
Abstract
Multiple aspects of social–emotional well-being have been identified as influential factors in adults’ and children’s physical activity and nutrition. However, the associations between social–emotional well-being, race and ethnicity, and health-promoting behaviors among urban youth remain understudied. This cross-sectional pilot study examines the relationships between social–emotional well-being and health-promoting behaviors. The study also explores how race and ethnicity affect physical activity and consumption of nutrient-dense foods among urban youth ages 11–19 (N = 100) in a small Northeastern city in the United States. The results do not indicate any associations between social–emotional well-being measures and health-promoting behaviors measured as fulfilling physical activity and fruit and vegetable intake guidelines. However, we found significant racial and ethnic differences in health-promoting behaviors. These findings indicate that prevention programs and policies aimed at enhancing urban youth’s engagement in physical activity and consumption of nutrient-rich foods need to be tailored based on racial, ethnic, and cultural contexts.
Introduction
There is a growing emphasis in social work practice to focus on urban youth’s social-emotional health (American Academy of Social Work and Social Welfare, n.d.)—notably the impact of psychosocial challenges on their physical health and well-being. Research has established that youth who lack social support, self-esteem, and/or coping skills are more likely to experience adverse physical and mental health outcomes (Gregory et al., 2020; Liu et al., 2023; Silva et al., 2014; Uchino, 2009). Moreover, youth living in urban communities may experience contextual barriers (i.e., increased stress, limited social connections, etc.) that lead to adverse health effects, such as increased risk of diabetes, high blood pressure, poor sleep, depression, and anxiety (Babey et al., 2016; Buttazzoni et al., 2021; Heller Isner et al., 2017; Hodgkinson et al., 2017).
Most of the research on the health and well-being of youth has focused on physical health problems, particularly adverse health behaviors such as sedentary activities, obesity, and chronic illness (Noonan & Fairclough, 2018). It has been posited that urban youth health behaviors, specifically, may also be affected by psychosocial factors related to their residence in urban communities (i.e., community violence, high crime rates, and poor neighborhood conditions) (Hoying & Melnyk, 2016; Regis et al., 2016; Sandercock et al., 2010). Additional inter- and intrapersonal factors such as family, friends and peer groups, and racial and ethnic identity can also influence youth well-being, dictating youth’s level of engagement in health-promoting behaviors (Poulos & Kulinna, 2022). However, one consistent shortcoming in the existing literature is that the attributes of social and emotional well-being (i.e., social support, sense of mastery, perceived stress, and coping), and health-promoting behaviors (i.e., physical activity and fruit and vegetable consumption) are often understudied among urban youth of color (Anderson Steeves et al., 2016). This pilot study utilizes the ecological systems theory to explore the relationships between social–emotional well-being and health-promoting behaviors among urban youth of color. Our second aim is to fill gaps in the literature by exploring how youth racial and ethnic identities may shape health-promoting behaviors.
Literature Review
Social–Emotional Well-being
Social-emotional well-being encompasses an individual’s ability to recognize and interpret challenges or strain, manage or overcome challenges and perceive their ability to control the outcomes of their lives (Australian Institute of Health and Welfare, 2012; Oberle, 2018). Social-emotional well-being is also informed by the perceived aid, assistance, and encouragement an individual receives from their personal social networks and community, which can impact self-regulation and the ability to navigate challenging times (Australian Institute of Health and Welfare, 2012; Lardier et al., 2019). Together, these factors work in concert to help regulate youth emotions and promote adaptive behaviors (Oberle, 2018). Social-emotional well-being is associated with improved mental health among youth, including decreased levels of anxiety and depression and increased psychological resilience (Australian Institute of Health and Welfare, 2012; Oberle, 2018).
Social-Emotional Influences on Health Behaviors
Social-emotional well-being facilitates improved self-regulation and decision-making, which can lead to healthier lifestyle choices (Oberle, 2018; Thoits, 2011). Existing literature has recognized the ways specific social-emotional components, such as perceived stress, sense of mastery, and level of social support, may influence health-promoting behaviors and outcomes (Caputo, 2003; Infurna & Mayer, 2015; Lai & Ma, 2016; Thoits, 2011). For instance, Thomas and Colleagues (2017) found that strong familial relationships promote positive health outcomes and impact someone’s well-being throughout their life course. Meaningful familial relations affect how individuals tolerate stress, engage in healthier behaviors, and promote higher self-esteem, leading to healthier lifestyles (Thomas et al., 2017). Comparable results were found in Harandi and colleagues’ (2017) meta-analysis, which has confirmed a correlation among social-emotional well-being outcomes. They posited that positive communication with peers and family may have several positive social-emotional well-being outcomes, including reducing anxiety, promoting a sense of security, increasing effective communication, and acting as a protective factor against individual stress. Both studies illustrate the importance of human connection and support, which often negates the negative impacts of isolation and leads to positive health outcomes (Harandi et al., 2017; Thomas et al., 2017). These studies contribute to our understanding of how behavioral patterns adopted during adolescence can influence overall health outcomes in adulthood and increase life expectancy (Infurna & Mayer, 2015; Lawrence et al., 2017). However, few studies focus on the unique needs of urban youth of color and how their social-emotional well-being may affect their engagement in health-promoting behaviors. Applying an ecological systems theoretical perspective may assist us in better understanding how social, environmental, and community-level factors influence health, specifically among urban youth of color.
Social-Emotional Well-Being and Urban Youth of Color Health Outcomes
Urban youth of color contend with increased levels of perceived stress related to poverty, neighborhood conditions (e.g., high crime, elevated levels of pollution, poor housing), community violence, and limited community support (Alicea et al., 2012). The stressors experienced by youth of color are often compounded by discriminatory practices, structural racism and victimization that increase in frequency as they age (Yusuf et al., 2022). Specific subgroups of urban youth are at increased risk of poorer mental and physical health outcomes due to inequalities based on race, gender, geographic location, and socioeconomic status (SES; Acevedo-Garcia et al., 2014; Alicea et al., 2012). In fact, the Centers for Disease Control National Center for Health Statistics’ recent reports indicate that many youths of color, and specifically Black and Hispanic/Latinx youth residing in inner-city communities, have a higher risk of developing obesity and obesity-related illnesses (Centers for Disease Control and Prevention [CDC], 2015, 2017). While national research has shown that sedentary behaviors and limited consumption of nutritious foods in childhood and adolescence often lead to obesity and other chronic illnesses in adulthood, little research has documented the social and emotional indicators that influence health-promoting behaviors among youth and specifically youth of color in urban settings (Lardier et al., 2019).
Theoretical Underpinning
A socio-ecological theoretical approach, including Ecological Systems Theory (EST), provides an inclusive framework for understanding human behavior and, specifically, the behavior of young people during their formative years. As developed by Urie Brofenbrenner, EST describes the functioning of environmental influences by grouping the environmental factors based on proximity to the individual within the micro-, meso, exo-, macro-, and chrono-system levels (Bronfenbrenner, 1989; Sallis et al., 2008). Hence, behavior is shaped by a complex interplay of (a) individual factors, (b) interpersonal relationships, (c) organizational entities, (d) community factors, and (e) systems and policy. Therefore, health outcomes are not simply a result of an individual’s chosen behaviors but are also influenced by outside forces such as social norms and accessibility of resources. The relational layer involves the supportive network of friends, peers, parents, family, community members, and professionals (e.g., teachers, counselors, religious leaders, mentors) who serve as supports. This theory illustrates the influence of multiple interactions that individuals have with their environments and asserts that individuals who receive encouragement, support, and skills from their environment will adopt healthy and safe behaviors. (Bronfenbrenner, 1989; Sallis et al., 2008).
These observations may be influenced by the individual’s microsystem which includes their immediate environment including family and peer relationships (Brofenbrenner, 1989). At the meso-system, interactions between microsystems create a dynamic process called reciprocal determinism where the relationships within the environment influence the individual’s behavior and at the same time their behavior informs the environment, forming a bidirectional relationship (Brofenbrenner, 1989, Sallis et al., 2008). Their interactions with others, coupled with their experiences, sense of mastery, or perceived control over the forces that affect one’s life, can create environments to fit their needs based on their interactions with said environments (Brofenbrenner, 1989; McAlister et al., 2008; Pearlin et al., 1981). The environment cultivated in youth families and within their communities impacts their integration into a larger society, in which their cultural influences and political and economic institutions at the macrosystem level also have a meaningful impact on their development (Brofenbrenner, 1989). Furthermore, an individual’s sense of mastery, social support, and ability to manage environmental stressors influence their overall behavior (Pearlin et al., 1981; Sallis et al., 2008).
In this study, ecological systems theory is applied to explore and discuss areas an understudied research area for urban youth of color. Specifically, this article seeks to delineate the ways in which their families, communities, and societal factors influence social-emotional well-being and encourages engagement in physical activity and consumption of nutrient-dense foods. It further recognizes that youth of color are affected by social influences and environmental interactions. Israel and colleagues (1998) posit that the ecological systems theory is a natural fit for research involving urban adolescents because it recognizes disparities in health status associated with poverty, lack of opportunity, racism, and powerlessness. When youth are actively involved in identifying problems/issues and resources personally and within their community, it offers them an opportunity to work for change, effectively builds resilience to risk, and improves health outcomes (Stokols et al., 2013).
Methods
The data for this cross-sectional pilot study is drawn from the Liberty-Light Healthy Youth Initiative (2016–2017), which surveyed youth (N = 100) in Grades 6 to 12 enrolled in the Liberty Partnerships Program and Summer Youth Employment Programs in a small Northeastern city of the United States. The Liberty-Light Healthy Youth Initiative included an in-person health promotion program that has provided youth with access to nutrition, physical activity, and enrichment activities. Youth participants completed a 54-item Likert-type-style questionnaire examining social support, coping, perceived stress, mastery, physical activity, and fruit and vegetable intake. This comprehensive pilot study investigates the relationship between urban youth of color’s social-emotional well-being and their health behavior based on nutrition and physical activity. The study is also interested in differences in their health-promoting behaviors, given the diversity of the youth population in the program. Institutional Review Board Office of Regulatory and Research Compliance at the co-authors’ university reviewed and approved ethical and safety considerations for recruiting and surveying youth participants.
Research Questions
Assessing urban youth’s health-promoting behaviors requires examining the contexts influencing their overall social-emotional well-being, their racial and ethnic backgrounds, and how they are associated with health-promoting behaviors. To overcome the limited evidence of the topic, this study seeks to explore the following research questions using a diverse sample of urban youth:
Participant Recruitment
Youth were enrolled in the pilot study based on recruitment that occurred at three local public schools (two middle schools, one high school), and youth-focused programs (Liberty Partnerships Program and Summer Youth Employment Program) working collaboratively on the Liberty-Light Healthy Youth Initiative within a small Northeastern U.S. urban city (population <100,000). Eligible participants were residents of the city, ages 10–19, English-speaking, obtained parental consent to participate and provided assent to participate in the study. Recruitment included mailing a recruitment letter to parents/guardians of youth participating in the youth-focused programs engaged in the Liberty-Light Healthy Youth Initiative explaining the nature and details of the study and requesting their consent for their youth to participate in a voluntary and anonymous research study. Convenience sampling methods were employed to recruit participants where any parent who received recruitment materials and were willing to provide consent for their youth’s participation were able to voluntarily enroll their youth in the study.
Youth who received parental consent were provided a youth recruitment letter explaining the nature and details of the study in layman’s terms and met with members of the research team to learn more about the study in plain language. After youth were well informed of the study, they were given the option to voluntarily provide assent to participate if they wished to move forward as participants in the study. Both parents and youth were made aware that participating in this study had no bearing on the youth’s participation in any extracurricular activities, their schooling, or youth-focused programs they were enrolled in, and they would be able to withdraw from the study at any point. All youth participants received a US$10 gift card for completing the study questionnaire and their parent or guardian received a US$5 gift card incentive for their support in coordinating their youth’s participation.
The study’s final sample was relatively small (N = 100) due to the limited resources available to conduct the study and its exploratory nature. This pilot study was proposed as a preliminary exploration of the association between the variables tested with the intent of developing a larger study using a representative sample.
Measures
Health-Promoting Behaviors
Physical activity was measured using the Patient-Centered Assessment and Counseling Exercise plus Nutrition (PACE+) Physical Activity Screening Measure specifically designed for use with adolescents (Prochaska et al., 2001). The measure includes two questions where youth self-report: (a) number of days they spent engaging in physical activity in the past 7 days and (b) the number of days they spent engaging in physical activity in a typical week. Youth could select the number of days in the past 7 days and a typical week of their lives that they engaged in physical activity based on their lived experience (1–7 days) for each question.
We calculated youth responses to each question (1–7 days) for an average score (
Fruit and vegetable intake was measured using the Patient-Centered Assessment and Counseling Exercise plus Nutrition (PACE+) Physical Activity Screening Measure (Prochaska & Sallis, 2004). Fruit and vegetable intake is determined based on youth responses to two questions regarding the number of servings of fruit per day (0 indicating fruit was not consumed at all and 4 indicating four servings or more were consumed) and the number of servings of vegetables they consume on a typical day (0 indicating vegetables were not consumed at all and 4 indicating four servings or more were consumed) (Prochaska et al., 2001, 2004). A chart with examples of a serving of various fruits and vegetables was provided to youth to help them determine the appropriate response that is aligned with their consumption. Youth responses to both questions were averaged (
Social-Emotional Well-Being
Guided by the previous research, the study uses four aspects of social-emotional well-being, John Henryism, mastery, perceived stress and social support, to explore the relationship between social-emotional well-being and health-promoting behaviors. The John Henryism Scale for Active Coping developed by Sherman James (1994) was used to measure youth’s use of resources to overcome challenges. This coping measure is constructed based on a sum of the 12 items where increased scores demonstrate a strong sense of mastery and tenacity when dealing with stressors (Adkins-Jackson & Levine, 2020; Fernander et al., 2003). This measure was specifically designed to be culturally congruent among people of color, incorporating the compounding stressors minoritized individuals face in everyday life (Hsieh et al., 2014). A test indicates α = .826, suggesting strong reliability.
Mastery is examined through a seven-item measure where greater mastery is indicated through higher mean scores (Pearlin et al., 1981). The measure examines how individuals perceive they have power over their abilities and their life outcomes and has been widely used among diverse groups (Rose et al., 2017). Youth with a strong sense of mastery have a more positive self-esteem and adaptive coping capacity. Pearlin et al.’s (1981) mastery measure demonstrated a good internal consistency with an α = .697 for our sample, acceptable given the measure had less than 10 items.
Perceived stress was measured using the Perceived Stress Scale (PSS-10) to examine how youth interpret stressful situations that may affect their physical or mental health (Cohen et al., 1983). The measure utilizes 10 items to assess how individuals interpret stressful situations that may affect their health and well-being. Items from this measure include, “In the last month, how often have you found that you could not cope with all the things you had to do?” and youth responded using a 5-point scale (0 = never, and 4 = very often). Scores of 13 are considered average, and scores over 20 indicate high stress. The PSS-10 measure used in this study is frequently used as a measure of stress because of its reliability and validity in youth and adults (Felton et al., 2017; Yeager et al., 2014). In the current sample, internal consistency was appropriate with α of .757.
Social support is examined through nine items from the National Survey of Black Americans developed by James and Gurin (1997). The items extracted from this instrument use Likert-type-style questions to identify how youth perceive their social networks (friends and family), the closeness of their relationships, and if they receive the same level of support that they offer friends and family. The questions were explicitly structured to capture Black Americans’ experiences effectively and efficiently (Jackson et al., 2003). This measure was tested for reliability, yielding a Cronbach’s α = .692, which is acceptable for a measure with less than 10 items.
Statistical Analysis
Data analysis was conducted using SPSS version 27. Due to the small sample size, the statistical significance level was set at a .05 level in all analyses. Descriptive information on each of the health behavior items was tabulated for the total sample and by race/ethnicity. Crosstabulations were produced by race for physical activity and fruit and vegetable guidelines as set by the United States Department of Health and Human Services (DHHS) (dependent variables). Analysis of Variance and Chi-Square tests were used to explore bivariate relationships. The two sets of logistic regression models estimated (a) The likelihood of fulfilling physical activity guidelines predicted by social-emotional well-being and race and ethnicity and (b) the likelihood of fulfilling the fruit and vegetable consumption guidelines predicted by social-emotional well-being.
For each of the dependent variables, four models were evaluated. Each model included one social-emotional well-being measure, race and ethnicity and the control variables. The results of the binary logistic regression analyses are presented as a series of odds. The baseline odds are set to 1.0. An odd ratio (OR) > 1.0 indicates a positive association between the factors of interest and OR less than 1.0 indicates the inverse. We calculated the 95% confidence intervals (95% CI) for statistically significant OR.
Results
Sample Characteristics
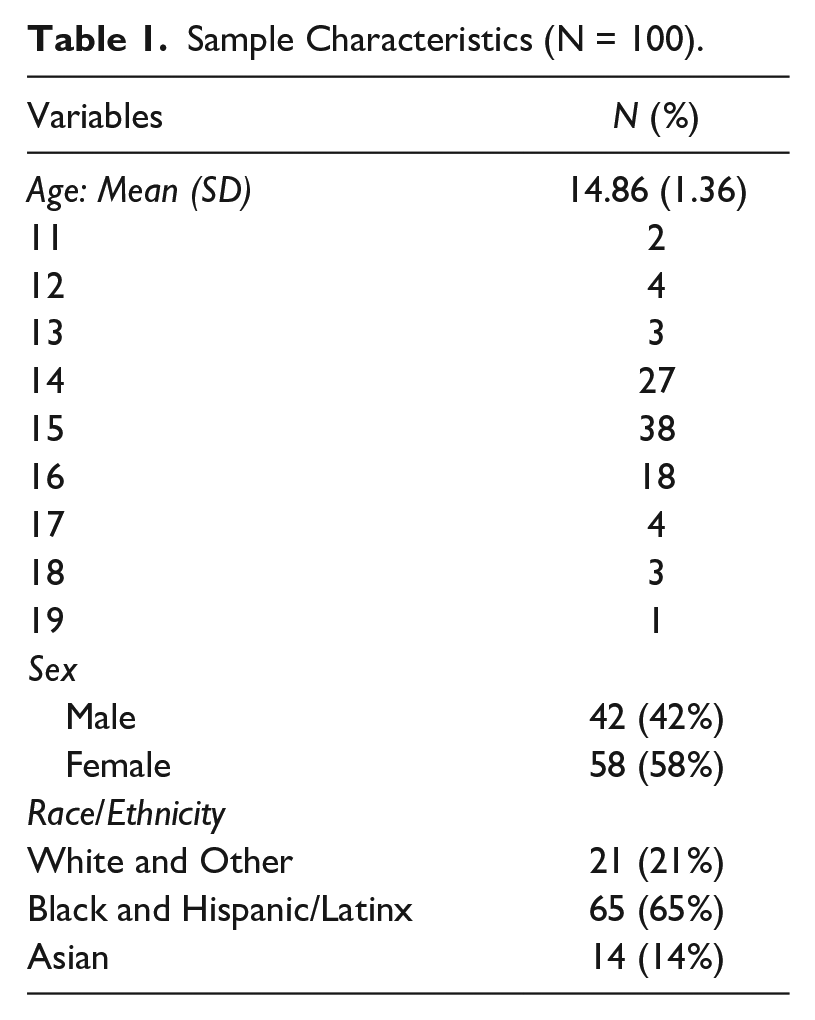
Table 1 shows the demographics of the sample where participants (N = 100) self-identified as 58% female, and the median age was 15 years (M = 14.86, SD = 1.356), with race examined as three categorical variables: Black and Hispanic/Latinx, Asian, and white and Other. Given the small sample size and similarities of the means in social-emotional well-being variables, we combined Black or African Americans and Hispanic/Latinx as one group. Given the presence of a large Asian identified youth in the sample, we created a separate Asian category. Black and Latinx make up the largest group in the sample (65%), followed by white and Other (21%) and Asian (14%).
Sample Characteristics (N = 100).
Health-Promoting Behaviors by Race and Ethnicity
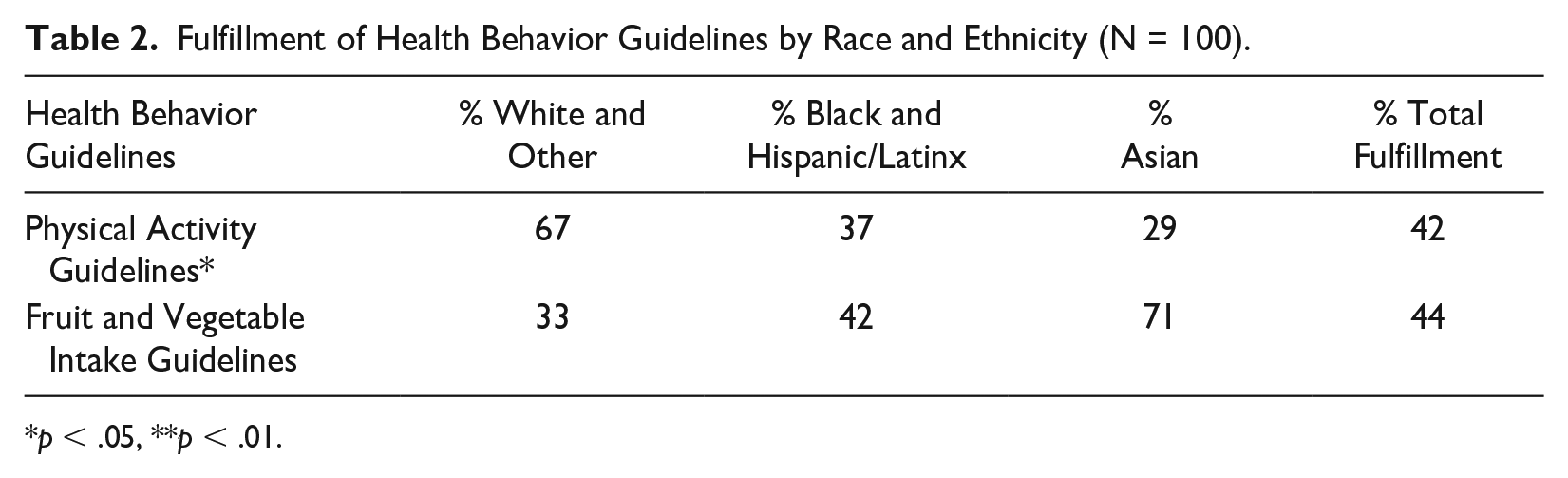
Overall, 42% of the sample fulfilled the physical activity guidelines and 44% fulfilled the fruit and vegetable guidelines (see Table 2). Results demonstrate statistically significant differences in prevalence across racial and ethnic groups. Black and Latinx (63%) and Asian (71%) youth in the sample did not fulfill the physical activity guidelines while about two-thirds of white and Other youth (67%) were fulfilling the guidelines. On the second outcome, fulfilling fruit and vegetable consumption guidelines, significant differences were found by race and ethnicity, but in different directions. While Black and Latinx youth (58%) did not fulfill the current guidelines; most Asian youth (71%) did. The majority of white and Other youth (67%) did not meet the fruit and vegetable guidelines.
Fulfillment of Health Behavior Guidelines by Race and Ethnicity (N = 100).
p < .05, **p < .01.
Predicting Health-Promoting Behaviors
Table 3 presents the first set of logistic regression results for fulfilling physical activity guidelines (yes or no) by social-emotional well-being indicators and race and ethnicity. After controlling for age and sex, mastery was not statistically significant. However, compared with white and Other youth, Black and Latinx youth were 70% less likely to fulfill physical activity guidelines while Asian youth were 80% less likely to fulfill physical activity guidelines (Table 3, Model 1). Active coping was not significant in the second model, but results indicated that compared with white and Other youth, Black and Latinx youth were 73% less likely to meet the physical activity guidelines. The third model found that perceived stress was not significant, while Black and Latinx youth were 68% less likely to meet physical activity guidelines compared with white and Other youth. Neither social support nor race and ethnicity were significant in the model with physical activity. A second set of logistic regression models was conducted to determine the likelihood that youth were fulfilling the guidelines for fruit and vegetable consumption (see Table 4). Social-emotional measures, mastery, active coping, perceived stress, and social support were insignificant predictors. However, there was a significant association between race and ethnicity and fruit and vegetable consumption in the last model. Specifically, Asian youth were nearly 5 times more likely to fulfill the fruit and vegetable consumption guidelines, compared with white and Other youth, but only in the model examining social support.
Logistic Regression Estimates of Social-Emotional Well-Being Factors and Race on Physical Activity.
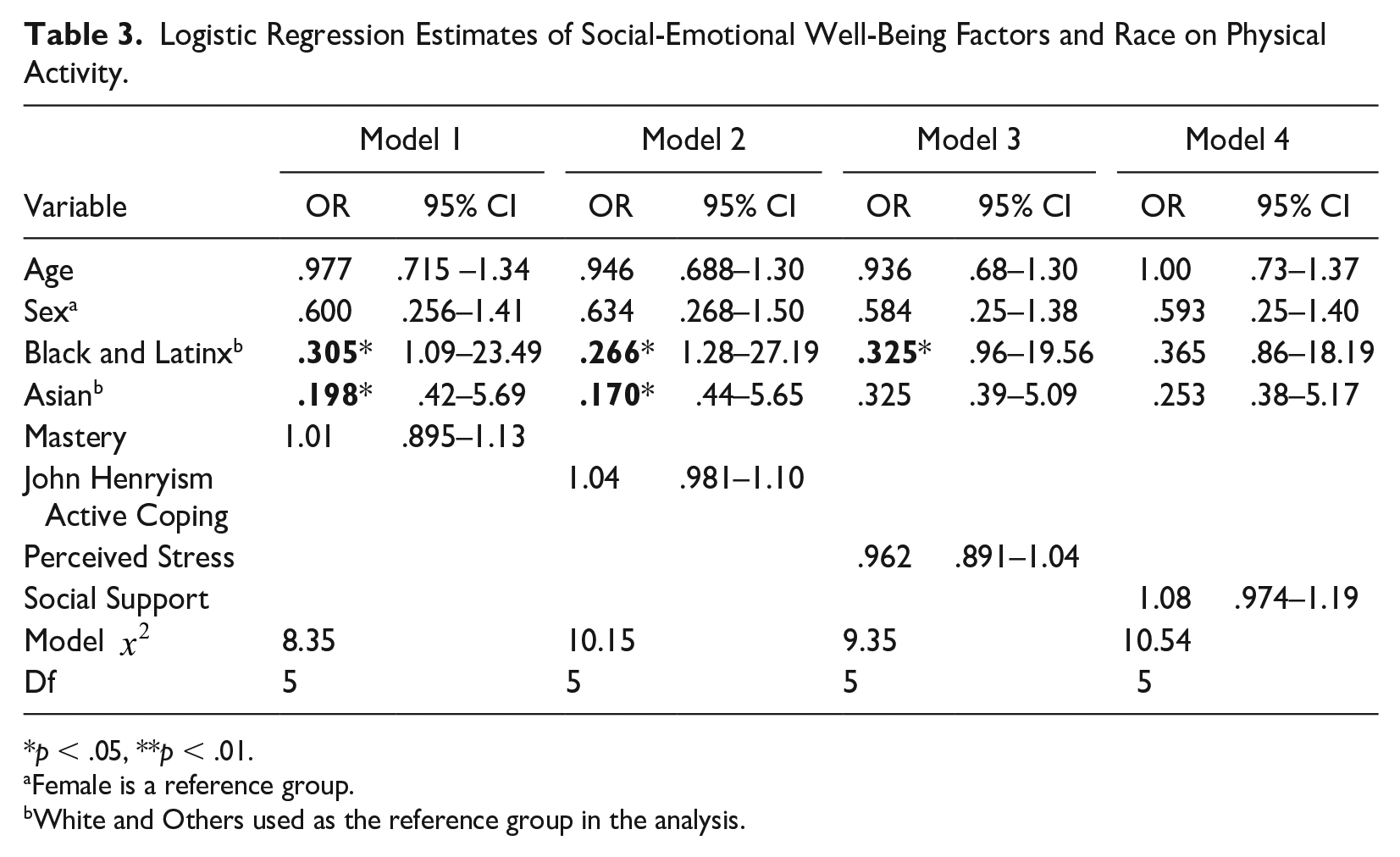
p < .05, **p < .01.
Female is a reference group.
White and Others used as the reference group in the analysis.
Logistic Regression Estimates of Social-Emotional Well-Being Factors and Race on Fruit and Vegetable Intake.
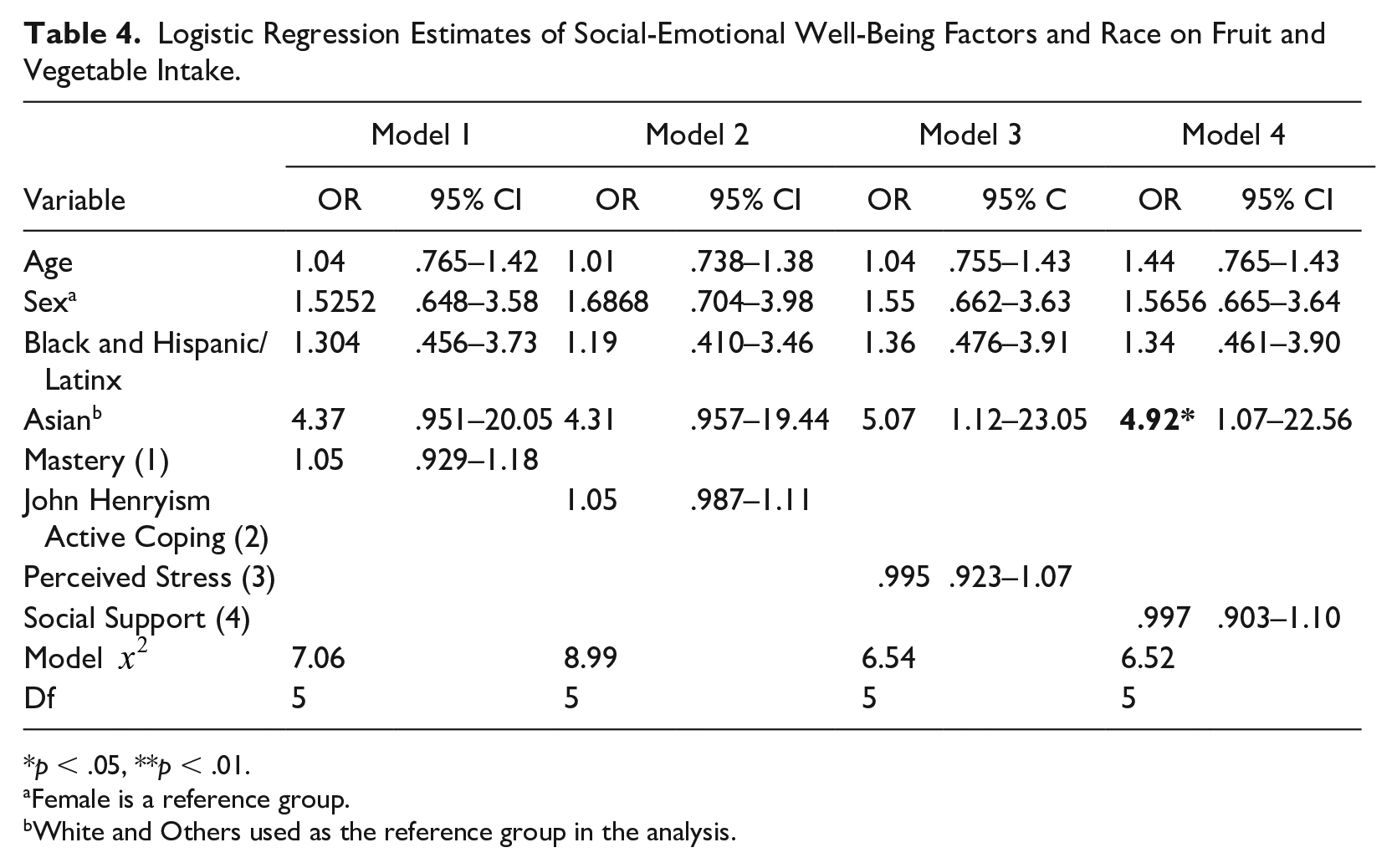
p < .05, **p < .01.
Female is a reference group.
White and Others used as the reference group in the analysis.
Discussion
Our study’s results indicating no statistically significant associations between social-emotional well-being and health-promoting behaviors were unexpected. However, the study’s findings add to the existing evidence of racial and cultural differences in engagement in health-promoting behaviors among youth (Chen et al., 2021; Hasson, 2018) Youth’s race and ethnicity were significant predictors of healthy eating and optimal physical activity, but their effects were not in consistent directions.
Chen and colleagues (2021) have found comparable outcomes in their analysis of the Youth Risk Behaviors Survey, where 14- to 17-year-old Asian youth were less likely to fulfill physical activity guidelines than white youth. However, differences were large in our study. According to Fulton (2020), physical inactivity is more common among racial and ethnic minorities. The Latinx population has a physical inactivity rate of 31.7%, and the non-Hispanic Black population’s rate is around 30%. These disparities significantly impact the health and well-being of these communities. A study of measuring changes showed increases in physical activity among non-Hispanic white youth over time but not among Mexican American or non-Hispanic Black youth, suggesting a possible disparity in physical activity (Gortmaker et al., 2012). Research has linked the lack of physical activity to obesity. In one such study, 12- to 15-year-old Mexican American youth were identified as the least active group in the sample, and they had had the highest prevalence of obesity (Belcher et al., 2010).
The lower levels of physical activity among Black and Latinx youth participants in this study may be attributed to neighborhood and community factors, including limited accessibility to safe and convenient places for physical activity, such as community parks, trails, and sidewalks. Research has shown that urban youth are less likely to engage in physical activity and consume adequate amounts of nutrient-dense foods than rural and suburban youth (Kim et al., 2021; Williamson et al., 2020; Wolfe et al., 2020). For instance, Kasehagen and colleagues (2012) examined neighborhood characteristics (e.g., poverty, access to parks and recreation centers, presence of sidewalks) and physical activity levels among youth in rural and urban communities. This study found that youth living in suburban and/or rural areas were more likely to engage in 20 minutes of physical activity, 5 days per week, compared with their urban counterparts (Kasehagen et al., 2012; Sandercock et al., 2010). Youth in rural and suburban communities also have more opportunities to engage in physical activities through increased access to recreational green spaces and spend less time engaged in sedentary behaviors. Residing in rural communities increases the likelihood of youth engaging in active leisure and increased physical activity levels compared with youth in urban communities, regardless of sex or age (Regis et al., 2016; Sandercock et al., 2010).
The results on the consumption of nutrient-dense foods among urban youth showed that while the effects of social-emotional well-being were insignificant racial/ethnic differences were significant. Our results of the increased likelihood of healthy eating by Asian youth are in alignment with results from previous studies. For example, Allen and colleagues (2007) utilized data from the California Health Interview Survey to examine risk behaviors among Asian and Latino youth in comparison to white youth and found that Asian youth consumed more servings of vegetables on a daily basis, in comparison to white youth. A cross-sectional study on fruit and vegetable intake among Hispanic middle school youth (Dave et al., 2009) found an association between lower fruit and vegetable consumption and acculturation, food insecurity, and demographic variables. Their results suggest that fruit cultural factors strongly influence fruit and vegetable consumption, which explains why Asian and Hispanic youth with lower levels of acculturation were consuming more fruits and vegetables.
Implications for Practice
This study’s results of this study have several implications for social work practice interventions to improve health outcomes for youth of color and future research. We believe that enhancing urban youth’s health-promoting behaviors requires the development of social work practice that is culturally relevant for diverse groups. Understanding cultural and social contexts behind youth behaviors would allow practitioners to develop effective service models and programs.
We also believe that social work practice models focused on socio-emotional well-being remain important given the evidence (Hoying & Melnyk, 2016). One such example of utilizing evidence-based interventions to enhance youth well-being and health behavior is the Creating Opportunities for Personal Empowerment (COPE) Healthy Lifestyle TEEN (Thinking, Emotions, Exercise, and Nutrition), an intervention that may support physical and mental health outcomes among urban youth (Hoying & Melnyk, 2016). This pilot program was facilitated among middle school urban youth with increased health promotion and education opportunities for underserved youth. Similarly, Howie and colleagues (2020) found a that many cross-sectional studies promoting youth sports participation to increase physical activity indicated a strong connection between social relationships and engagement in physical activity. Hu et al. (2021) also found that ethnicity, self-concept, and social support were positive predictors of physical activity among adolescents. Adapting interventions geared toward improving the social-emotional well-being of youth of color through racial and ethnic identity promotion may also support the development of evidenced-based treatment models to address mental and physical health outcomes among at-risk urban youth who otherwise would not have access to this level of assistance.
The findings also warrant social workers’ engaging in early intervention efforts, which support clinicians in better understanding sociocultural and psychosocial risk factors that may impact youth of color. Social workers should collaborate with youth and their families to allow them to feel sovereignty and include peer-led programs to increase accessibility in positive peer interactions. For instance, Revell and McLeod (2016) explored the benefits of walk-and-talk therapy, a counseling approach in which the counselor and client walk together outdoors during therapy sessions and found meaningful physical and mental health improvements among client participants. The findings indicated that clinicians engaging in walking sessions with their clients could offer holistic services that contribute to greater overall well-being, aid clients in overcoming feelings of being stuck, and enhance their physical wellness (Revell & McLeod, 2016).
Implications for Policy
Study findings suggest a need for policies that enhance and promote the overall well-being of youth in urban communities, emphasizing the need to increase physical activity and nutrient-dense food consumption among urban youth of color. As previously mentioned, youth in urban communities need better access to resources supporting physical activity. Hasson (2018) identifies several systemic barriers to physical activity that affect African American and Latino youth, such as limited access to safe places to exercise and physical activity equipment in the places they reside. Similarly, Huang and colleagues (2020) found that Asian and Latino youth were less active in neighborhoods that were not in close proximity to parks. They also found a positive association between park use and physical activity in parks and walkability-related features among Asian, Latino and African American youth residing in urban communities (Huang et al., 2020). The condition of neighborhoods, which encompasses safety concerns, lack of access to green spaces, and low access to play areas, inform the accessibility of spaces where youth can engage in physical activity. Creating policies that support communities in mitigating these challenges would have a meaningful impact on urban youth. One example of a policy change that may positively influence engagement in physical activity among urban youth is the creation of designated areas for youth to walk and play, and developing neighborhood gardens where youth feel like they can contribute to their community. The investment of community funds to develop dedicated spaces must also include increasing indoor physical activity spaces for the colder months to promote healthier lifestyle habits among youth and their families.
In addition to supporting the engagement of physical activity, enhancing the well-being of urban youths of color includes the promotion of fruit and vegetable consumption. Currently, the United States federal government sponsors programs that allow families to access fresh and healthy foods, such as Women, Infants and Children (WIC), SNAP food benefits, and Free School Meals for Children for those who qualify. However, consumption of fresh, nutrient-rich food remains low among at-risk, low-income, and urban families due to higher prices, complicated applications, and stigma surrounding government-related support (Bensley et al., 2014; Nguyen & Powell, 2015). A study examining mixed- status Mexican families’ access to WIC benefits found a negative association between the risk of deportation and the use of the program. This finding suggests that low-income, at-risk youth may not be able to access this critical program and obtain appropriate amounts of nutrient-dense foods based due to fear of immigration repercussions. A study examining the effects of increasing SNAP benefits through the American Recovery and Reinvestment Act did not find any changes in diet quality among low-income youth (Hudak et al., 2021). These findings suggest that there is an unmet need based on the assumptions made regarding the types of foods low-income families will purchase through SNAP benefits, where many low-income families consist of heads of households who are working long hours or multiple low-wage jobs to make ends meet and may not have the time to prepare foods made with fresh foods, relying on already prepared foods with less nutritional value (Hudak et al., 2021; Smith et al., 2013). Increasing SNAP benefits and reducing restrictions on the types of foods purchased with benefits may help address this issue (Hudak et al., 2021). In addition, Ball et al. (2018) suggest implementing education-based campaigns to improve access to nutrient-rich foods through vendors, such as the WIC farmer’s market and lead to increases in fruit and vegetable consumption. Specifically targeting families at higher risk of decreased fruit and vegetable consumption and overall food insecurity, many of which are communities of color in urban settings, may improve their likelihood of consuming nutrient-dense foods. These policies would also have a consequential impact on increasing resources for communities in general, such as reducing community violence and creating safer neighborhoods.
Study Limitations
Several limitations must be considered in this study. First, data were collected using a self-administered questionnaire where study participants self-reported information about their racial and ethnic identity, social-emotional well-being and health-promoting behavior (fruit and vegetable intake and physical activity). There is a risk of inaccuracy or inconsistency of self-reported data (i.e., study participant may under or overestimate their responses) and there is a potential for social desirability biases. Second, the small sample size impacts the adequacy of statistical power and increases the risk of type 2 errors. The limited sample size and risk of error also create a vulnerability to small effects and large variability. It is unclear why the social-emotional well-being factors did not predict physical activity and fruit and vegetable consumption among the sample. However, we suspect that the lack of robust statistical power may have been an issue for our study. Finally, this study used a cross-sectional design preventing the assumption of causal inferences and long-term trends also cannot be established.
Need for Future Research
Future research may address the limitations in this study’s exploration of urban youth’s social-emotional well-being, race and ethnicity, and health-promoting behaviors. Continued inquiry on this subject should encompass a larger sample to strengthen statistical significance and increase the generalizability of results. Existing research suggests that socio-economic status (SES), parental education level, neighborhood factors, gender and sexual minority status, and access to adequate health care (availability and cultural competency of providers, and health insurance coverage) contribute to health-promoting behaviors among youth and adolescents (Babey et al., 2016; Kim et al., 2021). A large sample will allow the delineation of racial and ethnic groups so, we have more clarity on understanding cultural contexts while accounting for social economic status. The inclusion of data on neighborhood characteristics would also provide a deeper understanding of environmental factors and their influence on urban youth of color’s social-emotional well-being, participation in physical activity, and consumption of fruit and vegetables. Future research should also include an investigation of the influence of self-esteem on youth’s sense of mastery, the ways stressors are internalized, and the implementation of adaptive and maladaptive coping skills (Liu et al., 2023). Any future investigations of youth social-emotional well-being should also encompass qualitative data to provide an in-depth understanding of other contributing factors and how they may contribute to their psychosocial functioning based on the youth’s perspective (Lardier et al., 2019).
Continued research must explore the effects of social support (i.e., aid, assistance, or encouragement from friends, family, school, religious groups, or professional help) and its relationship to health-promoting behaviors such as physical activity and consuming nutrient-rich foods such as fruits and vegetables. In addition, research is needed to bridge the gaps between psychosocial attributes (e.g., sense of mastery, coping ability, and perceived stress), environmental factors, and social supports to enhance urban youth’s and specifically, urban youth of color’s health outcomes and overall well-being. Studies aimed at developing a more in-depth understanding of this relationship may provide compelling data and resources to address rising incidents of physical and mental illness among this population.
Conclusion
The findings of this study emphasize the critical need to enhance urban youths, and specifically youth of color’s, engagement in physical activity and consumption of nutrient-dense foods like fruits and vegetables. Resonating with the existing literature, the results of this study revealed racial and ethnic differences in following guidelines toward healthy development among urban youth. Urban youth of color, specifically, are at increased risk of adverse health outcomes when their social-emotional well-being is compounded with additional environmental and societal risk, restricting their ability to engage in health-promoting behaviors (Alicea et al., 2012; Kasehagen et al., 2012).
The disproportionately low engagement in health-promoting behaviors among urban youth of color is likely a contributing factor in the increased rates of obesity and obesity-related health concerns in this group (Kasehagen et al., 2012; Skinner et al., 2018). Adding to this growing concern are the rates of obesity and obesity-related health issues that are persisting into adulthood, shortening life expectancy, and adding to the rapid growth in the development of chronic illnesses among communities of color (Acevedo-Garcia et al., 2014; Otto et al., 2017; Pivovarov et al., 2015; Skalamera Olson et al., 2017). It is crucial to invest in efforts that increase opportunities to engage in physical activity and make the consumption of fruit and vegetables accessible to address the rapidly growing health disparity in the development of preventable chronic illnesses in our society. For social work practitioners, researchers, and policy advocates, it is especially important to continue to develop innovative methods of addressing racial disparities in health-promoting behaviors. Additional study in this area will assist social work practitioners and researchers in the development of preventive intervention methods to support this population (DHHS, Agency for Healthcare Research and Quality, 2022).
Footnotes
Disposition editor: Cristina Mogro-Wilson
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.