
Abstract
Cases of kala-azar reported during 2013–2018 in Bihar, India were retrospectively analysed. Of 2187 villages reporting cases of kala-azar in 2018, 573 (26.2%) had reported no case in the previous five years but contributed to 20% of disease burden in 2018. On applying potential thresholds of kala-azar outbreaks, 805, 519 and 103 villages reported more than twice, thrice and five times their previous five-year annual average in 2018, respectively. Indoor residual spraying (IRS) in villages reporting any case of kala-azar in the past three years as per current guidelines could cover 72% of incident cases in 2018 vis-a-vis 80% if villages reporting cases in the past five years were considered. Therefore, IRS may be expanded to villages reporting cases in the past five years. Village case trends can be utilised to configure potential outbreak alarms (early warning and response system) on a pre-organised dashboard. A data-driven strategy for villages newly reporting cases and those in potential outbreak situations could prove effective in achieving and sustaining the elimination of kala-azar.
Keywords
Introduction
The World Health Organization (WHO) defines a disease outbreak as the occurrence of cases in excess of normal expectancy. 1 Kala-azar has long been known to be an outbreak-prone disease since its first symptomatic documentation in Jessore district (now in Bangladesh) in 1824–1825.2,3 Before the advent of chemotherapy and dichlorodiphenyltrichloroethane (DDT) spray, kala-azar outbreaks were known to have a 90% case fatality rate, leading to a reduction of up to 25% of the population in some of the newly affected districts due to death and migration. 2 Poor nutrition and waning population immunity, which both predispose to enhanced conversion from the asymptomatic leishmania infection phase to symptomatic kala-azar disease, contribute to kala-azar outbreaks.4,5 Additionally, the Phlebotomus argentipes vector has a short flight range and the transmission efficiency of the vector is enhanced through biting persistence and multi-host feeding. 6 This contributes to the characteristic clustering of cases and outbreaks of kala-azar evolving focally and quickly within a few months. 7
In 2005, the kala-azar elimination programme received momentum as the governments of Bangladesh, India and Nepal signed a memorandum of understanding (MoU) to eliminate this disease as a public health problem by 2015. 8 Further, in 2014, a five-sided MoU was signed between these three countries with Bhutan and Thailand for a revised 2017 target for elimination. 9 India has seen an impressive 10-fold reduction of the annual kala-azar burden in the past 10 years. Currently, the WHO target of this year for the elimination of kala-azar as a public health problem from the Indian sub-continent (Bangladesh, India and Nepal) is being pursued. 10
Sustained achievement of <1 case per 10,000 at the sub-district level has been adopted as the elimination threshold for India. 10 The immediate sub-district level in India is the sub-division or anumandal level. A typical district of 600,000–6,000,000 people in an endemic area comprises 3–5 sub-divisions. 11 However, within the Indian context of kala-azar elimination, community development blocks or prakhand are considered to be at the sub-district level. This is because health data are aggregated and health programmes are being managed at the block level. As of 2019, only 6% of the 633 endemic blocks in India remained above this threshold.
This elimination threshold is widely known in the endemic area and acts, as a rule of thumb as to which blocks are prioritised for monitoring. The Accelerated Plan for Kala-azar Elimination was launched in 2017 in which the block-level strategy was further fine-tuned – for highly endemic blocks with an annual incidence > 1 per 10,000 population, borderline blocks with an incidence in the range of 0.8–1 per 10,000 and for those with fluctuating kala-azar incidence. 11 Early diagnosis and treatment and integrated vector management are the two main strategies outlined under the kala-azar elimination programme. 12 Indoor residual spraying (IRS) is the main vector control intervention currently being adopted.
The need for a village-level strategy as opposed to an extensive block-level strategy has long been felt by experts, especially with regard to vector control interventions.3,13 This found resonance with the National Kala-azar Roadmap 2014, which mandated that IRS be conducted twice a year in those villages that had reported a kala-azar case in the past three years.14,15 Subsequently, a concept was evolved of ‘hotspot’ or ‘high-risk’ villages which usually report five or more cases in a year. 12 A list of 139 such villages in India were thus suggested for prioritisation. 12
The state of Bihar accounts for nearly 75% of the burden of kala-azar. In the endemic area, there are 33 districts with 458 blocks, 11 each of which are supposed to have approximately 100,000 people. However, 121 blocks actually have a population of >300,000 and 17 blocks have a population of >500,000. 11 Thus, even if there is an outbreak of 49 kala-azar cases in one year in a village in such a highly populated block of 500,000 people, it would remain below the elimination threshold if no other village in the block reports a case of kala-azar. With kala-azar, there is a high level of spatial and temporal clustering and its distribution varies widely even within hamlets of the same village. This provides justification for further exploring a village level strategy.
The aim of the present study was to describe the village-level endemic situation especially with regard to potential outbreaks and the emergence of cases of kala-azar in villages that reported no case in previous years. I also wished to explore the application of village-level endemicity to criteria for IRS activity.
Methods
The Kala-azar Management Information System (KAMIS platform, https://www.ka-mis.org/) was launched in 2015–2016 with the support of Care India. It enables entry of individual patient-level data at the primary healthcare level. It also allows aggregation of data and visualisation of the dashboard by the district vector-borne disease control officer (DVBDCO). Reliable data are available on this platform going back to January 2013 on account of retrospective data entry after its launch. Since patient information is mandated to be entered within three days of registration, the KAMIS platform also provides a near real-time trend of cases of kala-azar.
A retrospective data analysis was made of the cases of kala-azar reported in Bihar. The line list of patients with kala-azar in Bihar registered between 1 January 2013 and 31 December 2018 was downloaded from the KAMIS platform in April 2019. The data were anonymised to prevent identification of individual patients. Data cleaning was done to remove entries where ‘village name’ was blank. Subsequently, a pivot table was generated using the fields of district, block and village in hierarchical order and year of registration in the column field. Then, local village-wise criteria for a plausible outbreak were generated based on the annual average of kala-azar cases in 2013–2017.
Outbreak thresholds based on past five-year data have already been used for malaria. Similarly, past five-year kala-azar data of the particular village were used to evolve the criteria for outbreak alerts in any current year. Two criteria were applied sequentially to reflect the unexpectedness of the number of cases of kala-azar reported in the village and those villages reporting ≥ 5 cases among these. For the first criteria of unexpectedness, three thresholds for possible outbreaks of kala-azar in 2018 were identified at village level: those reporting more than twice, thrice and five times the annual average of cases (reported for the five-year period of 2013–2017). Among these, villages reporting ≥ 5 cases in 2018 were further identified. These have been classically taken as ‘hotspot’ or ‘high-risk’ villages in the programme. Villages reporting no cases during 2013–2017 and subsequently reporting ≥ 1 case in 2018 were taken as ‘new villages’. Contribution of these villages to the total number of cases in 2018 was calculated district-wise. Conversely, contribution of the previous three-year endemic and five-year endemic villages was also calculated for the total number of cases of kala-azar reported in the districts in the year 2018.The cases of kala-azar reported in 2018 were evaluated based on whether they would be covered in their vicinity according to currently applicable criteria for conducting IRS in those villages reporting at least one case of kala-azar in the years 2015–2017. This was compared with the coverage if the expanded IRS criteria of the past five years was used, i.e. covering the villages which reported at least one case of kala-azar in 2013–2017.
All analyses were done for both the district level and aggregately for Bihar state. Microsoft Excel software 2019 was used to perform the analyses.
Results
Data were available for 34,598 cases of kala-azar from 9972 villages in Bihar state, India from 1 January 2013 to 31 December 2018. Among these, 9399 villages had reported at least one case of kala-azar during the five-year period from 1 January 2013 to 31 December 2017. The total number of cases of kala-azar reported during this five-year period was 30,973. A total of 35,042 villages constitute the endemic area of 33 districts in Bihar. 11 Thus, in the endemic area, 26.8% villages had reported cases in the preceding five-year period of 2013–2017.
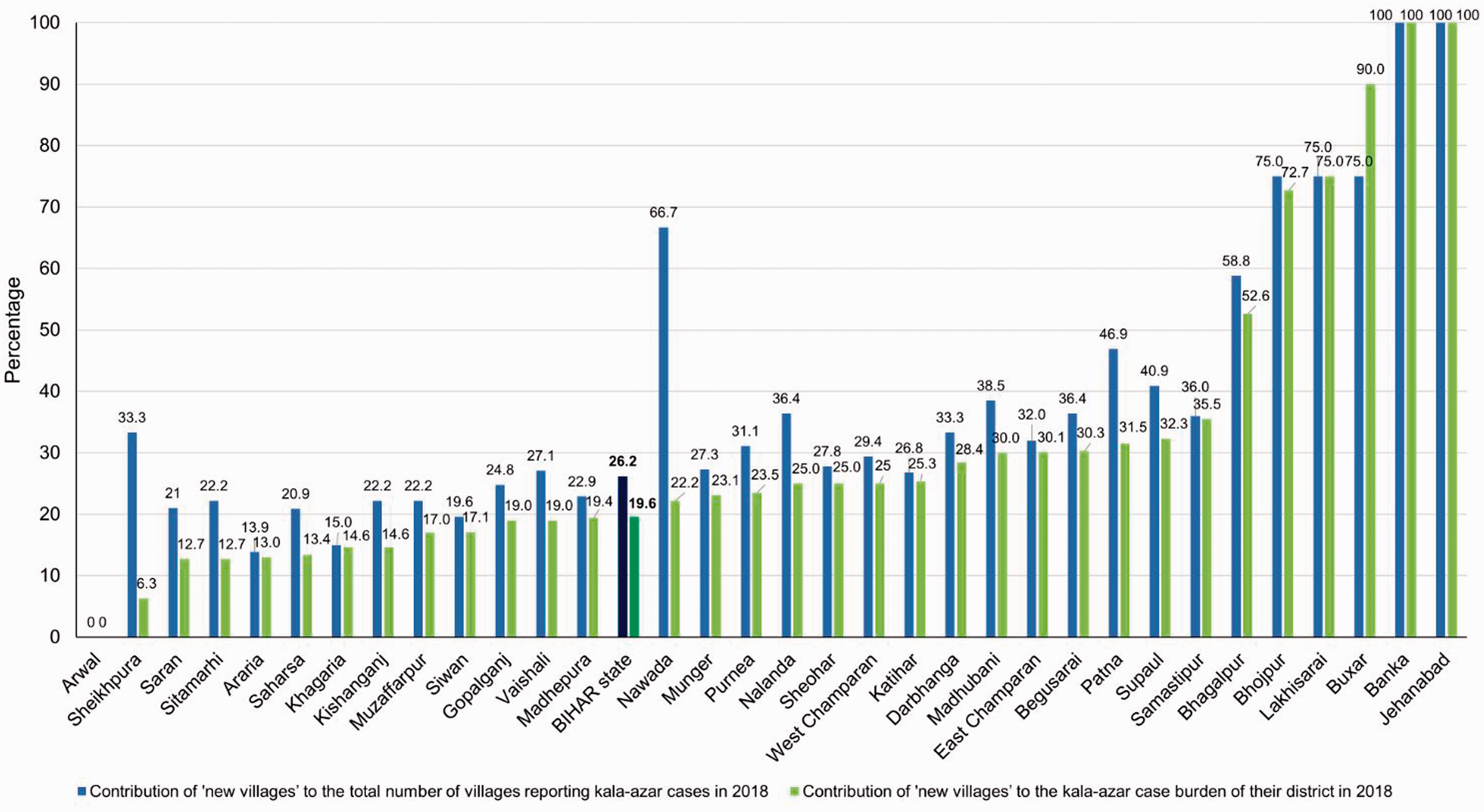
The 3625 cases reported in 2018 in Bihar were contributed by 2187 villages (Figure 1). Of these villages, 573 (26.2%) were ‘new villages’, which had not reported any cases of kala-azar in the years 2013–2017 (Figure 1). Conversely, around three-quarters (n = 1614) of the villages reporting cases in 2018 had already reported at least one case during 2013–2017. Contribution of the ‘new villages’ to the number of cases of kala-azar reported in 2018 in Bihar was 19.6% (Figure 2). The contribution of ‘new villages’ to the number of cases of kala-azar reported in their respective districts is shown in Figure 2.
Hierarchical relationship between villages identified with potential kala-azar outbreak situation in 2018 in Bihar, India. Each arrow points to a subset of the number of villages mentioned in the preceding box. District-wise contribution of ‘new villages’ (reporting cases in 2018 but not during 2013–2017) to the total number of villages reporting cases of kala-azar in 2018 and their contribution to kala-azar case burden in 2018.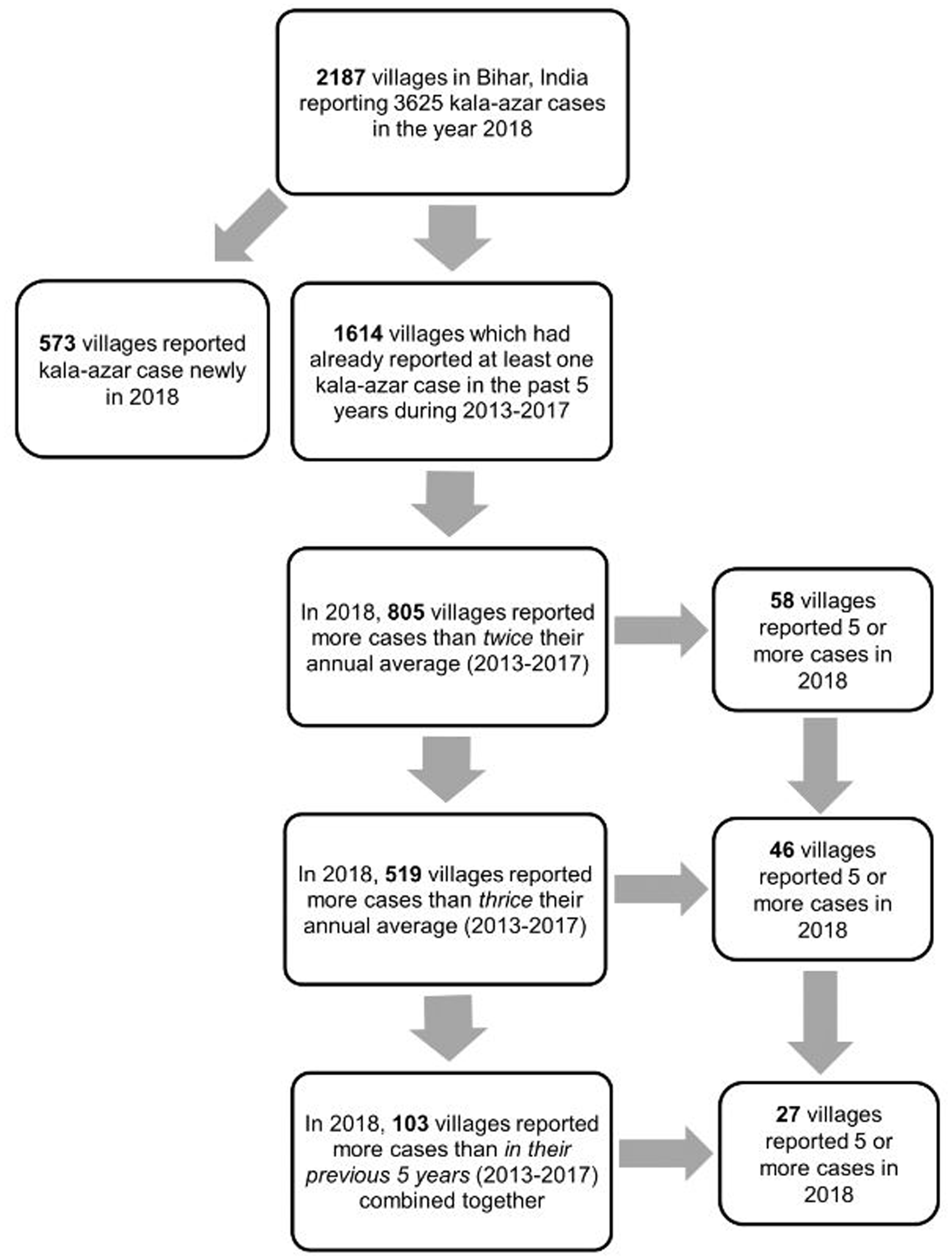
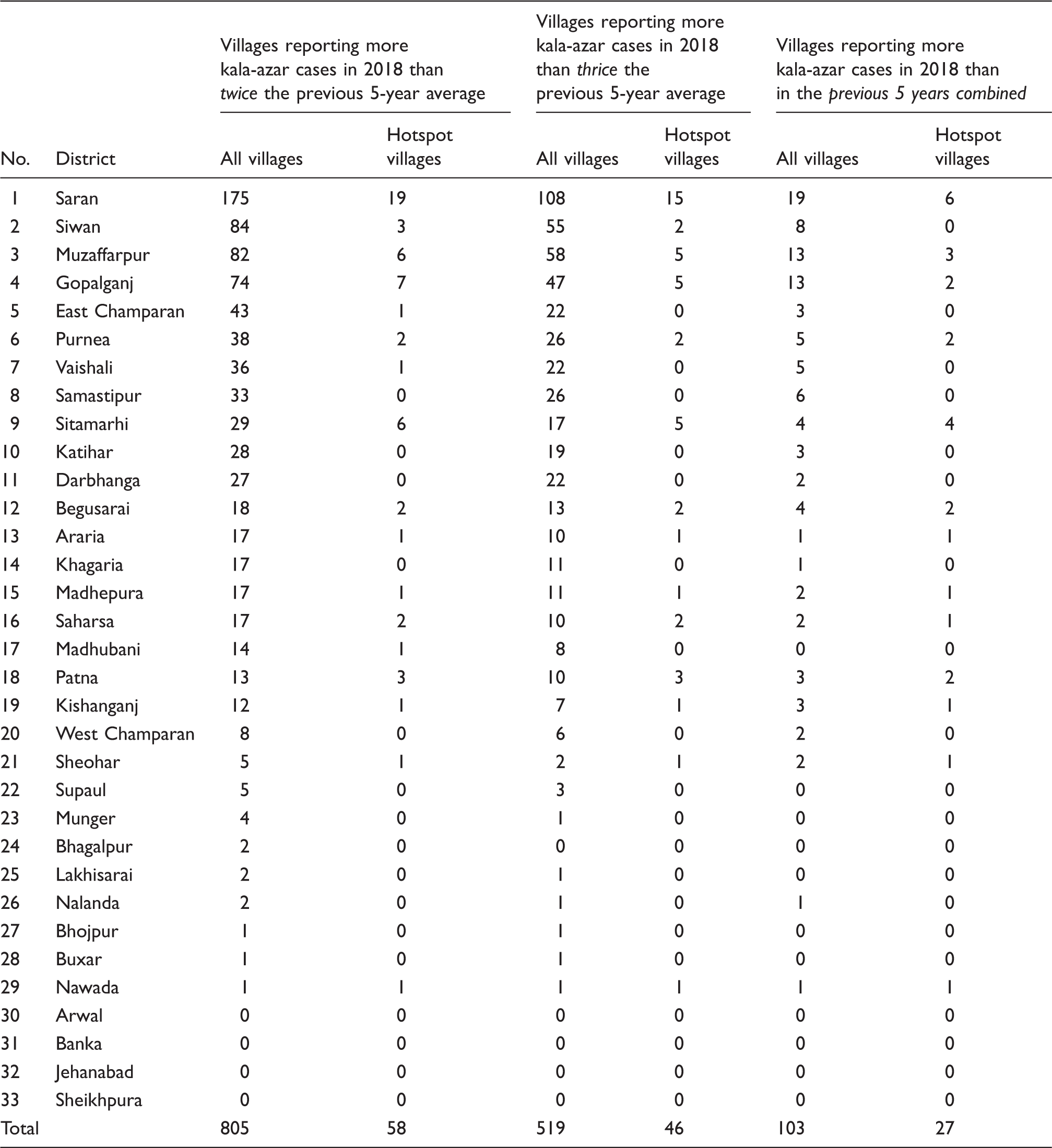
Villages in Bihar with potential kala-azar outbreaks in 2018 based on more than twice, thrice or five times their annual average of the previous five years (2013–2017) for the village and hotspot villages (≥5 cases reported in a year) among them.
The criteria of conducting regular IRS in villages reporting at least one case of kala-azar in the past three years could cover the vicinity of 72.4% incident kala-azar cases in 2018 (Figure 3). In the proposed expanded criteria of taking villages reporting at least one case of kala-azar in the past five years, 80.4% of kala-azar cases emerging in 2018 could be sprayed in their vicinity (Figure 3). In the expanded criteria, 26/33 districts could have coverage of around two-thirds or more incident kala-azar cases reported in 2018 compared to only 19/33 for the existing criteria (Figure 3).
Comparison of indoor residual spraying coverage of incident kala-azar cases in 2018 by utilising the current selection criterion of villages which reported at least one case in the previous three years vs. the proposed expanded criterion of taking villages which reported at least one case in the previous five years.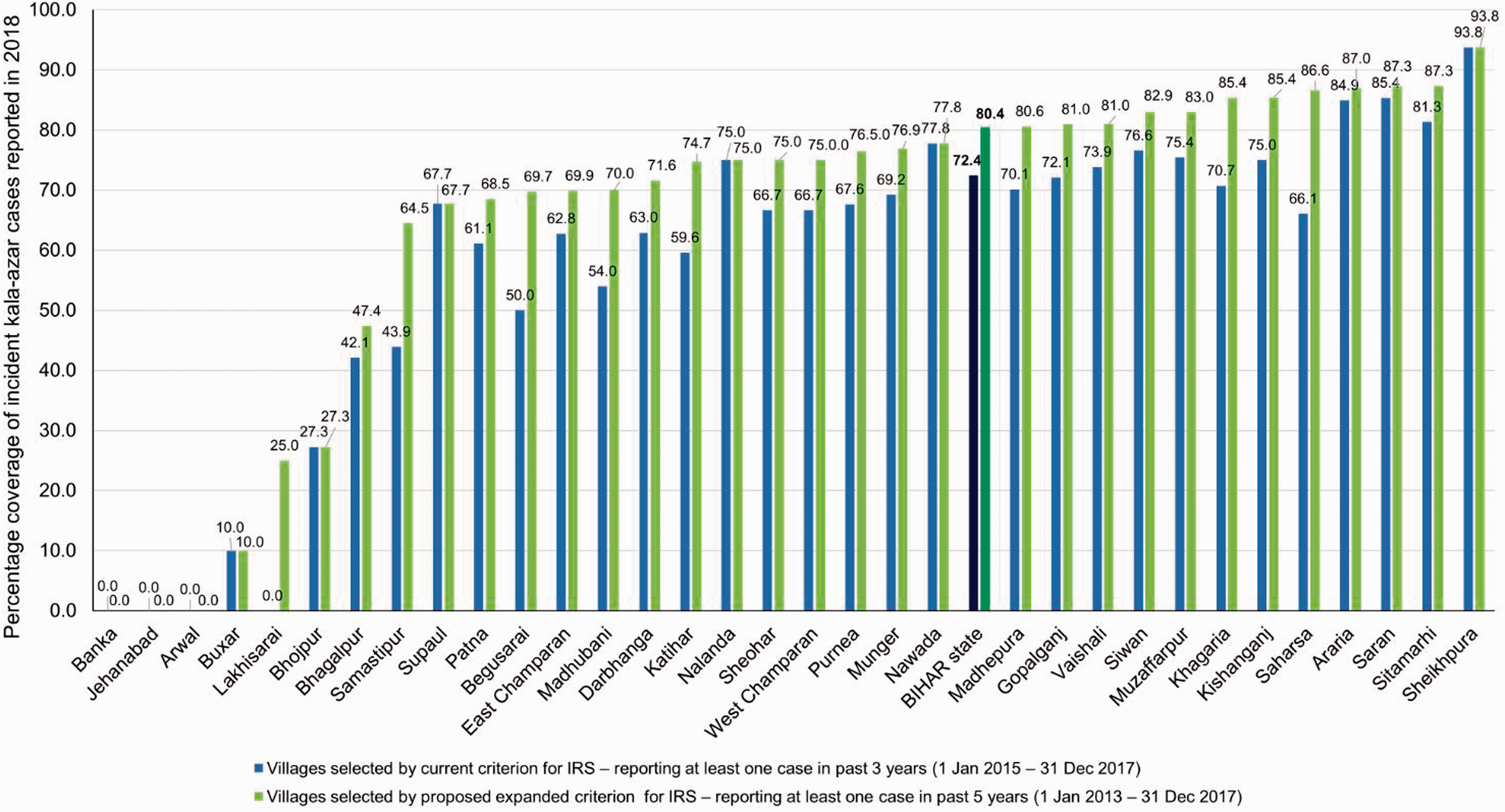
Discussion
The implications of the analysis of ‘new villages’ are manifold. Owing to the paucity of long-term data of 10–20 years in the KAMIS system, the emergence of cases in the ‘new’ villages could not be strictly classified as newly occurring transmission in the village. However, the villages newly reporting cases in 2018 would indicate a relatively recent focus of kala-azar transmission within the endemic area. These villages could be prioritised for aggressive strengthening of surveillance and case finding activities so that spread of kala-azar beyond the established endemic villages could be contained. The already existing dashboard of the KAMIS portal could be configured so that the emergence of such villages could trigger an alert.
The finding that > 80% of cases were being reported by those villages that had reported cases in 2013–2017 has considerable programmatic implications. Blanket IRS of all villages in high-endemic blocks was adopted in the 59 high-endemic blocks in the first regular spraying round of 2019 in Bihar, as an exception to the three-year-endemic village criteria (Supplemental file 1). Overall, in the endemic area, only one-quarter of all villages had reported cases during the reference period of 2013–2017. Even in the high-endemic blocks, this proportion might be expected maximally to approach 50%. Thus, blanket IRS strategy might be costly and inefficient in targeting infected sandflies, as the majority of villages targeted as such would not have reported cases within the past five years. 16 Additionally, < 20% of all cases are expected to be contributed by the ‘new villages’. A village-level study done in the 1990s had similarly concluded blanket spraying to be unnecessary and not cost-effective. 13 Furthermore, as seen in agricultural settings, blanket spraying could promote development of insecticide resistance among the insect vectors. 17 Thus, in the future, focusing on the existing endemic village-specific strategy would be preferable to a blanket approach of covering all villages in highly endemic blocks.
However, broadening vector control activities from villages to those reporting at least one case in past 3–5 years should be attempted. This would ensure that vector control activities are adopted in the vicinity of > 80% of incident cases. At the Bihar state level, focal spraying is required within 50 m or 250 houses surrounding each incident kala-azar case. However, this is not implemented regularly as manpower and insecticide are not separately allocated for focal spraying but may be provided from residual savings after conducting the two regular annual rounds of IRS. With the ongoing annual reduction in cases, the expanded criteria may therefore not overburden the programme. Focal spraying can also be done sparingly for only those selected villages newly reporting cases in 2018 and which would not have been covered through the regular IRS using the expanded criteria.
Furthermore, individual patient and village-level aggregate data are available through the KAMIS platform on a concurrent basis. The electronic database is now mature enough to provide village-wise kala-azar case trend for the past seven years. This provides an opportunity for developing a fine-tuned village-level strategy for elimination, including that of detection and response to outbreaks. It is suggested that, to start with, twice the previous five-year average criterion be used to trigger a preliminary alert for outbreak detection during the current year. This is so that early control measures such as active case search and quality vector control measures could be adopted for the village. Further prioritisation of villages reporting three or more and five or more cases may be taken among these, if resources are limited and in case of large outbreaks.
This study demonstrates that, with the advancement of information systems in kala-azar, the use of local criteria suited to the endemicity of each particular village is feasible for taking key decisions in the elimination programme. Such use of real-time data for triggering outbreak alerts has been demonstrated through use of early warning and response systems (EWARS) in other infectious diseases such as dengue and polio.18,19 Minimal additional resources will be required for this purpose since the existing KAMIS dashboard could be improvised for the purpose. Also, future research could focus on the development of predictive tools based on the already available trend of kala-azar cases to predict which villages could prospectively evolve into large outbreaks.
Conclusion
It is expected that the response to kala-azar outbreaks shall be of increasing importance in the maintenance phase of elimination as there is a higher risk of outbreaks in previously endemic and low-endemic areas. 20 An explosive kala-azar outbreak of 74 cases in Kosra village situated in a low-endemic area, provides an appropriate example. 7 A village-level strategy for the prompt identification and outbreak response is not only likely to help reduce the kala-azar burden but would also help sustain the reduction of cases in the maintenance phase of any kala-azar elimination programme.
Supplemental Material
sj-pdf-1-tdo-10.1177_0049475520953647 - Supplemental material for Time for a village-level strategy for the elimination of kala-azar (visceral leishmaniasis) in India: analysis of potential kala-azar outbreak situation in 2018
Supplemental material, sj-pdf-1-tdo-10.1177_0049475520953647 for Time for a village-level strategy for the elimination of kala-azar (visceral leishmaniasis) in India: analysis of potential kala-azar outbreak situation in 2018 by Suman Saurabh in Tropical Doctor
Footnotes
Acknowledgements
The author acknowledges the Kala-azar Management Information System (KAMIS) platform for providing the data of kala-azar patients during 2013–2018. Data are owned by the Directorate of National Vector Borne Diseases Control Programme, Ministry of Health and Family Welfare, New Delhi. They are thanked for providing the stakeholders with access to the database as per need basis. The author also acknowledges support while being employed as Zonal Coordinator – Neglected Tropical Diseases with the World Health Organization – India office.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.