
Abstract
In dengue endemic regions, a chief complaint of nocturnal fever often is a pathognomic phrase that triggers an investigation for dengue. This article looks at cases of patients who were tested for dengue based on their symptoms of weakness and loss of appetite, without fever as fever was absent in most cases. The article also examines the changes in weight that occur after diagnosis of dengue and compares it to weight loss (if any) that occurred prior to the diagnosis. Dealing with the anorexia and weight loss is challenging for physicians, patients and family members.
Introduction
Dengue is caused by the dengue virus (den1-4), which is a Flavivirus (RNA), spread via the Aedes aegypti mosquito. It is prevalent in tropical climate countries, as the environment is ideal for breeding mosquitoes. Approximately 100 million people are affected by dengue yearly, making it a leading cause of death in the tropical and subtropical regions. 1 Its effects range from asymptomatic to death due to fulminant shock and haemorrhage.
Symptoms include sudden onset of fever, headache, retro-orbital pain and back pain, along with severe myalgia giving rise to the colloquial designation ‘Break-bone fever’. Additional symptoms include anorexia, nausea or vomiting, marked cutaneous hypersensitivity and a macular rash, starting at the trunk and spreading to the extremities of the face. 2 Fever being the prevalent symptom, dengue is also often referred to as dengue fever. In a review of dengue on the following websites – CDC.gov, medicinenet.com, webmd.com, medlineplus.com and Wikipedia.com – anorexia is not listed as a symptom. It is presented as a mere footnote in Harrison’s Principle of Internal Medicine 2 and World Health Organization 2009 Guidelines for diagnosis, treatment, prevention and control of dengue. 3 It is however included in The Principles of Medicine in Africa. 4
Since most clinicians are trained to recognise fever as the primary symptom, its absence may cause this entity to go undiagnosed. The fact that anorexia was the main presenting complaint in our cohort of geriatric patients underscores the importance of this observation, since subsequent malnutrition and weight loss may complicate recovery.
We present a collection of 10 cases seen at Mercy Clinic – NHI in Belize, Central America from August to September 2013.
Case reports
From August to September 2013, there was a spike in the number of dengue cases seen at the clinic. On average, during the rainy season, there is about one case per month. This year, over a 6-week period, there were 10 confirmed cases.
The two most common presenting symptoms of the 10 patients that triggered testing for dengue were chief complaints of loss of appetite and/or feeling weak. Of the 10 cases, only one presented with a chief complaint of fever, while another said he had chills, but the chief complaint was loss of appetite and/or weight.
The cases examined the following parameters: age; sex; weight at 3, 2 and 1 month prior to diagnosis, at the time of diagnosis, and 1 month after (if available); symptoms – fever, rash, headaches, body aches, bleeding, loss of appetite and weakness; labs – IgG, IgM and CBC. Whether or not the patient was diabetic was also recorded.
The average age of patients was 71.9 years. There were four male patients and six female patients. The two most common presenting symptoms that patients complained of were loss of appetite (8 out of 10) and weakness (9 out of 10). Conversely, only two of the 10 patients complained of fever, none complained of rash or bleeding, two complained of body ache and one complained of a headache (Figure 1).
Symptoms patients presented with at the time of diagnosis with dengue.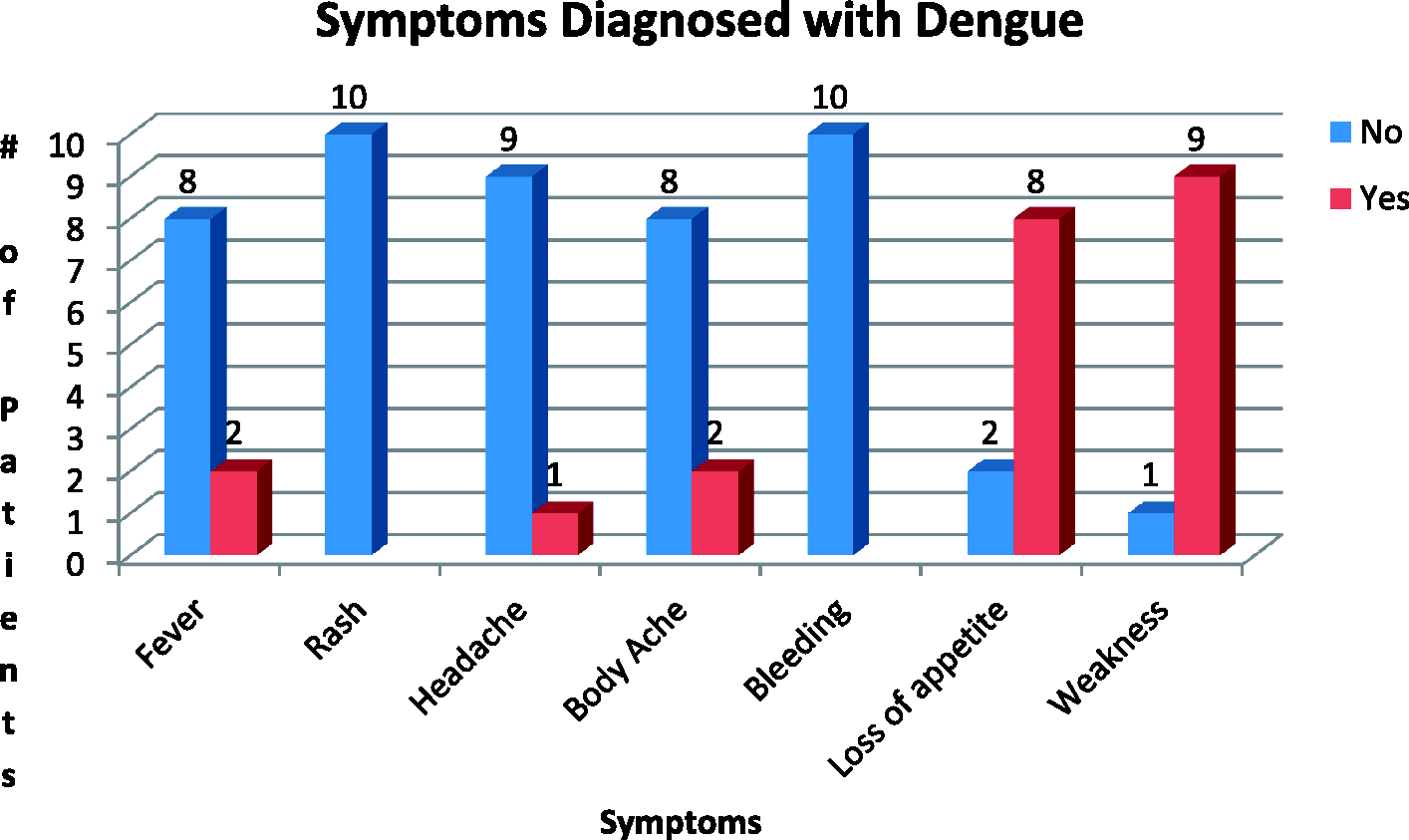
A lack of appetite could lead to a change in weight; hence, the weight changes pre and post diagnoses of dengue were examined to insure that the weight loss was attributed to the dengue and not to any pre-existing conditions. The overall weight difference before diagnosis was an average weight gain of 0.25 lbs (0.11 kg). At the time of diagnoses, the average weight loss was 7.3 lbs (3.31 kg), with the most dramatic weight losses being 24 lbs (10.9 kg) and 15 lbs (6.8 kg) in 1 month or less (Figure 2).
Average weight change (lbs) that occurred during dengue.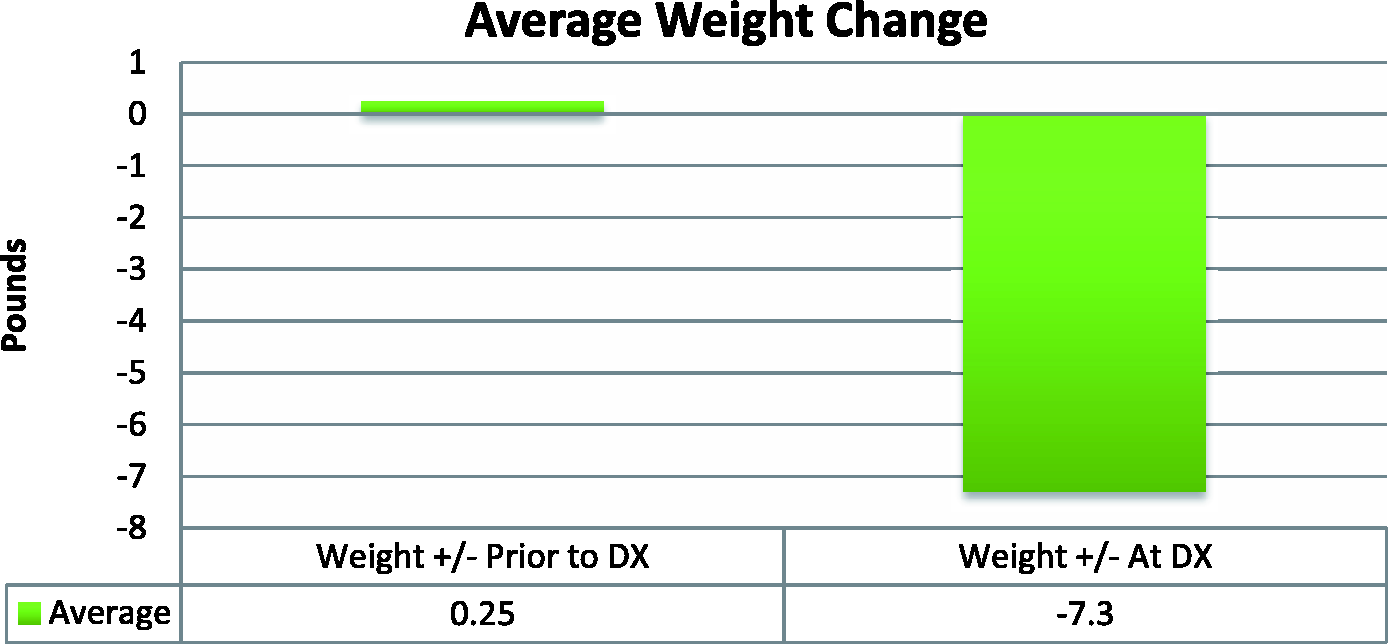
Testing was done using the Dengue Rapid Test at a local laboratory. It should be noted that in the 6-week period, a total of 10 patients were tested and all were IgM positive, and eight were IgG positive. A positive IgM indicates that the patients were either currently or very recently infected. Only one patient’s platelet count fell below the 150,000 µL level at 89,000 µL. It was followed up 2 days later where it increased to 112,000 µL. The patient denied any history of bleeding. Four patients were diabetic.
Management and outcome
There are no specific antiviral drugs for dengue; however, maintaining proper fluid balance is important. 5 Treatment is supportive, varying from oral rehydration therapy at home with close follow-up, to hospital admission with administration of intravenous fluids and/or blood transfusion. 3 In our cases, all 10 patients were treated as outpatients, and no hospital admission was required; of the two patients who had noted fever as a symptom, both were afebrile at the time of the clinic visit. Acetaminophen (Paracetamol) was recommended, along with rest and oral rehydration, as a standard treatment for all patients. The dosage of hypoglycaemic agents for diabetics was adjusted according to their anorexia.
Unintentional weight loss and under-nutrition are common problems in the elderly.6–9 Our patients were advised to add a liquid high energy dietary supplement.
Discussion
Although fever is the hallmark symptom of dengue/dengue fever, testing for dengue in the absence of fever may be necessary for geriatric patients in endemic regions. There is no dispute with the guidelines put forth by the World Health Organization, but an additional awareness of symptoms of anorexia in geriatric patients should be closely followed up. Anorexia can wreak havoc for an elderly patient. Furthermore, complications can arise if the patient is taking a concomitant medication that can reasonably lead to hypoglycemia.
An unintentional decline in weight is always a great cause for concern. A positive dengue test, with no previous history of weight loss, may lead to the reasonable conclusion that the weight loss is due to the dengue.
A sudden decline in strength was also a very prevalent symptom. While it is a subjective feeling that cannot be quantified, it is a very important piece of information.
‘Globally, the reported incidence of dengue has been increasing. Although climate may play a role in changing dengue incidence and distribution, it is but one of many factors; given its poor correlation with historical changes in incidence, its role may be minor. Other important factors potentially contributing to global changes in dengue incidence and distribution include population growth, urbanization, lack of sanitation, increased long-distance travel, ineffective mosquito control, and increased reporting capacity.’ 1
Conclusion
It is important for physicians to test for dengue if a geriatric patient in an endemic region (Figure 3) presents with chief complaint(s) of anorexia and/or weakness in the absence of fever. Part of the treatment plan should include counselling on nutrition and liquid supplemental diets to help improve outcome and mitigate or even reverse any weight loss that may have occurred secondary to anorexia. Sometimes it is not the disease itself that causes the greatest concerns to the patients and healthcare providers, but rather what ensues afterwards.
WHO 2011 map of countries where dengue has been reported.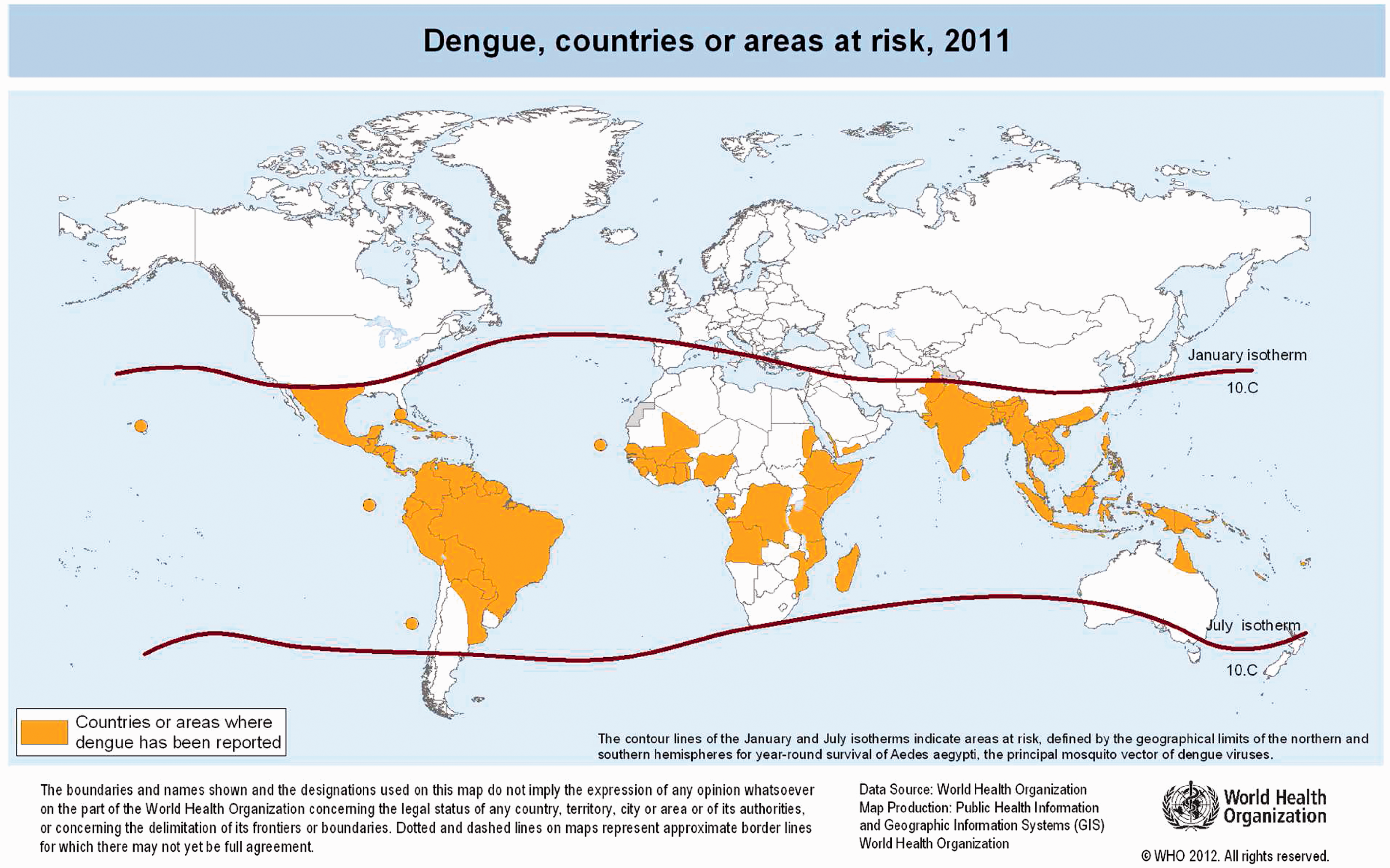
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.