
Abstract
Research on adolescent development and well-being has demonstrated the beneficial effects of social support and self-esteem for positive adjustment. However, there has been little examination of the associations between adolescents’ social support, self-esteem, and well-being within a Caribbean framework, and consideration to family factors that may moderate such associations. Accordingly, the current study explored the associations of perceived family and peer social support, self-esteem, and psychological well-being within the framework of several family contextual factors among 334 Jamaican adolescents (Mage = 14.56, 51% boys). Family support showed direct and indirect associations with depression, anxiety, stress, and well-being through self-esteem while peer support only showed a direct positive association with well-being. Furthermore, several contextual factors demonstrated important associations with the variables of interest, though none of these significantly altered model fitness. The results demonstrate the protective nature of social support and self-esteem for Jamaican adolescents, and suggest that further longitudinal examinations are warranted.
Keywords
Adolescents today lead diverse and challenging lives given the numerous personal and environmental factors influencing their development and well-being (Margolin, 2006; Nanninga, Jansen, Knorth, & Reijneveld, 2015; Weber, Puskar, & Ren, 2010; Zimmer-Gembeck & Skinner, 2016). Sociocultural disparities within Jamaican society may place these adolescents at increased risk over their American or European counterparts (Dreher & Hudgins, 2010; Lambert & Lyubansky, 1999; Meeks Gardner, Powell, & Grantham-McGregor, 2007; Weber et al., 2010). For example, Jamaica’s cultural history has led to a preponderance of matrifocal households considered by some Caribbean scholars to be a functional response to Jamaica’s unique colonial past (Brown & Johnson, 2008; Hickling, Matthies, Morgan, & Gibson, 2008; Ricketts & Anderson, 2008). Nonetheless, such disparities in family structure may predict negative outcomes, including low levels of perceived support, self-esteem, and well-being, along with higher levels of depression and anxiety (Lindsey, Joe, & Nebbitt, 2010; Shahar & Henrich, 2016; Smith & Moore, 2013; Van Dale et al., 2014). While such outcomes are detrimental to adolescent adjustment, some scholars suggest greater emphasis be placed on family processes as these appear particularly salient for developmental outcomes (Bastaits, Ponnet, & Mortelmans, 2012; Causey, Livingston, & High, 2015). The current study aimed to examine whether Jamaican adolescents exposed to greater family advantage (e.g., living in two-parent homes or with higher parental education) reported better adjustment than their counterparts. Second, we examined the direct and indirect effects of perceived family and peer social support on adolescent psychological well-being, through self-esteem, while considering several socioeconomic family-related factors.
Dynamics of the Caribbean Family
One of the most distinctive features of the Jamaican family is the high prevalence of the matrifocal household (Brown & Johnson, 2008; Dreher & Hudgins, 2010; Hickling et al., 2008; Samms-Vaughn, 2001). This type of family structure has historically been the norm within Jamaica and the wider Caribbean society (Brown & Johnson, 2008; Ricketts & Anderson, 2008; Roopnarine & Jin, 2016; Samms-Vaughn, 2001), and has been noted as vastly different to that of the traditional nuclear family. The legacy of slavery, colonization, and indentured servitude resulted in Jamaican families being characterized by a range of different conjugal unions providing varied contexts for the socialization of children (e.g., visiting relationships), and the dependence on the mother as the primary source of economic and social support (Brown & Johnson, 2008; Dreher & Hudgins, 2010; Ricketts & Anderson, 2008; Roopnarine & Jin, 2016; Samms-Vaughn, 2001, 2008). Although not ideal, research on Caribbean families has refuted claims that single-parent families were more detrimental to child development, thus altering the perception that such families are dysfunctional (Brown & Johnson, 2008; Phillips, 2012; Sieh, Visser-Meily, & Meijer, 2013).
Nonetheless, few studies conducted within Jamaica noted differential outcomes by the various types of family structures (see Brown & Johnson, 2008; Hutchinson et al., 2004; Meeks Gardner et al., 2007; Samms-Vaughn, 2008). However, the findings among these studies indicate that the differences noted in adolescent outcomes by family structure are embedded within other sociodemographic differences including child age, parental support, education, stress, socioeconomic status (SES), and poverty. This may suggest that an examination of family structure differences should consider sociodemographic factors that may be more important to child and family outcomes. One such sociodemographic difference is that children exposed to greater advantage within their family and social contexts (e.g., higher SES and parental education) report higher levels of self-esteem, social and emotional support, and lower internalizing symptoms (Bastaits et al., 2012; Brown & Johnson, 2008; Costello, Swendsen, Rose, & Dierker, 2008; Ersoy, Özcan, & Agargün, 2008; Hickling et al., 2008; Weber et al., 2010). For example, Samms-Vaughn (2008) reported that Jamaican children living in less stable common-law and visiting unions, and those in single-parent homes showed lower cognitive and academic achievement. However, family status had differential effects on children’s cognitive, academic, and behavioral outcomes through low levels of parental education, high parental stress, limited stimulation and parental participation in children’s activities, and economic disadvantage. Similarly, Ricketts and Anderson (2008) found that children of families below the poverty line (predominantly those living in common-law unions) were most at risk of experiencing low levels of parent–child interaction and connectedness, as well as higher levels of corporal punishment.
While these studies highlight the negative effects of living in a single-parent family combined with other economic and social adversities, some studies paint a different picture. Brown and Johnson (2008) revealed children’s perceptions of their families differed by age, SES indicators, and family structure. Older children living in single-parent families (mainly rural Jamaican matrifocal) reported less negative qualities compared with their younger counterparts and those from nuclear families who reported greater relational quality. Similarly, Dreher and Hudgins (2010) found that children living in a nuclear family structure did not have any significant advantages over single-parent families as the latter had multiple-union patterns and maternal siblings, which provided developmental advantages for these children. Evidently, family functioning is complex and offers varying outcomes for child and adolescent well-being depending on other socioeconomic contexts. Consequently, empirical investigations should consider aspects of the family’s social structure in understanding how these may affect psychosocial factors relevant for adolescent development.
Self-Esteem, Social Support, and Psychological Well-Being
Psychological well-being can be conceptualized as a state of positive functioning and a high degree of satisfaction with self in the domains of autonomy, environmental mastery, personal growth, and positive relations with others (Ryff & Keyes, 1995). Prior investigations (e.g., Bastaits et al., 2012; Hutchinson et al., 2004) indicate that psychological well-being is influenced by both external (social and environmental) and internal (personal) factors. One such factor is self-esteem, which has empirically demonstrated consistent associations with aspects of positive psychosocial adjustment over the life span, and is predictive of adaptive physical and psychosocial health (Causey et al., 2015; Ersoy et al., 2008; Leary, Tambor, Terdal, & Downs, 1995; Margolin, 2006; Sowislo & Orth, 2013). Self-esteem has often been conceptualized as one’s affective evaluation of self (Leary & Baumeister, 2000; Leary et al., 1995; Sowislo & Orth, 2013), and is associated with higher levels of life satisfaction and psychological well-being (e.g., Bastaits & Mortelmans, 2016; Bastaits et al., 2012), lower levels of anxiety and depression, loneliness, and stress (Ersoy et al., 2008; Margolin, 2006; Sowislo & Orth, 2013). Self-esteem appears to be a global predictor of psychological adjustment, and its cultivation is therefore essential in adolescence.
Along with self-esteem, perceived social support consistently demonstrates positive associations with adolescent well-being (Bastaits & Mortelmans, 2016; Causey et al., 2015; Costello et al., 2008; Lindsey et al., 2010; Van Dale et al., 2014). Social support is the emotional and instrumental warmth and care that a group provides to the needs, desires, and plans of the individual (Bastaits & Mortelmans, 2016; Causey et al., 2015; Weber et al., 2010). Empirically, social support has been linked to lower levels of depression and anxiety, loneliness, risky sexual behavior, and suicidal ideation (Causey et al., 2015; Costello et al., 2008; Kalina et al., 2011; Lindsey et al., 2010; Pace, Zappulla, & Di Maggio, 2016; Weber et al., 2010). In addition, during adolescence, it becomes important to separately examine the effects of family and peer support as peers become important attachment figures and sources of support during this time (Allen, 2008; Margolin, 2006; Pace et al., 2016; Van Dale et al., 2014).
Family and peer social support may have differing associations with adolescent well-being because they provide fulfillment of different psychological needs (Allen, 2008; Pace et al., 2016). As children transition into adolescence, peers become meaningful providers of support and security, while relationships within the family often become secondary within the attachment hierarchy (Allen, 2008). During this time, adolescents become more autonomous in their parental interactions, while peers provide important sources of information related to feelings of self-worth, self-efficacy, and social expectations (Pace et al., 2016; Zimmer-Gembeck & Skinner, 2016). For Jamaican adolescents, there may be a greater struggle to become more autonomous and to form meaningful peer relationships given the overt (e.g., violent lyrics from dance hall music) and covert (e.g., high prevalence of substance use) societal messages that reinforce poor self-image, conflictual relationships with others, and low self-esteem (Hickling et al., 2008). Nonetheless, youth experiencing difficulties that exceed their coping resources often turn to their families for support over friends and/or community members (Allen, 2008; Lindsey et al., 2010; Margolin, 2006; Zimmer-Gembeck & Skinner, 2016). This suggests that families remain important sources of support during adolescence and may be more powerful influencers than peers. Therefore, considering the direct and differential associations of perceived family and peer-related social support, both are warranted to examine, with the expectation that family support will more strongly associate with adolescent outcomes.
Consistent with the widely held belief that both social support and self-esteem are noteworthy assets for adaptive outcomes, researchers have posited that self-esteem derives from meaningful interpersonal sources such as families, friends, communities, and schools (Bastaits & Mortelmans, 2016; Ersoy et al., 2008; Leary et al., 1995; Sowislo & Orth, 2013). Furthermore, sociometer theory (Leary & Baumeister, 2000; Leary et al., 1995) suggests that self-esteem acts as a sociometer that helps to nurture one’s need for belongingness by motivating one to be a part of a group where he or she feels valued as a desirable member. Therefore, the more individuals feel accepted and supported by their families and peers, the higher their level of self-esteem as they have perceived a sense of social inclusion. Similarly, sociometer theory helps to account for the associations of social support, self-esteem, and psychological adjustment, whereby self-esteem is related indirectly with psychological adjustment through beneficial aspects of social inclusion (Leary & Baumeister, 2000; Leary et al., 1995). For example, socially excluded individuals (those who perceive low social support from interpersonal networks) often report higher levels of loneliness and depressive symptoms (Sowislo & Orth, 2013). Notably, these associations are yet to be empirically tested cross-culturally and may vary based on important socioeconomic differences.
Gender Differences in Adolescent Well-Being Outcomes
In keeping with the differences noted in adolescent outcomes by aspects of family contextual factors, adolescent gender has also demonstrated differences in several factors examined within this study. Female adolescents consistently report higher levels of internalizing symptoms (Kalina et al., 2011; Lambert & Lyubansky, 1999; Nolen-Hoeksema & Hilt, 2013; Pace et al., 2016; Sieh et al., 2013). In addition, male compared with female adolescents report higher levels of self-esteem and psychological well-being (Bastaits et al., 2012; Hutchinson et al., 2004; Sieh et al., 2013; Smith & Moore, 2013) but less social support from family, friends, and important others (Kalina et al., 2011). Similarly, among a Jamaican sample (n = 2,580), several gender-based moderations are evident in the associations of well-being, age, religiosity, and life satisfaction (Hutchinson et al., 2004). Evidently, gender is important to consider when exploring correlates of adolescent well-being.
The Present Study
The purpose of this study was to examine associations of family contextual factors (i.e., living status/family structure, perceived socioeconomic wealth, maternal and paternal education, and parental union status) with perceived family and peer social support, self-esteem, negative affect (depressive, anxious, and stressful symptoms), and well-being among Jamaican adolescents. As adolescence is commonly defined chronologically as ages 10 to 18 years (Curtis, 2015), young people within this age span comprised the target population for the present study. The next aim examined how perceived family and peer support and self-esteem related to adolescent well-being, as well as to determine whether there was an indirect relationship of family and peer support with well-being through self-esteem. Finally, given evidence for differences in perceived support and child outcomes according to family structure and child gender, differences in model paths were examined according to these factors. Meeting these aims was expected to inform whether future investigations should emphasize issues related to family process (e.g., family support) or family structure. We therefore hypothesized the following:
Method
Participants
Participants were 334 students ranging in age from 10 to 18 years (M = 14.56, SD = 1.94, 51% boys) attending a secondary educational institution in St. Andrew, Jamaica. About one half (48.9%) of adolescents were Black and the others were from a variety of different or mixed sociocultural backgrounds (e.g., Chinese, Indian, Asian, and Lebanese). In terms of family structure, 70.1% reported living in a two-parent household and the remainder in a single-parent or “other” household type. Students predominantly lived in a family where either the mother held a graduate (37.8%) or undergraduate degree (37.5%), or the father held a graduate (39.1%) or undergraduate degree (26.0%). The total sample pool was 350 and student and parental consent to participate was received for 334 students (95% response rate).
Measures
Along with the demographic information sheet measuring important family contextual factors such as adolescent age, gender, perceived socioeconomic status, parental education and union status, and current living status/family structure, the following measures were employed:
Psychological well-being
Adolescent’s well-being was measured with the Depression, Anxiety, and Stress Scale–Short Form (DASS-21) and the Psychological Well-being Scale–Short Version (PWB-18). The DASS-21 (Lovibond & Lovibond, 1995) measured depressive, anxious, and stress symptoms. Participants responded using a 4-point Likert-type scale ranging from 1 (did not apply to me at all) to 4 (applied to me very much or most of the time). Items were summed, creating composite scores for depression, anxiety, and stress, where higher scores indicated greater distress. Cronbach’s α for depression, anxiety, and stress were .87, .79, and .79, respectively. The PWB-18 (Ryff, 1995) was adapted for use with adolescents from the original Psychological Well-being Scales. Participants responded on a 6-point scale, ranging from 1 (completely disagree) to 6 (completely agree). Summing all items formed the total score, where higher scores indicated higher levels of well-being. Cronbach’s α was .84.
Perceived social support
The Multidimensional Scale of Perceived Social Support (MSPSS; Zimet, Dahlem, Zimet, & Farley, 1988) assessed the adequacy of perceived social support from family and friends (Ersoy et al., 2008). Participants responded on a 7-point scale, ranging from 1 (very strongly disagree) to 7 (very strongly agree). Four items for each scale were summed to create total composite scores, where higher scores reflect greater perceived support from family and peers. Cronbach’s α for the family and peer support scale were .88 and .89, respectively.
Self-esteem
The Rosenberg’s Self-Esteem Scale (RSES; Rosenberg, 1965) measured perceptions of global self-esteem (Kalina et al., 2011). The scale is composed of 10 items where participants responded on a 4-point scale, ranging from 1 (strongly disagree) to 4 (strongly agree). Five of the 10 items were reversed scored then all items were summed to create a total score. Higher scores indicated greater levels of self-esteem. Cronbach’s α in the current study was .88.
Procedure
Approval for this study was provided by the university ethics committee. Following approval, the principal provided consent for the study to be conducted within her school. A random sampling technique was utilized where a list of all the classes at each grade level (Grades 7-13) from the secondary educational institution was garnered by the participating researchers. After a pilot study of 34 Grade 7 students, a random selection was taken among the list of all the classes, where two classes from each grade level were selected. Once everyone in the class met the inclusion criteria, the entire class was sampled at the time and day aligning with each class’ Personal Development period. Participants were reassured of their anonymity, and research investigators were present to answer questions.
Overview of Analyses
To replace missing data, Little’s Missing Completely at Random (MCAR) test was used to determine that the data was missing completely at random ( χ2[710, N = 334] = 325.66, p = 1.0). As such, estimation maximization was then used to maintain all participants in the analyses. Ms, SDs, and correlations between all variables were calculated, as well as t tests to compare all variables according to gender and living status (i.e., adolescents from two-parent compared with one-parent households). The proposed model was tested using full information maximum likelihood (FIML) estimation within AMOS software (IBM Corporation). This model was tested to evaluate hypotheses pertaining to the direct effects of social support from family and from friends on well-being, as well as the indirect effect of social support on well-being via self-esteem. To evaluate model fit, both goodness-of-fit indices (χ2, χ2 relative to sample size, comparative fit index [CFI], and root mean square error of approximation [RMSEA]) and parameter estimates for model paths were considered (Kline, 2005). To test hypotheses regarding indirect pathways, bootstrapping was used to estimate standard errors and 95% confidence intervals (CIs) for all direct and indirect effects. Multiple group models were then fit to identify differences in model fit according to gender and living status. To evaluate a competing hypothesis that self-esteem would be associated with well-being via perceptions of social support, an alternate model was tested with self-esteem as the predictor and perceived parent and peer social support as mediators.
Results
Means, Standard Deviations, and Correlations
Table 1 presents Ms, SDs, and correlations between measures. Social support from family and friends were positively intercorrelated, and both were positively associated with self-esteem and psychological well-being and negatively associated with depression and anxiety. Social support from family, but not from friends, was negatively associated with stress and participant age, and positively associated with perceived economic wealth and father’s education. Self-esteem was negatively associated with depression, anxiety, and stress, and positively associated with psychological well-being. Self-esteem was also negatively associated with age, and positively associated with perceived economic wealth. Females, compared with males reported significantly higher levels of social support from friends, t(331) = −2.24, p = .03, depression, t(331) = −2.11, p = .04, and stress, t(331) = −2.53, p = .01. Adolescents from two-parent compared with one-parent households reported significantly higher levels of social support from family, t(331) = −2.35, p = .02, perceived economic wealth, t(331) = −2.84, p = .005, and mother’s education, t(331) = −2.79, p = .006.
Means, Standard Deviations, and Correlations Between All Variables (N = 334).
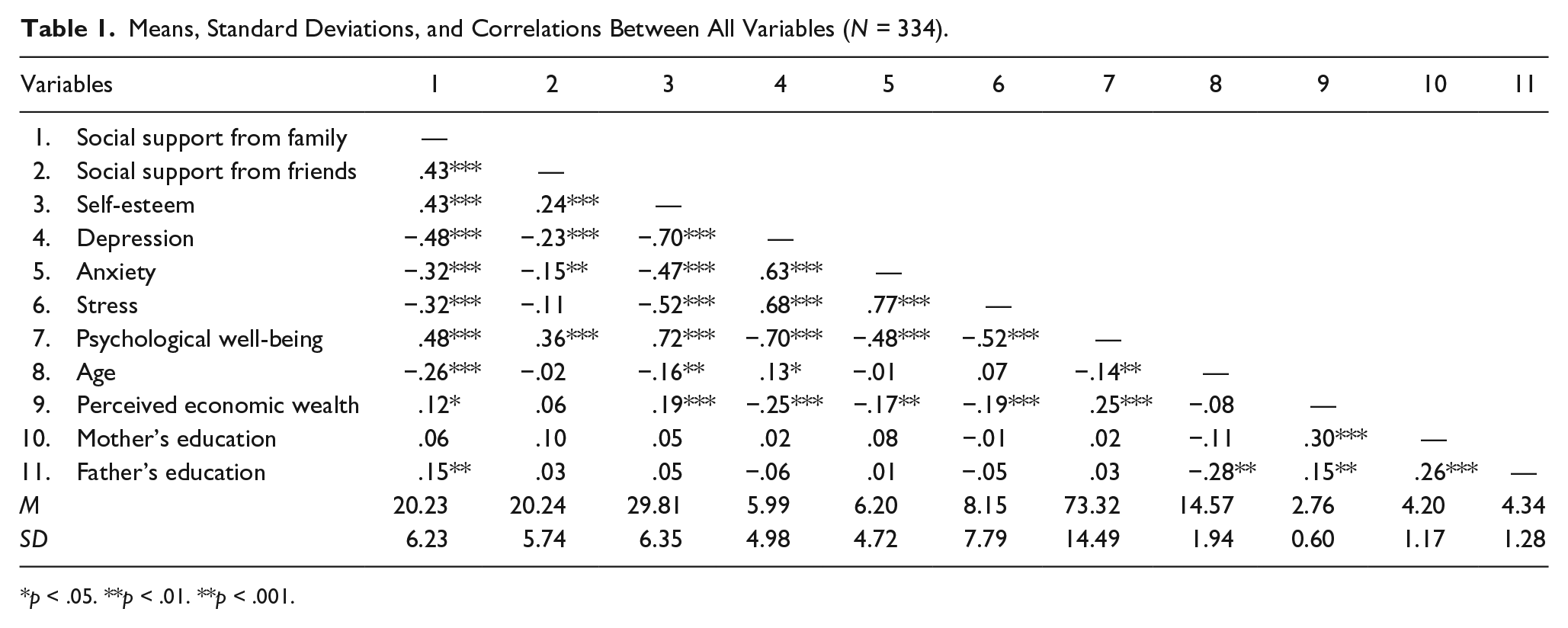
p < .05. **p < .01. **p < .001.
Direct and Indirect Pathways From Social Support, From Family and Friends, to Adolescent Psychopathology and Well-Being
The model demonstrated an excellent fit with the data, χ2(3, N = 334) = 1.57, p = .67, χ2/df = 0.52, CFI = 1.00, and RMSEA = .00 (90% CI = [.000, .072]), p = .87. The variance explained by the model was 21% for self-esteem, 53% for depression, 26% for anxiety, 30% for stress, and 58% for psychological well-being. Table 2 presents the path estimates, standard errors, and CIs. Figure 1 shows the significant model paths.
Direct and Indirect Associations Between Social Support and Adolescent Psychopathology and Well-Being, via Self-Esteem (N = 334).
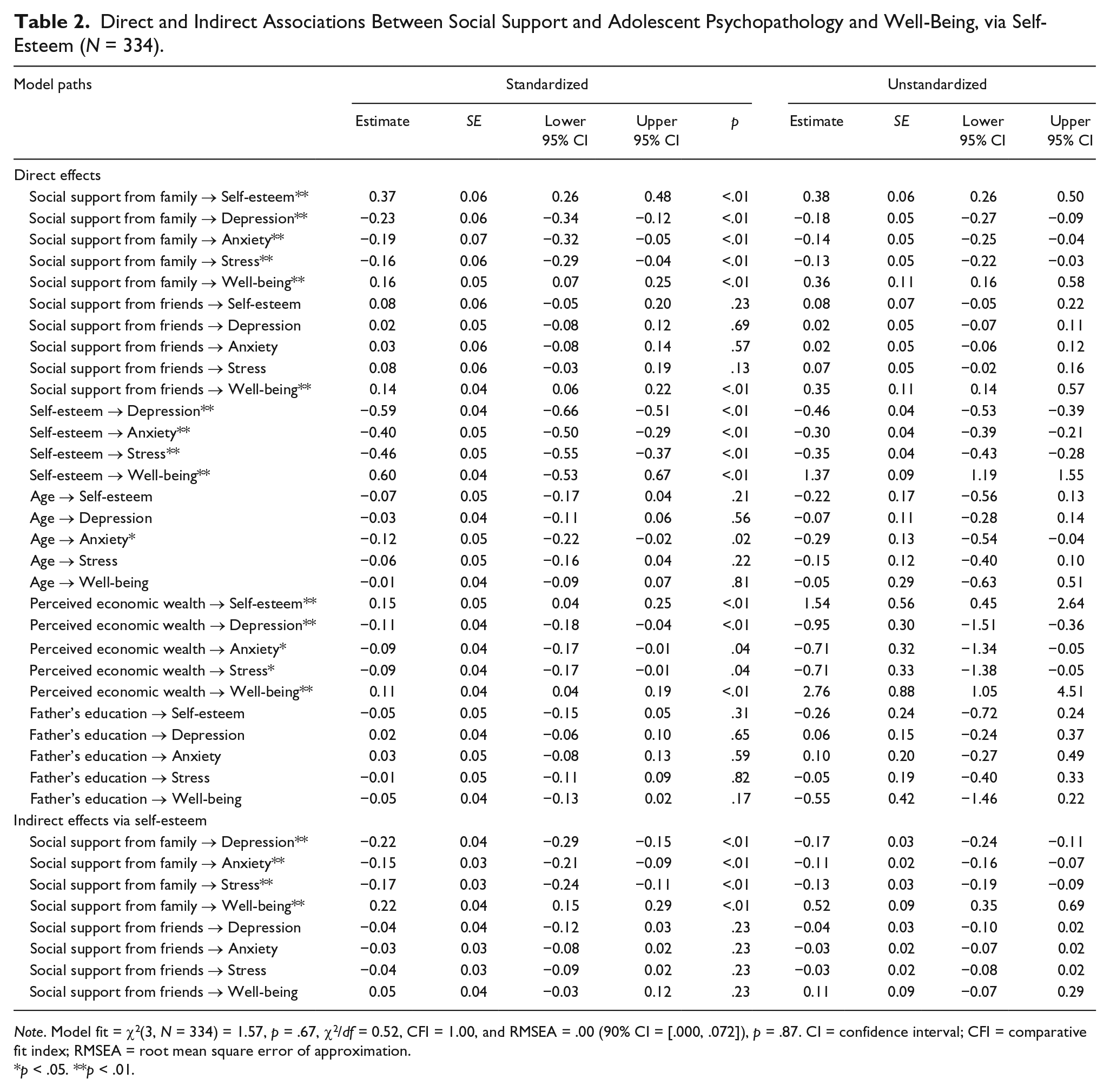
Note. Model fit = χ2(3, N = 334) = 1.57, p = .67, χ2/df = 0.52, CFI = 1.00, and RMSEA = .00 (90% CI = [.000, .072]), p = .87. CI = confidence interval; CFI = comparative fit index; RMSEA = root mean square error of approximation.
p < .05. **p < .01.
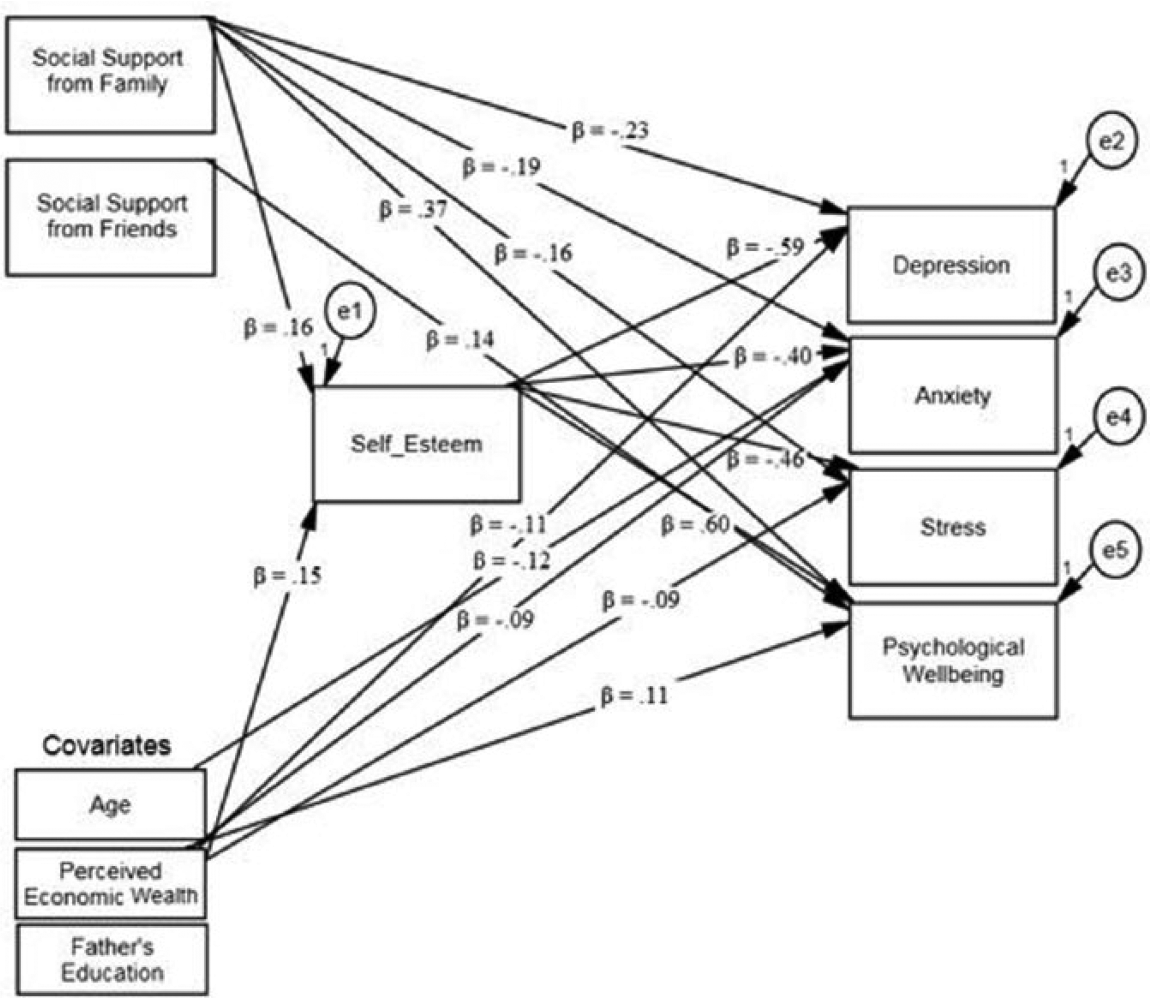
Significant model paths.
Social support from family members showed direct negative associations with depression (β = −.23, p < .01), anxiety (β = −.19, p < .01), and stress (β = −.16, p < .01), and a direct positive association with psychological well-being (β = .16, p < .01). Social support from friends showed a direct positive association with psychological well-being (β = .14, p < .01). Social support from family, but not from friends, also showed a direct positive association with the proposed mediator self-esteem (β = .37, p < .01), and self-esteem showed direct associations with depression (β = −.59, p < .01), anxiety (β = −.40, p < .01), stress (β = −.46, p < .01), and psychological well-being (β = .60, p < .01). In partial support of the hypothesized mediational pathway, social support from family also showed an indirect association with lower depression (β = −.22, p < .01), anxiety (β = −.15, p < .01), stress (β = −.17, p < .01), and high psychological well-being (β = .22, p < .01), via self-esteem.
As indicated by bivariate correlations, participant age, perceived economic wealth, and father’s education were included as covariates into the final model. Age showed a weak negative association with anxiety (β = −.12, p = .02), and perceived economic wealth was associated with higher self-esteem (β = .15, p < .01) and psychological well-being (β = .11, p < .01), and lower depression (β = −.11, p < .01), anxiety (β = −.09, p = .04), and stress (β = −.09, p = .04).
Multiple Group and Alternate Models
Multiple group structural equation modeling (SEM) showed that the model fit did not significantly differ when model paths were unconstrained or allowed to differ between males and females, χ2diff(52, N = 334) = 54.79, p = .37, or between adolescents from two-parent and one-parent households, χ2diff(52, N = 334) = 69.46, p = .05, compared with when equality constraints were applied to all paths. To evaluate the competing hypothesis (i.e., that self-esteem would be associated with well-being via perceived social support), an alternate model was fit where self-esteem and perceptions of parent and peer social support were exchanged, making social support from parents and peers the mediators. The alternate model demonstrated a poor fit with the data, χ2(2, N = 334) = 53.84, p < .001, χ2/df = 26.92, CFI = .96, and RMSEA = .28 (90% CI = [.218, .346]), p < .001.
Discussion
This study presents a novel examination of associations among three concepts—perceived support, self-esteem, and psychological well-being—within a broader framework of several family contextual factors (i.e., living status/family structure, perceived socioeconomic wealth, parental education and union status). Combined, the findings reveal the importance of family and peer support to adolescents’ overall sense of psychological well-being, as well as their differential effects on self-esteem, which in turn related to higher levels of positive adjustment. The notion that adolescents exposed to greater family advantage experience greater adaptive outcomes was supported though these factors do not necessarily moderate the pathways from social support to overall psychological well-being. These findings are essential to clinical scientists within Jamaica, and the wider Caribbean, as they increase understanding of the mediated pathways in which experiences of relational support are associated with adolescent experiences of self-esteem and psychological adjustment.
Unique Outcomes of Family and Peer Support
Consistent with our hypotheses and prior studies (Bastaits & Mortelmans, 2016; Causey et al., 2015; Costello et al., 2008; Kalina et al., 2011; Pace et al., 2016), perceived social support from family and peers were differentially related to adolescent well-being outcomes, with the former demonstrating a more robust and stronger set of associations. Adolescents who perceived more support from their family also reported higher levels of psychological well-being and self-esteem, and lower levels of depression, anxiety, or stress, while greater perceived support from peers only related to greater feelings of well-being. The results corroborate the protective role that social support plays in adolescents’ lives. Furthermore, the findings illustrate the importance of perceived support from the family as primary attachment figures, even when intimacy needs shift to more peer-related connections during adolescence (Allen, 2008; Lindsey et al., 2010; Shahar & Henrich, 2016).
These findings are essential for the Jamaican context as they underscore the importance of positive interactions within Jamaican families and their implications for adolescents’ adaptive outcomes. This is important as past research within this population highlights the moderate to high prevalence of punitive, authoritarian, and harsh physical discipline practices endorsed by Jamaican parents; particularly those living within a lower socioeconomic or rural context (Brown & Johnson, 2008; Hickling et al., 2008; Meeks Gardner et al., 2007; Ricketts & Anderson, 2008). While such parenting practices have decreased more recently, current investigations still report evidence of intolerant responses to child misbehavior (Smith & Moore, 2013), which may dissuade children from seeking support and acceptance from family during challenges. Drawing on results from the present study, Jamaican parents are encouraged (and greater resources, such as parenting workshops, may be needed) to promote feelings of warmth, security, and trust within the family, rather than utilizing more punitive practices, to support adolescent well-being. Emphasis on such strategies remain important given the strong cultural heritage, situational stressors (e.g., parenting stress and economic hardship), and developmental histories that support resistance to engaging in more authoritative parenting practices (Brown & Johnson, 2008; Hutchinson et al., 2004; Ricketts & Anderson, 2008; Samms-Vaughn, 2008).
In addition, our findings corroborate that having support from family helps adolescents feel better about themselves and allows them to use this level of esteem to face perceived challenges. Therefore, the findings also speak to the protective benefits of self-esteem in adolescent populations (Bastaits et al., 2012; Causey et al., 2015; Costello et al., 2008; Ersoy et al., 2008; Sowislo & Orth, 2013) and supports the assertions of the sociometer theory of self-esteem, whereby self-esteem is thought to have evolved as a result and a gauge of one’s social acceptance to assist with avoiding alienation and rejection (Leary & Baumeister, 2000; Leary et al., 1995). Our results demonstrate that higher levels of self-esteem are positively associated with various indices of adjustment. Furthermore, self-esteem comprises a mechanism through which perceived family support is positively related to indicators of well-being, suggesting that being positively regarded by significant others may buffer against negative emotions and promote adjustment, through supporting positive views of self (Leary & Baumeister, 2000; Leary et al., 1995; Sowislo & Orth, 2013). Similarly, when we tested our competing hypothesis (i.e., perceived family and peer support as mediators of the association between self-esteem and adjustment), the model demonstrated a poorer fit to the one we hypothesized. Though our study is correlational in nature and we cannot assume a direction of association, such a finding provides an initial step in confirming the notion that adolescents’ overall sense of self-worth derives from positive, nurturing, and supportive familial relationships.
Consistent with prior studies (Lindsey et al., 2010; Margolin, 2006; Shahar & Henrich, 2016) but inconsistent with others (Pace et al., 2016) is that perceived peer support neither predicted self-esteem nor any of the internalizing symptoms in our structural model. Though in bivariate correlations, peer support was significantly associated with these outcomes as hypothesized, when taking into consideration the powerful protective factors of family support and self-esteem, peer support failed to reach significance. While peers may provide a meaningful source of support in relation to peer-related experiences of rejection, victimization, or aggression (Pace et al., 2016; Van Dale et al., 2014; Zimmer-Gembeck & Skinner, 2016), when it relates to negative mental health experiences, peers may be less supportive and possibly even rejecting (Lindsey et al., 2010; Margolin, 2006; Shahar & Henrich, 2016). Thus, instead of seeking support from friends for experiences that may display vulnerability or personal deficit, which in turn may elicit further social exclusion, this sample of adolescents may perceive it better to seek support from family.
The Sociodemographic Context and Psychosocial Outcomes
In the present study, adolescents from one-parent compared with two-parent households perceived significantly lower levels of social support from family members, potentially placing the many Jamaican youth from one-parent households at elevated risk for psychological maladjustment. Notably, family structure did not moderate model paths, indicating that the associations between perceived social support, self-esteem, and well-being were consistent across Jamaican adolescents from one-parent compared with two-parent households. These findings align with previous studies of Jamaican (Brown & Johnson, 2008; Dreher & Hudgins, 2010; Meeks Gardner et al., 2007) and American youth (Ryan & Claessens, 2013), which suggests that not only children from one-parent families may be at heightened risk of disadvantage and maladjustment, but also that it may be the family processes associated with household structure that are particularly important, such as parental provision of support and stimulation.
The present findings also revealed several significant associations of other family contextual factors. Indicators of SES (i.e., perceived economic wealth, and to a lesser extent, father’s education) emerged as distinct protective contextual factors. In addition, in the structural model, perceived economic wealth was significantly associated with higher levels of self-esteem and psychological well-being, and with lower levels of internalizing symptoms. These findings confirm that adolescents exposed to greater advantage by means of higher SES have better indicators of positive adjustment, and further confirms past literature within Jamaica regarding the benefits individuals of a higher social class experience (Brown & Johnson, 2008; Dreher & Hudgins, 2010; Hickling et al., 2008; Meeks Gardner et al., 2007). Prior Caribbean literature supports that individuals who perceive and experience greater socioeconomic advantage also report higher levels of emotional and psychological well-being. One reason for this is that families who report lower SES experience greater levels of stress and poverty, and limited access to health care and educational opportunities, all of which have been identified as significant risk factors for physical and psychological maladjustment (Brown & Johnson, 2008; Dreher & Hudgins, 2010; Ersoy et al., 2008; Ricketts & Anderson, 2008; Samms-Vaughn, 2008).
The present findings support an emphasis in future research on socioeconomic factors and family processes for understanding Jamaican adolescent well-being. However, these results should be interpreted with caution given the difference in socioeconomic backgrounds of participants in this study and prior Jamaican samples (e.g., Brown & Johnson, 2008; Meeks Gardner et al., 2007; Samms-Vaughn, 2001, 2008). More specifically, 70.1% of the present sample lived in two-parent households (whether married or common-law unions) and a high percentage of adolescents sampled had parents who received higher levels of education. In contrast, samples employed by previous studies of Jamaican and Caribbean families are characterized by mothers sharing primary responsibility for physical and emotional support while having several visiting relationships that may or may not translate to marital or common-law unions (Brown & Johnson, 2008; Hickling et al., 2008; Roopnarine & Jin, 2016; Samms-Vaughn, 2001, 2008). Despite these differences, the findings highlight three things. First, Jamaican adolescents from middle- to upper-class backgrounds may also experience emotional difficulties that stem from limited family and peer support (see Hickling et al., 2008). Second, adolescents from single-parent families may not necessarily experience more negative outcomes than those from two-parent families as outcomes are also linked to a range of other social and economic indicators (Dreher & Hudgins, 2010). Third, the findings highlight the importance of exploring direct and indirect mechanisms for adolescent well-being within the complex nature and structure of family functioning; an approach recommended in future studies examining a wider cross section of youth.
Finally, gender differences were evident in the present study, where adolescent girls demonstrated higher levels of depression and stress as well as greater perceived support from peers. These results among Jamaican youth are consistent with past research concerning American and European adolescents (Costello et al., 2008; Kalina et al., 2011; Pace et al., 2016; Sieh et al., 2013), as female adolescents are repeatedly found to be more vulnerable to internalizing symptoms than males. Some reasons for this greater vulnerability include, but are not limited to, female adolescents’ greater use of more negative coping strategies such as rumination, gender-related pubertal changes, greater reactivity to negative life events, and possibly greater socialization for sensitivity to interpersonal concerns (Costello et al., 2008; Nolen-Hoeksema & Hilt, 2013; Pace et al., 2016). The latter of which may also account for why adolescent girls (in comparison with boys) also perceive greater levels of support from their peers. Theoretical explanations indicate that girls are more socialized to value and respond to interpersonal support more than their male counterparts (Nolen-Hoeksema & Hilt, 2013; Pace et al., 2016), and it appears this is also the case for Jamaican girls. Nonetheless, gender did not moderate model paths, highlighting the gender-neutral and culturally universal benefits of perceived family support for adolescent self-esteem and well-being.
Implications, Limitations, and Future Directions
Regardless of contextual differences, perceived family support and self-esteem are two protective factors that should be emphasized in prevention and intervention programs specific to adolescent well-being. School mental health settings have a unique opportunity to develop educational programs that promote self-esteem in youth and emphasize the importance of increasing supportive connections to family members (Costello et al., 2008; Lindsey et al., 2010; Weber et al., 2010). Furthermore, efforts should be made to include family-based support in adolescent treatment models of internalizing disorders, as prior research has demonstrated that family-based intervention has comparable effects on adolescent well-being to individual cognitive-behavioral therapy (Das et al., 2016). Antistigma mental health interventions may also prove beneficial in helping to foster a more supportive peer environment to help buffer the risk of depression or anxiety in adolescence (Costello et al., 2008; Lindsey et al., 2010). Given that those adolescents with reduced socioeconomic advantage are at greater risk, community-based creative activities or Internet-based prevention and treatment initiatives could be better integrated to ensure greater reach for more disadvantaged youth (Das et al., 2016).
This study is not without limitations. First, the cross-sectional design does not permit causal inferences or confirm directions of associations. As such, future studies should consider a longitudinal examination of the current model. Second, the reliance on self-report measures may have inflated associations because of shared method variance. Third, as mentioned earlier, the highly educated sample is not typical of the wider Jamaican population and as such may limit the generalizability of findings. Future studies should sample adolescents outside of urban-based, secondary school settings.
Conclusion
The current study modeled the direct and indirect pathways of two important sources of support and self-esteem on adolescent well-being within a Jamaican setting, while placing emphasis on the familial context that helps to shape these associations. Given the strength of these findings, the results can serve as a guide to both developmental and clinical scientists for use in testing and developing future prevention programs that emphasize family warmth, support, and involvement as protective factors for increasing adolescents’ level of esteem, and decreasing the incidence and prevalence of emotional difficulties. Furthermore, given adolescence is typically a period of heightened emotional arousal, future research should continue to explore both the risk and protective factors, as well as developmental processes that serve to enhance or impair psychological well-being over time among adolescents within Jamaica and the wider Caribbean.
Footnotes
Acknowledgements
The authors thank the students who participated in the study and the parents who gave consent for their participation. They also extend special thanks to Drs. Kai Morgan and Stacey Brodie-Walker, and Mr. Matthew McKenzie who assisted with the organization of this research project and data entry, and Ms. R. Christina Fenton who assisted with the final review. Acknowledgments also to the guidance counselors and administration at the school who assisted with the organization of data collection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.