
Abstract
Background: Our current understanding of tibiofemoral kinematics in the anterior cruciate ligament (ACL)-deficient knee is very limited. Using vertical open-access MRI, it is possible to accurately analyze tibiofemoral motion in patients with isolated rupture of the ACL.
Study: Prospective cohort study.
Purpose: To assess if ACL rupture alters normal knee weightbearing kinematics.
Methods: Tibiofemoral motion was assessed through the arc of flexion from 0 ° to 90 ° in 10 patients with isolated rupture of the ACL in one knee and a normal contralateral knee. Midmedial and midlateral sagittal images were analyzed in all positions of flexion in both knees to assess the tibiofemoral relationship.
Results: In the lateral compartment of the knee, the tibial plateau is persistently subluxed anteriorly throughout the arc of flexion from 0 ° to 90 ° (flexion facet center to posterior tibial cortex distance of 15.8 mm ± 2.9 in ACL-deficient knees compared to 21.4 mm ± 1.4 in normal knees at 0 ° extension, P< .0001) when compared to normal knees. The medial tibiofemoral relationship is unchanged compared to normal knees.
Conclusion: Rupture of the ACL changes tibiofemoral kinematics producing anterior subluxation of the lateral tibial plateau.
Clinical Significance: Altered kinematics may explain, at least in part, the increased incidence of secondary osteoarthritis in patients with ACL rupture.
The anterior cruciate ligament (ACL) is the primary restraint to anterior tibial translation in the knee.10,19,30 Rupture of the ACL leads to excess anteroposterior laxity of the knee and may produce instability. 17 The excess laxity predominantly involves the lateral compartment of the knee with internal rotation of the tibia occurring relative to the femur.28,31 Instability of ACL-deficient knees is manifested by the knee giving way during exercise, which involves “pivoting” or “cutting” reproduced clinically by the pivot-shift test. Cadaveric studies have shown increased anterior tibial translation in the loaded knee throughout flexion.7,41 Unfortunately, in vitro biomechanical studies are unable to accurately simulate the effects of both gravity and muscle contraction on the tibiofemoral articulation.
The kinematics of the in vivo weightbearing ACL-deficient knee are not well understood. Imaging the living weightbearing knee has been a technical challenge. X-rays have been used for weightbearing stress radiography such as the lateral monopodal stance test, which showed increased anterior tibial translation when the patient stood on one leg at 20° of flexion. 14 Almekinders and Chiavetta have also shown increased anterior tibial translation at full extension in the ACL-deficient knee. 1 Beynnon et al have recently used stress radiography to show increased anterior tibial translation from nonweightbearing to weightbearing in patients with rupture of the ACL compared to normal knees. 6 These publications are limited by the difficulty of accurately identifying the superimposed bony landmarks of the medial and lateral sides of the knee on a plain lateral knee radiograph.
We have recently shown that the bony landmarks used in stress radiography lateral knee films to identify the lateral tibial plateau are inaccurate and unable to measure the midmedial and midlateral points of the tibial plateau. 31 Knowledge of the kinematics of the weightbearing ACL-deficient knee is important not only to allow us to understand the short- and long-term effects of this injury but also to improve treatment options. Until recently, MRI has been limited in the study of knee kinematics because the conventional “closed” magnet configuration prevented weightbearing in vivo. To our knowledge, this is the first study to investigate weightbearing tibiofemoral kinematics in both medial and lateral compartments of the ACL-deficient knee using “open-access” MRI from extension to 90° flexion.
Materials and Methods
Consent was obtained from 10 patients (7 men, 3 women) with isolated unilateral rupture of the ACL who were symptomatically unstable and awaiting reconstruction. All had been diagnosed by clinical examination and MRI. Patients were excluded if they had an associated meniscal tear, another ligament injury, a symptomatic contralateral knee, pain at the time of clinical examination, or symptoms in their hip, ankle, or foot. The contralateral normal knee was used as the control by direct comparison. The mean age of the patients was 29 years (range, 25-35 years) with the mean time from injury to performing the MRI scan being 12 months (range, 6 months-3 years). Five of the patients’ injuries were from soccer, 3 from skiing, and the remaining 2 from falling.
MR Scanning
All patients were scanned using the open configuration Signa SP MR Imaging System (General Electric Medical Systems, Milwaukee, Wis). This consists of a 0.5 tesla superconducting magnet with two coils housed in separate but communicating cryostats. The vertical open “double–doughnut” configuration of the scanner allows the patients to stand and progressively squat to 90° flexion (Figure 1). The patients positioned their feet shoulder width apart with the longitudinal axis of the foot in the sagittal plane (neutral rotation). Laser-guided isocenter lines in the sagittal and coronal axes were used to ensure correct positioning of the knee in the center of the magnetic field with the tibia in neutral rotation.
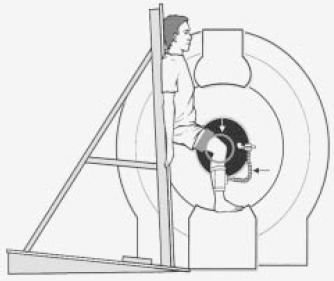
Weightbearing dynamic MRI using an open-access scanner. White arrow, MR coil; black arrow, MR tracker.
Sagittal T1 images (5-mm thick, 0-mm spacing) across the entire knee articulation (approximately 15 images per sequence) were taken with the patient standing and the knee scanned at extension 0°, 20°, 45°, and 90° of flexion (angle measured with a goniometer). This allows both medial and lateral compartments of the knee to be imaged simultaneously and visualized separately. The patients’ contralateral normal knees were also scanned in all positions as a control.
MR Tracking
Assessment of joint motion using MR tracking was first described in 1999 by Pearle et al. 35 The MR signal in an MR tracking procedure is detected by a small radiofrequency coil that is applied around the leg, just below the knee. To provide a signal source, the catheter tip is placed in a small chamber containing copper sulphate for maximum sensitivity. MR signals detected with the coil are sent to the scanner via the miniature coaxial cable embedded in the outer lumen of the catheter. The coil has a limited sensitive volume, and when the received magnetic resonance signal is subjected to frequency analysis, a peak is visualized in the power spectrum. This indicates the location of the coil, and images can then be obtained in reference to this fixed point. Hence, the MR tracking recognition system allowed the same sagittal plane to be imaged regardless of the degree of knee flexion. The sagittal plane is specific to the magnetic field and not to the tibia.
Measurements
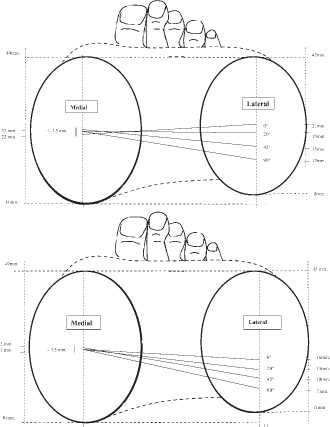
The position of the posterior femoral condyles relative to the tibia was measured in the midmedial and midlateral sagittal sections of the knee according to the method of Iwaki et al. 25 The centers of the posterior circular surfaces of the femoral condyles—the flexion facet centers (FFCs)—were identified by placing acetate overlays with circles of varying diameters over the midmedial and midlateral compartments of the knees on sagittal imaging. The distance between this center and a vertical line drawn from the ipsilateral posterior tibial cortex was measured for each position with a Vernier caliper and corrected for magnification (Figure 2). Changes in this distance between increments of flexion equate to relative motion of the femur on the tibia with flexion. The accuracy of this technique has been shown to be ± 1.5 mm for each measurement.26,34,35

Measurement of the position of the posterior femoral condyles relative to the tibia after Iwaki et al. 25 FFC, flexion facet center; d, distance measured to ipsilateral posterior tibial cortex.
Statistics
The data for normal and ACL-deficient knees had a normal distribution. A post hoc power analysis, with a power of .80 being considered acceptable, confirmed that n = 10 was sufficient for comparison, and the paired Student t test was used to compare the displacements of the normal and ACL-deficient knees. A P value of less than .05 was regarded as statistically significant.
Results
The relative tibiofemoral motion medially and laterally is very different, as our group has previously noted.23,26,37 The measurements of the normal knees in the current study are identical to those of our previous studies of normal knees (Table 1, Figure 3A). Although medially there is negligible relative displacement of the femur on the tibia, laterally the femur progresses posteriorly on the tibia during flexion.
A, The positions of the femoral condyles as given by lines connecting their flexion facet centers at 0° to 90° in the contralateral normal knees. B, The positions of the femoral condyles as given by lines connecting their flexion facet centers at 0° to 90° in the ACL-deficient knees.
Data for Normal Knees: Posterior Tibial Cortex to Flexion Facet Center (mm)
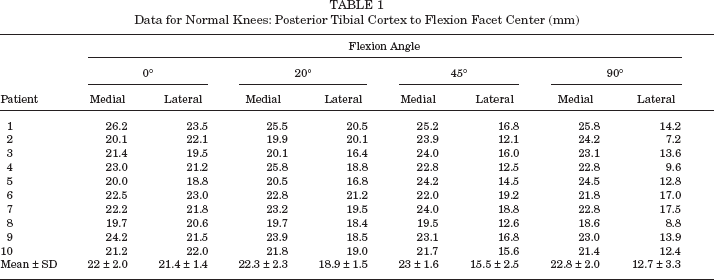
From the data in Tables 1 and 2, there was no statistically significant difference between normal and ACL-deficient knees in medial tibiofemoral motion at any position of flexion (0°, P = .6; 20°, P = .4; 45°, P = .19; 90°, P = .15).
Data for ACL-Deficient Knees: Posterior Tibial Cortex to Flexion Facet Center (mm)
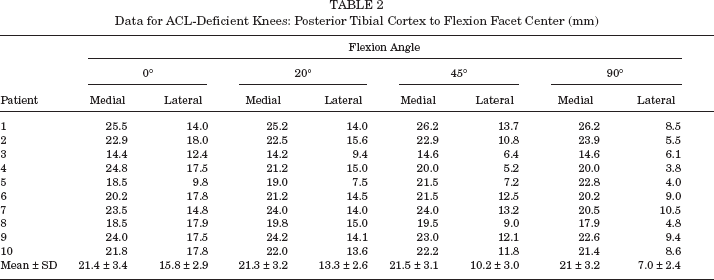
In the lateral compartment, there was no difference between knees in the extent of excursion of the femur posteriorly on the tibia with flexion from 0° to 90°. In the ACL-deficient knees, it was 8.8 mm, and in the normal knees, it was 8.7 mm.
The significant finding was that for every measurement in the lateral compartment in the ACL-deficient knees, the femur was subluxed posteriorly on the tibia compared to the normal knees (Tables 1 and 2, Figures 3 and 4). From the data in Tables 1 and 2, we can see that in the ACL-deficient knees the displacement of the femur posteriorly on the tibia is consistent and statistically significant throughout the arc of flexion (0°, P < .00007, with lateral compartment FFC to posterior tibial cortex means of 15.8 mm ± 2.9 in the ACL-deficient knees compared to 21.4 mm ± 1.4 in the normal knees; 20°, P < .0004, with lateral compartment FFC to posterior tibial cortex means of 13.3 mm ± 2.6 in the ACL-deficient knees compared to 18.9 mm ± 1.5 in the normal knees; 45°, P < .0007, with lateral compartment FFC to posterior tibial cortex means of 10.2 mm ± 3.0 in the ACL-deficient knees compared to 15.5 mm ± 2.5 in the normal knees; 90°, P < .0006, with lateral compartment FFC to posterior tibial cortex means of 7.0 mm ± 2.4 in the ACL-deficient knees compared to 12.7 mm ± 3.3 in the normal knees).
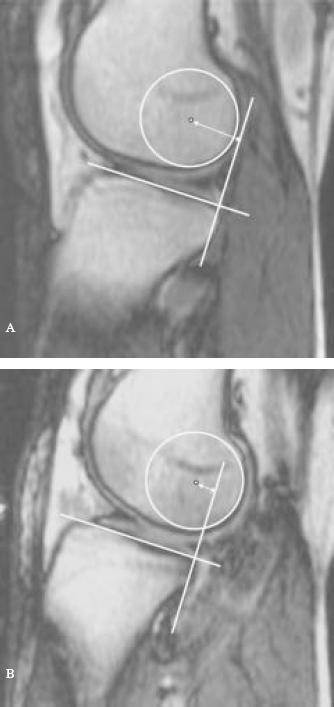
A, Normal tibiofemoral alignment in lateral compartment. B, Tibiofemoral alignment in lateral compartment of ACL-ruptured knee showing anterior tibial translation/posterior femoral translation.
Discussion
There are numerous publications on the increased sagittal laxity of the ACL-deficient knee using radiography, arthrometry, gonylaxometry, and radiostereophotogrammatic analysis [RSA]. † All of these techniques have their limitations with exposure to radiation, invasiveness of the procedure, inability to image the soft tissues, inaccuracy, and poor reproducibility of the methods, among others.
References 3, 10, 14, 15, 18, 19, 21, 22, 24, 26, 28, 29-32, 37-39, 41, 42, 44.
The kinematics of the normal knee have previously been described by our unit.23,25,36,40 Essentially, in the normal knee there is negligible movement in the medial side throughout the flexion-extension arc from hyperextension to 120° flexion. In the lateral side, however, there is progressive posterior translation of the lateral femoral condyle through the flexion arc. The differential mediolateral motion equates to axial rotation: external femoral/internal tibial rotation accompanying knee flexion.
We have recently submitted work on investigating the anteroposterior laxity of the ACL-deficient knee using open-access MRI. 31 The excess sagittal laxity observed in ACL-deficient patients is predominantly in the lateral compartment. This observation, coupled with our findings in the weightbearing ACL-deficient knee, supports the description “anterolateral laxity” with reference to the impact of ACL deficiency.
Positioning of the feet in either internal or external rotation would change the tibiofemoral position in the sagittal plane and alter the results of weightbearing dynamic MRI scans. Great care was therefore taken, with the help of the laser-guided isocenter lines, to ensure a neutral rotation of the tibia while weightbearing in the interventional open magnet.
Our results show that rupture of the ACL, as an isolated injury, does not affect medial compartment kinematics. However, the impact laterally is to allow anterior tibial translation. Coupled with the lack of change in the medial compartment, the ACL-deficient knee therefore achieves a position of greater internal tibial rotation during flexion. This means that, due to external femoral rotation, the lateral femoral condyle approaches the posterior limit of the lateral tibial plateau, thereby facilitating the pivot shift phenomenon, or giving way during activity. It also fits with the characteristic bone-bruise pattern (posterior lateral tibia and midpart of the lateral femoral condyle) on MRI associated with a fresh ACL rupture, which is presumably due to posterior subluxation of the lateral femur on the lateral tibia.20,31,33 In the same way with the relatively posterior position of the lateral femoral condyle, it is easy to predict the increased incidence of lateral meniscal tears, particularly of the posterior horn found with ACL rupture. 5 Our unit has previously shown that the posterior horn of the lateral meniscus is highly mobile with knee flexion. 43 Posterior displacement of the lateral meniscus is a sign of anterior displacement of the tibia and has been recognized as an indirect sign of ACL rupture in nonweightbearing closed-magnet MRI studies.20,33 Abnormal lateral knee kinematics also may explain the increased incidence and unusual pattern of osteoarthritis seen in isolated ACL-deficient knees.13,27
All of the studies, such as ours, that have shown increased anterior tibial translation relative to the femur in the ACL-deficient knee are contradicted by recent invasive RSA studies.8,9 Brandsson et al used tantalum markers inserted percutaneously around the knee to perform RSA in the ACL-deficient knee with the knee flexing from 55° to full extension while ascending a platform. Brandsson et al have controversially suggested that between extension and 55° of flexion, the kinematics of the ACL-deficient knee differ from the normal knee with increased external tibial rotation combined with anterior subluxation of the lateral femoral condyle. 8 These findings are contrary to our study. Indeed, Kärrholm et al 28 have previously suggested that there is increased posterior tibial translation after rupture of the ACL—a finding contrary to published arthrometric, stress radiographic, and MRI studies of the ACL-deficient knee.3,14,18,24,31,39 RSA studies are limited by the exposure to radiation, inability to image the soft tissues, invasive nature of the procedure, and problems with analysis reliability such as those related to the “cross-talk” phenomenon. Open MRI has the great advantage of being noninvasive; there is no restriction to multiple images, no exposure to radiation, and it facilitates weightbearing and accurate visualization of both compartments of the knee separately and simultaneously in a physiological weightbearing mode. A limitation of this study is that we examined the kinematics of a “wall slide” rather than a true unsupported physiological squat, which would have been ideal. It is possible that the results may be different with a true squat, and this would be an interesting topic for future investigation.
Our finding of pathological posterior translation of the lateral femoral condyle in ACL-deficient patients throughout the arc of flexion is important not only for tailoring physiotherapy programs to reduce lateral anterior tibial translation but also for surgical reconstructive techniques to restore normal tibiofemoral kinematics.16,17 This study in conjunction with our previous work implies that for long-term success, both anteroposterior laxity and tibiofemoral axial rotation should be restored when surgical reconstruction is contemplated. There is good evidence that modern ACL reconstructive techniques reduce the excess anteroposterior laxity, but it is not clear if normal kinematics are restored.2,4,9,11,12 We are currently investigating tibiofemoral kinematics following successful ACL reconstruction and assessing if reconstruction restores more normal kinematics.