
Abstract
Diphtheria is a potentially fatal infection owing to its life-threatening complications of respiratory obstruction and myocarditis. Less often reported is diphtheritic polyneuropathy (DP), which refers to signs and symptoms of various cranial nerve involvement and/or limb neuropathy within six weeks of a compatible clinical illness suggestive of diphtheria. We report four cases of DP occurring in a limited outbreak of 19 cases and review the literature. The most common cranial nerves affected were VII, IX and X. Importantly, all four cases had received their infant vaccinations. Diphtheria antitoxin and prednisolone were the mainstay of management in addition to physiotherapy support. All were discharged home and have made a good recovery. We conclude that DP is not so uncommon and its occurrence among children who had been vaccinated requires a review of the vaccination programme and schedules.
Introduction
Diphtheria is a life-threatening toxin-mediated infection caused by Corynebacterium diphtheriae.1,2 While the respiratory form is the most common, it often results in systemic complications such as myocarditis and neurologic manifestations owing to the spread of the exotoxin produced by the organism.2,3 Diphtheritic polyneuropathy (DP) is a rare but severe neurological complication that occurs particularly in individuals who are not immunised or inadequately immunised.4–6 Diphtheria used to be a leading cause of childhood mortality before the widespread implementation of vaccination programmes.1,2,7 Although the incidence of diphtheria has drastically declined in many parts of the world owing to successful immunisation programmes, 8 it remains endemic in certain regions where vaccination coverage is suboptimal.7,9 Consequently, cases of DP can still be seen in these areas.10,11 This is defined as cranial nerve involvement and/or limb neuropathy within six weeks of compatible clinical illness suggestive of diphtheria.6,12,13 The incidence of DP is directly proportional to the severity of intoxication.6,14 DP results from the spread of the diphtheria toxin via the bloodstream, leading to demyelination and axonal degeneration of peripheral nerves. The toxin invades Schwann cells and exerts its damage by inhibiting protein synthesis within neurons. This inhibition leads to a cascade of cellular events, resulting in both demyelination and axonal damage, hallmarks of the condition. The transport down the axon of newly synthesised protein with eventual destruction of the myelin sheath accounts for the delay in neuropathic symptoms after initial infection. DP is generally considered a demyelinating neuropathy with proximal to distal spread of weakness and prominent sensory features.5,12–16
DP typically presents weeks after the onset of the primary infection. This latency ranges from ten days to three months.11,16,17 DP is usually multiphasic in onset with paralysis of the soft palate and posterior pharyngeal wall being the first signs. Bulbar dysfunction develops during the first two weeks.15,18 The peripheral neuropathy often presents as a progressive paralysis spreading from proximal to distal muscle groups, with associated sensory disturbances. Because of its clinical features, especially cranial nerve involvement, limb weakness and autonomic dysfunction, it can easily be misdiagnosed as Guillain-Barré syndrome. 19 Given the relative rarity of the condition and its potential severity, early recognition and appropriate management are critical.2,6 DP is a potentially reversible condition, and surviving patients often report few or no residual neurologic symptoms. Motor symptoms improve within two to four months.13,17
DP, though traditionally considered rare, may actually be more prevalent than previously thought.
Case reports
During an outbreak of diphtheria that occurred between May and September 2024 in Edo state, Nigeria, 4/19 cases of suspected diphtheria were diagnosed with DP. Diagnosis of diphtheria was made based on clinically compatible symptoms and confirmed bacteriologically in some of the patients. Data obtained from the case notes of each child with DP included symptomatology and duration of symptoms, immunisation history, treatment and treatment outcomes, including presence/absence of other complications. Data were de-identified and stored in a password-protected computer accessible only to the first author. As this was a chart review, ethical clearance and waiver of consent were sought from the University of Benin Teaching Hospital Research and Ethics Committee.
At the onset of clinical symptoms of DP, each child received a complete neurological examination and at every follow-up visit. There were three girls and one boy aged between 4 and 11 years. They all lived in urban areas. Latency varied from 10 to 44 days (mean, 30 ± 8) with the first symptoms appearing between the 4th and 6th week for three patients and within the first two weeks in one patient.
The first symptoms were numbness in the soft palate in two patients, and dysphonia with dysphagia in three. All had pareses of motor cranial nerves. One presented with muscular hypotonia and quadriparesis. Two presented with reduced or absent tendon reflexes, and three with gait abnormalities. There was no peripheral sensory disturbance in all but one had disdiadokokinesis. All four had received diphtheria immunisation in early childhood.
Disturbance of cranial nerves VII, IX and X were the most frequently observed cranial neuropathy (Table 1). Motor dysfunction of V was seen in one, and palsy of XII was observed in two. The latter was accompanied by drooling and regurgitation of liquid food through the nose, with aspiration into the trachea triggering coughing episodes.
Clinical features, treatment and outcome of four cases of diphtheritic polyneuropathy.
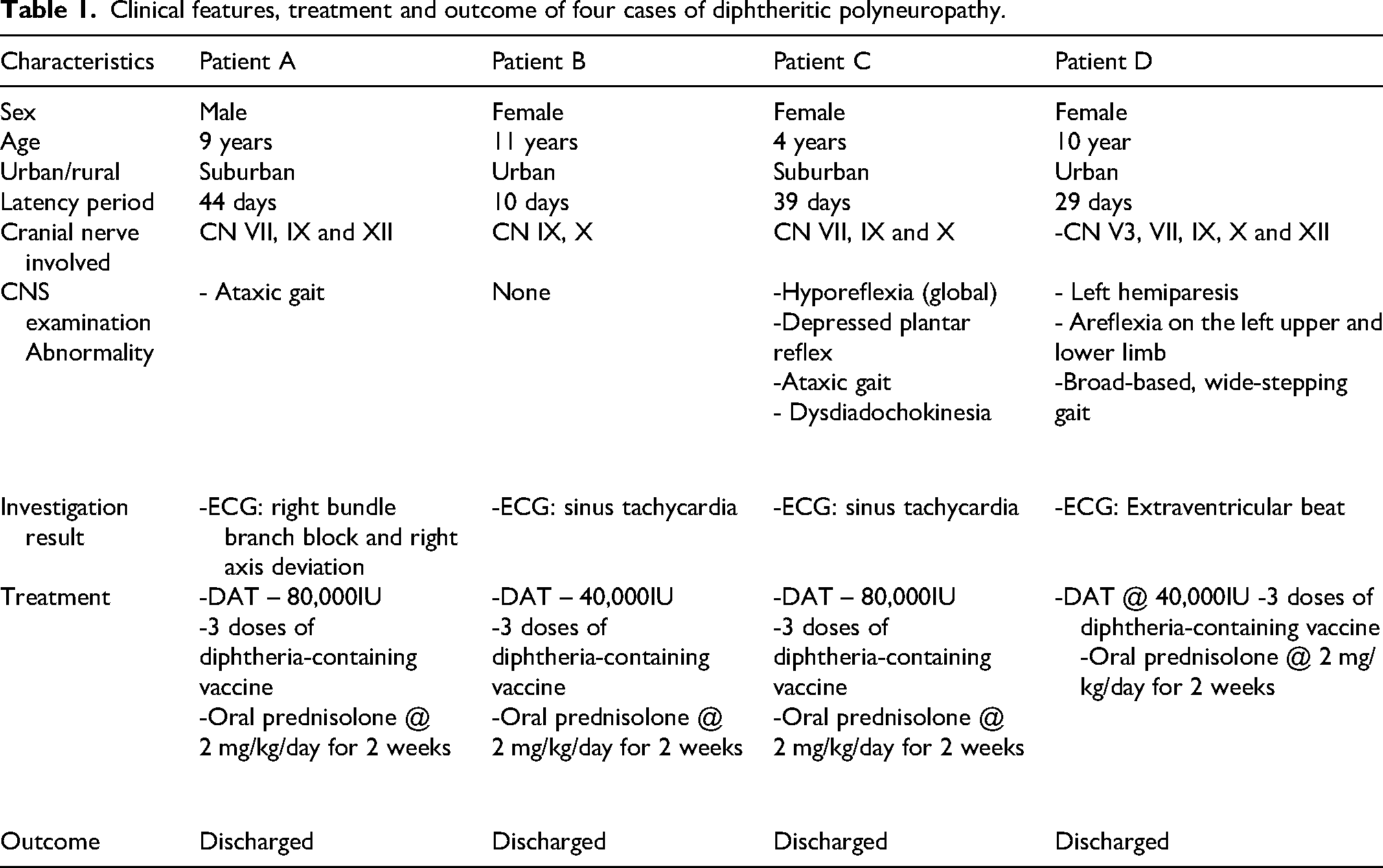
Motor disturbances in the extremities were observed in four. Proximal quadriparesis was observed in one, while the other three had a variable degree of motor weakness affecting the upper and lower limbs. One had muscular hypotonia and tendinous areflexia, while another had hyporeflexia. Superficial reflexes were depressed in one, while three had gait abnormalities.
None, however, was noted to have sensory abnormalities. Joint position sense, tactile discrimination and vibration sense were intact at the time of review.
Subtle incidental ECG abnormalities were noted in three, while one had right bundle branch block and right axis deviation. Two had sinus tachycardia, and one had extra-ventricular beats. We were unable to test for nerve conduction velocity.
All patients received amoxicillin and metronidazole, and two received 40,000 IU of diphtheria antitoxin (DAT), while the other two received 80,000IU. All received three doses of diphtheria-containing vaccines following discharge and hydrogen peroxide gargle. All four received prednisolone at a dose of 2 mg/kg for two weeks.
All four made full neurological recovery at their last evaluation, which was at six months post-diphtherial illness for three, and at nine months for the remaining patient.
Discussion
DP remains a significant concern in our location. 20 A significant variability in clinical presentation necessitates careful evaluation and tailored management. DP is dependent on the severity of intoxication. 13 Severe presentation was seen despite previous vaccination, even requiring tracheostomy, while also presenting with myocardial dysfunction.10,20 It is possible that immunity may wane over time or that seroconversion did not occur at the time of their primary immunisation.5,20,21 This finding emphasises the need for booster doses at school entry or adolescence to sustain immunity, especially during outbreaks, but also to prevent such outbreaks, and the development of DP.20,22
Initial symptoms of DP are bulbar palsy and cranial nerve deficits. 15 Elevated cerebrospinal fluid protein without pleocytosis, and specific electrophysiological patterns, may aid in differentiating DP from other neuropathic conditions.5,6,16 Electrophysiological studies in cases of DP typically reveal a mixed pattern of demyelination and axonal degeneration, reflecting the widespread neural damage caused by the toxin.5,13,15
The timely administration of DAT is an essential component in the management. DAT acts on unbound toxin and may not be effective if the toxin is already bound to tissues. However, one child received DAT after myocarditis had set in, but before the onset of symptoms of DP, which appeared to limit its progression. Thus, we believe that DAT still plays a useful role in the management of the DP. 23
Elimination of Corynebacterium diphtheriae is achieved with erythromycin and penicillin.22,23 Supportive care, particularly physiotherapy, plays a critical role in managing muscle weakness, improving mobility and reducing the risk of long-term disability.4,15,17 Nonetheless, significant morbidity may persist, as the recovery process is often prolonged and may require extended rehabilitation efforts.4,13,18
Footnotes
Ethical approval
Ethical approval for this study was obtained from the University of Benin Teaching Hospital Health Research Ethics Committee with protocol number ADM/E22/A/VOL.VII/4831141824 on 28 May 2025.
Author contributions
AES conceptualised the study, recruited the patients, designed the proforma for data abstraction, reviewed the Sdata, the initial draft and approved the final draft. PEI contributed to the concept, conducted the neurologic examination of the patients, contributed to the design of the proforma, reviewed the data, wrote the initial draft and approved the final draft. SA contributed to the concept, abstracted the data from the case notes, reviewed the data and approved the final draft. OO contributed to the concept, abstracted the data from the case notes, reviewed the data and approved the final draft.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.