
Abstract
In resource-limited settings such as rural Nepal, the lack of intra-operative fluoroscopy often forces clinicians to choose between suboptimal conservative management or referral to distant centres. Our case series presents the feasibility of the titanium elastic nailing system for displaced childhood both-bone forearm fractures using tactile feedback and portable radiography instead of a C-arm. While the rate of open reduction was higher than in a fluoroscopy-guided series (2/9 for radius, 4/9 for ulna), all cases achieved stable intramedullary placement and clinical union. This approach offers a viable alternative for maintaining surgical standards in so-called ‘blind’ settings.
Keywords
Introduction
Forearm fracture is the most common fracture in the paediatric age group. 1 Stable and minimally displaced forearm fracture can be properly managed with closed reduction and cast application. 2 However, surgical management is indicated in displaced unstable fractures and in fractures which cannot be reduced by closed manipulation to an acceptable degree, and in children older than 12 years. The most common complication of conservative management is malunion which can lead to significant loss of function, particularly pronation and supination. 1
Among children with diaphyseal forearm fractures which require surgical management, intramedullary fixation is considered the gold standard. This has the benefits of shorter operative time, improved cosmesis, easy follow-up management and easier hardware removal. Osteosynthesis with an elastic stable nailing system is considered an excellent method for intramedullary fixation. It provides stability by the principle of three-point fixation. While delayed union, non-union, re-fracture, infection, skin irritation, implant migration or failure, nerve and tendon injury and compartment syndrome are reported complications, 3 these are relatively uncommon.
The use of fluoroscopy during fracture reduction allows easy, accurate reduction and helps correct insertion of titanium elastic nailing system (TENS). 4 In many rural healthcare centres in Nepal however, fluoroscopy is unavailable, and patients can often not afford the travel or cost of referral to a tertiary centre. Our experience is to use a ‘tactile-guided’ technique and portable radiography.
Case series
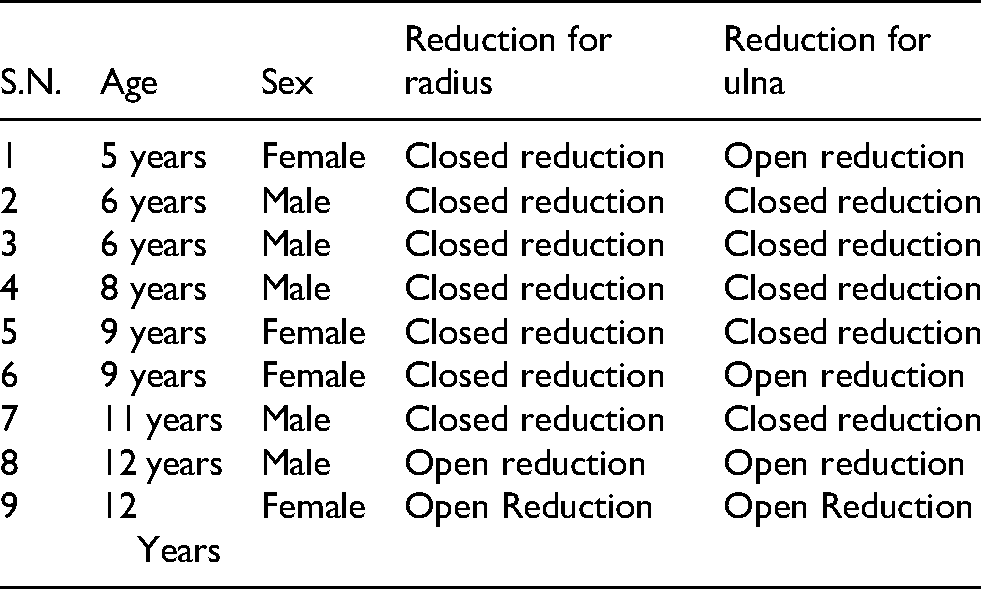
We identified nine cases of both-bone forearm fracture in children requiring surgical management, five boys and four girls, with a mean age of 8.6 years. Surgical management of all the cases was performed without intra-operative fluoroscopy guidance.
Operative technique
Pre-operative preparation required radiographs of the afflicted forearm in both antero-posterior and lateral views, measured for angulation, rotation and displacement. The narrowest diameter of intramedullary canal was measured. A nail size of 60%–70% central bony canal diameter was selected pre-operatively. Skin marking for the proposed entry site of the nail and fracture sites was made pre-operatively. Skin marks were also made 2 cm proximal to the distal radial physis and 2 cm distal to the olecranon physis (Figure 1).
Patients were kept supine with a tourniquet in place but not inflated except when required by open reduction intra-operatively. The radius was fixed first, as its manipulation is easier. The ulna then usually reduces spontaneously. If it does not, manipulation is usually difficult and often requires open reduction. This requires less soft tissue dissection than for the radius.
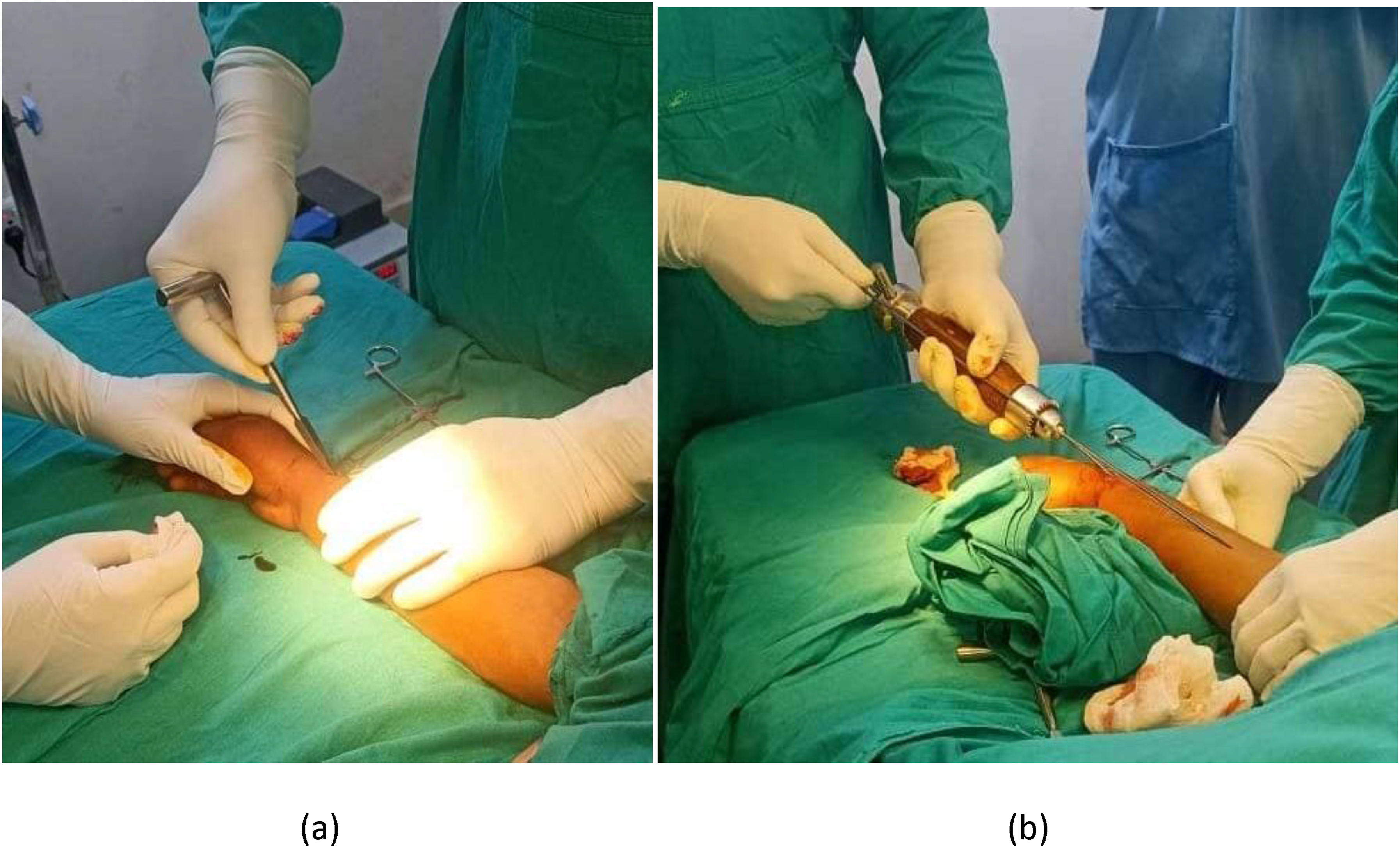
A skin incision of 1 cm is made distal to the radial skin marking, palpating the centre of the bone laterally. Blunt dissection to bone is made to preserve the superficial radial nerve and cephalic vein. An awl is placed directly onto the bone, and its near cortex is perforated. The awl is initially held perpendicularly, and gradually the angle is decreased to 45⁰ (Figure 2a). Pre-contouring of nail is not done. An appropriately sized nail is inserted with the help of a T-handle into medullary canal, advancing it by an oscillating movement. If the nail has been passed superficially, no resistance would be experienced, and it would be palpable subcutaneously. If the nail crosses the second cortex into interosseous space, there is a sudden give after initial resistance.
The nail is advanced until the fracture site is reached; this is determined by using another nail of the same length placed over the skin (Figure 2b). Once it is confirmed that the nail tip is at the fracture site, reduction is performed according to angulation or displacement by traction. The passage of the nail into the intramedullary canal or into soft tissue can be detected by the resistance felt. No more than two closed attempts are attempted. If it proves impossible to pass the nail by the closed method, an open reduction is performed, and the nail is passed under direct vision. It is then passed to the radial tubercle again estimating its position by using another nail of the same length over the skin. Finally, confirmation of intramedullary placement of TENS is confirmed by portable radiography.
In a similar way, a nail is passed in the ulna from proximal to distal starting 2 cm distal to the physis which was marked pre-operatively under X-ray guidance.
Among nine cases in our series, two radius and four ulna fractures required open reduction.
All cases were kept in an above-elbow slab post-procedure for 3 weeks. After plaster removal, gentle motion exercises were started.
Discussion
Fracture reduction and intramedullary insertion of TENS under fluoroscopy guidance has the potential advantage of accurate reduction as it provides a real-time image and takes less time with a decreased need for open reduction and soft tissue dissection.
However, intra-operative fluoroscopy is rarely available in low-resource settings. Intramedullary fixation is considered the gold standard for childhood both-bone shaft fracture management. 5 We demonstrate that TENS fixation is surgically possible without fluoroscopy. Its major disadvantage is increased operative time and increased need for open reduction. This risks nerve and vessels injury, reduced periosteal blood supply, delayed fracture union and cosmetic problems. Furthermore, in the absence of fluoroscopy, intramedullary nail placement may be difficult. However, these hurdles can be overcome with a little experience from tactile feedback.
The advantages, however, in rural settings are significant. It is thus possible to avoid the ‘referral gap’ where patients are often lost due to prohibitive travel costs and other expenses. Furthermore, the ‘blind’ technique eliminates radiation exposure for the surgical team, a notable benefit in operating theatres lacking proper lead shielding.
Preoperative marking for entry site made for TENS nail under radiography. Using an awl to create an entry point at the distal radius. (b) Using a nail of identical length over the skin surface to estimate the advancing intramedullary length.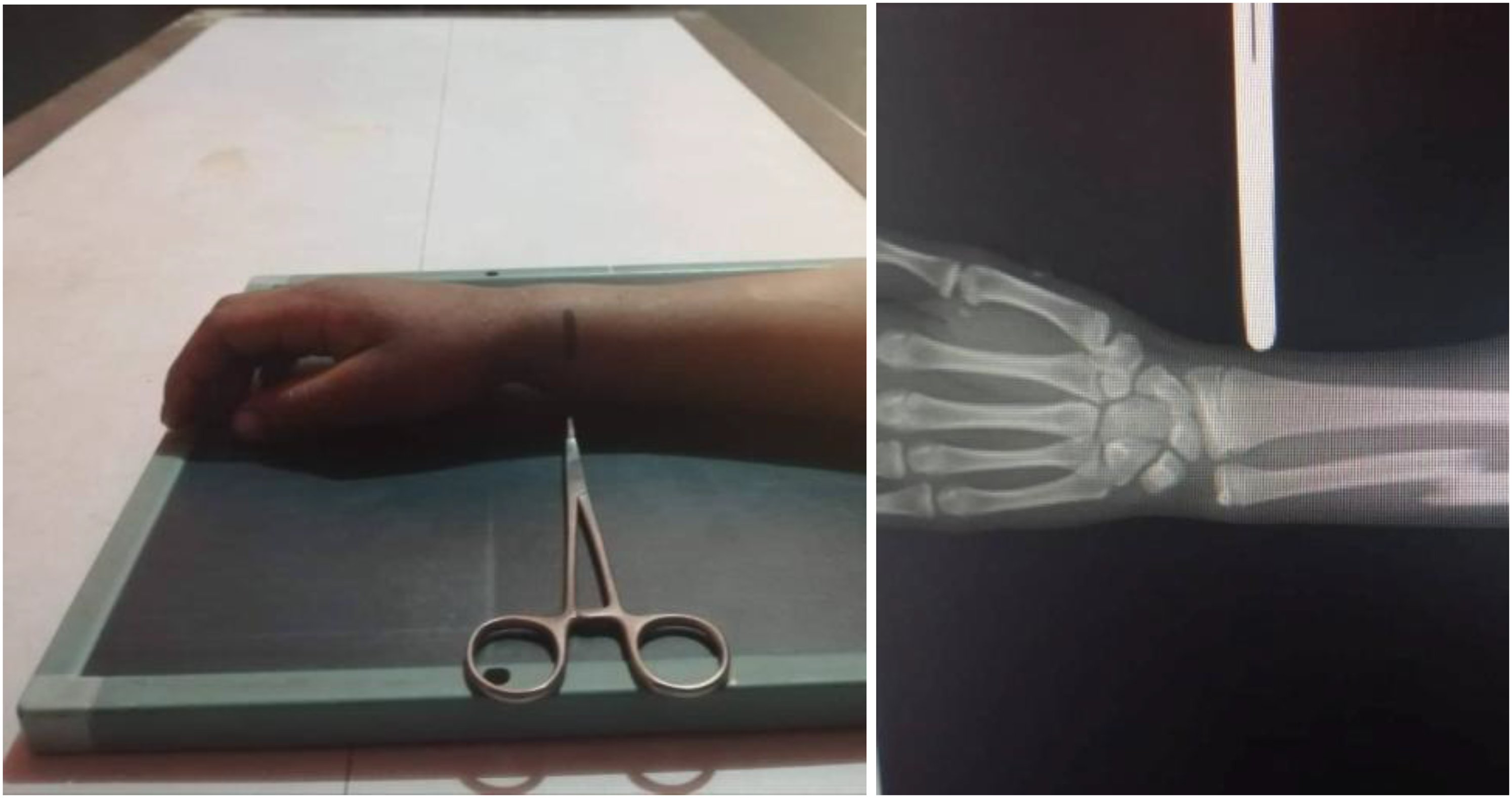
Footnotes
Acknowledgements
The author would like to express his sincere gratitude to the clinical and nursing staffs of Saileshwori hospital, Doti for their dedicated support in patient care. Special thanks to the patients and their parents for being part of the study.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.