
Abstract
This study examined the association between digital literacy (DL) and depression among older adults with chronic diseases and tested the moderating role of self-rated health (SRH). A cross-sectional secondary analysis was conducted using data from the 2023 National Survey of Older Koreans, including 8,588 adults aged 65 years or older with at least one chronic disease. Depression was assessed using the Short Form of the Korean Geriatric Depression Scale. Hierarchical regression and moderation analyses were performed, adjusting for sociodemographic covariates. Higher levels of DL were associated with lower depression. SRH was a significant predictor of depression and moderated the relationship between DL and depression, with a significant protective effect of DL observed only at low and average levels of SRH. DL may help reduce depression among older adults with chronic diseases, particularly those with poorer perceived health.
Introduction
South Korea has experienced rapid population aging since entering an aged society in 2017. In 2024, adults aged 65 years and older accounted for 19.6% of the total population, a figure projected to reach 25.5% by 2030 (Statistics Korea, 2024). As the older population has grown, the prevalence of chronic diseases has risen sharply, with 89.2% of older adults having at least one chronic condition (National Health Insurance Service, 2024). Managing chronic diseases often involves complex treatment regimens and polypharmacy, which increase the burden of self-management and elevate the risk of depression among older adults (Zhang et al., 2025).
According to the 2023 National Survey of Older Koreans, 11.3% of adults aged 65 years and older report depressive symptoms, with prevalence increasing with age (Kang et al., 2023). Late-life depression is associated with reduced disability-free survival, higher risks of persistent physical disability, and increased mortality (Jeong et al., 2022; Roebuck et al., 2023). Older adults with chronic diseases are particularly vulnerable, as the risk of depression increases with the presence and number of chronic conditions (Du et al., 2025). Identifying factors that influence depression in this population is therefore important, particularly in rapidly aging societies where chronic disease management increasingly relies on individual self-management capacities.
Digital literacy (DL) refers to the ability to access information and to communicate through digital technologies such as the internet, applications, social media, and mobile devices, and is considered an essential skill in contemporary society (Rani, 2025). Although South Korea is among the fastest OECD countries in digital technology adoption, a substantial digital divide persists among older adults (Lee, 2024). Since the COVID-19 pandemic, the rapid digitalization of social and public services has further widened gaps in information access, contributing to increased social isolation and lower life satisfaction among older adults (Lee, 2024; Tiirinki et al., 2020). Older adults with chronic diseases face particular challenges in navigating increasingly digitalized healthcare systems (Kelly et al., 2025; Shams-Ghahfarokhi, 2025). Previous studies have shown that higher DL among older adults is associated with lower levels of depression and higher life satisfaction (Kim et al., 2025; Lu, 2024), and that DL interventions can reduce depressive symptoms (Lee et al., 2022).
Based on social cognitive theory (SCT), individuals’ cognitive capabilities and self-efficacy interact with environmental factors to shape their behaviors and emotional outcomes (Bandura, 2001). DL, defined as the cognitive and functional ability to understand and use information in digital environments, enables individuals to engage in online interactions, maintain social relationships, and expand social networks. Through these processes, DL may function as an important psychosocial resource by reducing social isolation, expanding opportunities for successful interpersonal experiences, and thereby enhancing self-efficacy (Di & Wang, 2025; Kim et al., 2023; Yuan et al., 2025). Meanwhile, low self-efficacy and social isolation have been identified as key factors associated with increased levels of depression (Bandura et al., 1999; Luo, 2023). Taken together, these findings suggest that DL is associated with depression through mechanisms such as self-efficacy and social integration. However, depression in older adults is a multifactorial phenomenon that cannot be fully explained by DL alone. Despite this complexity, most previous studies have primarily focused on the direct relationship between DL and depression, while relatively limited attention has been given to moderating variables that may account for individual differences.
While SCT elucidates the mechanisms through which DL may reduce depression, it does not account for individual differences in how these mechanisms operate. The common-sense model of self-regulation (CSM) provides a complementary perspective by explaining how individuals’ subjective health perceptions influence their emotional responses and self-regulatory behaviors, including engagement with coping resources such as DL (Leventhal et al., 2016). Self-rated health (SRH) reflects individuals’ perceptions of their overall physical and mental health and has been shown to be a strong predictor of psychological, physical, and social quality of life among older adults (Kim, 2020). Previous research has consistently demonstrated that poorer SRH is associated with higher levels of depression among middle-aged and older adults (Leng et al., 2025). Even among older adults with the same chronic conditions, depression levels vary substantially depending on how individuals perceive their own health (Park et al., 2016). DL can function as a resource that enhances self-regulation by improving health information-seeking and problem-solving abilities (van der Vaart & Drossaert, 2017). However, the effectiveness of such resources may vary depending on how individuals perceive their own health. According to the CSM, individuals’ health perceptions shape their emotional responses and coping behaviors (Leventhal et al., 2016), suggesting that even when individuals possess the same level of resources, differences in cognitive appraisal—namely SRH—may influence how these resources are utilized and the outcomes they produce. Accordingly, SRH may be better conceptualized not as a mediator through which the effect of DL operates, but as a conditional factor that moderates the strength and direction of the relationship between DL and depression. This underscores the need to empirically examine the moderating role of SRH in the present study.
Research examining the relationship between DL and depression among older adults has steadily increased (Kim et al., 2024), including studies based on national-level datasets. However, most previous studies have analyzed older adults as a single group without distinguishing those with chronic conditions (Park & Yoo, 2023; Song et al., 2025), thereby insufficiently reflecting the specific vulnerabilities and needs of older adults with chronic diseases. Older adults with chronic diseases require greater digital competence for ongoing self-management and health information seeking; however, they are also particularly vulnerable to digital exclusion due to declining physical function and technological barriers (Li et al., 2025). Despite these characteristics, research that systematically examines the relationship between DL and depression specifically among this population remains limited. Furthermore, although SRH has been consistently identified as an important factor associated with depression (Leng et al., 2025), relatively little research has examined whether SRH moderates the association between DL and depression. By focusing on older adults with chronic diseases and examining SRH as a moderator, this study extends previous research and provides evidence for identifying subgroups who may benefit most from targeted DL-related interventions and policy support.
Accordingly, this study aims to examine the effect of DL on depression among older adults with chronic diseases using nationally representative data from the 2023 National Survey of Older Koreans and to investigate the moderating effect of SRH on this relationship. Through this approach, the study seeks to identify factors that mitigate or exacerbate depression among older adults in the digital era and to provide foundational evidence for the development of DL-enhancing interventions targeting older adults with chronic diseases. The research questions of this study are as follows: (i) Is DL significantly associated with depression among older adults diagnosed with chronic diseases? (ii) Does SRH significantly moderate the association between DL and depression among older adults diagnosed with chronic diseases?
Methods
Study Design
This study is a secondary data analysis using the 2023 National Survey of Older Koreans. It employs a cross-sectional correlational design to examine the effect of DL on depression among older adults with chronic diseases and to test the moderating effect of SRH. The conceptual research model is presented in Figure 1.
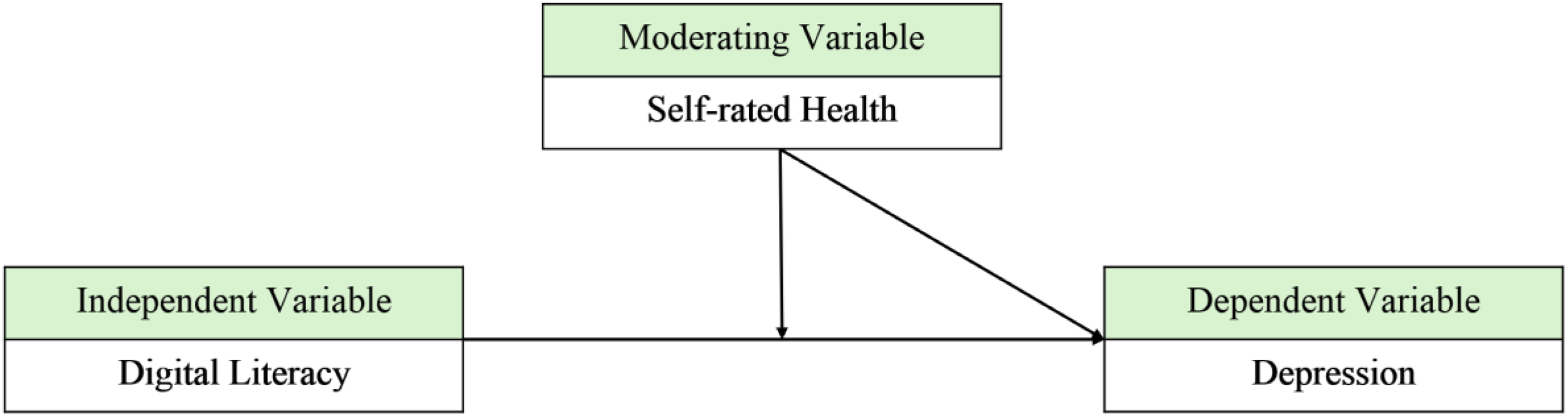
The conceptual research model.
Participants and Data Collection
This study used data from the 2023 National Survey of Older Koreans, a nationwide survey of community-dwelling older adults in South Korea. The National Survey of Older Koreans is a legally mandated survey conducted every three years in accordance with Article 5 of the Elderly Welfare Act and is designed to comprehensively assess not only health status but also overall living conditions among adults aged 65 years and older nationwide (Kang et al., 2023). The 2023 survey was completed using a stratified sampling design and included 10,178 adults aged 65 years and older from 7,605 households across 977 survey districts. After excluding incomplete or unreliable responses, the final dataset comprised 10,078 participants from 7,556 households, including 123 proxy respondents (Kang et al., 2023). For the present study, the analytic sample was restricted to adults aged 65 years or older who had been diagnosed with at least one chronic disease. Individuals with missing data on any of the main study variables were excluded. After applying these inclusion and exclusion criteria, a total of 8,588 older adults were included in the final analysis (Figure 2).
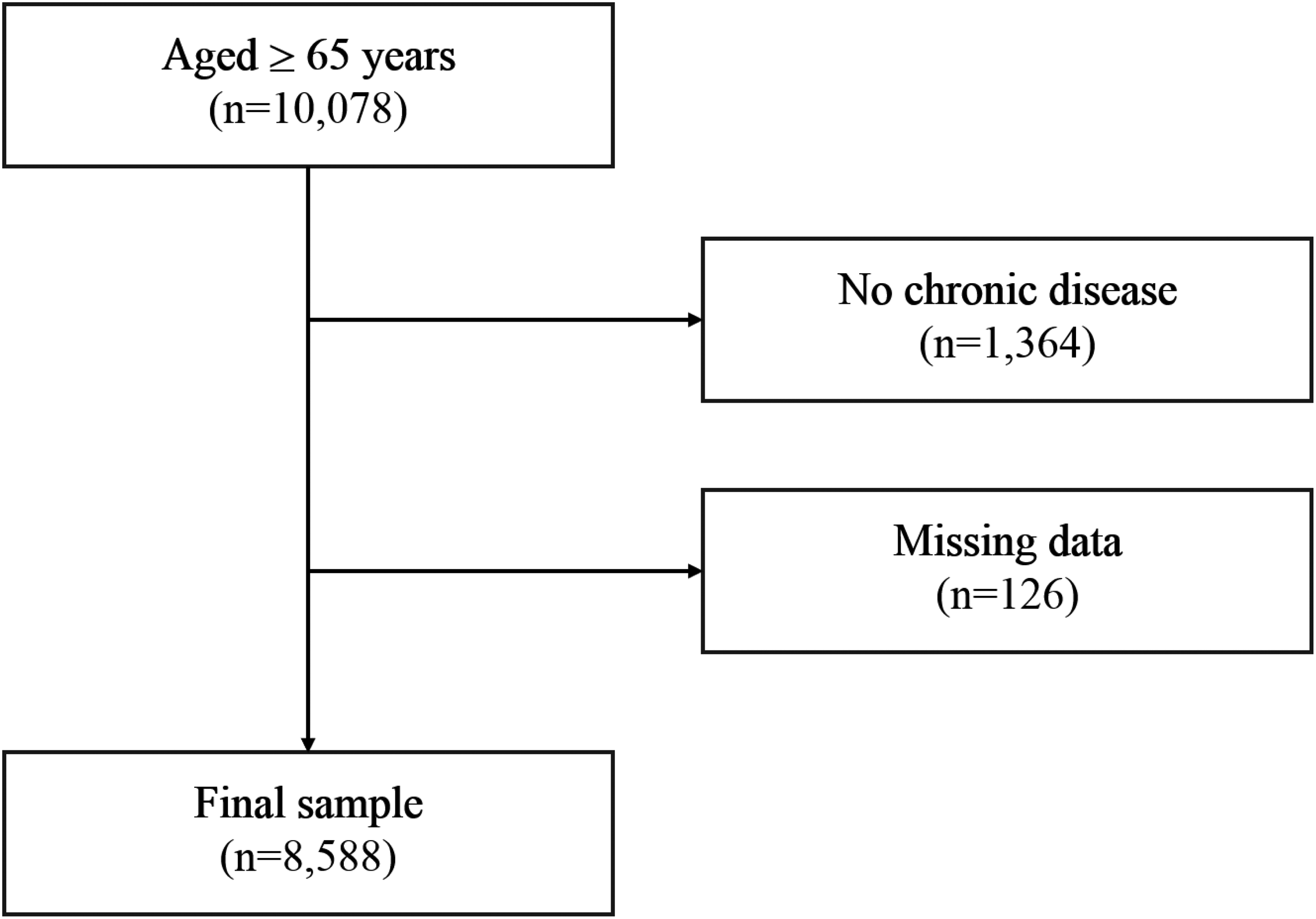
Flow diagram of sample selection.
Measures
Dependent Variable: Depression
Depression was measured using the Short Form of the Korean version of the Geriatric Depression Scale (SGDS-K) included in the National Survey of Older Koreans. The scale consists of 15 dichotomous items, each answered with “yes” or “no.” In this study, affirmative responses indicating the presence of depressive symptoms were coded as 1, and negative responses were coded as 0. Reverse-coded items (items 1, 5, 7, 11, and 13) were recoded accordingly and included in the total score. Total scores ranged from 0 to 15, with higher scores indicating higher levels of depression.
Independent Variable: Digital Literacy
Based on previous studies (Kwon, 2023; Lee & Namgung, 2025), DL was defined as the ability to independently use digital devices such as personal computers, smartphones, tablet PCs, and kiosks, without assistance from others. DL was measured using a 13-item scale derived from the survey question: “Can you perform the following activities using a PC, mobile phone, tablet PC, or kiosk without help from others?” The items assessed various digital activities, including messaging, video calls, and information searching. Each item was coded as 1 (“yes”) and 0 (“no”), and total scores ranged from 0 to 13, with higher scores indicating higher levels of DL.
Moderating Variable: Self-Rated Health
SRH was assessed using the survey question: “How would you rate your usual health status?” Responses were measured on a 5-point Likert scale ranging from 1 (“very poor”) to 5 (“very good”), with higher scores indicating a more positive perception of one's health.
Control Variables
Based on prior research, variables shown to be associated with DL and depression among older adults were included as control variables: gender, age, educational attainment, household income, marital status, activities of daily living (ADL), economic activity status, and life satisfaction. Previous studies have reported higher levels of depression among women, individuals with lower educational attainment, poorer SRH, lower life satisfaction, and those not engaged in economic activity (Park & Yoo, 2023). In addition, higher depression levels have been observed among individuals with reduced ADL, older age, lower household income, and unmarried status (Liu et al., 2023; Song et al., 2025).
Data Analysis
Data analyses were conducted using SPSS version 29.0 (IBM Corp., Armonk, NY, USA). The analytical procedures were as follows:
Descriptive statistics, including means, standard deviations, and percentages, were calculated to summarize participants’ general characteristics and the main variables (DL, depression, and SRH). Pearson correlation analyses were performed to examine the associations among the main variables. Hierarchical regression analyses were conducted to assess the incremental explanatory power of factors influencing depression among older adults. To examine the moderating effect of SRH on the relationship between DL and depression, moderation analysis was performed using the SPSS PROCESS macro (Model 1).
Ethical Considerations
This study was conducted with an exemption approval from the Institutional Review Board (IRB) (IRB No. ewha-202511-0029-01). The analyzed data were stored on a password-protected computer accessible only to the researchers. All research-related data will be retained for three years following the completion of the study and will be permanently destroyed thereafter.
Results
The Sociodemographic Characteristics of the Participants
The sociodemographic characteristics of the participants are presented in Table 1. Of the total sample, 3,253 participants (37.9%) were male and 5,335 (62.1%) were female. Regarding marital status, 4,969 participants (57.9%) reported having a spouse, whereas 3,619 (42.1%) did not. In terms of educational attainment, the largest proportion had completed elementary school (n = 2,652, 30.9%), followed by high school (n = 2,275, 26.5%), middle school (n = 1,850, 21.5%), no formal education (n = 1,347, 15.7%), and college education or higher (n = 464, 5.4%). More than half of the participants were not engaged in economic activity (n = 5,346, 62.2%), while 3,242 participants (37.8%) reported current economic participation. The mean age of the participants was 74.46 years (standard deviation [SD] = 6.74), and the average number of chronic diseases was 2.54 (SD = 1.44). The mean annual household income was 31.35 million KRW (SD = 32.38 million KRW).
The Sociodemographic Characteristics of the Participants (N = 8,588).
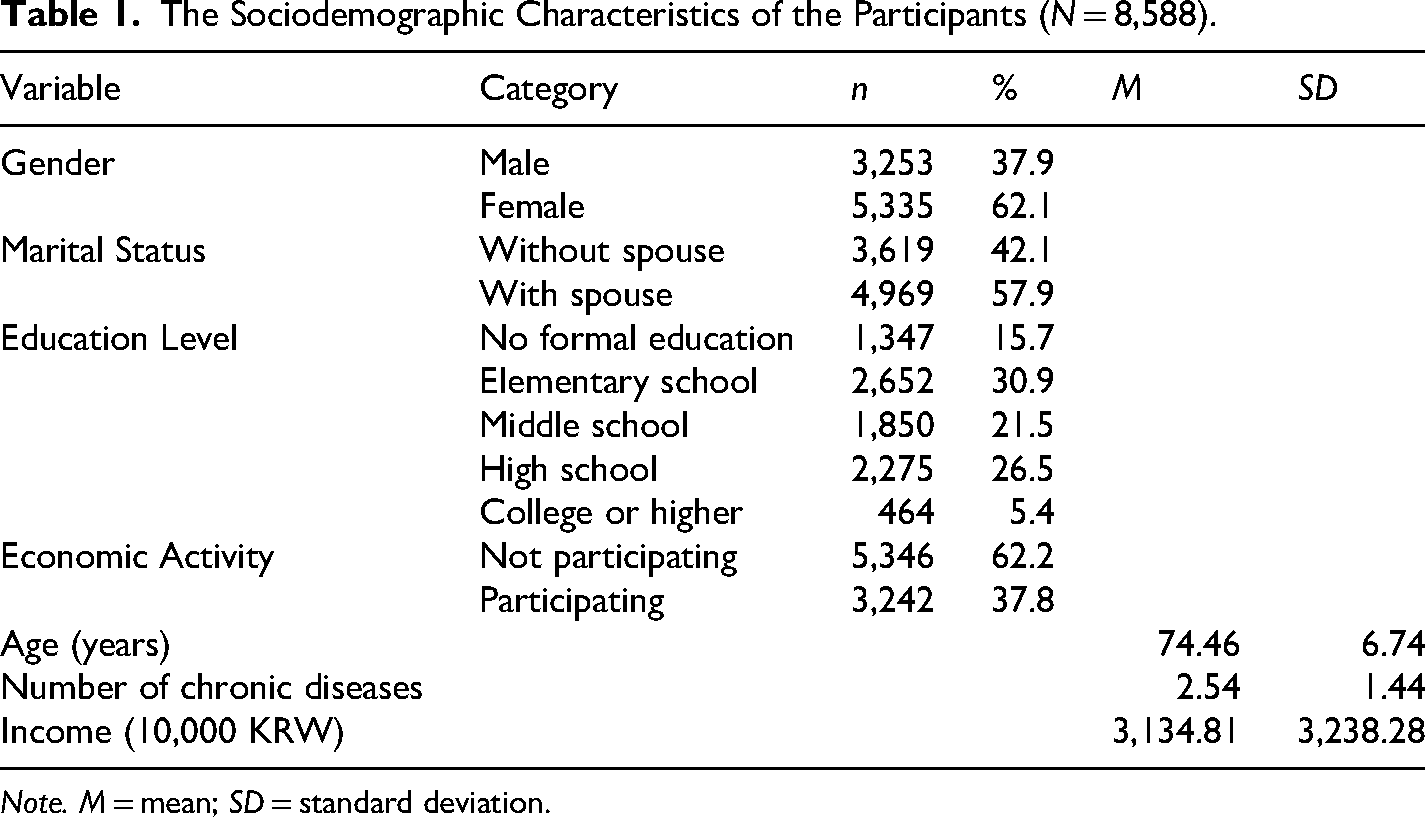
Note. M = mean; SD = standard deviation.
Descriptive Statistics, Reliability, and Correlation Analyses of the Main Variables
Descriptive statistics, reliability, and correlation analyses of the main variables are presented in Table 2. The mean scores were 3.07 (SD = 0.88) for SRH, 4.06 (SD = 3.43) for DL, and 3.34 (SD = 3.30) for depression. The reliability of the measures was high, with Cronbach's alpha values of .840 for depression and .890 for DL. SRH was significantly negatively correlated with depression (r = −.464, p < .001) and positively correlated with DL (r = .393, p < .001). Depression was also negatively correlated with DL (r = −.258, p < .001).
Descriptive Statistics, Reliability, and Correlations Among Main Variables (N = 8,588).
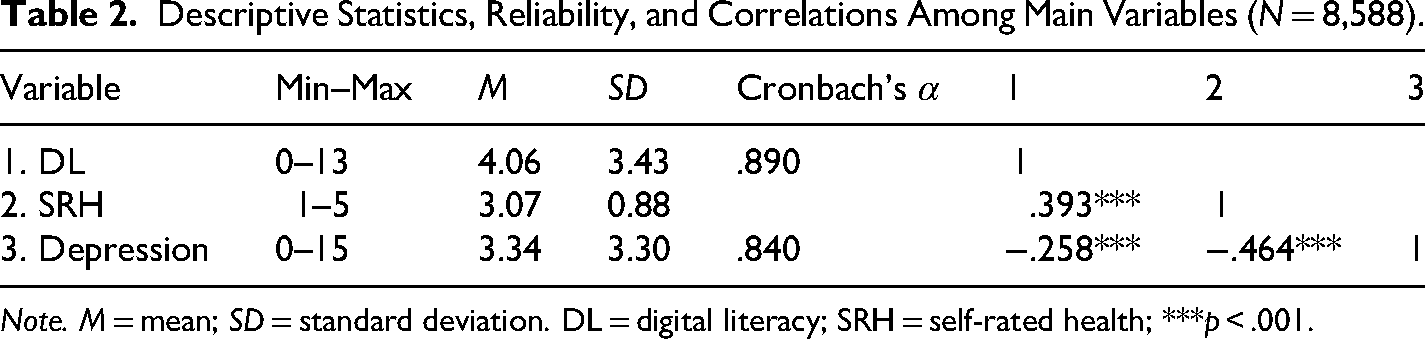
Note. M = mean; SD = standard deviation. DL = digital literacy; SRH = self-rated health; ***p < .001.
Results of the Hierarchical Regression Analysis
Results of the hierarchical regression analysis are shown in Table 3. In Model 1, control variables (gender, age, marital status, education, number of chronic diseases, ADL, economic activity, income, and life satisfaction) explained 34.7% of the variance in depression (R2 = .347). Adding DL in Model 2 significantly increased explanatory power (ΔR2 = .001, F-change = 7.38, p = .007). In Model 3, the inclusion of SRH further increased the explained variance to 36.7% (ΔR2 = .019, F-change = 260.03, p < .001), indicating its independent predictive effect.
Results of the Hierarchical Regression Analysis (N = 8,588).
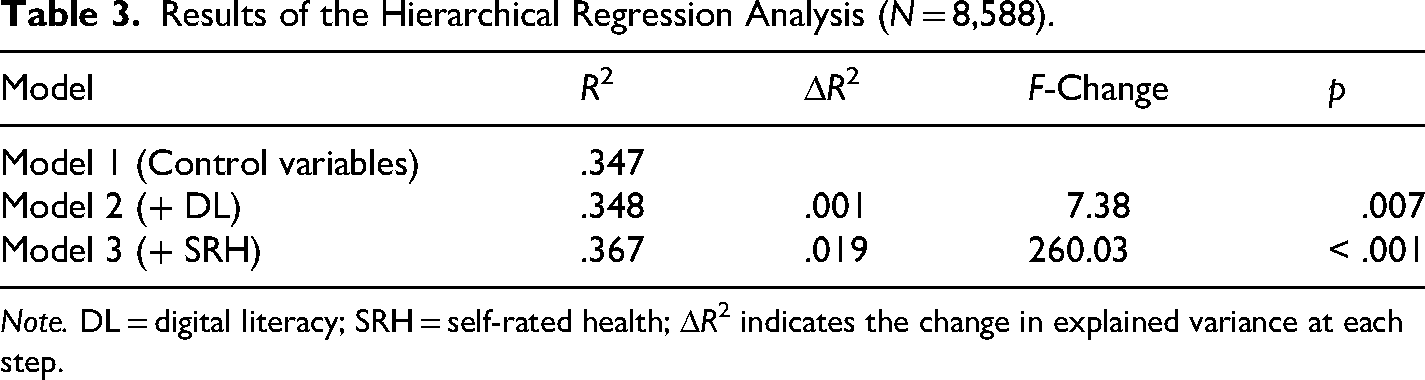
Note. DL = digital literacy; SRH = self-rated health; ΔR2 indicates the change in explained variance at each step.
The Results of the Moderation Analysis
The results of the moderation analysis using the SPSS PROCESS macro (Model 1) are presented in Table 4. Gender, age, marital status, number of chronic diseases, ADL, economic activity, income, life satisfaction, and education were included as covariates. Tolerance values were ≥ .312 and VIF values ranged from 1.123 to 3.207, indicating no multicollinearity. DL had a significant negative effect on depression (β = −0.024, p = .049), and SRH was also a significant predictor (β = −0.654, p < .001). The interaction between DL and SRH was significant (β = 0.032, p = .002), with a 95% bootstrap confidence interval that did not include zero (LLCI = 0.012, ULCI = 0.052), confirming a moderating effect. Among control variables, higher depression levels were observed in males, younger participants, those without a spouse, individuals with more chronic diseases, and those requiring ADL assistance (p < .01). Economic activity and life satisfaction were associated with lower depression levels (p < .001), whereas household income was not significant (p = .799).
The Results of the Moderation Analysis (N = 8,588).
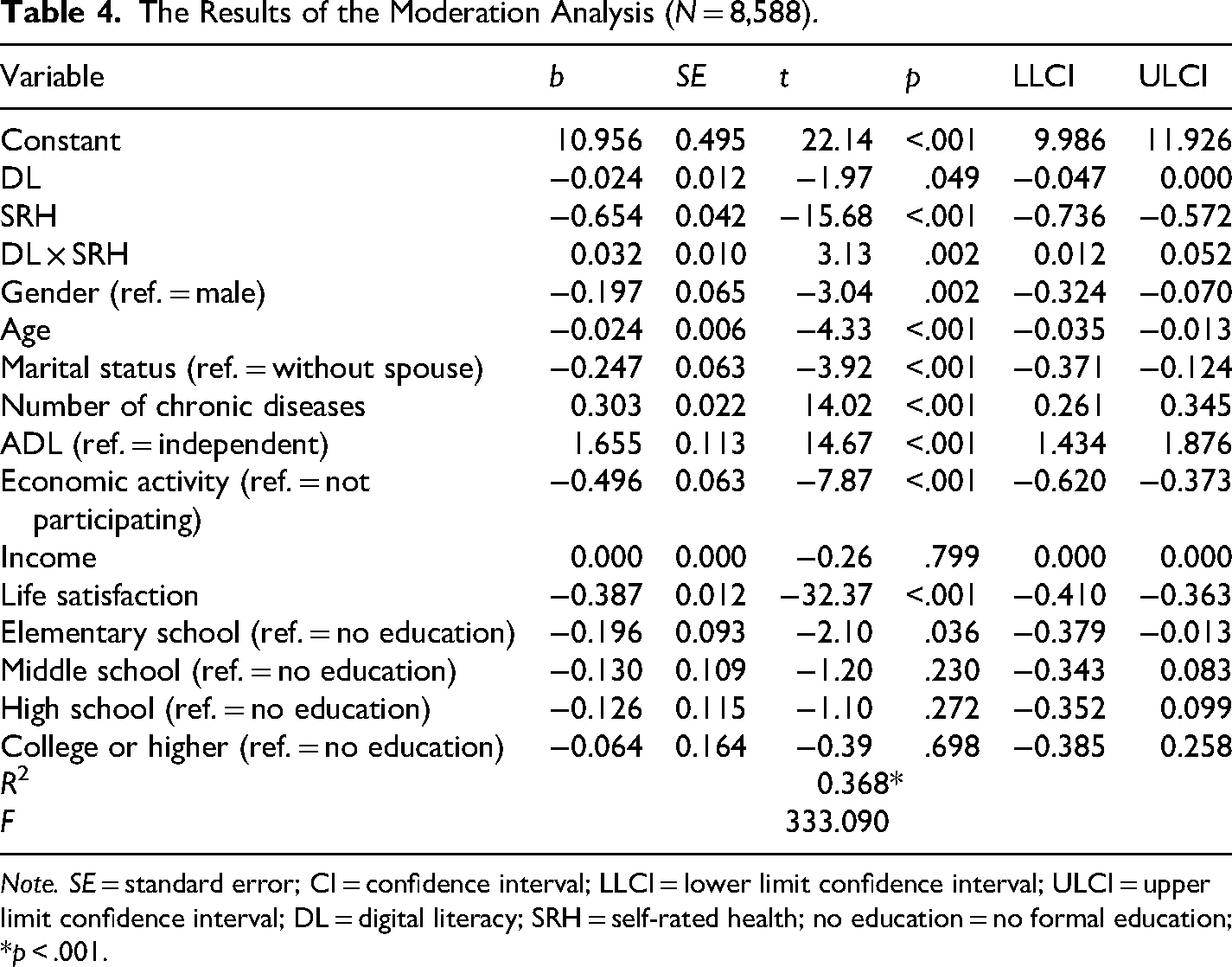
Note. SE = standard error; CI = confidence interval; LLCI = lower limit confidence interval; ULCI = upper limit confidence interval; DL = digital literacy; SRH = self-rated health; no education = no formal education; *p < .001.
Subsequently, the conditional effects of SRH were examined using the pick-a-point approach (mean and ±1 SD). DL was significantly associated with lower depression at low (−1 SD; b = −0.052, p = .002) and mean levels of SRH (b = −0.024, p = .049), but not at high levels (+1 SD; b = 0.005, p = .733). Figure 3 illustrates that depression decreased with increasing DL among individuals with low or average SRH, while no clear association was observed among those with high SRH.
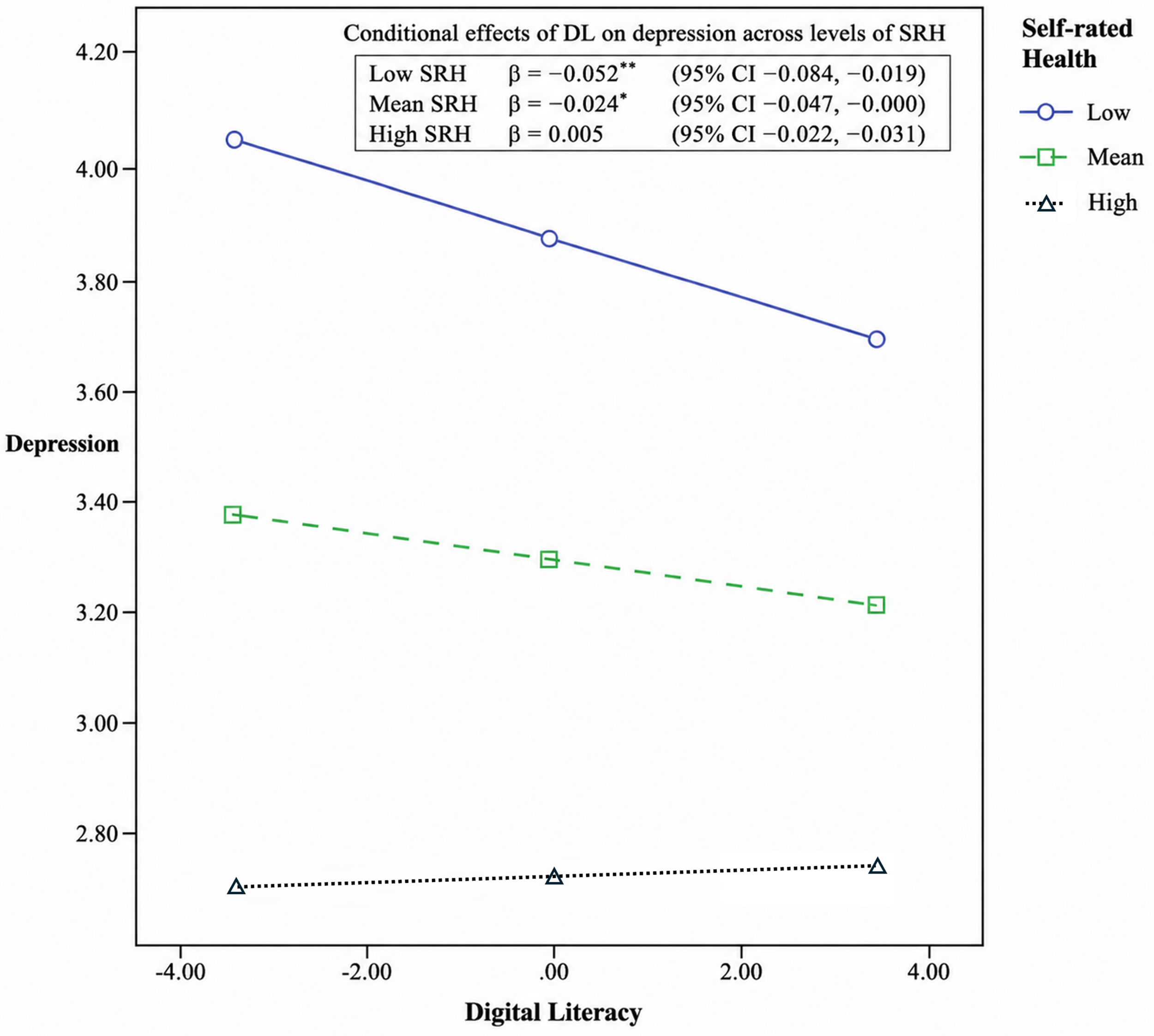
Results of the moderating effect analysis.
Discussion
This study examined the effect of DL on depression among older adults with chronic diseases using nationally representative data from the 2023 National Survey of Older Koreans and tested the moderating role of SRH. The findings showed that higher DL was associated with lower levels of depression, and that this association was significantly moderated by SRH.
The negative association between DL and depression is consistent with previous research (Park & Yoo, 2023; Song et al., 2025) and suggests the potential relevance of DL-enhancing nursing interventions for older adults with chronic diseases. However, these findings should be interpreted with caution. Although DL showed a statistically significant association with depression, its incremental explanatory power was relatively small, suggesting that its substantive contribution to explaining depression may be limited compared with stronger variables such as SRH. In addition, the cross-sectional design does not allow for causal inference, and the observed association may partly reflect reverse causality. Therefore, DL should be interpreted not as a dominant determinant of depression, but as a potentially modifiable correlate that may be relevant within broader psychosocial and health-related contexts. Given the close associations between high levels of depression in older adults and increased risks of persistent physical disability and mortality (Jeong et al., 2022; Roebuck et al., 2023), there is a clear need in clinical and community settings to systematically assess DL and provide standardized, tailored interventions. Such efforts may contribute to improved mental health, overall health outcomes, and quality of life.
In Korea, where digital health services and telemedicine are rapidly expanding (Lee & Kim, 2024), disparities in DL may contribute to health inequalities by restricting access to health information and healthcare services among older adults with chronic diseases. These findings suggest that social, healthcare, and policy-level strategies addressing digital exclusion may be relevant to comprehensive mental health support in later life. However, such implications should be interpreted as preliminary and should be further tested through longitudinal and intervention studies.
SRH emerged as the strongest correlate of depression and a significant moderator of the relationship between DL and depression, consistent with prior studies indicating that the buffering effect of DL varies by individual characteristics (Hegan et al., 2023; Song et al., 2025). According to the CSM, individuals’ emotional responses and self-regulatory behaviors are shaped by their cognitive appraisal of health (Leventhal et al., 2016). When health is perceived as poor, illness threats are appraised more strongly, increasing vulnerability to negative emotions (Paredes et al., 2021). In this context, DL may function as a self-regulatory resource by facilitating health information seeking and access to healthcare, and may be associated with lower levels of depression (Akepaer, 2025).
In the present study, higher DL was associated with lower depression levels among individuals with low or average SRH, with the strongest effect observed among those with poor perceived health. In contrast, no significant association was found among those with high SRH, suggesting that individuals with positive health perceptions may already possess sufficient psychological and functional resources (Jung, 2022; Kong & Zhu, 2025), limiting the additional impact of DL. These findings align with previous research showing that the mental health benefits of digital technology are more pronounced among older adults with greater health limitations or chronic disease burden (Wen & Mejia, 2023; Zhang et al., 2023).
This moderation pattern can be interpreted from a resource substitution perspective. According to this perspective, one resource can compensate for or substitute for another, such that the fewer resources a group possesses, the more strongly other resources are associated with psychological well-being (Ross & Mirowsky, 2006). In this study, DL can be understood as a functional and cognitive resource that is related to individuals’ capacity to effectively cope with various situations. In particular, lower SRH is associated with higher levels of stress and negative affect (Leng et al., 2025). Under such conditions, DL may function as a compensatory resource that offsets limited internal resources, which may explain why DL showed a stronger negative association with depression among individuals with lower SRH.
This interpretation is also consistent with the stress-buffering hypothesis, which posits that psychosocial resources are more effective under conditions of greater stress or vulnerability (Cohen & Wills, 1985). Previous research has shown that higher levels of stress are associated with lower SRH (Lee & Choi, 2025), suggesting that lower SRH may reflect a more negative appraisal of one's health and greater perceived vulnerability, thereby increasing the relevance of coping-related resources. In this context, DL may function as a resource that facilitates access to health information and services, leading to a more pronounced negative association with depression under conditions of greater vulnerability.
Overall, this study provides empirical evidence that the effect of DL on depression among older adults with chronic diseases varies according to SRH. These results suggest that DL interventions should be tailored to vulnerable subgroups, particularly those with poor perceived health, rather than applied uniformly. Targeted interventions may enhance technology acceptance and contribute to improved mental health and quality of life (Batra et al., 2024). Older adults who perceive their health negatively may face compounded disadvantages, including limited access to health information and increased psychological isolation, if they also struggle in digital environments (Kim et al., 2025; Zhao et al., 2022), underscoring the need for stepwise and customized interventions.
This study has several limitations. First, the reliance on self-reported measures of DL, SRH, and depression may have introduced reporting bias, potentially leading to an underestimation of depressive symptoms or an overestimation of DL, which may have attenuated the observed associations. Second, the cross-sectional design precludes causal inference and raises the possibility of reverse causation, whereby lower levels of depression may facilitate greater digital engagement, potentially inflating the observed protective effect of DL. Third, SRH was assessed using a single-item measure, which may not fully capture multidimensional health status and could have introduced measurement imprecision, biasing moderation estimates toward the null. Fourth, DL was operationalized as the ability to perform basic digital tasks independently, which may primarily capture functional skills rather than encompassing the broader and multidimensional nature of DL (van der Vaart & Drossaert, 2017). This may limit the extent to which the findings reflect more advanced cognitive or critical aspects of DL. Regarding generalizability, although the use of nationally representative data supports inference among community-dwelling older adults in Korea, caution is needed when extending these findings to institutionalized populations or to settings with different digital and healthcare environments.
Based on these findings, future research should employ longitudinal designs to clarify causal relationships and examine the long-term protective effects of DL. Qualitative studies are also needed to explore older adults’ lived experiences in digital environments. Finally, the development and evaluation of stepwise, nurse-led, and tailored DL interventions targeting older adults with low SRH are recommended, as such approaches are likely to be effective in both clinical and community settings and to promote mental health and health equity.
Conclusion
This study examined the effect of DL on depression among older adults with chronic diseases using nationally representative data from the 2023 National Survey of Older Koreans and tested the moderating role of SRH. Higher DL was associated with lower depression levels, and this relationship varied by SRH: the negative association was significant among individuals with low or average SRH but not among those with high SRH. These findings provide empirical evidence that the association between DL and depression may differ according to health perceptions. For older adults with chronic diseases who perceive their health status as poor, functional DL may represent a self-regulatory resource that is associated with lower emotional vulnerability, underscoring the need for targeted rather than uniform DL support strategies.
Footnotes
Acknowledgments
The authors would like to express their sincere gratitude to Professor Sung-Hee Bae and Professor Geon-Jeong Lee, Ewha Womans University, for their insightful comments and guidance throughout this research.
Ethical Approval Statement
This study was approved by the Institutional Review Board (IRB) of Ewha Womans University (IRB No. ewha-202511-0029-01).
Patient Consent Statement
Not applicable.
Authors’ Contributions
The concept and design of the study were carried out by Hyein Seo and Subin Yu. The acquisition of subjects and/or data was prepared by Hyein Seo. Data analysis and interpretation were performed by Subin Yu. The manuscript preparation was done by Hyein Seo and Subin Yu.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Clinical Trial Registration
Not applicable.