resilient adolescents simultaneously utilized not only problem-focused but also the emotion-focused coping strategies. The competent group primarily used problem-focused coping, while the struggling group primarily used emotion-focused strategies. Finally, the vulnerable adolescents used neither problem-focused nor emotion-focused strategies. Practical implications of the results were discussed to guide professionals.
Introduction
Living as an adolescent in South Korea is associated with many difficulties. Academic demands and competition are high for adolescents, who have little time for sleep, let alone leisure activities (Lee & Larson, 2000). About 73.2% of Korean adolescents receive private education after school to keep up with competition in school (Ministry of Health and Welfare, 2013). Needless to say, life satisfaction among Korean adolescents is the lowest among OECD countries. Around half (50.4%) of Korean adolescents in 2014 reported that they were unsatisfied with their school lives and 61.4% reported suffering from stress. Finding it difficult to cope with their stress, 9.2% of adolescents turn to smoking and 16.7% to alcohol. Some adolescents (about 7.9%) even thought of suicide as the only solution. About 11% of adolescents run away from home due to conflict with parents (Statistics Korea, 2015).
Daily stress also contributes to difficulty in effective coping and elevated aggression in adolescents (Jin, Park, & Bae, 2011). As a result, prevalence of school violence in South Korea has garnered considerable public attention (Lee, Lim, Lee, & Oh, 2009). In 2013, about 17.1% of adolescents reported that they had teased others and 9.0% had bullied others by ostracizing them (Ministry of Health and Welfare, 2013). In order to deal with these maladaptive behaviors among adolescents, researchers (Baek & Moon, 2009; Park & Kim, 2004; Shin, Shin, Kim, & Cho, 2010) have identified a number of contributing factors. This research, directed at the phenomenon of adolescent delinquency, has yielded integrated models that include personal, family, peer, and school variables. The common feature of recent integrated delinquency models is that they are psychosocial, that is, they show that a set of individual factors (e.g., gender, academic achievement, and self-concept) interacts with contextual or social factors (e.g., peer affiliation, parental involvement, and school bonding) to explain delinquency (Calhoun, Glaser, & Bartolomucci, 2001; Kerpelman & Smith, 2005; Ronis & Borduin, 2007). In this context, risk factors to delinquency were identified. While investigating the interactions between individual and environmental risk factors in adolescents’ delinquent behaviors, researchers came across nondelinquent youths who had experienced risk and challenges in their childhood history (e.g., parents’ divorce and poverty) but had been able to overcome those obstacles (Dyer & McGuinness, 1996; Luthar, Cicchetti, & Becker, 2000; Masten, 2009; Masten & Powell, 2003). They were called “resilient adolescents,” cases in which risk factors did not hinder the individual’s successful adaptation.
Resilience refers to “the phenomena characterized by good outcomes in spite of serious threats to adaptation or development” (Masten, 2001, p. 228). Most studies (Masten, 2009; Rutter, 2006; Zautra, Hall, & Murray, 2010) have reported that the resilience of an individual grows by interacting with the environment and the growth promotes well-being or protects individuals from being overwhelmed by risk factors. Accordingly, several researchers (Dumont & Provost, 1999; Kim, Lee, Yu, Lee, & Puig, 2005; LaFromboise, Hoyt, Oliver, & Whitbeck, 2006) have studied how resilient adolescents overcome difficult situations, such as maltreatment, catastrophic life events, and urban poverty.
Coping is a conscious process that an individual engages in to manage a problem and regulate emotions. Rutter (1990) argued that successful engagement with adversity generates protective coping mechanisms. Coping strategies influence how an individual manages a stressful event (Lazarus & Folkman, 1984). Generally, coping strategies fall into three types: problem focused, emotion focused, and avoidance (Endler & Parker, 1990a, 1990b). Using the problem-focused coping strategies, the individual faces his/her problem head on (i.e., the person takes action to fix or resolve the problem). Using emotion-focused coping strategies, the individual tries to diminish his/her negative emotions due to stress (e.g., the person watches TV as a distraction). Avoidance coping strategies involve evading both negative emotions and finding solutions to problems, in the hope that the problem will disappear on its own (e.g., the person puts off an important task because it evokes discomfort).
Most studies (Dumont & Provost, 1999; Higgins & Endler, 1995; Steinhardt & Dolbier, 2008) have indicated that problem-focused coping strategies are associated with better outcomes (e.g., less psychological dysfunction), whereas emotion-focused and/or avoidance coping strategies are associated with psychological dysfunction. However, some studies (Bonanno, Noll, Putnam, O’Neill, & Trickett, 2003; Braverman, 1992; DiPalma, 1994) reported that using avoidance and emotion-focused coping strategies in the active period of the stressful situation was more adaptive than using other coping strategies. For example, Worthington and Scherer (2004) reported that using emotion-focused coping strategies (e.g., forgiveness) is the only realistic option when the source of stress is uncontrollable. Here, the individual can use these strategies to reduce health risks and promote health resilience. Likewise, Coifman, Bonanno, Ray, and Gross (2007) reported that repressive coping, one of the emotion-focused coping strategies, served a protective function and promoted individual resilience in times of extremely negative events such as a death of a beloved person.
Traditionally, researchers took a person-focused research on resilience by identifying resilient individuals using the diagnostic model of Masten and Reed (2002), with risk level and adaptation level as key criteria. Based on levels of risk and adaptation, Masten and Reed categorized groups as follows: (a) resilient, consisting of adolescents who have adapted well despite high-risk levels; (b) struggling, adolescents with high-risk levels but having difficulty in successful coping; (c) competent, including adolescents who have adapted well, but have experienced low risk; and (d) vulnerable, including adolescents who have difficulty to adapting despite experiencing low risk. Many researchers (Masten et al., 1988; Nathan, 1991; Ungar, 2015) caution against using negative term as “maladaptive” due to the possibility of labeling effects. However, most resilience research started from looking into the strengths of at-risk individuals in order to alter the deficit-based focus on damages and loss experienced (Werner & Smith, 1992). So the purpose of categorizing individuals was to find distinctive characteristics of individuals who recovered from adversity (O’Leary & Ickovics, 1995) and look for mechanisms that could be used to build resilience in other groups as well. As an effort to prevent labeling effects, the current study used the word “struggling” to reflect the difficulty in adaptation and attempts to overcome difficulties. Liebenberg et al. (2016) also reported that these struggling children and adolescents may also have “hidden” strengths that are not easily detected by significant others.
Several studies (Kim et al., 2005; Martinez-Torteya, Bogat, Eye, & Levendosky, 2009) have examined the protective factors that differentiate the resilient group from the other three groups. However, most studies (Masten & Obradovic, 2006; Masten et al., 1999) have reported strong similarities between the two highly adaptive groups (i.e., the resilient and competent groups), despite their divergent adversity exposure, and also striking differences between the resilient and maladaptive (struggling) groups, despite their shared adversity exposure. Few studies reported on differences between the resilient and competent groups on several protective factors (e.g., self-esteem). Some researchers assumed that resilient adolescents might use different coping strategies from those competent adolescents use in adverse situations (Braverman, 1992; Coifman et al., 2007; DiPalma, 1994). They stated that maladaptive coping strategies (e.g., avoidance, emotional, and repressive coping strategies) which usually impede resilience could serve a protective function and promote individual resilience at times.
This study aimed to identify unique coping strategy usage of the resilient group that differentiates them from the other three groups (i.e., competent group, struggling, and vulnerable group) and especially from the competent group. Using descriptive discriminant analysis (DDA), the study sought to identify the extent to which the four groups differed and which coping variables (i.e., problem-focused, emotion-focused, and avoidance coping strategies) were associated with these group differences. It was hypothesized that resilient adolescents would utilize problem-focused coping mechanisms and would be less likely to utilize emotion-focused and avoidance coping strategies. This study could be helpful for understanding how the resilient adolescents cope with difficult situations.
Method
Participants
Study participants (N = 1446) were voluntarily recruited from middle and high schools in South Korea. This sample was composed of 640 middle school students (Grades 7–9, 44.3% of the total population) and 806 high school students (Grades 10–12, 55.7% of the total population). In middle school, “7th grade” indicates students are at least 13 years of age. Likewise, “10th grade” in high school means students are 18 years of age maximum. Therefore, at the time of data collection, the participants’ age range was around 13 to 18 years (SD = 1.5). There were 725 male students, 50.1% of the sample, and 721 female students, 49.9% of the sample. Regarding developmental challenges at home, 120 students (9.3%) were from single-parent families and 35 students (2.4%) had experienced a parent’s death. Concerning economic challenges, 175 students (12%) had unemployed parents and 365 students (25%) experienced economic difficulties at home. In regard to social challenges, 342 (23.7%) students had violated school rules or had disciplinary action. There were 209 students (14.5%) who smoked or drank alcohol, while 97 students (6.7%) were involved in gang activity. Approval from the institutional review board was obtained and respondents provided informed consent to participate in this study. Participation in the study was strictly voluntary. The questionnaire consisted of 152 items and students were given around 10 minutes to respond to the questionnaire. Students were allowed 15–20 minutes of recess time in class to participate in the study. Students who needed more time were allowed an additional 5–10 minutes after class. Missing values for each item ranged from 0.1% to 3.5% of the whole sample. To deal with missing values, we employed the expectation-maximization algorithm method.
Measures
Risk factors
The Risk Factors Scale (Kim, 2004) is a self-report questionnaire designed to measure risk level. This scale divides risk factors into four areas (individual, familial, social support, and community) and risk events into two types (uncontrollable and controllable). A panel of eight experts in the counseling field examined the representativeness of the items. They also distinguished uncontrollable risk (22 items, e.g., parent divorce and mental disorder) events from controllable risk events (28 items, e.g., smoking, low grade point average). The questionnaire comprised 50 items rated on a four-point Likert scale ranging from 0 (No experience at all) to 3 (Severe experience of adversity). Participants reported whether they had experienced such risk events within the past two years of their lives and rated the seriousness of the event. Items include “Have you had an accidental injury within the past two years?” and “Did your parents get divorced within the past two years?” for uncontrollable risks and “Did you violate school rules within the past two years?” and “Did you smoke or drink alcohol within the past two years?” as examples of controllable risks. Due to the low score of uncontrollable event sum scores (M = 3.14, SD = 4.64) and since even controllable events could be overwhelming (Johnson, 1986), this study used the overall risk experience to divide groups. The overall risk level was computed by summing the item ratings into a single score, with higher scores indicating higher risk. The scree plot also indicated that a single factor best represented the measure. In Kim’s 2004 sample, the reliability coefficient was .93 for all items, .86 for controllable risk events, and .73 for uncontrollable risk events. Cronbach’s alpha for all items was .90, .86 for controllable risk events and .79 for uncontrollable risk events in this sample. McDonald’s coefficient omega was .94 for the overall scale, .95 for controllable risk events and .88 for uncontrollable risk events.
School adaptability level
Kim (2004) derived this self-report measure of school adjustment from several other scales (Cho, 1984; Epstein & MacPartland, 1976; Garlington, 1984; Kim, 1993; Moon, 2001). Its 50-item scale has three subscales: academic adjustment (20 items), social adjustment (20 items), and school environment adjustment (10 items). The academic adjustment subscale examines academic performance (sample item: “I listen carefully in class.”). Social adjustment subscale items assess whether the individual follows school rules and maintains relationships with teachers and classmates (sample item: “I follow school rules.”). School environment adjustment refers to the student’s satisfaction with school life (sample item: “I am enjoying school life.”). Participants responded to each item according to their school life on a 5-point Likert scale ranging from 1 (Strongly disagree) to 5 (Strongly agree). Since this study looked on the general adaptability level, the total score was used as a measure to divide groups. All 50 items had high internal consistency (Cronbach’s α = .93) and .91 for academic adjustment, .85 for social adjustment, and .87 for school environment adjustment. McDonalds’ coefficient omega was .97 for the overall scale, .97 for academic adjustment, .94 for social adjustment, and .94 for school environment adjustment.
Coping strategies
The Coping Inventory for Stress Situations (CISS; Endler & Parker, 1990a, 1990b) is a 48-item measure for determining typical patterns of coping strategies for stressful situations. The present study used the Korean version (Kim, 2001) of the CISS. The Korean version excluded 10 items from the original scale because they did not correspond to the coping strategies they ought to describe when translated in Korean. Respondents are asked to indicate how much one engages in activities stated in the items in the experience of a difficult, worrying, or distressing situation on a five-point Likert scale ranging from 1 (Not at all) to 5 (Very much). This measure has three subscales: problem-focused coping (16 items; sample item: “Use my time better”), emotion-focused coping (11 items; sample item: “Become tense”), and avoidance-focused coping (11 items; sample item: “Go to a party”). Using problem-focused coping strategies mean applying solving strategies to a stressful situation. Emotion-focused coping strategies mean engaging in emotional behavior, such as blaming themselves or ruminating, in stressful situations. Individuals using avoidance-focused coping strategies tend to avoid and distract in stressful situations. The Korean version (Kim, 2001) of the CISS was validated as a three-factor structure and reported high internal consistency for all 38 items (α = .89) as well as for each subscale: problem-focused coping (α = .89), emotion-focused coping (α = .84), and avoidance-focused coping (α = .83). Also, several Korean scholars (e.g., Kim & Chon, 1993; Lee, 2012; Masten, 2001) reported that problem-focused coping strategies are related to positive psychological variables (i.e., subjective well-being), whereas emotion-focused and/or avoidance coping strategies are associated with negative psychological variables (i.e., depression). In this sample, Cronbach’s alpha for all 38 items was .94, .93 for problem-focused coping, .88 for emotion-focused coping, and .86 for avoidance-focused coping subscales. McDonalds’ coefficient omega was .98 for the overall scale, .99 for problem-focused coping, .95 for emotion-focused coping, and .94 for avoidance-focused coping.
Data analysis
The data were analyzed using SPSS 21.0. First, the participants were divided into four groups by adaptation and risk: (a) the resilient group were those with high adaptation (school adaptability) and high adversity (risk factors), (b) the struggling group comprised those with low adaptation and high adversity, (c) the competent group comprised those with high adaptation and low adversity, and (d) the vulnerable group comprised those with low adaptation and low adversity (see Figure 1). We derived this classification from the diagnostic model of Masten and Reed (2002), by classifying individuals into groups using adaptation and adversity as two axes. This approach was previously used by Shaffer, Coffino, Boelcke-Stennes, and Masten (2007) to distinguish resilient families. Kim and Kim (2004) also used the same risk event and school adaptation scale to differentiate resilient adolescents. This study used the mean of risk event total scores (M = 18.06) to divide participants into high- and low-risk groups. We also divided participants into high- and low-adaptation groups, by mean of total school adaptation scores (M = 156.14). In Kim and Kim’s (2004) study on adolescents, around 31% reported that they experienced no risk events, and the cutoff score for high-risk level was similar to that of the sample used in this study. This method was also adapted in Buchanan’s (2008) and Kim, Seo, and Jo’s (2005) study. Next, using DDA, we examined how the three coping variables differentiated the four groups. To control for demographics, gender was entered into the discriminant analysis along with the three coping variables.
Theoretical classification of groups according to Masten and Reed (2002)’s classification.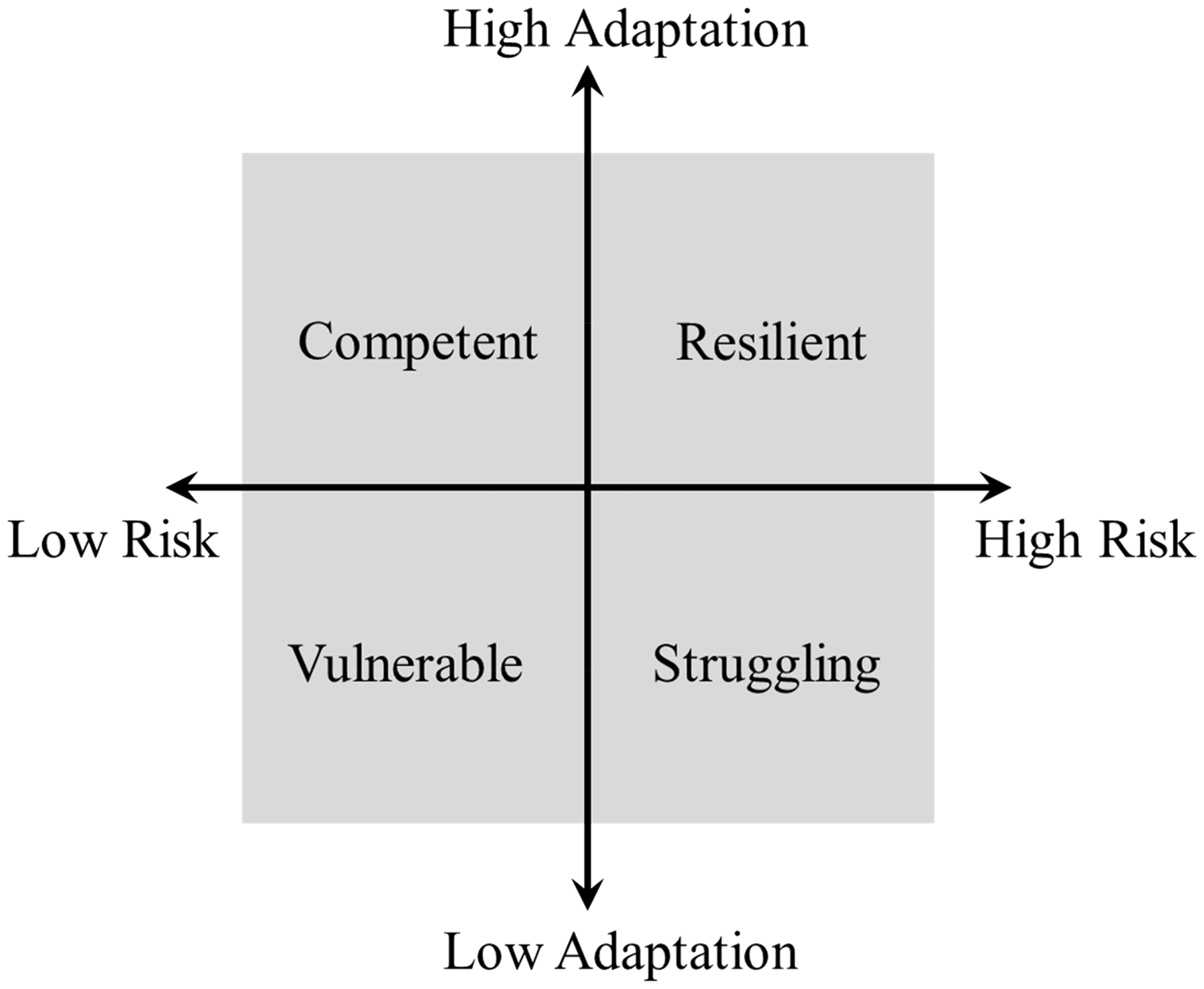
Results
Means, standard deviations, and correlations among research variables.
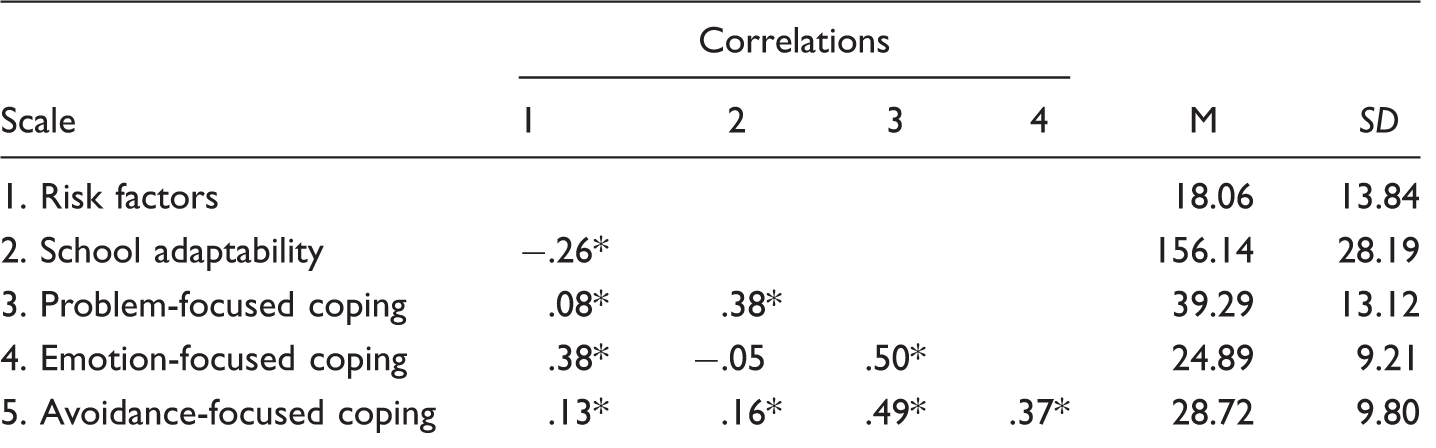
p < .01.
Means and standard deviations of the research variables for each group.
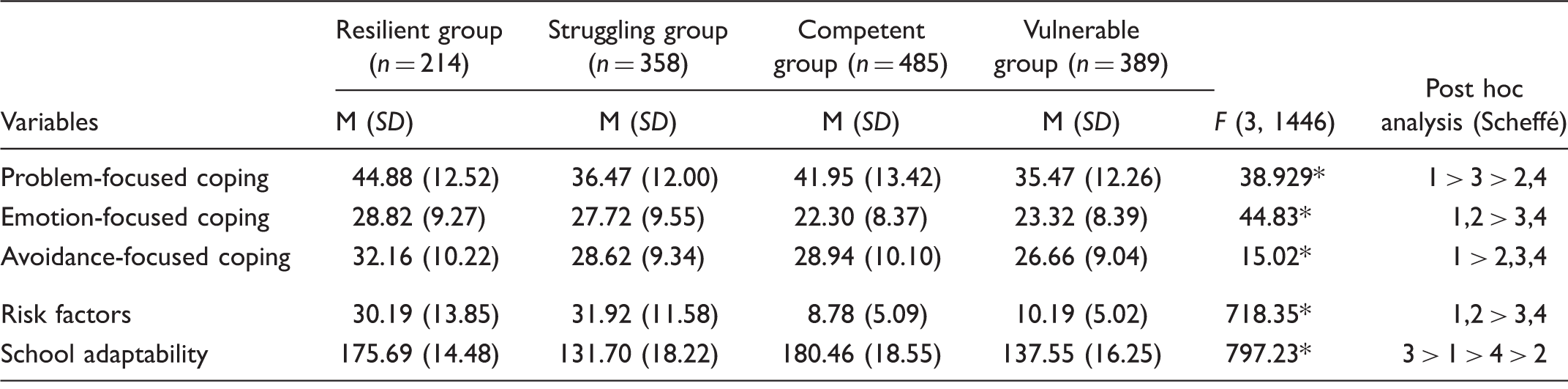
p < .01.
Wilks’ Lambda and canonical correlations for groups.

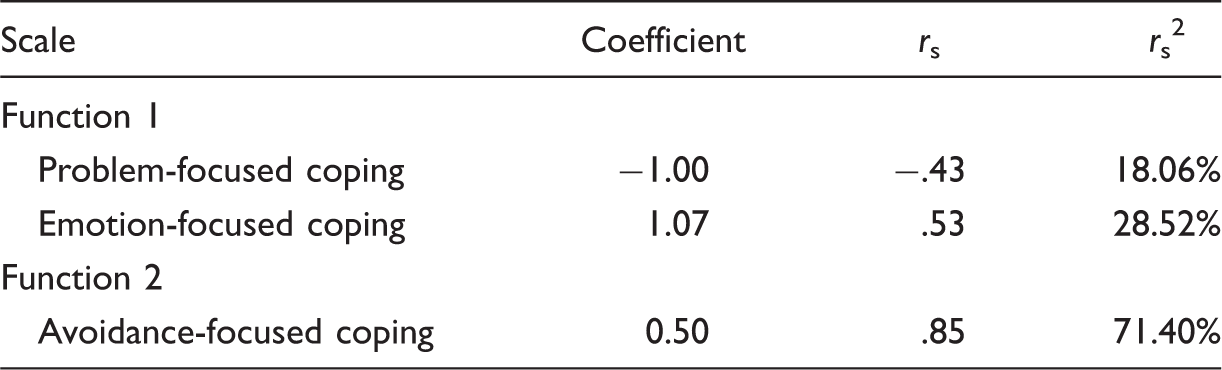
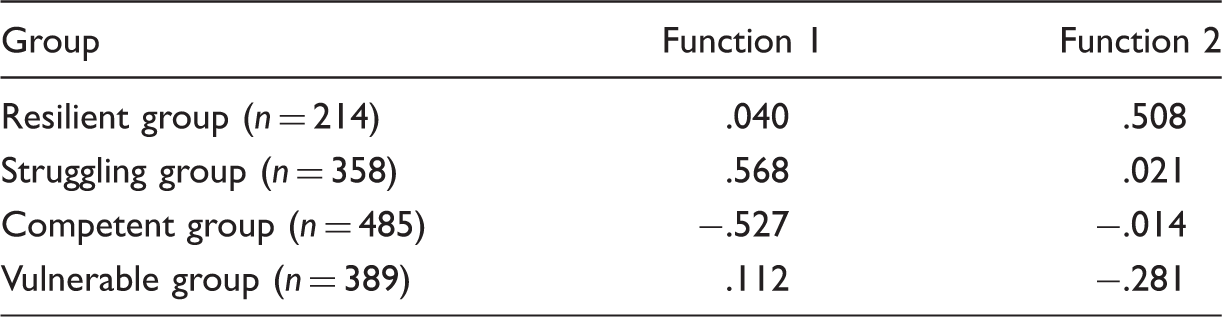
Standardized discriminant function and structure coefficient for the groups.
Group centroids.
Discussion
The current study aimed to identify the coping strategy profiles of resilient adolescents and identify characteristics of resilient adolescents by comparing them with other groups. While previous researchers (Beasley, Thompson, & Davidson, 2003; Campbell-Sillsa, Cohana, & Stein, 2006) looked for differences in each coping strategy independently, the current study attempted to distinguish profiles consisting of all three coping strategies using DDA.
Of 1446 students, only 214 (14.8%) students were classified into the resilient group. These students reported experiences regarding risk events (e.g., substance use, interpersonal problems, academic stress, family conflicts/breakdown) but still maintained focus on their school life (e.g., concentration in class, good relationships with friends and teachers) as did the competent group which comprised 24.76% of the whole sample. On the other hand, 747 students (51.7%) were classified into either the struggling group (n = 358, 24.8%) or the vulnerable group (n = 389, 26.9%). Struggling and vulnerable groups had difficulty with school life (e.g., receiving disciplinary action, less involvement in school activity) while being subject to different risk severity. The results of this study were consistent with statistics that show more than half of Korean students have difficulty with adjusting to school life and suffer from stress (Statistics Korea, 2015). Culturally, eastern Asian nations (Korea, Japan, and China) tend to emphasize the competition among students for academic achievement. Cultural emphasis on academic achievement is closely related with Korean adolescents’ psychological maladjustments such as depression and suicidal thoughts (Jeon, 2007). For future studies, it is important to consider cultural factors that affect students’ adaptation.
The DDA results indicated that resilient group employed not only problem-focused but also emotion-focused coping strategies, simultaneously. On the other hand, the competent group primarily used problem-focused coping and the struggling group primarily used emotion-focused strategies. Finally, the vulnerable group used neither problem-focused nor emotion-focused strategies. This evidence supports the benefits of using a flexible and rich repertoire of coping strategies and choosing which strategy adequately fits the demands of complicated, traumatic situations (Punamäki, Mhammed, & Abdulrahma, 2004; Rutter, 2000; Saarni, 1999; Schnider, Elhai, & Gray, 2007).
Previous studies have provided inconsistent evidence on how problem-focused and emotion-focused coping strategies affect children’s mental health. Several researchers have suggested that coping effectiveness may depend on the nature of the stressors (Band & Weiss, 1988) and that the effectiveness of some strategies is stressor-specific (Rutter, 2000). Indeed, some coping strategies previously known as ineffective worked for children in some situations (e.g., war zone areas) (Band & Weiss, 1988; Rutter, 2000). These results indicate that there may not be a single best coping strategy. Researchers agree that promoting just problem-focused strategies may not be sufficient, depending on the characteristics of the situation. Likewise, Punamäki et al. (2004) suggested that diverse, even opposing, coping responses might be effective at protecting children’s mental health in life-endangering situations.
Apparently, the nature of traumatic events frequently determines the choice of an effective coping strategy (e.g., reconstructing, active affiliation, passivity, and denial). For example, family-related difficulties, such as divorce and neglect, are associated with low reconstructing, whereas economic hardship often occurs with low active affiliation. In addition, active affiliation moderates between exposure to traumatic events and post-trauma symptom disorder, whereas denial moderates between exposure to traumatic events and aggressive symptoms. Therefore, considering that resilient groups do well at recovering from difficult and painful experiences, we could suggest that simultaneously utilizing two coping strategies (i.e., problem-focused coping and emotion-focused coping) would be more helpful for children recovering from hardships and would thereby increase the possibility of flexible coping skill adaptations, suitable to certain hardships.
Because both the resilient and competent groups utilized problem-focused coping strategies, it can be inferred that this type of strategy might be particularly useful. This is consistent with conclusions from previous studies that the use of problem-focused coping strategies is negatively correlated with children’s emotional and behavioral problems (Compas, Malcarne, & Fondacore, 1988; Compas, Worsham, Ey, & Howell, 1996). On the other hand, the effect of emotion-focused strategies seems somewhat confusing since the resilient group uses them as much as struggling and vulnerable groups do. In fact, this result does not support findings from previous studies. Unlike problem-focused coping strategies, which have demonstrated relatively consistent positive effects, the role of emotion-focused coping strategies are somewhat mixed and require further investigation.
The finding that resilient adolescents had emotion-focused coping skills is consistent with Braverman’s (1992) results. Braverman reported that emotion-oriented coping mechanisms could be beneficial in certain contexts because emotional venting, rather than repressing emotional states or reactions, is useful. On the other hand, researchers have found that the resilient group was not alone in its use of the emotion-focused coping strategies. Both struggling and vulnerable adolescents share the same coping mechanism. In conjunction with the above observations, studies find emotion-focused coping correlates positively to children’s behavioral problems (Compas et al., 1996), and that traumatized children typically utilize emotion-focused, avoidant, and distractive coping strategies (Tolan, Guerra, & Montaini-Klovadahl, 1997). With regard to this surprising result, perhaps the view of Schnider et al. (2007) sheds some light. Schnider and colleagues stated that using emotion-focused coping strategies without engaging in problem-focused behavior is maladaptive, whereas emotion-focused coping while engaging in problem-focused behavior is adaptive. Apparently, emotion-focused coping may help one find balance in daily life activities immediately after a crisis; however, heavy reliance on emotion-focused strategies can ultimately lead to mental health problems in the long run (Holahan & Moos, 1987). Several researchers (Almqvist, 2000; Bat-Zion & Levy-Shiff, 1993; Montgomery, 1998; Punamäki, 2000) accounted for this by explaining that at-risk children tended to be less constructive and depended more on emotion-focused coping mechanisms, such as denial, because exposure to trauma preoccupies their resources (Eth & Pynoos, 1985; Punamäki & Puhakka, 1997; Saarni, 1999). Vitaliano, Maiuro, and Russo (1987) addressed this issue, commenting that the use of emotion-focused coping could be effective as long as the use of problem-focused coping is more pervasive than emotion-focused coping. In this sense, the study findings increase the importance of encouraging at-risk adolescents to utilize emotion-focused coping strategies along with problem-focused coping strategies.
The present study also suggests that teachers, counselors, and parents of at-risk students in South Korea should encourage and instruct students various coping strategies together. More specifically, this study suggests that assistance is needed for adolescents to move forward from just using emotion-focused coping strategies and learn how to utilize problem-focused coping strategies together when faced with traumas and life challenges. In fact, one study estimates that 50%–60% of the general population has experienced potentially traumatic events or hardships (Kessler, Sonega, Bromer, Hughes, & Nelson, 1995), and another finds 67% of young college students have experienced comparable traumatic events (Bernat, Ronfeldt, Calhoun, & Arias, 1998). The risks of traumatic events such as divorce, separation, school violence, and unexpected death of friends or family may be impossible to avoid completely. Therefore, we assert that adolescents’ effective coping skills could be improved by helping them learn to use various coping strategies together. In this sense, encouraging adolescents to learn to apply various and flexible coping skills may help prevent them from being traumatized and, furthermore, may be useful for recovery from overwhelming challenges.
Several limitations apply. One shortcoming concerns group divisions. Participants were categorized by mean adaptation and adversity levels, so that each group resembled the group divisions of Masten and Reed (2002). In the process, individuals who scored around the cut-off score could be categorized into different groups although they showed similar characteristics. Accordingly, further research is needed to classify the groups into the 30% with higher adaptation or higher adversity scores and the 30% containing those with lower adaptation or lower adversity scores, to make each group better resemble the theory of Masten and Reed (2002). Luthar and Zelazo (2003) noted that in person-centered analyses on resilient individuals, there is a lack of consensus on the criteria to classify some individuals as “resilient” while others are categorized as “non-resilient,” which can result in an arbitrary model. They emphasized that when discerning resilient individuals against others, it is less important whether an individual is labeled “resilient” or not. Rather, this division is to help researchers identify behavioral and psychosocial variables that would lead one to become resilient. In this context, the cutoff score of risk events and school adaptation level in this study may not be identical with other adolescent samples, but still has meaning since the characteristics of resilient individuals are made more clear through the division.
Also, by using the summary score for each scale (risk and adaptation level), the categories were simplified and made easy to understand. However, information on the characteristics of risk and adaptation of groups was reduced. Converting continuous data into groups may result in lower power in statistical analyses. More comprehensive measures and items are needed to assess adaptation, beyond only focusing on adaptation to school life. For example, a study might misclassify a student who leads a happy life at home but does not enjoy school into the less adaptive group. In addition, self-report data are inherently problematic, particularly so when one asks youths to respond to survey statements that they may have never thought about before. There is also possibility of careless responding among students since the time given (15–20 minutes) to fill the questionnaire was relatively short for some students. Therefore, further psychometric work is needed.
Lastly, this study focused more on the characteristics of resilient individuals than on other groups. Although the results of the study are consistent with most resilience research (e.g., Werner & Smith, 1992) which examines the strengths of resilient individuals, we recommend that the characteristics of individuals in other groups should be investigated as well in future research for more abundant findings. In addition, the future studies would be recommended to consider effects of demographics on the profiles of coping strategies (e.g., gender, education level, and ethnic diversity).