
Abstract
Visceral leishmaniasis (VL) has been reported in the last decade from the hilly state of Uttarakhand, India. We report 47 cases from the non-endemic Garhwal region of this state which, over the last 10 years, were treated successfully. We conclude that the transmission cycle of VL is established in this region. Effective vector control measures are warranted to prevent the disease becoming a health problem, albeit not a major one given its excellent response to drugs.
Introduction
Visceral leishmaniasis (VL) mainly affects poor people in Africa, Asia and Latin America, and is associated with malnutrition, population displacement, poor housing, weak immune system and lack of resources.1–3 A recent review shows that over 98 countries and territories are endemic for leishmaniasis. It is estimated that approximately 0.2–0.4 million of new VL cases and 0.7–1.2 million of new cases of cutaneous leishmaniasis occur each year worldwide. More than 90% of global VL cases occur in six countries: Bangladesh, Brazil, Ethiopia, India, South Sudan and Sudan. 4 Global health observatory data show new cases of VL being consistently reported from India; 20,571 new cases were reported in 2012. 5
The existence of a pocket of the disease and vector, predominantly Phlebotomus argentipes, in the Kumaon region of the non-endemic north Indian hilly state of Uttarakhand has already been substantiated. 6 We reported the presence of VL and its drug sensitivity from the Garhwal region of Uttarakhand in 2007, 7 which is located at a similar altitude of 1500—2500 m above sea level. Over the last 7 years, many more cases of VL have come to the fore suggesting the establishment of a hotspot of VL in the Garhwal region as well. We undertook this hospital-based retrospective study to analyse the demographic characteristics, the clinical, haematological and biochemical profile of the patients and the outcomes of VL in this region.
Methods
All patients of VL consecutively diagnosed and treated at the single tertiary referral centre of the Garhwal region of the north Indian state of Uttarakhand presenting over the last 10 years were included in the study. The clinical and laboratory data were retrieved from the hospital records and the outcomes were ascertained from the hospital records as well as contacting the people on telephone wherever possible.
Analysis of the demographic, clinical, biochemical and haematological data was performed and the mean was used as the measure of central tendency and standard deviation as the measure of dispersion for descriptive statistics.
Results
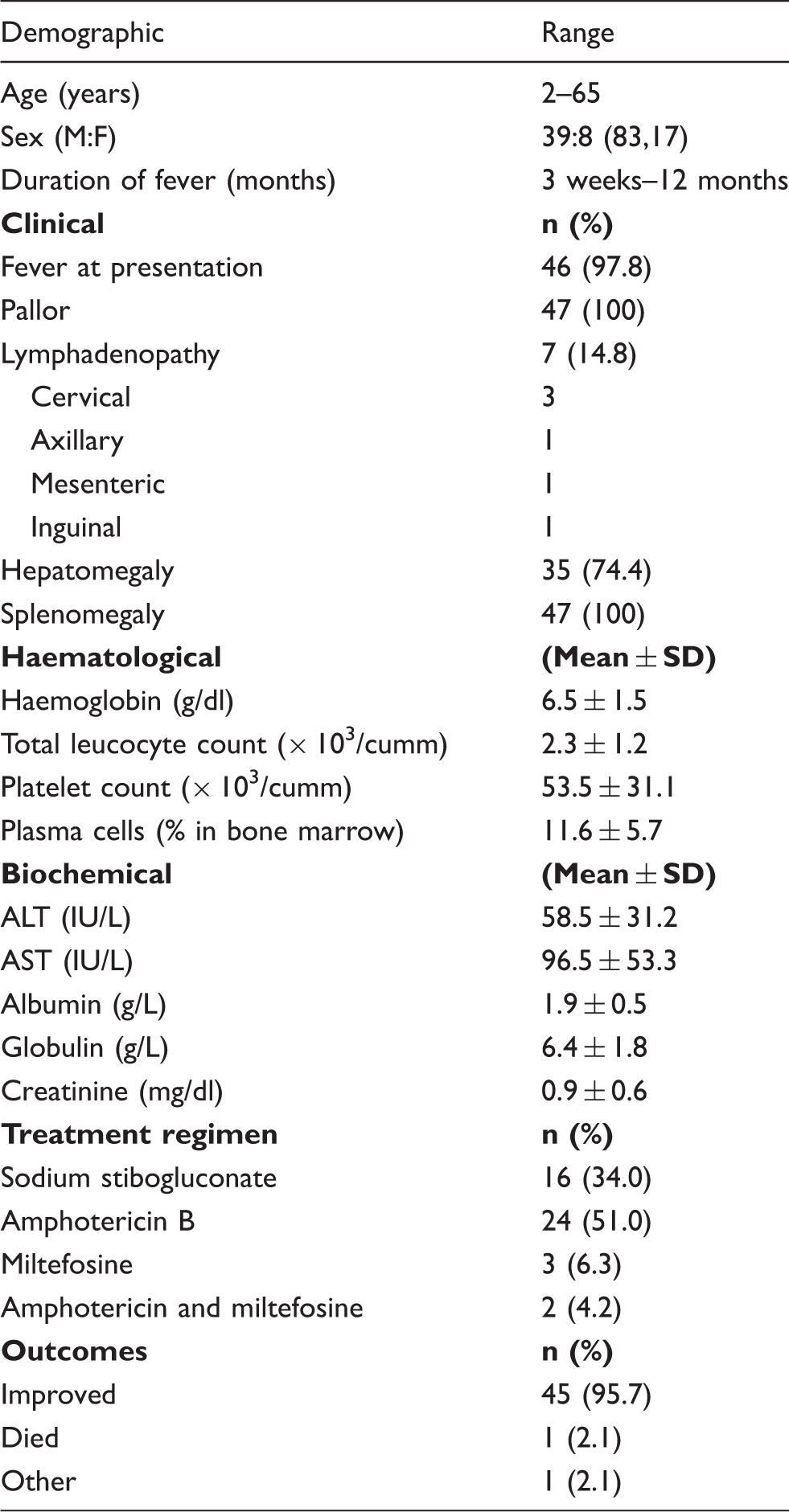
Between August 2004 and July 2014, 52 cases of VL were diagnosed and treated at this centre. Of these, 47 were from the Garhwal region of Uttarakhand and had never visited any of the endemic areas. All but one tested negative for HIV infection. All the patients were diagnosed on the basis of clinical features and demonstration of Leishmania donovani (LD) bodies in the bone marrow. Additionally, five (10.6%) had a positive serological test with rK39 immuno-chromatographic strip; splenic aspirate was utilised in two circumstances.
Profile of patients with VL (n = 47).
Discussion
The hilly Garhwal region of Uttarakhand can be considered as a hothouse of VL in India, encouraging transmission of the protozoan. The construction of the huge Tehri Dam initiated migration of labourers from the states of western Uttar Pradesh and Bihar which are endemic for VL. Subsequently improved road links, increased mobility and the ecological changes after the Tehri Dam became functional have apparently caused an environmental shift in favour of vector proliferation leading to an emergence and establishment of the disease in this region. Also, the animal reservoir in the region is still elusive and is a subject of future study.
The increased reliance on Amphotericin B and miltefosine for treatment over sodium stibogluconate in recent times has not been due to the emergence of resistance to the old drug. Low toxicity profile and shorter regime has shifted treatment in their favour; moreover, the dwindling demand of the antimony compounds has resulted in reduced availability of the drug as well. Nevertheless, 95% success rate of treatment suggests the continuing sensitivity of the protozoan to the drugs.
Conclusion
VL is being increasingly diagnosed in the residents of Garhwal region of the Himalayan state of Uttarakhand. The poor association with HIV infection and 95% sensitivity to the established drugs are the cardinal features of VL in Uttarakhand. The protozoan is de novo from Uttarakhand apparently as the patients had never ventured outside Garhwal. However, molecular mapping is needed to confirm the ancestry.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.