
Abstract
Rumination is a cognitive habit involving repetitive negative thinking (RNT). It is a risk factor for depression and develops during late childhood. Targeted interventions to reduce rumination are critical for reducing risk for and impact of depression. Therefore, quick and sensitive scales are needed to capture concrete, quantifiable changes in rumination habit. We developed and evaluated the Tracking Rumination As a Stable Habit (TRASH) measure, to align with Rumination-Focused Cognitive Behavioral Therapy (RF-CBT). The scale was derived, modified and expanded on from the Habit Index of Negative Thinking (HINT). TRASH assesses automaticity and consistency of the habit, quantifiable elements of the daily habit. As part of a larger trial of RF-CBT, 120 adolescents (age mean [sd]: 15.73 [1.11], 67.5% female) completed all scales. Internal reliability of the scale was high (overall α = 0.86, Automaticity α = 0.85, Consistency α = 0.72). The scale demonstrated moderate to strong convergent validity with existing measures of RNT (rs [118] = 0.43 to 0.46). Associations with anxiety, worry and depression measures were modest and variable (rs [118] = 0.13 to 0.63). Divergent and/or nonrelated validity with scales, included null and negative relationships (rs [118] = −0.23 to 0.39). Exploratory analyses identified a general RNT factor (including worry, rumination), a TRASH subfactor, and distinct affective RNT subfactors (e.g., angry, apathetic). Treatment by time interactions suggest similar changes over time in RNT scales, as well as the RNT main factor and the TRASH subfactor. Additional research is needed for the TRASH scale, if it may be sensitive to concrete changes in rumination.
Background
Rumination is a habitual cognitive process characterized by repetitive, passive self-focus on negative emotions and experiences. Rumination has been most extensively researched in the context of depression, guided by the seminal Response Styles Theory, which proposed that rumination is a stable and habitual tendency to dwell on negative information during sad or depressed mood (Nolen-Hoeksema, 1991; Nolen-Hoeksema et al., 2008; Nolen-Hoeksema & Morrow, 1993; Smith & Alloy, 2009; Watkins & Nolen-Hoeksema, 2014). There is now substantial evidence that rumination is a transdiagnostic process that confers increased risk for, and maintenance of, multiple mental health diagnoses (Ehring & Watkins, 2008). In a theoretical integration of existing theory and evidence, Watkins and Roberts’ (2020) H-EX-A-GO-N model proposes that rumination develops as a habitual response (H) to low mood and outlines the role of impairments in the application of executive control (EX), abstract processing (A), and negative biases (N) in susceptibility to rumination, often in the face of goal discrepancies (GO). H-EX-A-GO-N extends Response Styles Theory and Control Theory accounts of rumination to outline distal and proximal mechanisms underlying rumination. Central to both Response Styles Theory and H-EX-A-GO-N is the conceptualization of maladaptive rumination as learned habitual response to stressful experiences that is characterized by more abstract, negative, and passive thinking and behavior. Whilst rumination initially occurs as a normal, goal-directed response to problems and difficulties (goal discrepancies; adjunctive to what may be naturally observed as problem solving; Watkins & Roberts, 2020), repeated pairing of negative emotional states and rumination can lead to this becoming a learned response style (Watkins & Nolen-Hoeksema, 2014). Reinforcement of rumination occurs through avoidance of unpleasant experiences, provision of motivation to complete tasks, and/or perceived contribution to understanding and planning. Frequent and prolonged periods of exposure to stress and low mood can result in repeated rehearsal and consolidation of rumination, producing a learned habitual stimulus-response pairing early in development (Grierson et al., 2016; Shaw et al., 2019). This learned response may contribute to the onset, duration, and recurrence of depression, sustained passivity in action, and an abstract processing style (Smith & Alloy, 2009). Habitual rumination can be difficult to control because it is cued automatically, may be linked to certain locations, internal states and contexts, and it is difficult to target clinically because of its negatively reinforcing consequences.
Rumination is an important treatment target for individuals at risk for depression and its relapse (Just & Alloy, 1997). In individuals with remitted major depressive disorder (MDD), elevated rumination levels predict MDD recurrence (Figueroa et al., 2019). Targeting rumination directly as a maladaptive coping behavior in teens, such as via rumination-focused cognitive behavioral therapy (RF-CBT), may reduce depression recurrence (Bessette et al., 2020; Cook et al., 2019; Jacobs et al., 2016; Topper et al., 2017). Rumination and worry are conceptually and empirically similar RNT cognitive processes (McEvoy et al., 2010); the most frequently used and best validated scales (e.g., Ruminative Response Scale of the Response Styles Questionnaire; Penn State Worry Questionnaire) involve abstract and negative repetitive thought and exacerbate anxiety and sad mood, with potential areas of distinction noted in relation to function (regret vs threat anticipation) and temporal relation (past vs future) (Gustavson et al., 2018; Muris et al., 2004; Stade & Ruscio, 2023). Clinical research demonstrates that rumination and worry are highly correlated, suggesting that rumination and worry have many shared clinical elements for therapeutic targeting (de Jong-Meyer et al., 2009; Fresco et al., 2002; Kalmbach et al., 2016; Kircanski et al., 2018; McEvoy et al., 2013; Puccetti et al., 2025; Stade & Ruscio, 2023).
Repetitive negative thinking (RNT) describes the shared transdiagnostic features of rumination and worry, recognizing these as key risk factors for psychopathology (Ehring & Watkins, 2008). Our H-EX-A-GO-N model of habit-based RNT will benefit from development of specific tools for measuring RNT in daily life. For example, rumination is set in motion not only by stressful experiences, but also by habit-based features like time of day, for example during a morning coffee or in bed at night before sleep. There may be sensory (e.g., darkness and bed covers) or contextual features (e.g., being alone, parents arguing down the hall, social comparison when viewing media). For our purposes, within a habit-framed treatment model of RNT, we focus on the duration, intensity, controllability, and the function(s) of RNT as key variables to be measured given their implications for assessment and treatment (Hoyer et al., 2009; Raes, 2010). For example, these are concrete elements of experience that could be perceivable and are integrated into the diary and therapy parts of RF-CBT. Collection of these measures enables to move beyond “tendency” and “self-described” experiences of rumination to concrete elements that can be changed. Moreover, these in turn can allow for elaboration and nuance within the H-EX-A-GO-N model of RNT.
Despite a strong and consistent link to transdiagnostic clinical disposition and outcomes, rumination is measured infrequently in clinical settings (Baik & Newman, 2023; Ehring, 2021; Kennedy et al., 2024). The most widely used measures of rumination in research focus predominantly on content and frequency of the habitual response style (e.g., Ruminative Responses Scale [RRS]; Nolen-Hoeksema & Morrow, 1991; Treynor et al., 2003), identifying reflective and brooding subtypes. The measure also has a depression subscale, and all three subscales have a modest relationship with depressive symptoms (Nolen-Hoeksema et al., 2008). Brooding rumination is more strongly implicated in transdiagnostic psychopathology relative to reflective rumination (McEvoy et al., 2013; Shaw et al., 2021; Treynor et al., 2003). More recently, scales have been developed to capture specific emotional triggers for rumination like sadness and anger (e.g., Sadness and Angry Rumination Inventory [SARI]; Peled & Moretti, 2010), how individuals think about negative experiences and problems (Bijttebier et al., 2015; Ehring et al., 2011), or frequency and awareness of negative self-thinking (Habit Index of Negative Thinking (HINT); Verplanken et al., 2007).
There are important conceptual distinctions between how a therapist could use rumination scales to try and measure changes in thought content, processing styles, habitual characteristics, in comparison to more tractable, concrete metrics like frequency, intensity, controllability, and situational characteristics (Colvin et al., 2021). For example, whilst the RRS scale used to measure rumination has been highly valuable for developing our understanding of rumination, it is difficult to evaluate week-to-week changes with a scale that is designed to evaluate rumination as a habit, in general, and does not have as many quantifiable elements. Notably, within rumination-focused CBT, there is a therapeutic focus on increasing awareness of rumination, including context and controllability, and practicing alternative, more effective strategies to weaken or replace the ruminative habit (Watkins, 2016). At a theoretical level, key habitual aspects of rumination include the automaticity of rumination (degree of control, how easily is the habit triggered, the initiation of thoughts without awareness or intention) and its consistency (does it occur in similar situations and times, in response to the same stimuli or cues, even in the absence of immediate stressors) (Wood & Neal, 2007). Reliable indices to quantify these characteristics would be valuable to support assessment and ongoing monitoring of the habitual aspects of rumination and to improve their targeting in treatment. In early work, automaticity of negative thought from the HINT scale shows improved predictions of mental health outcomes compared to frequency of RNT (Verplanken et al., 2007). As such, the use of scales, new and existing that tie more concretely to the goals, intentions and strategies of the therapy would aid both patients and therapists in effective delivery of the intervention.
To more sensitively assess the strength of the habitual rumination in everyday life and its change following targeted treatment, our group created a new scale for use within a randomized clinical trial evaluating RF-CBT by expanding an existing measure of rumination automaticity (Verplanken et al., 2007). Our revised scale (Tracking Rumination as a Stable Habit; TRASH) preserves items relevant to automaticity and adds items intended to assess cue-response consistency. This study examines the psychometrics of TRASH in a clinical sample of adolescents with remitted MDD (rMDD). We hypothesized that the TRASH subscales would have moderate to strong internal reliability and converge with existing measures of rumination and clinical scales of anxiety, depression, and worry. In addition, while we expected strong convergence with existing measures of rumination, we also evaluated whether TRASH assesses unique aspects of rumination not captured in other scales. Moreover, visual analog scales for rumination (rumVAS) were used to determine if we can more directly assess quantifiable changes in frequency, distress, duration, and control of ruminative thought. We examine the relationships between TRASH and impulsivity, distractibility, avoidance, and inhibition, to test conceptual divergence of these constructs that are related to clinical depression but are not part of RNT. These are constructs (e.g., impulsivity, distractibility, avoidance, and inhibition) that are aligned with the experience of an internalizing disorder like depression. These constructs can even be related to rumination (e.g., avoidance) for some, but not all, individuals who engage in habitual rumination. We included these constructs and measures to look at specific aspects of change in rumination with RF-CBT, not more general changes or adaptative behaviors. We hypothesized that these behavioral indices associated with depression may be elevated in individuals who experience mental health challenges, but that they should not relate specifically to RNT.
Method
Participants and Procedures
Baseline data were analyzed for 120 participants recruited for the R61 and R33 phases of a pre-registered RCT examining RF-CBT for adolescents with rMDD and elevated rumination (Langenecker et al., 2024; Roberts et al., 2021). Adolescents were recruited from the Salt Lake City, UT and Columbus, OH areas through radio and community advertisements. Eligible participants were ages 14 to 18 with a history of MDD, with at least partial remission for two weeks. Eligible participants also had RRS scores above a T score of 50 by age and sex. All participants who completed baseline assessments were included in factor analyses, including those who were ineligible for the trial (NCT03859297
Measures
Rumination Response Scale (RRS) is a 22-item self-report measure that assesses ruminative response tendencies to feelings of sadness and depression, including brooding and reflection (Nolen-Hoeksema & Morrow, 1991; Treynor et al., 2003). The RRS had strong internal consistency (α = 0.93) in a sample of adolescents (Liang & Lee, 2019). Scores were computed by summation of responses for all items, and subsets of items for each subscale.
Sadness and Anger Rumination Inventory (SARI) is a 22-item self-report questionnaire that measures ruminations about one’s anger (SARI anger) or sadness (SARI sadness). The original 22-item version demonstrated excellent internal consistency in adolescents (sadness α = 0.95, anger α = 0.96; (Peled & Moretti, 2007). For our analyses, we used the recommended 19-item version (Peled & Moretti, 2010). Scores were sums of items from each respective subscale.
Behavioral Inhibition Scale (BIS) is a 7-item scale (sum of scores) that measures trait-like responses to avoid negative consequences (Carver & White, 1994; Figueroa et al., 2019), a subscale of the larger Behavioral Inhibition System and Behavioral Activation System (BIS/BAS) questionnaire which measures sensitivity to punishment, non-reward, and novel stimuli. The BIS demonstrated good internal consistency in young adults (α = 0.75; Carver & White, 1994).
Impulsive Behaviors Scale for Children (UPPS-P-C) is a 40-item self-report measure that assesses 5 factors of impulsivity: negative urgency, premeditation, perseverance, sensation seeking, and positive urgency (Zapolski et al., 2010). In an adolescent sample, internal consistency for each factor ranged from α = 0.79 to α = 0.95 (Tomko et al., 2016). Scoring followed the standard procedure of summating the responses and reversed responses for items in each subscale.
Screen for Child Anxiety Related Disorder (SCARED) is a 41-item self-report measure of anxiety, including panic and associated somatic, generalized worries, separation, social, and school refusal anxiety symptoms (Birmaher et al., 1997, 1999). Internal consistency of SCARED subscales ranged from good to excellent in an adolescent sample, with α ranging from 0.74 to 0.94 (Birmaher et al., 1997). Scores were sums of items from each respective subscale.
Penn State Worry Questionnaire for Children (PSWQ-C) is a 14-item self-report measure of worry in children and adolescents (Chorpita et al., 1997) adapted from the adult-based PSWQ. It assesses generality, intensity, and uncontrollability of worry (Păsărelu et al., 2017). The PSWQ-C demonstrated excellent internal consistency in a clinical adolescent sample (α = 0.91; Pestle et al., 2008). Scores were calculated by summing all items, with items 2, 7, and 9 reversed.
Rumination Habit Visual Analog Scale (rumVAS) is a 4-item self-report measure that we developed for quantification of elements of the experience of the rumination habit through a 10-point visual analog scale (scores are on the 10 point scale), modified from a previously published scale that examines rumination frequency and distress caused by ruminative behavior (Wichelns et al., 2016). rumVAS assesses the frequency, sense of control, duration, and distress experienced during rumination.
Mind Wandering Deliberate and Spontaneous Scales (MW-D & -S) are each 4-item self-report measures of deliberate and spontaneous mind wandering behaviors (Carriere et al., 2013), where scores are summations of all respective items. In adolescent samples, the MW-D and MW-S demonstrate good internal consistency (α = 0.82 and α = 0.81, respectively; Carciofo & Jiang, 2021).
Multidimensional Experiential Avoidance Questionnaire for Adolescents (MEAQ-A) is a 39-item self-report measure of one’s tendency to avoid negative internal experiences, adapted for adolescents. Subscales assess distress aversion and the use of distraction/suppression and repression/denial to avoid distress (Gámez et al., 2011). The MEAQ-A demonstrates internal consistencies ranging from α = 0.70 to 0.80. Subscale scores are sums of their respective items.
Children’s Depressive Rating Scale Revised (CDRS-R) is a 17-item, clinician-administered scale that combines child and caregiver report in a clinician-determined scale to assess depressive symptoms (Poznanski & Mokros, 1996) and was used to assess past week symptoms for the present study. The CDRS-R demonstrated good internal consistency in adolescent samples, ranging from α = 0.74 to 0.92 (Mayes et al., 2010). Scoring is adjusted weighting, sum of scores from parent and child interviewed ratings.
Treating Rumination as a Stable Habit (TRASH) asks participants to self-report aspects of ruminative habit over the previous two weeks. We devised this as a shorter, modified form of HINT (Verplanken et al., 2007) for repeated measurement within a clinical trial. TRASH was developed to have two subscales with five items each (see Table 3 for all items): Automaticity (happens without awareness, e.g., “I start before I realize I’m doing it”) and Consistency of the ruminative response to the same cues/contexts (similar locations, situations, times of day, e.g., “I do it in the same place(s)”). Responses are assessed on a 5-point Likert scale, and items are summed for sub and total scores. Understanding and increasing awareness of the ruminative habit are early key goals in the RF-CBT therapeutic model before the therapeutic process can effectively target the rumination habit.
Analyses
All analyses were conducted in R version 4.5.2 (R Core Team, 2024). Factor analyses were conducted with the psych package (Revelle, 2024). Missingness structure was evaluated with the naniar package (Tierney & Cook, 2023). A description of missing data handling is included in the supplement.
TRASH Reliability and Factor Structure
Internal reliability in this sample was assessed using Cronbach’s α across all items, and for Automaticity and Consistency subscales. An exploratory factor analysis (EFA) examined the underlying structure of TRASH. Parallel analysis and Bayesian Information Criterion (BIC) identified the best fitting number of factors. Factors were extracted by principal axis factoring due to non-normality of the data and obliquely rotated via the oblimin algorithm as we anticipated correlation between factors. A confirmatory factor analysis was also run with lavaan package (Rosseel, 2012) to examine fit estimates of the hypothesized two factor structure of TRASH. Model fit was evaluated against a saturated model (chi-square) and a null independence model (CFI, TLI).
TRASH Construct Validity
To assess construct validity, we examined correlation coefficients between TRASH and hypothesized convergent and divergent scales. Correlation probability values were adjusted with the Benjamini-Hochberg procedure. For convergent validity, we anticipated a strong positive correlation between TRASH, existing measures of rumination (RRS, SARI), and to a lesser extent clinical scales of anxiety, depression, and worry (SCARED, CDRS-R, PSWQ respectively). For divergent validity, we anticipated weak positive or negative correlations between TRASH and scales related to impulsivity (UPPS), distractibility (MWDS), avoidance (MEAQ), and inhibition (BIS), although our specific research sample with history of depression who are seeking treatment - presents some potential for restriction of range or bias in this regard.
Exploratory Bifactor Analyses
While we expected strong convergence with existing measures of rumination, we also evaluated whether TRASH assesses unique aspects of rumination not captured in other scales (i.e., Automaticity and Consistency). We conducted two exploratory bifactor analyses (EBFA). The first EBFA (narrow) included items from a set of scales specifically measuring rumination and worry (TRASH, RRS, SARI, PSWQ, rumVAS). The second EBFA (broad) included items from all scales used for convergent/unrelated/divergent validity evaluation (TRASH, RRS, SARI, PSWQ, rumVAS, SCARED, CDRS-R, UPPS, MWDS, MEAQ, BIS), the results of which are in the supplement (Table S2). For both analyses, we posited an RNT factor on which all items load and allowed items to load onto additional group factors with oblique rotation. The number of factors to extract was determined by parallel analysis and BIC. Individual loadings on factors were determined through extraction by principal axis factoring using each item’s squared multiple correlations (EBFA 1), or by minimum residual (EBFA 2). Bifactor rotation (Jennrich & Bentler, 2011) using the biquartimin function provided final factor structures. A confirmatory factor analysis modeling each of TRASH automaticity, TRASH consistency, RRS, PSWQ-C, SARI anger, SARI sadness as separate factors provided fit estimates.
Treatment Sensitivity
To evaluate the sensitivity of the TRASH to rumination focused RFCBT relative to existing scales, we conducted analyses (unblinding for MBT only) aimed at elucidating pre-post differences in automaticity, consistency, and closely related RNT constructs (RRS, PSWQ-C). Only participants with all relevant data at both time points were included (n = 55). Items at both pre and post treatment were standardized by calculating z-scores using the mean and standard deviation from pre-treatment data. Factor scores for each time point were computed using pre-treatment factor loadings. Linear mixed-effects models (LMMs) were constructed with the lme4 (Bates et al., 2015) and lmerTest (Kuznetsova et al., 2017) packages, including an interaction effect between treatment group and time point and a random intercept for subject. Post hoc estimates were generated via the emmeans package (Lenth, 2025). Results were visualized with ggplot2 (Wickham, 2016).
Results
Demographics and Clinical Variables
Baseline Sample Characteristics of the 120 Adolescents

Note. RRS, Rumination Response Scale. TRASH, Tracking Rumination As a Stable Habit. SARI, Sadness and Anger Rumination Inventory. VAS, Visual Analogue Scale. CDRS-R, Children’s Depression Rating Scale Revised. SCARED-GAD, Screen for Child Anxiety Related Disorders-Generalized Anxiety Disorder.
Internal Consistency of Rumination and Related Scales
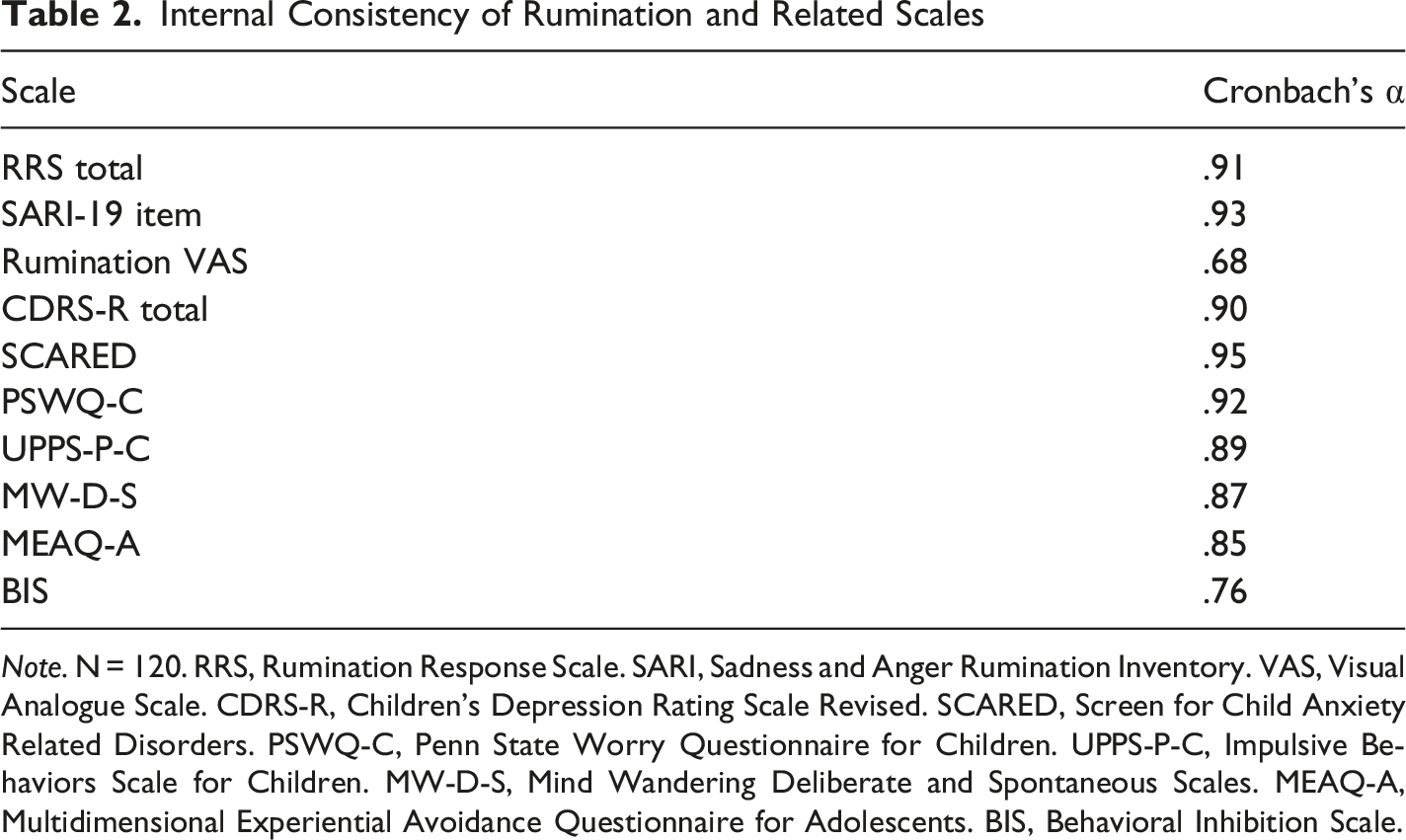
Note. N = 120. RRS, Rumination Response Scale. SARI, Sadness and Anger Rumination Inventory. VAS, Visual Analogue Scale. CDRS-R, Children’s Depression Rating Scale Revised. SCARED, Screen for Child Anxiety Related Disorders. PSWQ-C, Penn State Worry Questionnaire for Children. UPPS-P-C, Impulsive Behaviors Scale for Children. MW-D-S, Mind Wandering Deliberate and Spontaneous Scales. MEAQ-A, Multidimensional Experiential Avoidance Questionnaire for Adolescents. BIS, Behavioral Inhibition Scale.
Internal Consistency and Factor Structure of TRASH
TRASH Items and EFA Loadings
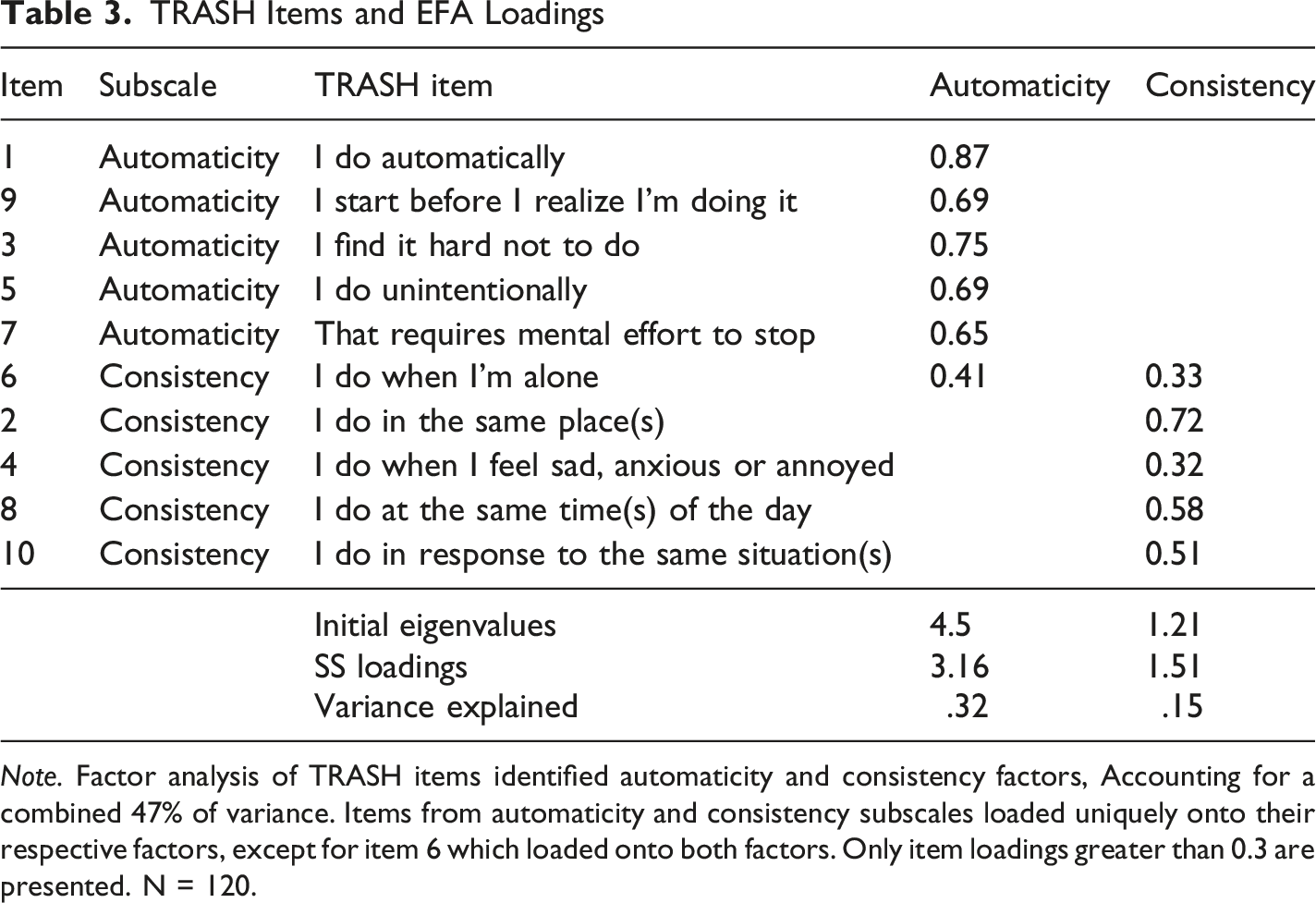
Note. Factor analysis of TRASH items identified automaticity and consistency factors, Accounting for a combined 47% of variance. Items from automaticity and consistency subscales loaded uniquely onto their respective factors, except for item 6 which loaded onto both factors. Only item loadings greater than 0.3 are presented. N = 120.
Convergent and Divergent Validity
TRASH Automaticity and Consistency subscales (n = 118) demonstrated moderate to strong convergent validity with established RNT measures, including RRS (Automaticity r [n = 118] = .43, p < .001; Consistency r [118] = .46, p < .001), SARI sadness (Automaticity r [118] = .46, p < .001; Consistency r [118] = .46, p < .001), PSWQ (Automaticity r [118] = .63, p < .001; Consistency r [118] = .44, p < .001). Weak correlations were observed for SARI anger (Automaticity r [118] = .27, p < .001; Consistency r [118] = .29, p < .001). For clinical scales, correlations were mixed, with the SCARED (Automaticity r [118] = .54, p < .001; Consistency r [118] = .48, p < .001), CDRS-R (Automaticity r [118] = .13, p < .001; Consistency r [118] = .08, p < .001). Non-RNT trait measures had generally lower correlations; MEAQ-A (Automaticity r [118] = .07 to .29, p < .001; Consistency r [118] = .09 to .26, p < .001), and MWDS (Automaticity r [118] = .20 to .35, p < .001; Consistency r [118] = .19, p < .001), and UPPS-P-C (Automaticity r [118] = −.02 to .09; Consistency r [118] = −.23 to .08), although see BIS (Automaticity r [118] = .40, p < .001; Consistency r [118] = .29, p < .001). See Figure 1 for an arrayed, color-coded representation of RNT-related relationships, and Figure S1 for all scales. Correlation coefficient matrix between RNT-related scales, adjusted with the Benjamini-Hochberg procedure. *p < .05 & p ≥ .01, **p < .01 & p ≥ .001, ***p < .001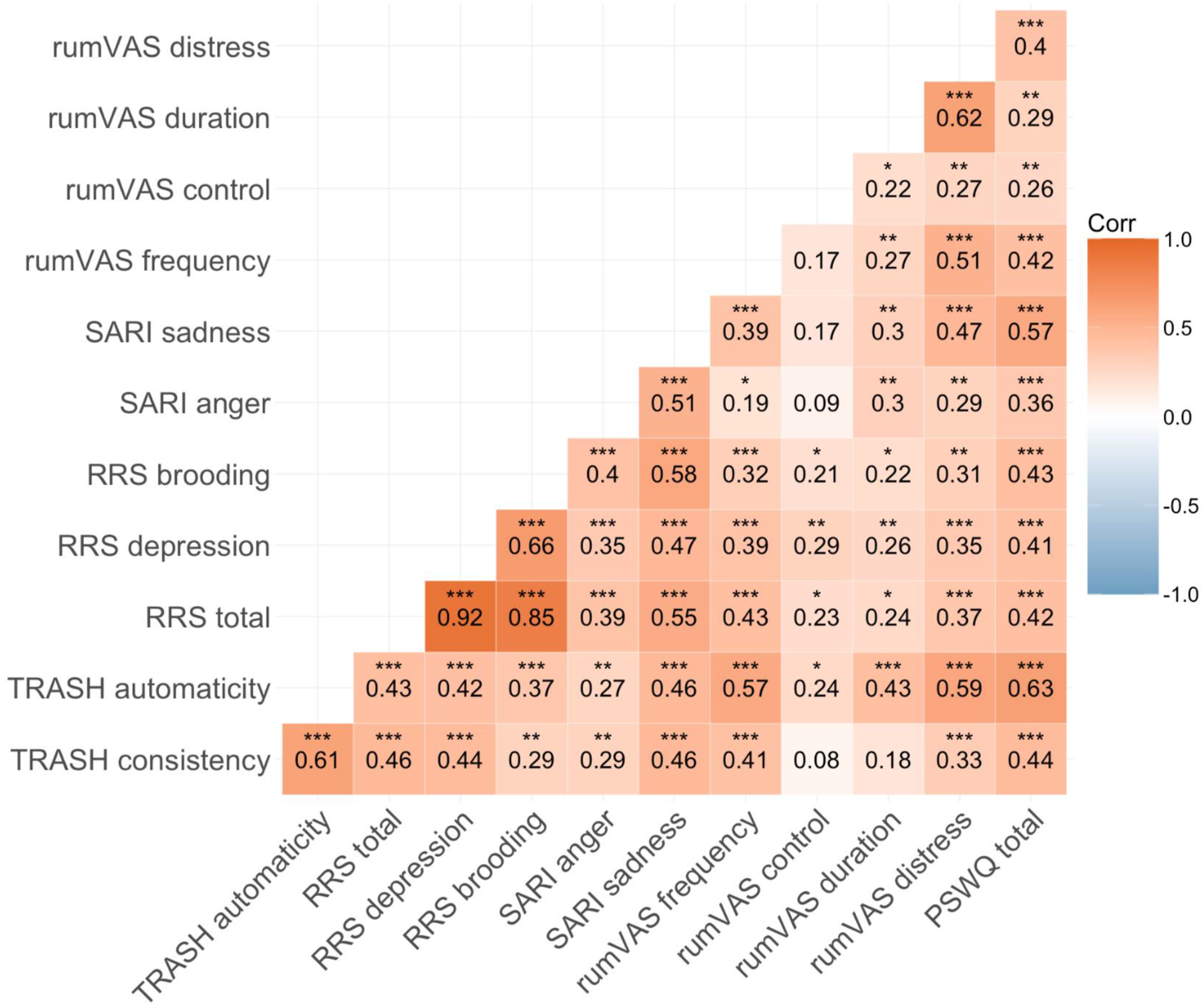
Exploratory Bifactor Analysis 1 (Narrow, RNT Focused Analysis of Worry and Rumination Scales Only)
Exploratory Bifactor Analysis Item Loadings
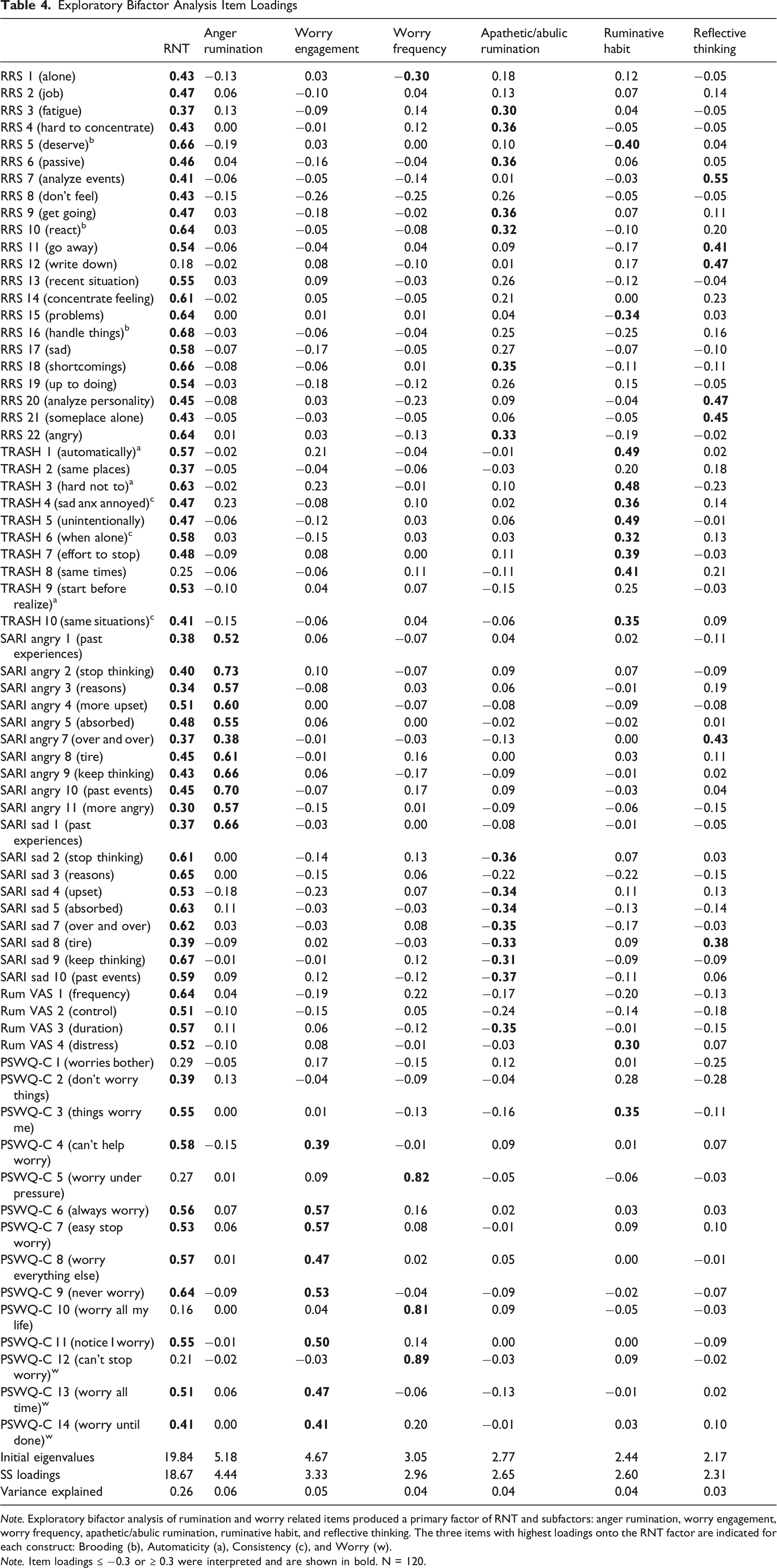
Note. Exploratory bifactor analysis of rumination and worry related items produced a primary factor of RNT and subfactors: anger rumination, worry engagement, worry frequency, apathetic/abulic rumination, ruminative habit, and reflective thinking. The three items with highest loadings onto the RNT factor are indicated for each construct: Brooding (b), Automaticity (a), Consistency (c), and Worry (w).
Note. Item loadings ≤ −0.3 or ≥ 0.3 were interpreted and are shown in bold. N = 120.
Factor Score Correlations
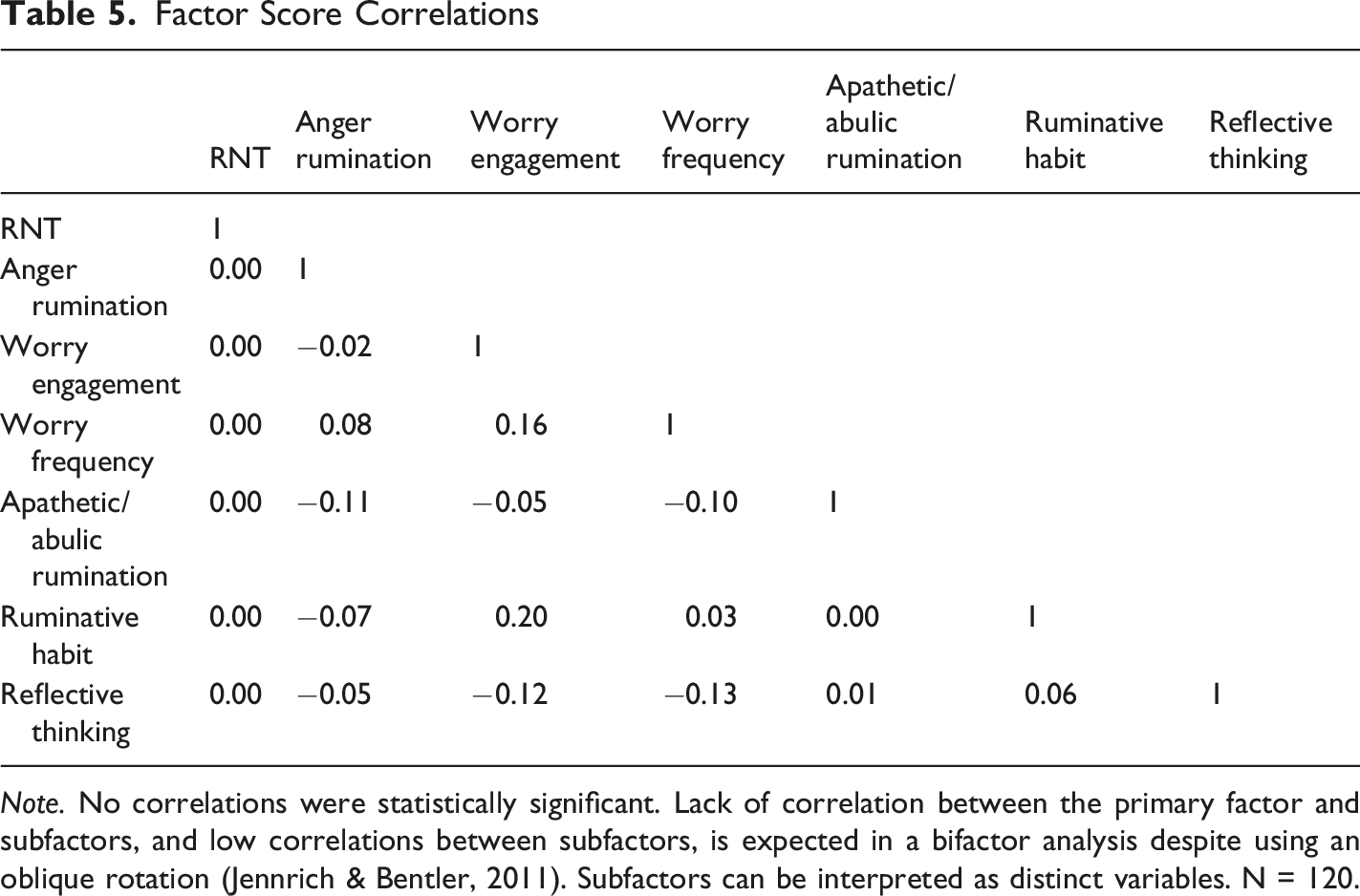
Note. No correlations were statistically significant. Lack of correlation between the primary factor and subfactors, and low correlations between subfactors, is expected in a bifactor analysis despite using an oblique rotation (Jennrich & Bentler, 2011). Subfactors can be interpreted as distinct variables. N = 120.
Treatment Effects
Significant negative interactions (9 models; n = 29 RF-CBT, 11 TAU, 15 Relax Tx) for the RF-CBT treatment group by time were observed for 5 models: RRS (t [55] = −2.37, p = .02), TRASH consistency scale (t [55] = −2.23, p = .03), PSWQ-C (t [55] = −2.11, p = .04), RNT factor (t [55] = −2.61, p = .01), and TRASH automaticity factor (t [55] = −2.29, p = .03). The treatment by time interaction for TRASH automaticity scale failed to reach significance (t [55] = −1.87, p = .07), and these were not evident for any other measure (consistent with a preliminary analysis with insufficient statistical power). Post hoc, within-group pre-post comparisons for RF-CBT group only indicated significant changes in RRS (t-ratio [58.2] = 5.82, p < .001), TRASH automaticity scale (t-ratio [58.2] = 6.17, p < .001), TRASH consistency scale (t-ratio [58.2] = 4.58, p < .001), PSWQ-C (t-ratio [58.2] = 4.62, p < .001), RNT factor (t-ratio [58.2] = 6.34, p < .001), worry engagement factor (t-ratio [58.2] = 3.24, p = .02), and ruminative habit factor (t-ratio [58.2] = 3.98, p = .002). Pre-post differences in the Relaxation group were only observed for the RNT factor (t-ratio [58.2] = 3.09, p = .03). Model-based estimates are included in the supplement (Tables S3 & S4) and plotted in Figure 2. Post hoc estimated marginal group means with 95% confidence intervals for constructs hypothesized to respond to RF-CBT. All data were standardized to pre-treatment data prior to entry into the model and factor scores were calculated using the pre-treatment factor structure loadings. Panels A through D are standard scores for the scales. TRASH automaticity (factor scores) and TRASH consistency (factor scores) reflect factor scores from the TRASH-only factor analysis (Panels E and F). RNT, worry engagement, and ruminative habit reflect factor scores from the narrow (rumination-related scales) factor analysis (Panels G, H, and I). Δ = Glass’s Δ from raw pre/post means, scaled by pre-treatment SD. N = 55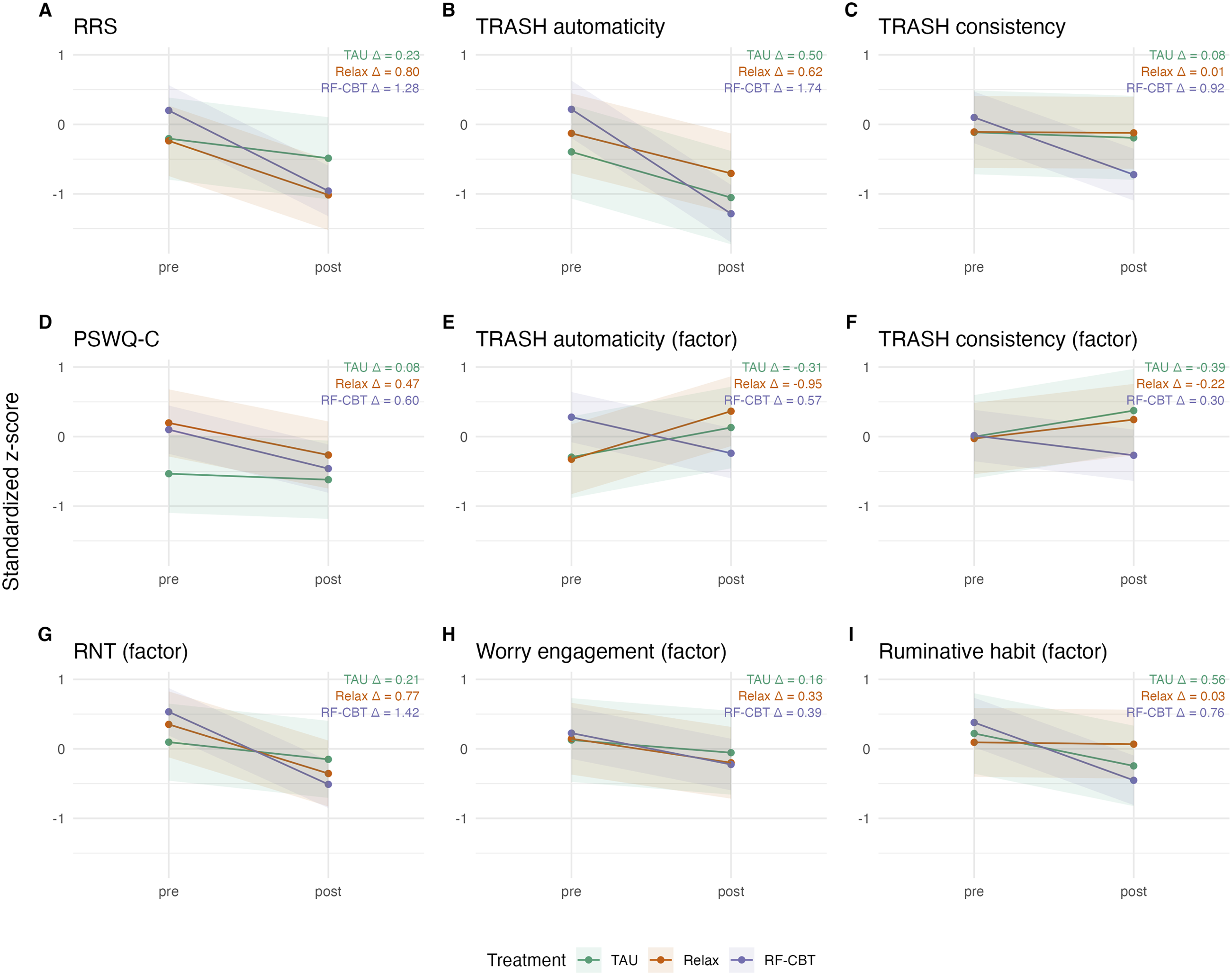
Discussion
Rumination, a form of RNT, is associated with higher risk for the onset, exacerbation, maintenance, and recurrence of depression (Watkins & Roberts, 2020), and poorer outcomes (Clancy et al., 2020; Mazzer et al., 2019; Zawadzki, 2015). Measures of trait rumination such as the RRS and SARI are designed to assess content and general response tendencies such as frequency. They do not directly assess process or temporal components (i.e., automaticity and consistency) of rumination in everyday life. A brief measure that directly captures the habitual strength of rumination is potentially valuable for tracking therapeutic change, including in future treatment studies and clinical practice that targets rumination. Tracking Rumination As a Stable Habit (TRASH) was designed to enable more sensitive and face valid assessment of the automaticity and consistency of the ruminative habit. Generally, TRASH demonstrated strong internal structure and measured two habit factors, as hypothesized. Moreover, an explicit exploratory bifactor analysis of RNT measures (new and existing) identified a distinct ruminative habit factor that was separable from a general RNT factor. TRASH questions also loaded onto the general RNT factor. Subfactors identified emotional (anger and apathy) as well as cognitive elements of rumination or perseverative negative thought (e.g., worry engagement, frequency).
We found significant correlations between our revised TRASH measure and existing measures of rumination, residual depression, worry, and anxiety. Furthermore, items related to worry (i.e., PSWQ-C) loaded onto a general factor of RNT in addition to a separate worry factor (engagement, frequency; Table 4). Convergence of rumination and worry are expected based upon prior literature (de Jong-Meyer et al., 2009; Fresco et al., 2002; Kalmbach et al., 2016; Kircanski et al., 2018; McEvoy et al., 2013; Puccetti et al., 2025; Stade & Ruscio, 2023). While worry and rumination are sometimes conceptualized with respect to different temporal frameworks (future/past respectively), patients may tend to experience rumination and worry flowing together into ongoing repetitive thought (e.g., repetitive thoughts about past difficulties trigger concerns about the future and vice versa). TRASH and RRS scores were moderately related to overall anxiety, panic and GAD, and weakly or unrelated related to subscales of separation, social, and school avoidance anxieties, consistent with generalized anxieties being more closely related with RNT than context-specific fear-based symptoms.
We hypothesized TRASH items would load onto a discrete subfactor within the bifactor analysis. In alignment with our hypothesis, bifactor analyses were able to delineate a separate “habit rumination” subfactor that included most (8 of 10) of the TRASH items - Automaticity and/or Consistency items (more day-to-day experiences, triggers or situations), separate from more general aspects of worry and rumination. Of the two items from the TRASH scale that did not load on the subfactor, they had subthreshold, positive loadings. These questions pertained to a more general pattern of ruminating (e.g., “when sad/upset/distracted”). Items related to worry, rumination, automaticity, and consistency all loaded onto a single RNT bifactor. Because these items assessing habit strongly loaded with more contextual and experiential items on ruminative content, it is possible that habit and emotional content of rumination are highly consistent in adolescents with remitted MDD. Response Styles Theory explicitly links RNT to moments of feeling sad and down. Alternatively, youth may experience difficulty separating triggers (e.g., things that make me ruminate, in general) and contexts (e.g., places and times and people with whom I ruminate) of rumination before psychoeducation about RNT. We were able to show in specific post hoc analyses that there is (preliminarily) reduction of TRASH and RRS in those with history of MDD who received RF-CBT, at a differential rate compared with other therapies (note, insufficient power as the trial is not yet finished). In addition, ruminative habit measurement may be more amenable to repeat assessments of specific habitual aspects with ecological momentary assessment. The ruminative habit subfactor also included the VAS distress item as a positive loading, while two RRS items were inversely loaded on the subfactor (“What am I doing to deserve this?” and “Why do I have problems others don’t have?”). They are inversely loaded, suggesting they are separate from the TRASH subfactor, which is linked more to automaticity (higher items are automaticity 1, 3, and 5). RF-CBT specifically aims to increase awareness of the habit to reduce automaticity through raising awareness, and practice with replacement behaviors (Watkins, 2016).
These results suggest some modest utility for using TRASH Automaticity and Consistency items but call for consideration of omitting item 9 (…start before realize), and item 2 (…in the same places) in repeated assessments (see Table 3). Shortened bifactor subscales for affective elements (worry, sadness, anger) might be useful for specific experimental manipulations or treatment subcomponents, although these may be more niche and unstable elements of the rumination habit. Notably, the visual analog scales did not appear to have a unifying structure that might aid in clinical use and may not be useful for measuring change during rumination interventions. They may reflect more temporally sensitive, or unstable, elements of rumination.
Measuring change with treatment was the original intent of creating the TRASH, yet it was not the specific goal of this manuscript. Nonetheless, showing specific treatment change with TRASH under RF-CBT provides preliminary support for the clinical potential of the scale. With that in mind, the post hoc results with preliminary pre- and post-treatment data do show greater reduction of both RRS and TRASH in the sample with RF-CBT. The direct wording of the TRASH, with both quantity and location for automaticity and consistency elements, may have great face validity and traction for clinical use relative to the RRS. Subsequent work by our group and others can address this question. Further, the brevity and ease of use of the TRASH may relate to repeated use in clinical contexts. We recommend using an average score for the TRASH subscales and total scale, so that the clinician and patients alike can estimate severity of RNT and degree of change with treatment (e.g., 1 = low/absent habit, 3 = modest habit, 5 = strong habit). As the bifactor model would suggest, rumination and worry do share much variance in the main factor. Clinical distinctions about the focus of worry (future) and rumination (past), along with other nuanced distinctions, may have some value in specific treatment techniques, whereas the broad factor is worthy of targeting as well.
Limitations
There are several limitations to consider for the work presented here. The current analyses are secondary to the clinical trial primary outcomes and utilize a volunteer sample. A volunteer sample does not match well all teens who might arrive for clinical care (e.g., availability, monetary incentives, motivation for change). This sample (the RRS range of 35-85 is wide but elevated and does not include low/normative or occasional rumination) may have restricted our ability to understand rumination nuanced differences with other scales. Missingness can also have untoward influences on results, particularly because attrition is often related to clinical characteristics. The impact of attrition, interaction with clinical characteristics, and implications for use of TRASH with RF-CBT are incomplete here as the trial is still ongoing. When the blind is broken for the investigators, we will be able to fully evaluate this important limitation and understand the implications. There were eight individuals who completed the baseline consent but did not complete the questionnaires that went into these factor analyses. In addition, at this stage, only about 40% (N = 55) of the sample had completed all scales pre and post intervention, so there is not a direct linkage between the factor analyses and convergent/divergent statistics with the clinical change data. Further, exploratory bifactor analyses were conducted on a relatively small sample compared to the number of items included in the analyses; these should be considered exploratory initial results to spur follow-on studies with larger samples. The sample also captured a limited age range of youth (14 to 18-year-olds) at a particularly sensitive developmental stage. Broader age ranges will be necessary to generalize results across the lifespan. While this study of youth with rMDD and elevated rumination provides an excellent sample with clinical experience of depression and elevated rumination for validating clinical sensitivity of the TRASH in relation to the RRS and PSWQ, these data may only represent the positive tail of a skewed distribution. Further, the modal range of most ruminative scores may not enable enough range to psychometrically validate clinical variability. In non-clinical controls with low rumination, the concepts and questions from the TRASH may have minimal or mixed relevance to their day to day lives. The scales and differences here are nuanced, as RF-CBT resulted in decreases in RRS, TRASH scales, PSWQ, and related bifactors, if at slightly different rates (and with only 2/3 of the expected sample in this prelim analysis). Presently, there is a great deal of overlap, and individual clinical models and preferences may drive decision making. However, the TRASH scales provide face validity and ask concrete questions. We also acknowledge that people may not perceive/make the subtle distinctions between the concrete questions (e.g., time, place, context) and general tendencies (e.g., when I am sad, in general). The TRASH subcomponents complement the functional analysis that is applied in RF-CBT, which is centered on gathering more details and specifics regarding the experiences leading up to, during, and following habit-driven rumination episodes. The subcomponents are also well-aligned with the evaluation of changes over the course of treatment that are therapeutically meaningful. There are also considerable differences in scales that were weakly or unrelated to TRASH. For example, UPPS-P Lack of premeditation was negatively correlated and unrelated to TRASH consistency and automaticity respectively. For divergent validity, it is not necessary to have inverse correlations, but rather correlations that sort closer to 0. As an example, residual depression symptoms were correlated with RRS (r = .32), but not with either TRASH scale (r = .13 for automaticity and r = .08 for consistency). Convergent validity can range from weak (e.g., r ∼ .20) to modest (r ∼ .40), to strong (r ∼ .60), to colinear (r > .70). Finally, this study’s recruitment and enrollment period largely coincided with the COVID-19 pandemic and subsequent years. Youth generally reported higher rates of anxiety, depression, and post-traumatic symptoms during the pandemic (Marques de Miranda et al., 2020; Racine et al., 2021). Adolescents enrolled during the pandemic may reflect a unique cohort and experience of the ruminative habit relative to those enrolled pre- or post-pandemic.
Conclusion
We revised and expanded an existing scale (HINT) to implement a shorter, simpler, and face valid form (TRASH) that could be used repeatedly by clinicians to track that habitual strength of rumination over the course of treatment. Our intent was to marshal the specificity of the automaticity-related content from HINT and add consistency-related context items into the abbreviated form, and to demonstrate that it measured more discrete facets of the ruminative habit. The bifactor analysis results corroborates existing literature that RNT is a habit with general and specific emotion-based aspects and that a TRASH subfactor is present and changes with RF-CBT. Future work can focus on the application of shorter scale(s) for tracking rumination habit with automaticity and consistency relative to general RNT changes in clinical trials and in clinical care.
Supplemental Material
Supplemental Material - Tracking Rumination as a Stable Habit (TRASH); Scale Modification and Convergent Validity in a Clinical Sample of Youth With a History of Depression
Supplemental Material for Tracking Rumination as a Stable Habit (TRASH); Scale Modification and Convergent Validity in a Clinical Sample of Youth With a History of Depression by Matthew B. Thompson, Leah R. Thomas, Mindy Westlund Schreiner, Noah H. Kingston, Hannah Ollech, Leo Kalotihos, Caty Escobar, Urvi Wagh, Myah Pazdera, Erin Kaufman, Sheila E. Crowell, Henrietta Roberts, Katie L. Bessette, Scott A. Langenecker, Edward R. Watkins in Psychological Reports
Footnotes
Acknowledgements
We are grateful for the statistical consultation provided by Alexander Demos, University of Illinois Chicago.
ORCID iDs
Ethical Considerations
This study was approved by the Institutional Review Board (IRB) of University of Utah (IRB_00113733) on 10/22/2018, whose review was accepted by the IRBs of The Ohio State University (2023X0077) and Nationwide Children’s Hospital (STUDY00003890).
Consent to Participate
Written informed assent and consent to participate in this study were provided by participants and participants’ parent(s)/legal guardian(s), respectively.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: SAL and ERW disclosed receipt of the following financial support for the research for this article: This work was supported by the National Institute of Mental Health grant number MH116080 (mPIs SAL and ERW). KLB received financial support through NIMH T32 (MH073517).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.