
Abstract
Objective
To evaluate how specific psychiatric comorbidities relate to index length of stay (LOS), hospital costs, and in-hospital mortality during readmissions after HF hospitalization.
Methods
A retrospective cohort study was conducted using the 2016-2022 Nationwide Readmissions Database. Adults with a principal HF diagnosis were included. Psychiatric comorbidities were depression, anxiety, bipolar disorder, schizophrenia/psychotic disorders, post-traumatic stress disorder (PTSD), and substance use disorder (SUD). Outcomes were index LOS, inflation-adjusted costs, and in-hospital mortality during readmissions within 30 days and up to 1 year after discharge. Survey-weighted multivariable models adjusted for demographics, socioeconomic factors, hospital characteristics, discharge disposition, and comorbidity burden; P ≤ 0.001 was prespecified as the level of statistical significance.
Results
Among 31,886,859 weighted HF hospitalizations, psychiatric comorbidity was common. Anxiety was associated with longer LOS (β = 0.88 days; P < 0.001) and higher costs (β = $2779; P < 0.001) but there were no differences in 30-day or 1-year mortality. However, several diagnoses were associated with lower mortality, including depression (30-day OR = 0.86; 1-year OR = 0.86), bipolar disorder (0.66; 0.68), schizophrenia/psychotic disorders (0.68; 0.72), PTSD (0.73; 0.78), and SUD (0.87; 0.92) (all P < 0.001). Bipolar disorder showed the largest cost reduction (β = −$1320; P < 0.001) compared to HF patients without bipolar disorder.
Conclusion
Psychiatric comorbidity in HF is common. Anxiety is associated with increased hospital utilization, but is not associated with mortality, whereas several other diagnoses are associated with lower mortality. Costs were lower for depression and bipolar disorder. These diagnosis-specific patterns support targeted screening, early consultation, and integrated consultation-liaison care pathways during HF hospitalization.
Keywords
Introduction
Heart failure (HF) is a leading cause of morbidity, mortality, and rising healthcare costs in the United States. As of 2024, HF was estimated to affect approximately 6 million American adults aged 20 years or older, and this number is expected to rise as the population ages. 1 In 2023, HF was listed on more than 450,000 death certificates, accounting for nearly 15% of all U.S. deaths. 2 In 2012, the economic burden of HF was estimated at $30.7 billion, a figure projected to reach $69.7 billion by 2030. 3 HF therefore places a substantial and growing burden on the healthcare system and on society in the United States.
Psychiatric comorbidities occur frequently in HF and contribute to symptom burden, functional impairment, and reduced quality of life.4-6 The intersection of cardiovascular disease and psychiatric illness is central to consultation-liaison (C-L) psychiatry, in which psychiatric symptoms, diagnoses, and treatment decisions can shape hospital course, discharge planning, and follow-up care in medically complex patients. Meta-analytic data indicate that approximately 25% of patients with HF also meet criteria for depression. 4 However, the psychiatric burden in HF extends beyond depression to include substance use disorder (SUD), anxiety, post-traumatic stress disorder (PTSD), schizophrenia, and bipolar disorder. 5 These conditions may be under-recognized or undertreated in HF because of overlapping clinical presentations and competing medical priorities. When unaddressed, psychiatric comorbidities may worsen HF-related outcomes through mechanisms such as reduced treatment adherence, functional decline, and increased healthcare utilization.6,7
Most prior studies have linked psychiatric comorbidities in HF to adverse clinical outcomes, including higher hospitalization rates and mortality.6-8 However, existing evidence is constrained by inconsistent measurement of psychiatric diagnoses, reliance on smaller or geographically restricted samples, and limited assessment of diagnosis-specific effects. In addition, many studies have assessed psychiatric illness as a single exposure, which may obscure clinically important heterogeneity across diagnoses with distinct symptom profiles, treatment needs, and care pathways. Accordingly, this study examined diagnosis-specific associations between psychiatric comorbidities and HF outcomes, including index hospital length of stay (LOS), inflation-adjusted hospital costs, and 30-day and 1-year mortality, using a large, nationally representative Nationwide Readmissions Database (NRD).
Methods
Data Source
A retrospective cohort study was conducted using the 2016-2022 NRD, a component of the Healthcare Cost and Utilization Project (HCUP), which captures all-payer inpatient discharges from 30 states in the United States and represents approximately 60% of national hospitalizations. 9 Since each annual NRD file is independent, 1-year readmissions were assessed within the same calendar year. The NRD contains discharge-level information, including ICD-10-CM diagnosis codes, patient demographics, hospital characteristics, LOS, discharge disposition, and total charges.
Study Population
Included were adult patients aged 18 years or older who were hospitalized with a principal diagnosis of HF, identified using ICD-10 codes I50.1 through I50.9. Index discharges that resulted in in-hospital death, transfer to another acute-care hospital, or had missing demographic or readmission variables were excluded (Figure 1). Readmissions flagged as “planned” by HCUP were excluded from outcome ascertainment. The unit of analysis was the individual hospitalization. Each eligible HF hospitalization was considered an index admission for the LOS and cost analyses. Post-discharge outcomes were assessed using NRD readmission tracking within the same calendar year. Accordingly, 1-year outcomes reflect in-hospital mortality occurring during a readmission within 30 days or up to 1 year after discharge, as captured by discharge disposition. Because each annual NRD file is independent and the database does not capture out-of-hospital deaths, cross-year readmissions and deaths occurring outside the hospital were not observed. Cohort selection and sample size by year (unweighted and weighted)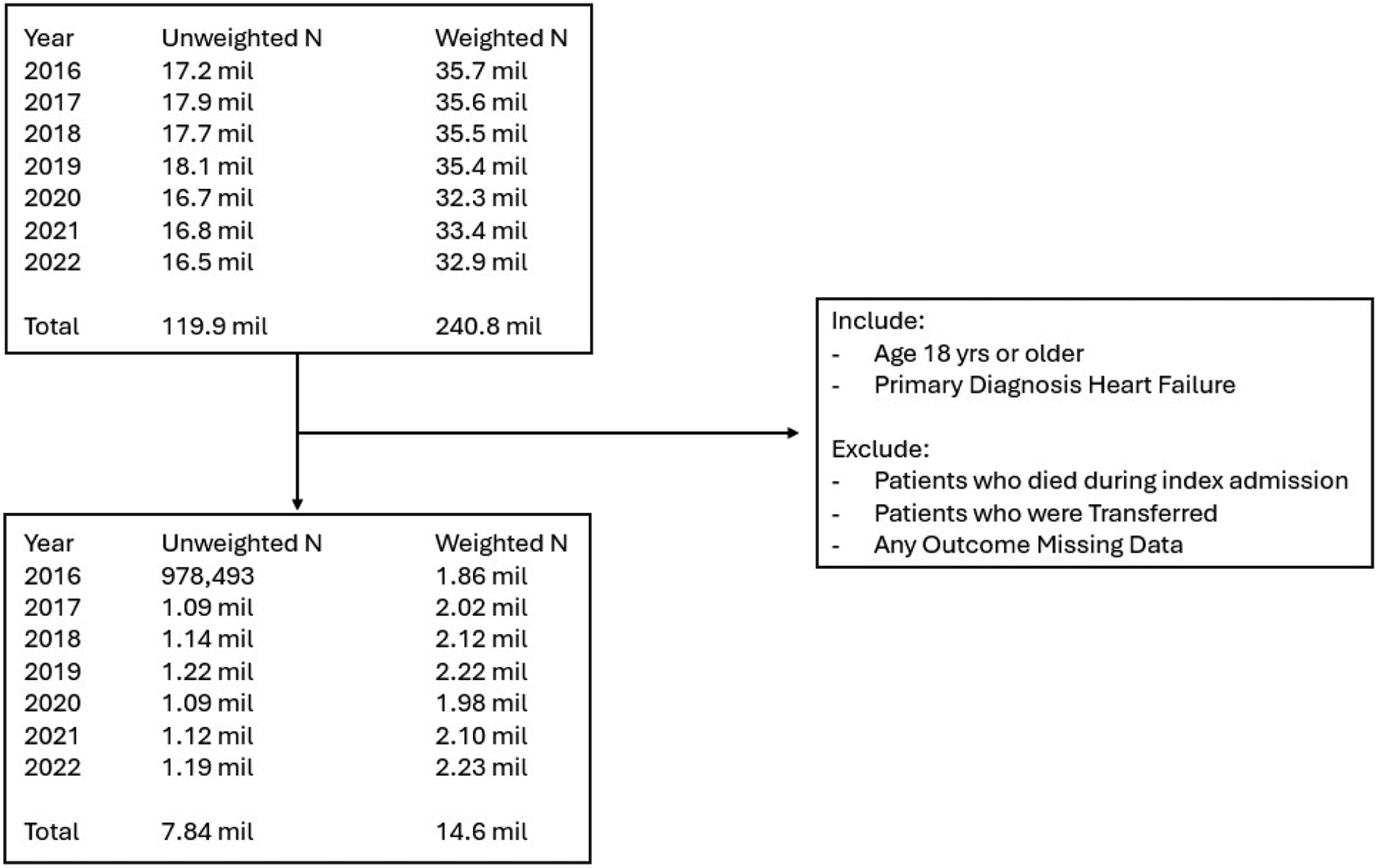
The Nationwide Readmissions Database (NRD), 2016-2022, was used to identify adult (≥18 years) index hospitalizations with a principal diagnosis of heart failure. Records were excluded for in-hospital death during the index admission, transfer to another acute-care hospital, or for missing outcome data. Unweighted counts reflect the NRD sample, whereas weighted counts represent national estimates.
Psychiatric Comorbidity Definitions
To examine the effects of psychiatric comorbidities, patients with 1 or more psychiatric diagnoses were identified using the following ICD-10 codes: depression (F32.0-F32.9, F33.0-F33.9), anxiety (F40.0-F41.9), bipolar disorder (F31.0-F31.9), schizophrenia/psychotic disorders (F20.0-F20.9, F25.0-F25.9), PTSD (F43.10-F43.12), and SUDs (F10-F16, F18-F19, nicotine was excluded because of clinical differences from the other substances). These comorbidities represent diagnosed (ICD-10-CM coded) psychiatric conditions recorded during the index hospitalization and may underestimate symptom-based prevalence because of underdiagnosis or undercoding. Although some ICD-10-CM codes include remission specifiers for certain conditions, discharge-level administrative data do not reliably capture symptom severity, chronicity, or whether a condition is active or in remission at the time of hospitalization across all diagnostic groups. Accordingly, psychiatric comorbidities in this study should be interpreted as documented (coded) diagnoses rather than as severity-stratified or symptom-based conditions.
Outcome Measures
Outcomes included index admission LOS, inflation-adjusted hospital costs, and mortality within 30 days and 1 year after the index discharge. LOS was defined as the number of days between admission and discharge. Hospital charges were converted to costs using HCUP cost-to-charge ratios and inflation-adjusted to 2022 U.S. dollars using the CPI-U. Mortality was determined using the discharge disposition recorded in the NRD and reflects only in-hospital deaths occurring during a rehospitalization within 30 days or 1 year after discharge.
Covariates
Covariates included patient demographics (age, sex, primary payer, and ZIP code-based income quartile), hospital-level characteristics (bed size, location, and teaching status), admission timing (weekend vs weekday), discharge disposition, and comorbidity burden measured using the Charlson Comorbidity Index (CCI). 10
Statistical Analysis
Survey-weighted estimates were calculated using HCUP discharge weights. Baseline characteristics were summarized as weighted means with standard errors (SEs) for continuous variables, and as weighted proportions with SEs for categorical variables. Differences between groups (ie, with vs without SUD) were assessed using weighted univariate linear regression or chi-square tests, as appropriate. Multivariable linear regression models were developed to estimate adjusted differences (β coefficients with 95 % confidence intervals) in index LOS and inflation-adjusted hospital costs, with adjustment for demographic, socioeconomic, and hospital factors. For mortality outcomes, survey-weighted logistic regression models were used to estimate adjusted odds ratios (ORs) with 95% confidence intervals for in-hospital mortality at 30 days and 1 year during readmission among patients discharged home after the index admission. Because of the large sample size, a stringent significance threshold of P ≤ 0.001 was applied to limit the type I error rate. Although statistical significance was set at P ≤ 0.001, 95% confidence intervals are reported for effect-size interpretation and comparability with prior literature; P-values are used to determine statistical significance under the prespecified threshold.
Software and Ethics Compliance
All analyses were conducted using Stata SE 18 (StataCorp, 2023). The study adhered to the HCUP Data Use Agreement, and as a retrospective analysis of de-identified data, it was exempt from institutional review board review.
Results
Cohort Characteristics
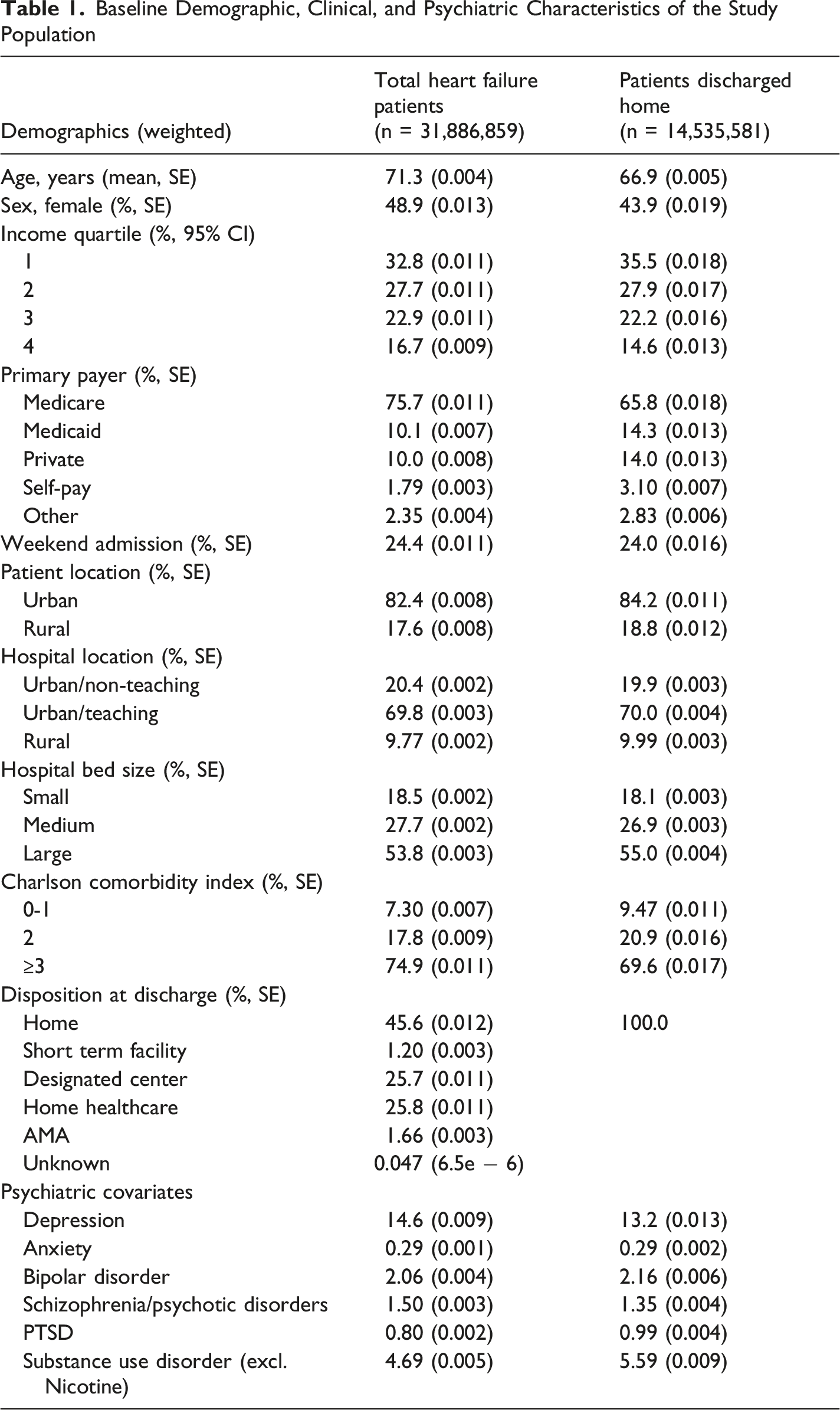
The initial analysis included 31,886,859 weighted hospitalizations for HF identified from the NRD. The mean patient age was 71.3 years (SE, 0.004), and women accounted for 48.9% of the cohort. Most patients were insured by Medicare (75.7%) and resided in urban settings (82.4%). The lowest income quartile contained the most patients (32.8%). More than half of admissions occurred at large hospitals (53.8%), and most patients were treated at urban teaching institutions (69.8%). Nearly three-quarters of patients had a CCI score of 3 or above. At discharge, 45.6% of patients were discharged home, 25.8% received home healthcare, and 25.7% were transferred to post-acute care facilities.
Patients discharged home represented 45.6% of the overall HF cohort (n = 14,535,581). The total HF cohort is presented to describe the overall national population of HF hospitalizations. In contrast, the home-discharge cohort is reported separately because discharge disposition is closely related to illness severity, post-discharge care setting, readmission risk, and mortality interpretation. Compared with the total HF cohort, patients discharged home were younger and included a smaller proportion of women. In addition, the proportion of patients in the lowest income quartile increased from 32.8% to 35.5%. The primary payer among patients discharged home remained Medicare; however, the proportion of Medicare beneficiaries decreased from 75.7% in the total HF cohort to 65.8% among patients discharged home. Conversely, the proportion of patients with private insurance increased from 10.0% to 14.0%. Although statistically significant differences were detected, the distribution of hospital characteristics remained similar between the total HF cohort and the home-discharge cohort.
Baseline Demographic, Clinical, and Psychiatric Characteristics of the Study Population
Index Admission LOS and Hospital Cost
Adjusted Association Between Psychiatric Comorbidities and Index Hospital Length of Stay and Costs
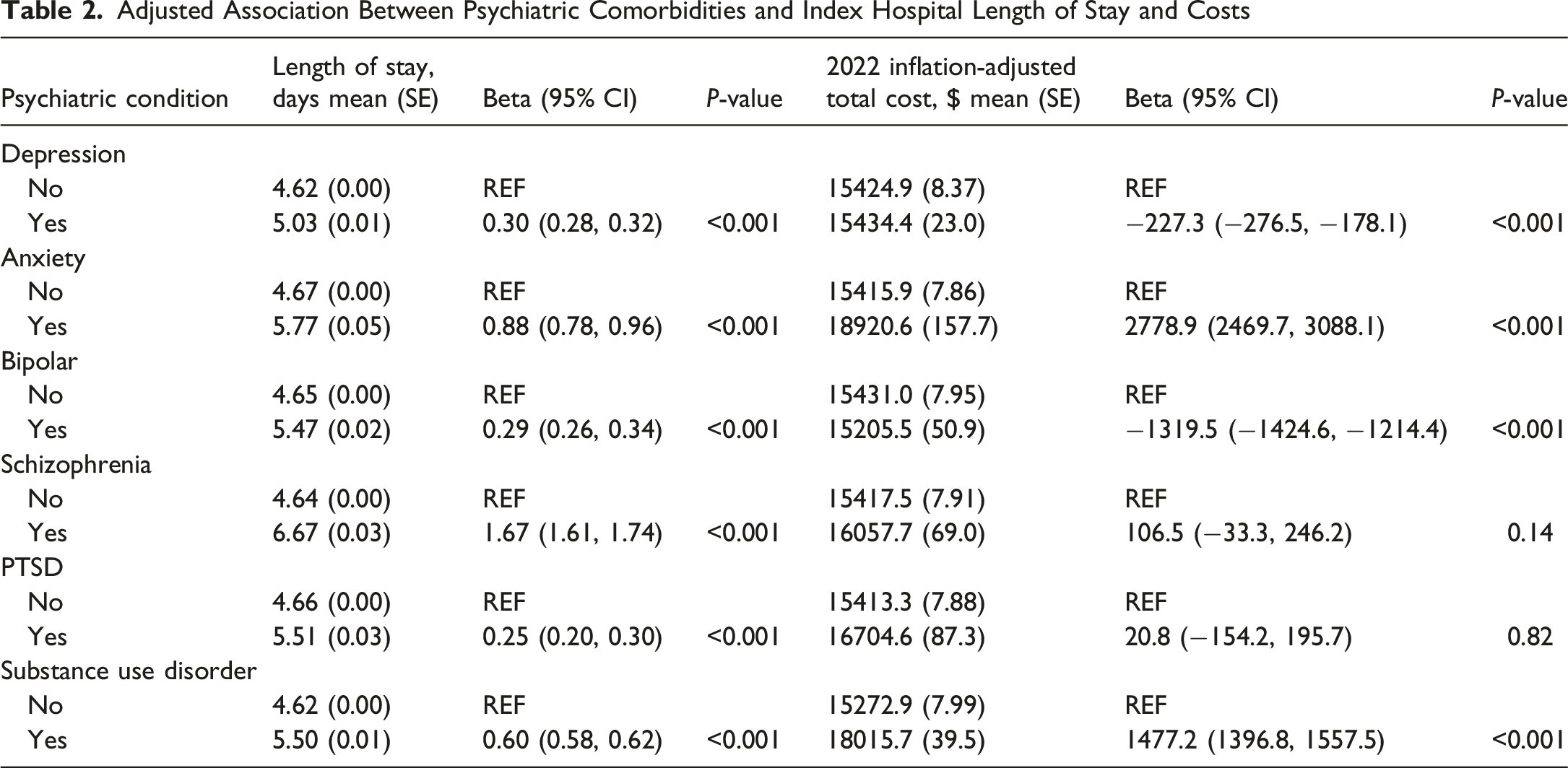
Multivariable linear regression, adjusted for demographics, socioeconomic status, and hospital characteristics, revealed diagnosis-specific effects on LOS (Table 2). Schizophrenia was associated with the largest increase in LOS, with patients staying 1.67 days longer than those without schizophrenia (β = 1.67; 95% CI, 1.61 to 1.74; P < 0.001). Anxiety disorders were also associated with a substantial increase in LOS (β = 0.88; 95% CI, 0.78 to 0.96; P < 0.001), while substance use disorder was associated with a smaller but statistically significant increase (β = 0.60; 95% CI, 0.58 to 0.62; P < 0.001). In contrast, depression status (β = 0.30; 95% CI, 0.28 to 0.32; P < 0.001), bipolar disorder (β = 0.29; 95% CI, 0.26 to 0.34; P < 0.001), and PTSD (β = 0.25; 95% CI, 0.20 to 0.30; P < 0.001) were associated with smaller increases in LOS.
Inflation-adjusted hospital costs followed a pattern distinct from LOS. Anxiety was associated with a substantial cost increase, with affected patients incurring an additional $2778 (β = 2778.9; 95% CI, 2469.7 to 3088.1; P < 0.001). In addition, SUD was associated with a $1477.2 increase in cost compared to no SUD (β = 1477.2; 95% CI, 1396.8 to 1557.5; P < 0.001). Depression was associated with lower costs, reducing the estimated hospital cost by $227.3 (β = −227.3; 95% CI, −276.5 to −178.1; P < 0.001). Bipolar disorder was associated with the largest cost reduction, with patients incurring $1319.5 less than those without bipolar disorder (β = −1319.5; 95% CI, −1424.6 to −1114.4; P < 0.001). Schizophrenia/psychotic disorders and PTSD were not significantly associated with cost.
Abbreviations: CI, confidence interval; LOS, length of stay; PTSD, post-traumatic stress disorder; SE, standard error; SUD, substance use disorder.
All values are survey-weighted estimates. Multivariable linear regression models were adjusted for age, sex, primary payer, ZIP code-based income quartile, hospital bed size, hospital location/teaching status, weekend admission, discharge disposition, and Charlson Comorbidity Index.
In-hospital mortality within the 30-day and 1-year readmission windows
Adjusted Association Between Psychiatric Comorbidities and In-Hospital Mortality During Readmissions
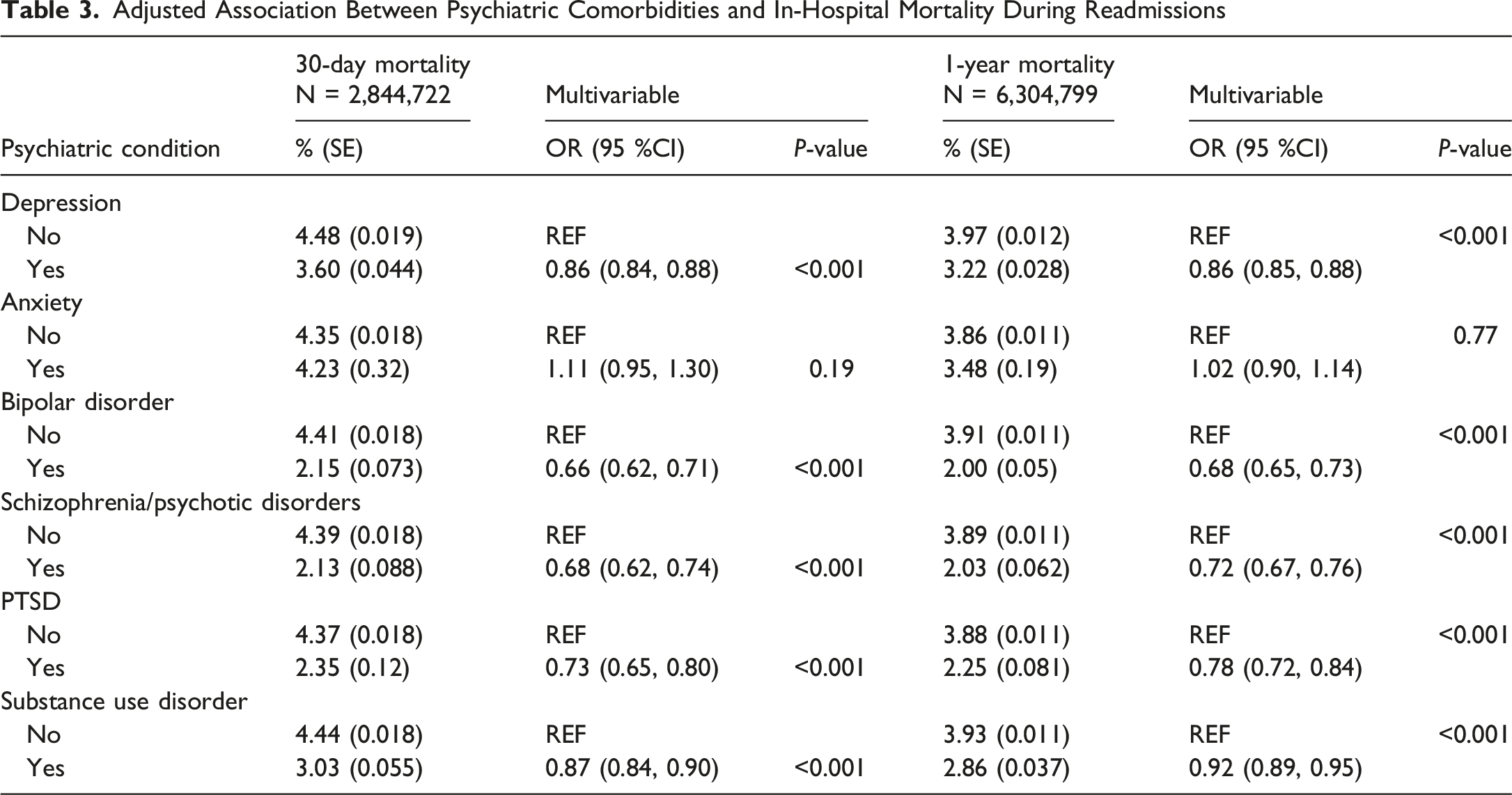
After multivariable adjustment, depression was associated with lower mortality at both time points: the OR for mortality during readmission at 30-day was 0.86 (95% CI, 0.84-0.88; P < 0.001), and the OR for mortality during 1-year readmission was 0.86 (95% CI, 0.85-0.88; P < 0.001). Bipolar disorder was associated with the lowest odds of mortality, with a 30-day readmission OR of 0.66 (95% CI, 0.62-0.71; P < 0.001) and a 1-year readmission death OR of 0.68 (95% CI, 0.65-0.73; P < 0.001), corresponding to approximately33% lower odds of death compared with HF patients without bipolar disorder.
Schizophrenia/psychotic disorders, PTSD, and SUD were also linked to significantly lower mortality. Schizophrenia/psychotic disorders were associated with 32% lower odds of 30-day readmission mortality compared with admissions without these disorders (0.68 (95% CI, 0.62-0.74; P < 0.001). Furthermore, 1-year readmission mortality decreased by 28% in the same group (0.72 (95% CI, 0.67-0.76); P < 0.001). PTSD was associated with a 27% and 22% reduction in the odds of 30-day and 1-year readmission mortality, respectively (30-day: OR of 0.73 (95% CI, 0.65-0.80; P < 0.001 and 1-year: OR of 0.78 (95% CI, 0.72-0.84; P < 0.001). SUD showed a modest reduction in 30-day and 1-year readmission mortality of 13% and 8%, respectively (30-day: OR of 0.87 (95% CI, 0.84-0.90; P < 0.001 and 1-year: OR of 0.92 (95% CI, 0.89-0.95; P < 0.001). Only anxiety did not show a significant mortality difference. Adjusted 30-day readmission mortality among patients with anxiety (4.23%) was similar to that among patients without anxiety (4.35%), with an OR of 1.11 (95% CI, 0.95-1.30; P = 0.19). Similarly, adjusted 1-year mortality did not differ significantly (OR = 1.02; 95% CI, 0.90-1.14; P = 0.77).
Abbreviations: CI, confidence interval; OR, odds ratio; PTSD, post-traumatic stress disorder; SE, standard error; SUD, substance use disorder.
Values are survey-weighted estimates. Multivariable logistic regression models were adjusted for age, sex, primary payer, ZIP code-based income quartile, hospital bed size, hospital location/teaching status, weekend admission, discharge month, discharge disposition, and Charlson Comorbidity Index. Mortality reflects in-hospital death occurring during a readmission within 30 days or 1 year after the index discharge.
Discussion
LOS and Cost Outcomes
In this contemporary national cohort of patients hospitalized for HF, psychiatric comorbidities were common and showed heterogeneous associations with index admission resource use. Anxiety and SUD were the only diagnoses linked to both longer LOS and higher costs, whereas depression and bipolar disorder were associated with lower index admission costs. Prior work in HF suggests that psychiatric comorbidity is associated with greater downstream utilization, including higher readmission risk after HF admission. 11 The findings of this study extend this literature by showing diagnosis-specific heterogeneity in index admission resource use: anxiety and SUD were associated with higher LOS and higher costs, whereas depression and bipolar disorder were associated with lower index admission costs. A recent retrospective, cross-sectional observational study reported that patients with psychological distress after myocardial infarction incurred higher medical expenditures and greater healthcare utilization. 12 Although that study reported higher expenditures overall, these results suggest the relationship is diagnosis-specific in HF, with higher costs for anxiety and SUD but lower index costs for depression and bipolar disorder.
Prior work indicates that some psychiatric conditions may be associated with lower use of invasive cardiovascular procedures during hospitalization. 13 However, the present study did not assess procedure utilization by psychiatric diagnosis, and this mechanism therefore cannot explain the diagnosis-specific cost patterns observed. Importantly, the variation in findings across specific psychiatric diagnoses highlights the need for diagnosis-specific stratification. For example, anxiety was found to be associated with a longer LOS and higher cost, possibly reflecting the established link between anxiety and adverse cardiovascular outcomes. 14 The association of schizophrenia/psychotic disorders with increased LOS but no difference in cost may reflect complex discharge planning and unmeasured differences in inpatient management.
Mortality Outcomes
The observed association between several psychiatric comorbidities and lower in-hospital mortality during readmissions warrants careful interpretation. With the exception of anxiety, all examined psychiatric comorbidities were associated with lower in-hospital mortality during 30-day and 1-year readmissions. These associations should not be interpreted as evidence of a causal or protective effect. Instead, they may reflect residual confounding, differential diagnostic recognition or coding, selection effects related to hospitalization and readmission, diagnosis-specific differences in illness severity or inpatient monitoring, and incomplete outcome capture because the NRD does not record out-of-hospital deaths. Taken together, these patterns indicate that psychiatric comorbidity in HF does not act as a uniform risk factor and should be interpreted in the context of prior literature that has often reported adverse associations. It is also important to acknowledge that patients with psychiatric conditions often experience poorer continuity of medical care, 12 which may influence downstream outcomes.
Comparison With Prior Evidence
Most prior studies and reviews have reported that psychiatric comorbidities, especially depression and anxiety, but also schizophrenia/psychotic disorders and SUD, are associated with worse outcomes in HF, including higher mortality and rehospitalization,6-8,13-17 with greater utilization also reported.6,11,18,19 The findings of this study differ from much of the prior literature in showing diagnosis-specific heterogeneity and lower observed in-hospital mortality during readmissions in several groups. These results highlight the need to stratify risk by specific psychiatric diagnoses rather than treating psychiatric comorbidity as a single exposure. Prior work frequently aggregated psychiatric conditions, which may obscure divergent associations; by disaggregating diagnoses and using a large, nationally representative cohort, this analysis reveals patterns that smaller or pooled studies could miss. Recognizing these divergences from prior work, it is important to consider the clinical and health-system implications of these findings, particularly how diagnosis-specific stratification may inform patient management and resource allocation.
Clinical and Policy Implications
The findings of this study demonstrate diagnosis-specific heterogeneity in how psychiatric comorbidities relate to HF outcomes, which argues against treating “any psychiatric comorbidity” as a single risk factor. Clinical risk models for mortality and readmission may benefit from incorporating specific diagnoses rather than a binary indicator, which may improve risk stratification accuracy and resource planning. For C-L psychiatry, these results support routine, structured screening for depression, anxiety, PTSD, psychotic disorders, bipolar disorder, and substance use at the time of HF admission, together with embedded referral pathways that do not depend on ad hoc requests.6,12
Because anxiety and SUD were associated with longer LOS and higher costs across this cohort, hospitals should consider early C-L psychiatry consultation for anxiety or SUD symptoms, standardized symptom management plans, and coordinated care pathways that may reduce potentially avoidable utilization. 20 For SUD, the combination of longer stays and increased costs alongside lower observed mortality suggests risk of incomplete outcome capture due to limitations of the NRD; care pathways should emphasize withdrawal management protocols, the initiation of medications for opioid or alcohol use disorder when indicated, and warm handoffs to outpatient treatment, with targeted efforts to reduce discharge against medical advice and to limit early readmissions.18,19 For schizophrenia/psychotic disorders, prolonged stays without an increase in cost reflect a corresponding increase in cost points to complex discharge planning; early coordination among C-L psychiatry, social work, and case management may prevent avoidable inpatient days while maintaining post-discharge safety. For depression, PTSD, and bipolar disorder, screening should still be paired with timely treatment initiation, structured follow-up, particularly because the lower observed in-hospital mortality during readmissions should not be interpreted as evidence that these conditions are protective.6,12
At the policy level, health systems should align quality metrics and reimbursement with integrated cardiac-psychiatric care, including EHR-based consult triggers for positive screens and diagnosis-specific care bundles, and ensure coverage for outpatient follow-up that sustains these inpatient gains. 12
Study Limitations
This study has several important limitations. First, administrative ICD-10 coding may not reliably capture psychiatric comorbidities in patients with HF. These codes do not distinguish symptom severity, chronicity, or timing of diagnosis, and underdiagnosis or undercoding could bias associations in either direction. In addition, discharge coding does not consistently distinguish active from historical or remitted psychiatric conditions across hospitals, which may contribute to misclassification and could bias diagnosis-specific associations. Because psychiatric diagnoses frequently co-occur, the diagnosis-specific associations reported in this study may also be influenced by psychiatric multimorbidity. The present analysis was designed to assess individual diagnosis-specific associations rather than combinations of psychiatric conditions; therefore, overlap among psychiatric diagnoses was not directly examined. Future studies should examine whether psychiatric multimorbidity confers additional risk beyond that of individual psychiatric diagnoses.
Second, the NRD captures readmissions only within the same calendar year and only within participating states. Patients who die after discharge, relocate, or are rehospitalized across state lines may be missed, potentially underestimating longer-term outcomes. Because the NRD does not record out-of-hospital deaths, mortality estimates reflect only in-hospital deaths during subsequent admissions and may underestimate the total mortality. Although the model was adjusted for hospital characteristics, including teaching status and location, residual confounding by hospital setting (eg, urban teaching vs non-teaching patterns in case mix, palliative care utilization, and discharge practices) may persist and could influence the observed associations.
Third, the database lacks detailed clinical information, including ejection fraction, ischemia burden, biomarker and angiographic findings, and medication adherence. Psychiatric treatment details, such as the use of psychotropic medications, psychotherapy, or C-L psychiatry involvement, were also unavailable. As a result, the influence of illness severity or treatment on outcomes could not be determined.
Fourth, differential coding practices across hospitals and states may have introduced variability in the classification of both HF and psychiatric conditions, potentially biasing the results. In addition, unmeasured social determinants of health (eg, housing stability, caregiver support, and access to follow-up care) may contribute to differences in outcomes but were not captured in this dataset.
Finally, although the NRD provides a large and nationally representative sample of U.S. hospitalizations, the findings may not be generalizable to non-participating states or to international healthcare systems. As with all retrospective observational studies, the results reflect associations rather than causality, and residual confounding remains possible despite multivariable adjustment.
Conclusion
In this large, nationally representative cohort of patients hospitalized for HF, psychiatric comorbidities were common and showed heterogeneous associations with hospital utilization and in-hospital mortality during readmissions. Anxiety and SUD were associated with longer LOS and higher hospital costs, whereas depression and bipolar disorder were associated with lower costs. Depression, bipolar disorder, schizophrenia/psychotic disorders, PTSD, and SUD were associated with lower observed in-hospital mortality during readmissions, whereas anxiety was not associated with mortality. These findings support diagnosis-specific risk stratification and integrated cardiac-psychiatric care pathways during HF hospitalization. However, the mortality findings should be interpreted cautiously, given the potential for residual confounding, administrative coding limitations, selection effects, and incomplete capture of out-of-hospital deaths. Future work should examine the mechanisms driving these heterogeneous associations and determine whether targeted psychiatric interventions can improve utilization and outcomes in patients with HF.
Footnotes
Ethical Considerations
This study used de-identified administrative data obtained through HCUP after completion of the required Data Use Agreement training and was exempt from institutional review board oversight.
Author Contributions
Austin A. Charles: Contributed to the conception and design of the study; contributed to interpretation of the data; drafted substantial portions of the manuscript; revised the manuscript critically for important intellectual content; approved the final version to be submitted; and agrees to be accountable for all aspects of the work. Kyle E. Thurmann: Contributed to the conception and design of the study; contributed to interpretation of the data; drafted substantial portions of the manuscript; revised the manuscript critically for important intellectual content; approved the final version to be submitted; and agrees to be accountable for all aspects of the work. Peter L. Ernst: Contributed to manuscript drafting and revision; contributed to interpretation of the data; revised the manuscript critically for important intellectual content; approved the final version to be submitted; and agrees to be accountable for all aspects of the work. Paul T. Kang: Contributed to acquisition, analysis, and interpretation of the data; performed the statistical analysis; revised the manuscript critically for important intellectual content; approved the final version to be submitted; and agrees to be accountable for all aspects of the work. Michael D. White: Supervised the study; contributed to the conception and design of the study; contributed to interpretation of the data; revised the manuscript critically for important intellectual content; approved the final version to be submitted; and agrees to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this study were obtained from the Healthcare Cost and Utilization Project (HCUP) Nationwide Readmissions Database (NRD), sponsored by the Agency for Healthcare Research and Quality (AHRQ). Under the terms of the HCUP Data Use Agreement, the authors are prohibited from sharing or distributing the dataset. Researchers may obtain access by applying through the HCUP Central Distributor and completing the required training and data purchase.