
Abstract
Despite the high prevalence and potential negative consequences of feeding disorders in children with autism spectrum disorder (ASD), there are surprisingly few studies that examine the efficacy of treatment exclusively with these children. Children with feeding disorders also frequently exhibit packing (holding or pocketing food without swallowing). Investigators have evaluated procedures in the general pediatric population to treat packing, and some have shown that procedures need to be combined to form an effective treatment. Although investigators have evaluated the efficacy of re-distribution, swallow facilitation, and a chaser, these procedures have not been evaluated specifically with children with ASD. Prior to the current investigation, we successfully used nonremoval procedures to increase acceptance of pureed foods and liquids and decrease the inappropriate mealtime behavior of two children diagnosed with ASD and feeding problems; however, in each case, packing emerged during initial treatment. We then used different combinations of re-distribution, swallow facilitation, and chaser treatments to decrease packing for both children.
Autism spectrum disorder (ASD) is a developmental disorder that affects about 1 in 88 children (Centers for Disease Control and Prevention, 2012). Children with ASD often display behavior problems, and feeding disorders are a common behavior problem exhibited by children with ASD. The feeding problems of children with ASD can cause more stress on families than the primary symptoms of ASD because the consequences of feeding problems are often more immediate and salient (Garro, Thurman, Kerwin, & Ducette, 2005).
Schreck, Williams, and Smith (2004) surveyed 472 caregivers of children between 5 and 12 years of age. They found that 72% of children diagnosed with ASD had feeding problems, which was significantly higher than same-aged peers without ASD. Children with ASD ate significantly fewer foods from all food groups, consuming approximately half the dairy, fruits, proteins, and vegetables consumed by children without ASD. Note that Schreck et al. interviewed families of children up to age 12, suggesting that children with ASD do not “grow out of” feeding problems. Zimmer et al. (2012) analyzed the extent to which children with ASD and a feeding disorder had nutritional deficiencies. They reported that children with ASD and a feeding disorder were at significant risk of at least one nutrient deficiency (e.g., protein, calcium, Vitamin B12, Vitamin D). Taken together, these data suggest that the prevalence of feeding disorders among children with ASD is high and may place these children at risk of nutritional deficiencies. A child who does not consume adequate nutrition may be at increased risk of learning and behavior problems (Volkert & Piazza, 2012). Children with ASD already experience social and communication deficits and this would be extremely harmful to their development if their feeding problem is left untreated.
There are several studies that have shown that behavior-analytic based treatments for the feeding problems of children with ASD are effective for improving the feeding behavior of children with ASD. For example, Najdowski et al. (2010) taught the parents of three children with ASD to implement a feeding treatment consisting of differential reinforcement of alternative behavior (i.e., highly preferred foods for acceptance of nonpreferred foods), nonremoval of the spoon, and bite fading, which resulted in high levels of acceptance and low levels of consumption initially. Although consumption increased after a change from differential reinforcement of acceptance to differential reinforcement of consumption, the authors did not demonstrate functional control of the differential reinforcement contingency change. Najdowski, Wallace, Doney, and Ghezzi (2003) used a similar procedure to increase the variety of one 5-year-old boy with ASD. When consumption remained low during initial meals, the authors included re-presentation in the treatment package. However, the authors did not evaluate the contribution of re-presentation to treatment efficacy. Finally, Sharp and Jaquess (2009) evaluated the effects of texture manipulations on the levels of mouth clean, inappropriate behavior, expulsion, and gagging of one 3-year-old boy with ASD. Levels of mouth clean, a product measure of swallowing in which the feeder looks into the child’s mouth to determine whether the child has swallowed an accepted bite, were lower and rates of expulsion and gagging were higher as texture increased beyond puree. The authors used a texture-fading procedure as treatment, but they did not demonstrate control for the texture-fading procedure.
In the studies by Najdowski et al. (2003), Najdowski et al. (2010), and Sharp and Jaquess (2009), problematic mealtime behavior emerged during treatment in that the participants did not consistently consume presented bites, instead, they either expelled (spit out) or packed (held food in the mouth without swallowing) bites. Although consumption improved during treatment, none of the studies demonstrated functional control over the procedures used to promote consumption (e.g., reduce packing).
Packing is a problematic mealtime behavior characterized by pocketing or holding food in the oral cavity without swallowing (Vaz, Piazza, Stewart, Volkert, & Groff, 2012). The criterion volume for packing typically exceeds a pea or grain of rice amount of food present in the mouth (see Buckley & Newchok, 2005; Gulotta, Piazza, Patel, & Layer, 2005; Sevin, Gulotta, Sierp, Rosica, & Miller, 2002; Vaz et al., 2012). Packing poses significant health concerns in that the individual is at risk of aspiration as well as decreased caloric intake (Gulotta et al., 2005). Investigators have evaluated procedures in the general pediatric population to treat packing. In one notable exception, Buckley and Newchok (2005) determined that simultaneous presentation was the active element of a treatment package also consisting of differential reinforcement with response cost to reduce packing in one child with ASD. Simultaneous presentation involved the presentation of a highly preferred food (i.e., chocolate cookie) on the spoon behind a bite of a table food the child packed. Gulotta and colleagues (2005) showed that the packing of four children decreased when the therapist used re-distribution. Re-distribution consisted of removing packed food from the child’s mouth and placing it on the child’s tongue. Lamm and Greer (1988) used a “light touch” (p. 155) across the posterior of the child’s tongue to facilitate swallowing, and Hoch, Babbitt, Coe, Duncan, and Trusty (1995) gently pressed and lightly dragged a rubber oral stimulator forward on participants’ tongues to achieve similar results. Vaz et al. (2012) used a chaser, a liquid, or a solid that the child swallowed consistently, to reduce the packing of three children. Re-distribution, swallow facilitation, and chaser procedures may compensate for poor oral-motor skills by aiding with bolus formation or propulsion, which are necessary behaviors for swallowing (Vaz et al., 2012). Although investigators have evaluated the efficacy of re-distribution, swallow facilitation, and a chaser, these procedures have not been evaluated specifically with children with ASD.
In some cases, investigators have shown that procedures need to be combined to form an effective treatment. For example, Volkert, Vaz, Piazza, Frese, and Barnett (2011) combined re-distribution and swallow facilitation with a flipped spoon to reduce packing. During treatment, the therapist removed packed food from the child’s mouth with a spoon. The therapist then inserted the spoon with food into the child’s mouth, turned the spoon 180°, placed the spoon on the back center of the tongue, and dragged the bowl of the spoon along the tongue toward the lips to deposit the food on the child’s tongue. Sharp, Odom, and Jaquess (2012) used a combination of nonremoval of the spoon, flipped spoon presentation and re-presentation, and reinforcement to decrease expulsion and increase mouth clean. During treatment, the therapist used a similar procedure to the flipped spoon described by Volkert et al., but the therapist placed the food onto the middle of the child’s tongue. These and other studies (e.g., Dempsey, Piazza, Groff, & Kozisek, 2011; Rivas, Piazza, Kadey, Volkert, & Stewart, 2011) suggest that complex feeding problems may require multi-component treatments to achieve efficacy.
Prior to the current investigation, we successfully used nonremoval procedures to increase the acceptance of pureed foods and liquids and to decrease the inappropriate mealtime behavior of two children diagnosed with ASD and feeding problems. Similar to participants in Najdowski et al. (2010), Najdowski et al. (2003), and Sharp and Jaquess (2009), problematic behavior, in this case in the form of packing, emerged during initial treatment. We evaluated a variety of treatments for packing prior to this investigation. We suspected that both participants in the current study had oral-motor skill deficits, and it is possible that these initial treatments in isolation did not effectively compensate for these deficits. We presented a decreased texture and a chaser to both children. With Nick, we also evaluated a flipped spoon on presentation and a decreased bolus size. For Cara, we evaluated blending, re-distribution, and swallow facilitation with a flipped spoon, and re-distribution and swallow facilitation with a nuk. None of these interventions were effective for either child. In light of these findings, we used different combinations of re-distribution, swallow facilitation, and chaser treatments to decrease packing for both children.
Method
Participants
Nick and Cara were 4 years of age and were admitted to an outpatient (Nick) or day-treatment (Cara) feeding disorders program. Both children were diagnosed with ASD. Nick received an ASD diagnosis from a licensed psychologist with expertise in diagnosis and treatment of ASD. A clinician with a master’s degree and expertise in diagnosing ASD administered the Child Development Inventory (Ireton, 1992), which indicated that Nick had speech, language, and gross/fine motor delays. Nick’s medical history included failure to thrive, prematurity, milk–soy protein intolerance, food allergies, gastroesophageal reflux, and vomiting. He received these medical diagnoses via his pediatrician or gastroenterologist prior to his admission to the program. Nick received Omeprazole and Reglan to manage his gastroesophageal reflux. He received more than 90% of his calories via gastrostomy tube. Nick consumed 4 to 5 ounces of water or juice and small amounts (i.e., 5 to 10, 1-cc bites) of chicken stars soup. He also accepted corn puffs, popcorn, Ritz crackers, and chips and held the food in his mouth until it dissolved. Cara was diagnosed with ASD by history. Cara also received a diagnosis of dysphasia from a speech language pathologist, and her IQ was in the average range per a Wechsler Preschool and Primary Scale of Intelligence–Third Edition (Wechsler, 2002). She also followed a gluten-free casein-free diet to address her ASD symptoms. Cara received approximately 50% of her needs at the time of her evaluation through consumption of vanilla rice milk and pear juice and a limited variety of Stages 2 and 3 baby foods such as peach cobbler, vegetable beef, organic applesauce, banana strawberry, and turkey and rice. An interdisciplinary team, which included a licensed psychologist, dietician, speech pathologist, and gastroenterologist, determined that both children were safe for oral feeding and the treatments described below.
Setting and Materials
Feeders and all observers were trained in applied behavior analysis and held a minimum of a bachelor’s degree. A licensed psychologist who was also a board certified behavior analyst supervised the feeders. Treatment occurred in a feeding disorders clinic at a major medical center in the Midwestern United States. Feeders conducted one meal per week for 1 hr with Nick. Feeders conducted two to five meals per day for 30 to 45 min per meal for Cara with at least 1 hr between the start of each meal (e.g., 9:00 am, 10:30 am). Each meal consisted of multiple five-bite sessions with brief breaks between sessions conducted in therapy rooms with one-way observation and sound. Feeders presented a level bolus of pureed canned garbanzo beans on a rubber-coated baby spoon to Nick (purees), one 0.6-cm × 0.6-cm masticated piece of Tyson grilled chicken breast on a rubber-coated baby spoon to Nick (table texture), and a level bolus of either frozen corn or frozen broccoli (one food per session) pureed with a Magic Bullet food processor on a small maroon spoon to Cara.
Interobserver Agreement
Two observers simultaneously but independently collected data on packing during 50%, 59%, and 35% of sessions for Nick (purees), Nick (table food), and Cara, respectively. We calculated interobserver agreement by summing occurrence (both observers scored the behavior) and nonoccurrence (both observers did not score the behavior) agreements; dividing by the sum of occurrence agreements, nonoccurrence agreements, and disagreements (one observer scored and the other observer did not score the behavior); and converting this ratio to a percentage. Mean interobserver agreement for packing, including caregiver training and follow-up, was 99% (range, 93% to 100%) for Nick (purees), 99% (range, 85% to 100%) for Nick (table texture), and 99% (range, 92% to 100%) for Cara.
Experimental Design
For Nick (purees), we used an ABCDAD design in which we added re-distribution (B) to nonremoval of the spoon (A); followed by nonremoval of the spoon, re-distribution, and swallow facilitation (C); followed by nonremoval of the spoon, re-distribution, swallow facilitation, and chaser (D). For Nick (table food), we used an ABCBCDEDE design in which we added a chaser (B) to nonremoval of the flipped spoon (A); followed by nonremoval of the flipped spoon, chaser, re-distribution, and swallow facilitation (C); nonremoval of the upright spoon, chaser, re-distribution, and swallow facilitation with a 0.6-cm × 0.6-cm bite (D); and nonremoval of the upright spoon and chaser with a 0.6-cm × 0.6-cm bite (E). For Cara, we used an ABAB design in which we added re-distribution, swallow facilitation, and chaser to nonremoval of the spoon.
General Procedure and Dependent Variables
The feeder presented bites approximately every 30 to 45 s by touching the utensil to the child’s lips while saying “Take a bite.” The feeder provided praise to Nick and Cara for accepting the bite within 5 s of presentation. If the child did not accept the bite within 5 s, the feeder held the utensil at the lips until the child opened his or her mouth such that the feeder could deposit the bite. The feeder prompted the child to “Show me” 30 s after the bite entered the child’s mouth. The feeder inserted a rubber-coated baby spoon into the mouth and rotated it 90° to prompt the child to open his or her mouth if the child did not open in response to the vocal prompt. If the child had no food in the mouth larger than a pea (Nick, purees, and Cara) or grain of rice (Nick, table texture) at the check, and the absence of food was not due to expulsion, the feeder provided praise, and the observer scored mouth clean. We modified the definition of mouth clean for Nick (table texture) to account for the small size of the presented bite. If the child had food in the mouth larger than a pea (Nick, purees, and Cara) or grain of rice (Nick, table texture) at the check, the feeder said “Swallow your bite,” and observers scored pack. Observers had five potential opportunities to score mouth clean or pack, which corresponded to one potential scoring opportunity for each of the five-bite presentations. For the first four bite presentations per session, the feeder presented the next bite after the mouth check, regardless of whether the child packed the bite. If the child packed the fifth bite, the observer scored pack at the check. The feeder then conducted additional checks every 30 s until the child swallowed the final bite or 10 min elapsed from session onset (Nick, purees and table texture) or 2 min elapsed from the mouth check of the fifth bite (Cara), but observers did not score mouth clean or pack for these subsequent checks. If the child had food in his or her mouth after the termination of the session, the feeder removed it. The feeder provided no differential consequence for inappropriate behavior (i.e., the feeder ignored all inappropriate mealtime behavior, and the bite remained at the child’s lips until the feeder could deposit it). Nick (purees) and Cara did not expel during the assessments. Nick expelled one bite in Session 18 of the table-texture assessment, and the feeder re-presented it. Nick swallowed that bite before the expiration of the 30-s interval.
Nick Purees
We increased acceptance of 12 pureed foods (i.e., canned peaches, canned pears, bananas, canned green beans, frozen French fries, canned sweet potatoes, minute rice, soy pudding, canned carrots, frozen waffles, canned peas, and crackers) selected by Nick’s mother using nonremoval of the spoon and noncontingent reinforcement. However, Nick frequently packed starches and peas. We attempted to treat packing with these foods using a variety of interventions as described above but were unsuccessful. Given Nick’s history of treatment with these foods, we initiated the treatment analysis with a single, pureed food that he did not have a history of consuming (i.e., canned garbanzo beans).
Nonremoval of the spoon
The feeder implemented the general procedure. In addition, the feeder provided continuous attention and access to toys identified via a choice assessment (Fisher et al., 1992).
Nonremoval of the spoon and re-distribution
The feeder implemented the general procedure. In addition, the feeder conducted an additional (i.e., in addition to the check at 30 s) mouth check 15 s after the bite entered Nick’s mouth and provided praise for mouth clean or conducted re-distribution if food larger than the size of a pea was visible in his mouth. During re-distribution, the feeder used the nonremoval procedure to (a) remove packed food from Nick’s mouth with a nuk, (b) insert the nuk with food back into Nick’s mouth, (c) place the nuk onto his mid-tongue, and (d) rotate the nuk 180° while dragging it toward the lips. After praise or re-distribution at the 15-s check, the feeder activated the timer for 15 s. At the 30-s check, the feeder implemented praise for mouth clean or re-distribution for pack and presented the next bite. The observer scored mouth clean or pack only at the 30-s check as described in the general procedure. If Nick packed the fifth bite, the feeder continued checking his mouth every 15 s and implemented re-distribution until he swallowed the bite or 10 min elapsed from session onset.
Nonremoval of the spoon, re-distribution, and swallow facilitation
The procedure was identical to re-distribution except the feeder deposited the packed food he or she removed from the mouth onto the posterior of the tongue and applied slight pressure while dragging the nuk toward the lips.
Nonremoval of the spoon, re-distribution, swallow facilitation, and chaser
The feeder implemented nonremoval of the spoon, re-distribution, and swallow facilitation as described above. The chaser was 4 cc of Neocate Jr. (milk-like thickness) in a pink flexi cup. We demonstrated that Nick accepted and swallowed Neocate Jr. on 91% of presentations in a treatment assessment conducted prior to this study, so we selected this liquid as the chaser. Immediately after the bite entered Nick’s mouth, the feeder touched the cup with the chaser to Nick’s lips while saying, “Take a drink.” The feeder kept the cup at Nick’s lips until Nick opened his mouth, and the feeder could deposit the drink (nonremoval of the cup). The feeder presented one chaser for each bite presentation, with a potential maximum of five chaser presentations, corresponding to one chaser presentation after each of the five-bite presentations. The feeder activated the 15-s timer as soon as the entire bite entered Nick’s mouth and implemented praise or re-distribution and swallow facilitation at the 15- and 30-s checks as described above.
After we established functional control of the treatment using garbanzo beans according to caregiver preference, the feeder introduced peas, sweet potatoes, and canned refried beans at a puree texture, beginning with Session 41. The feeder presented one food in each session. We trained Nick’s mother and nanny to implement treatment starting at Sessions 68 and 71, respectively, through Session 83. Approximately 1 month after training with Nick’s caregivers and implementation of the treatment package in the home, we observed Nick’s nanny conduct the treatment at the clinic (Session 84).
Nick Table Food
After increasing consumption of purees, the feeders taught Nick to chew table foods (i.e., canned peach, canned green bean, and Tyson grilled chicken breast), which he packed. Nick had the most difficulty swallowing masticated chicken so we selected this food for the current analysis. The focus of this study is on packing; therefore, we provide a brief overview of the chewing procedure, with the primary focus on the packing treatment. (Contact the author for chewing-treatment details and see Volkert, Peterson, Zeleny, & Piazza, 2014). The feeder used nonremoval of the tube to present Nick with a 0.6-cm × 0.6-cm piece of chicken inside an approximately 5.1-cm length of clear, flexible aquarium airline tubing that was 0.6 cm in diameter. The feeder inserted the tube into Nick’s mouth between the molars and prompted him to “chew” using least to most prompting (verbal, gestural, and physical guidance). Once Nick masticated the piece of food in the tube to a pulp-like consistency, the feeder removed the food from the tube, placed it on the rubber-coated baby spoon, and began the treatments described below.
Nonremoval with the flipped spoon
The feeder used the general procedure to present bites of masticated chicken with a flipped spoon. The feeder inserted the upright spoon with the masticated bite of chicken into Nick’s mouth, turned the spoon 180°, placed the spoon on the center of the tongue, and dragged the bowl of the spoon along the tongue toward the lips.
Nonremoval with the flipped spoon and chaser
The feeder implemented nonremoval with the flipped spoon and the chaser described above. The feeder increased the chaser to 8 cc at Session 7 to evaluate whether a larger bolus would be more effective.
Nonremoval with the flipped spoon, chaser, re-distribution, and swallow facilitation
The feeder implemented nonremoval with the flipped spoon and used the 8-cc chaser. The procedure for re-distribution and swallow facilitation with the nuk was identical to that for puree.
Nonremoval with the flipped spoon, chaser, re-distribution, and swallow facilitation (strip, no chew tube)
Once we established experimental control of the treatment package for packing, we advanced chewing by presenting chicken strips (0.6 cm × 0.6 cm × 5.1 cm) without a chew tube. The feeder used nonremoval of the strip to place the strip of chicken between Nick’s molars. The chew prompting was identical to that described above. The feeder removed the bite from Nick’s mouth once masticated and implemented the flipped spoon, chaser, re-distribution, and swallow facilitation treatment with the masticated bite.
Nonremoval with the flipped spoon, chaser, re-distribution, and swallow facilitation (0.6-cm × 0.6-cm bite, no chew tube)
Once Nick consistently chewed and swallowed the strip, we re-introduced the 0.6-cm × 0.6-cm pieces of chicken to Nick without the chew tube. The feeder used nonremoval of the upright baby spoon to present one 0.6-cm × 0.6-cm bite of chicken and prompted Nick to chew as described above. The feeder removed the bite from Nick’s mouth once masticated and implemented the flipped spoon, chaser, re-distribution, and swallow facilitation treatment with the masticated bite.
Nonremoval with the upright spoon, chaser, re-distribution, and swallow facilitation (0.6-cm × 0.6-cm bite, no chew tube)
The treatment sequence was identical to the nonremoval with the flipped spoon, chaser, re-distribution, and swallow facilitation (0.6-cm × 0.6-cm bite, no chew tube), except that the feeder used an upright, rather than a flipped spoon. That is, once Nick masticated the chicken, the feeder removed the masticated bite from Nick’s mouth and used nonremoval of an upright baby spoon to present the masticated bite.
Nonremoval with the upright spoon and chaser (0.6-cm × 0.6-cm bite, no chew tube)
Once Nick masticated the 0.6-cm × 0.6-cm bite of chicken, the feeder removed the bite from his mouth. The feeder used nonremoval of an upright spoon to present the masticated bite of chicken. Once the entire bite entered Nick’s mouth, the feeder activated the 30-s mouth-check timer and presented the 8-cc chaser as described previously. We no longer conducted the 15-s mouth check.
When we removed the re-distribution and swallow facilitation components from the treatment package, Nick’s packing increased. We then reinstated the chaser, re-distribution, and swallow facilitation treatment, and packing decreased to 0%. Therefore, we trained Nick’s nanny and mother at the clinic to implement nonremoval of an upright spoon, re-distribution, and swallow facilitation with the 0.6-cm × 0.6-cm bite and no chew tube as described above beginning at Sessions 51 and 53, respectively. At the clinic, we conducted follow-up 4 and 6 weeks following training with Nick’s mother serving as the feeder. During these appointments, we again discontinued re-distribution and swallow facilitation and only used the chaser as described above.
Cara
After we increased acceptance of 16 pureed foods chosen by her parents using nonremoval of the spoon, we performed a brief assessment in which we presented each of the foods singly during a five-bite session to identify the target foods for the packing treatment. Results of this assessment indicated that Cara engaged in high levels (>60%) of packing with 9 pureed foods (i.e., frozen corn, frozen broccoli, canned black-eyed peas, wheat- and gluten-free bread, frozen peas, frozen lima beans, canned Vienna sausage, canned pineapple, and eggs). As previously noted, we were not able to decrease Cara’s packing after implementing several interventions and she had the most difficulty with corn and broccoli; thus, we selected these foods for the current analysis.
Nonremoval of the spoon
The feeder implemented the general procedure.
Nonremoval of the spoon, re-distribution, swallow facilitation, and chaser
The feeder implemented nonremoval, re-distribution, and swallow facilitation with the flipped spoon, and the chaser as described for Nick (purees). The chaser was 8 cc of water in a flexi-cut cup. Water was a preferred liquid that we observed Cara readily consume on a daily basis outside of the structured sessions. Although we increased her consumption of Bright Beginnings during her day-treatment admission, we felt that this liquid was very calorically dense and we were concerned that she would receive too many calories too quickly given the volume of the chaser. The re-distribution and swallow facilitation were as described for Nick except that after the feeder removed the food from her mouth, he or she inserted the upright spoon with the food into Cara’s mouth, turned the spoon 180°, placed the spoon on the center of the tongue, and applied pressure to the spoon while dragging the bowl of the spoon along the tongue toward the lips. In addition, if Cara packed the fifth bite, the feeder continued checking her mouth every 15 s and implemented re-distribution and swallow facilitation until she swallowed or 2 min elapsed following the mouth check of the fifth bite.
Once we established experimental control of the treatment package with corn and broccoli, we introduced black-eyed peas, bread, peas, lima beans, Vienna sausage, pineapple, and eggs pureed with a Magic Bullet food processor. The feeder rotated between the four foods within a five-bite session. We then trained Cara’s mother and father at the clinic. In clinic, we also conducted follow up 2, 4, and 6 months after her discharge from the day-treatment program.
Results
Percentage of packing for Nick (purees, Figure 1) was high and variable during baseline (M = 85%; range, 40% to 100%) and remained high and variable during re-distribution (M = 84%; range, 60% to 100%). Although packing decreased when we added swallow facilitation, it remained at 50% (range, 20% to 80%). When we added the chaser, packing immediately decreased to and maintained at 0%, and we replicated this effect when we repeated this treatment package following baseline conditions (M = 3%; range, 0% to 40%). Packing remained low, even after we added new foods. Percentage of packing remained at zero or low levels with Nick’s mother and nanny, respectively, feeding. Packing was 0 at 1-month follow-up.
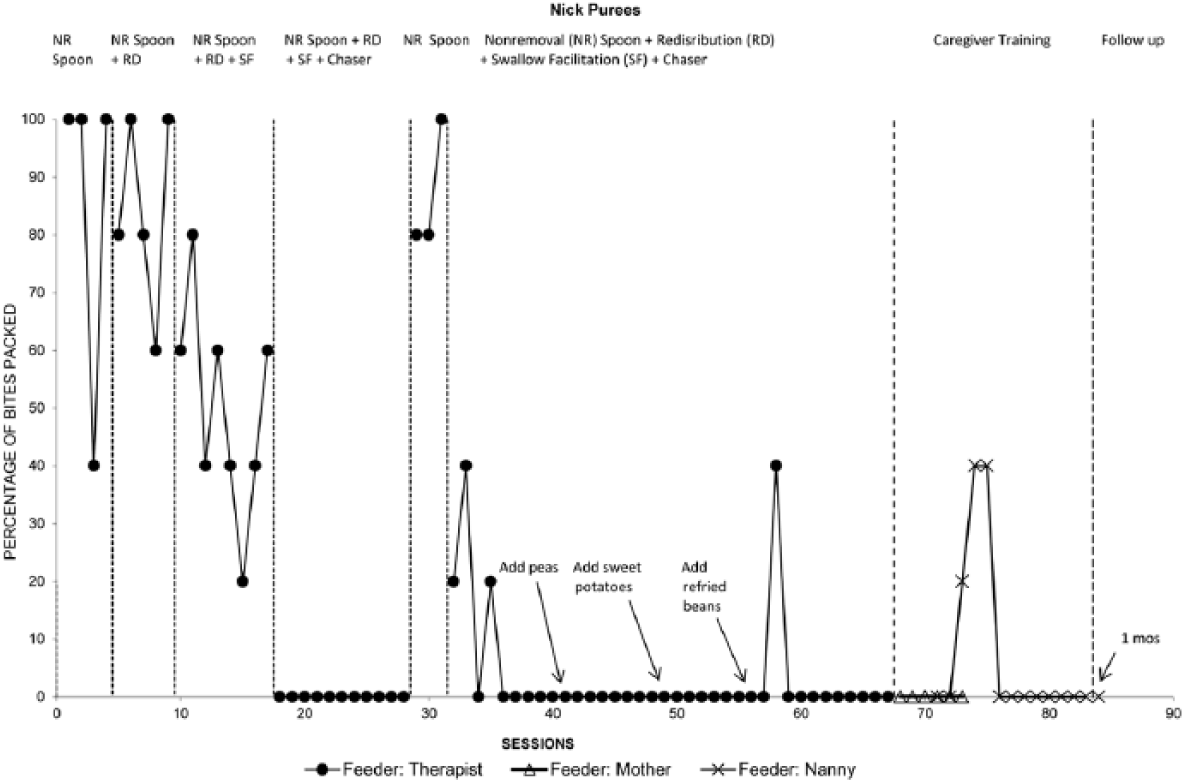
Percentage of bites packed for Nick with purees.
Percentage of packing for Nick (table texture, Figure 2) was high and stable during baseline (M = 87%; range, 80% to 100%). Although packing decreased when we added a chaser, it remained at clinically unacceptable levels (M = 73%; range, 20% to 100%). Packing decreased when we added re-distribution and swallow facilitation (M = 24%; range, 0% to 60%), and we replicated this effect during a reversal. Removal of distribution and swallow facilitation (i.e., chaser only) resulted in an increase in packing (M = 37%; range, 20% to 60%). We observed low levels of packing after we re-introduced the chaser and re-distribution and swallow facilitation treatment package (M = 2%; range, 0% to 20%). When we discontinued nonremoval with the flipped spoon, packing remained at zero. However, when we removed re-distribution and swallow facilitation from the treatment package, packing became more variable and increased (M = 38%; range, 0% to 80%). Packing decreased to zero and remained at zero when we reinstated re-distribution and swallow facilitation with the therapist as the feeder and throughout caregiver training. Packing remained at zero when we again removed re-distribution and swallow facilitation at 4- and 6-week follow-up.
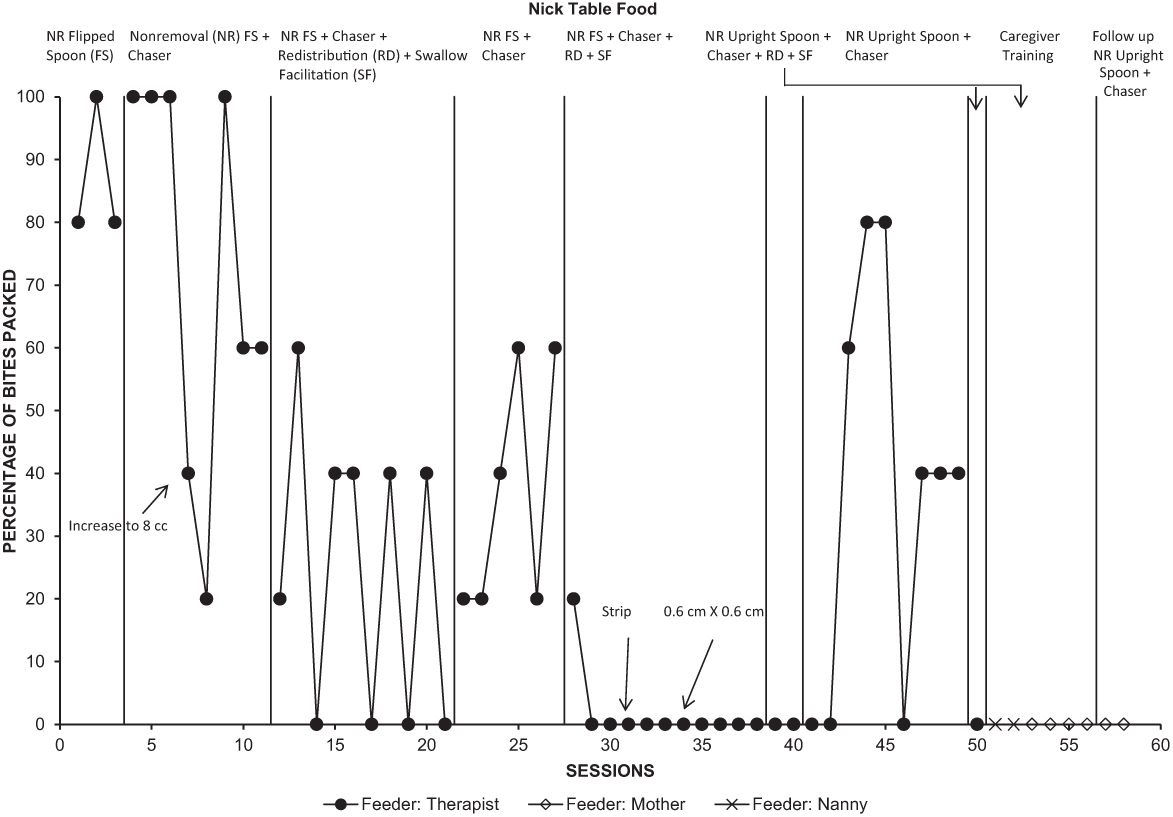
Percentage of bites packed for Nick with table food.
Mean percentage of packing for Cara (Figure 3) was 100% during both baseline phases and decreased to low levels during treatment (M = 12%; range, 0% to 80%). Packing remained at 0% after we introduced seven new foods. Percentage of packing was 8% (range, 0% to 80%) and 11% (range, 0% to 60%) with her mother and father, respectively, as feeders. Mean percentage of packing was 0%, 24%, and 0% during the 2-, 4-, and 6-month follow-up, respectively.
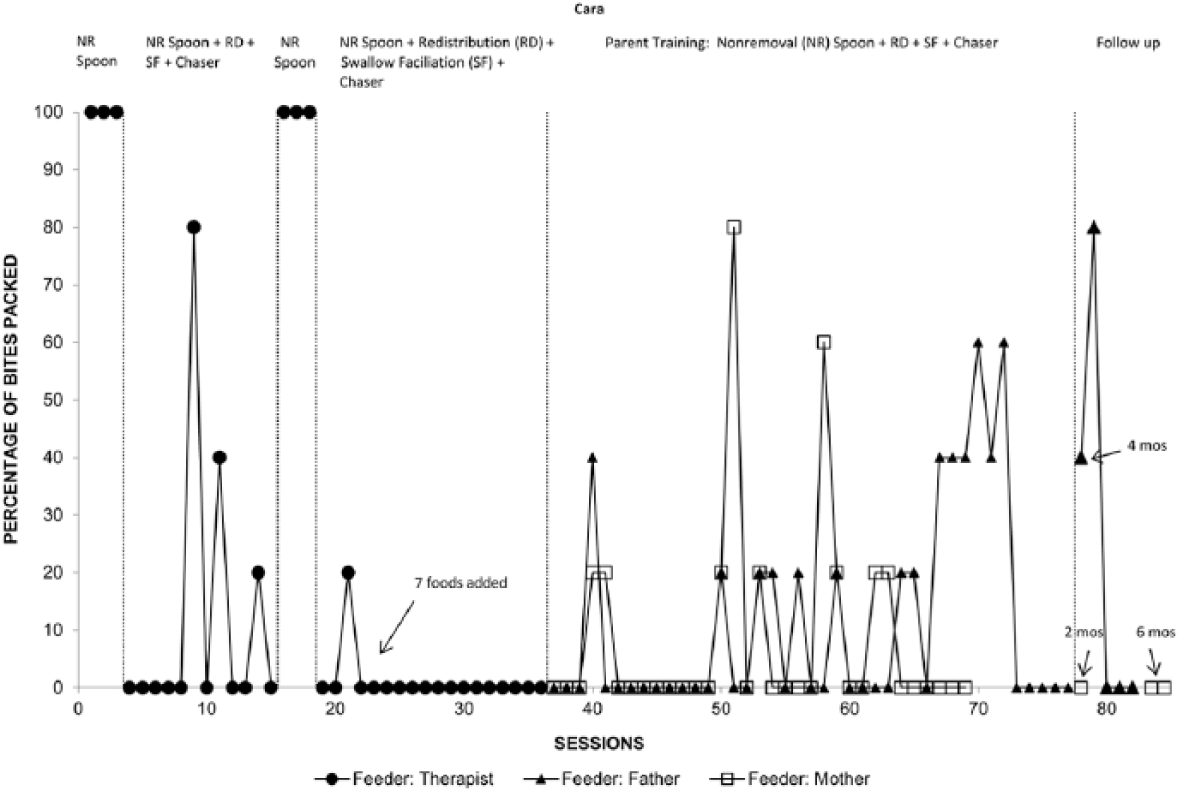
Percentage of bites packed for Cara.
Acceptance (i.e., the entire bite entered the child’s mouth within 5 s of presentation) was 99% (range, 60% to 100%), 100% (SD = 0), and 93% (range, 40% to 100%) for Nick purees, Nick table food, and Cara, respectively. However, total acceptance (i.e., the entire bite entered the child’s mouth at any point following presentation) was 100% (SD = 0) for Nick during the assessments with purees and table food and Cara. Although we did not collect data on acceptance of the chaser, the feeder implemented nonremoval of the cup which eliminated the possibility of the child refusing the chaser.
Discussion
Feeding problems are common in children with ASD (Seiverling, Williams, & Sturmey, 2010), and in some cases, feeding problems in children with ASD are associated with serious nutritional deficiencies. In the current investigation, both children had severe feeding problems in that Nick was over 90% dependent on a feeding tube for his calories and nutrition, and he only consumed small bites of table food that dissolved in his mouth after long periods of time (e.g., crackers). Although Cara did not have a feeding tube, she ate a limited variety of Stages 2 and 3 baby foods and only met 50% of her daily caloric needs by mouth at the time of her evaluation.
Like some children with ASD in previous investigations (Najdowski et al., 2003; Najdowski et al., 2010; Sharp & Jaquess, 2009), problematic feeding behavior in the form of packing emerged concomitant with increases in acceptance. Unlike the children in previous investigations, however, Nick and Cara did not respond to a single treatment such as re-distribution or swallow facilitation. Therefore, we combined procedures to reduce packing and produce clinically acceptable levels of consumption. Similarly, Dempsey et al. (2011) and Volkert et al. (2011) showed that multi-component treatments may be necessary to treat some children. These data are important because we demonstrate successful treatment of packing with children with ASD and feeding problems. Although feeding problems are common in children with ASD, we could find only one study that evaluated treatment for packing exclusively with children with ASD.
It is not clear why some children require multi-component treatments to reduce packing. Nick’s data demonstrate that re-distribution only and re-distribution and swallow facilitation did not effectively reduce packing. However, we did reduce packing when we added a chaser to re-distribution and swallow facilitation. Once Nick demonstrated success with pureed foods, we attempted to reduce packing for table-texture foods. Flipped spoon presentation plus chaser was not effective for Nick with table-texture foods. However, we successfully reduced packing when we combined the chaser with re-distribution and swallow facilitation using a nuk, thus replicating the finding for purees. During the table-food assessment, we were able to discontinue nonremoval with the flipped spoon after 11 sessions (8 appointments). However, packing again increased when we discontinued re-distribution and swallow facilitation, indicating the chaser alone was still not an effective treatment. It was only during follow-up on our fourth reversal of re-distribution and swallow facilitation that the chaser alone reduced packing. It was unclear what effect the ongoing treatment for chewing had on Nick’s packing with table food. It is possible that as Nick’s chewing skills improved, his packing decreased. However, this seems unlikely because we had been working on increasing Nick’s chewing skills for an entire year prior to this treatment analysis, and packing increased when we removed elements of the treatment package. On discharge from the outpatient program, Nick consumed age-appropriate portions of a variety of table foods (e.g., green beans, chicken, carrots, French fries, sweet potatoes, homemade pizza) in an average of 21 min without an intervention for packing in place, and he only received 2 ounces of Neocate Jr. via his gastrostomy tube.
The same treatment was effective for Cara. Similar to Nick, other procedures, including blending, decreasing food texture, re-distribution and swallow facilitation, and a chaser, did not reduce packing. Similar to Nick, she required a multi-component treatment. During outpatient follow up, we were able to advance four of the foods (i.e., black-eyed peas, bread, peas, and pineapple) to 0.6-cm × 0.6-cm pieces of table food, and packing remained low (M = 18%). We continued re-distribution, swallow facilitation, and the chaser, and we added differential positive (preferred toy) and negative (break) reinforcement for mouth clean per parental request.
Due to the invasiveness of the treatment procedures, one potential concern was whether the procedure was feasible for the feeder to implement due to high levels of inappropriate mealtime behavior (i.e., head turns, batting, and blocking). For Nick, rates of inappropriate behavior were low across the assessments with both purees and table texture (M = 0; range, 0 to 2.2 and M = 0.1; range, 0 to 1.3, respectively) during conditions involving the flipped spoon, re-distribution, and swallow facilitation procedures. For Cara, rate of inappropriate mealtime behavior was a mean of 2 (range, 0 to 12.7) during the nonremoval of the spoon, re-distribution, swallow facilitation, and chaser condition overall. For Cara, we also recorded inappropriate mealtime behavior that occurred during initial bite presentation and the re-distribution and swallow facilitation procedure separately, and less behavior actually occurred when the feeder implemented re-distribution and swallow facilitation (M = 0.4; range, 0 to 2.8).
Although identifying the operant mechanisms responsible for the effects of the multi-component treatment was not the aim of the current study, it is possible that the treatment compensated for poor oral-motor skills. The results of several studies have suggested that motor deficits are not uncommon in children with ASD (Ghaziuddin & Butler, 1998; Leary & Hill, 1996; Noterdaeme, Mildenberger, Minow, & Amorosa, 2002). For example, Ming, Brimacombe, and Wagner (2007) found that among 2- to 6-year-old children with ASD, the prevalence of hypotonia and motor apraxia was approximately 63% and 41%, respectively. The authors noted that the oral-motor apraxia of the children in the study was characterized by excessive drooling; open mouth during resting state; and inability to pucker lips, lick lips, or blow a bubble. Clearly, oral-motor apraxia could have a significant negative impact on feeding behavior. For example, a child who lacks adequate tongue control may have difficulty moving a bolus of food onto the tongue and/or propelling the bolus into the pharynx, responses that are important in the chain of behavior that results in swallowing. Also of concern was that in the Ming et al. study, children with hypotonia and/or motor apraxia were not more likely to receive interventional services (e.g., occupational therapy) to treat these impairments. The authors noted that this finding suggests that professionals are failing to recognize and treat fine motor and motor program deficits in children with ASD.
Examination of Nick and Cara’s feeding behavior is suggestive of the presence of oral- motor deficits and Cara was diagnosed with dysphasia. Recall that Nick held dissolvable food in his mouth for long periods of time, and Cara had experience only consuming baby food. Failure to advance texture of food may be indicative of a child’s lack of prerequisite skills for progressing through the age-typical sequence of feeding behaviors. During re-distribution and swallow facilitation, the feeder removes packed food from the child’s mouth and places it directly on the tongue while applying gentle pressure to the tongue. This sequence could compensate for deficits in oral-motor skills required for forming a bolus prior to swallowing and propelling the bolus into the pharynx. That is, the feeder places the bolus onto the tongue; thus, the child does not have to collect the bolus and move it to the tongue. The feeder also applies gentle pressure to the tongue while depositing the bolus, which may prompt or trigger a swallow response. The chaser also aids in bolus propulsion (i.e., moving the bolus toward the pharynx in preparation for swallowing) when swallow facilitation alone is insufficient for producing a swallow response (Vaz et al., 2012). A limitation of the current study was that it was not entirely clear how each component of the treatment contributed to the decreases in packing and whether all components were necessary. Future researchers should conduct a component analysis and systematically remove each treatment component to determine which are required to reduce packing.
Alternatively, negative reinforcement may have contributed to the decreases in packing because re-distribution and swallow facilitation were more aversive than swallowing and the child may have learned to swallow the bite to avoid the procedure (Volkert et al., 2011). It was also possible that reducing the texture of the packed food with the chaser may have reduced the aversive properties of eating and the motivation to avoid swallowing, thus decreasing packing (Vaz et al., 2012).
We scored mouth clean (converse of packing) at the 15-s mouth check but not as a different dependent variable (we scored mouth clean using the same key whether it occurred at the 15-s or 30-s mouth check). We also recorded whether the feeder conducted re-distribution and swallow facilitation for Nick (purees). Thus, we could analyze the within-session data to determine whether the feeder conducted re-distribution and swallow facilitation mid-interval and latency to mouth clean in seconds. We conducted an analysis of within-session data to determine whether food was in the mouth at the 15-s mouth check for each bite of a five-bite session (we converted to a percentage by dividing number of bites with food in mouth at 15-s mouth check by the number of bites that entered the child’s mouth and multiplied by 100). Food in the mouth at the 15-s check was a mean of 34% (range, 0% to 80%) and mean latency to mouth clean was 23 s when scored at the 15-s check (see top panel of Figure 4). For Cara, although we did not record whether the feeder conducted re-distribution and swallow facilitation, we did record inappropriate mealtime behavior that occurred during implementation of re-distribution and swallow facilitation as mentioned above to verify that food was in the mouth at 15 s for these bites. Based on these data and how closely latency to mouth clean when the feeder did and did not implement re-distribution and swallow facilitation mapped onto Nick’s data (see bottom panel of Figure 4), we determined that food in mouth at the 15-s check was a mean of 53% (range, 0% to 100%). Mean interobserver agreement for mouth clean during the analyzed sessions for both Nick (purees) and Cara was 95% (range, 85% to 100%).
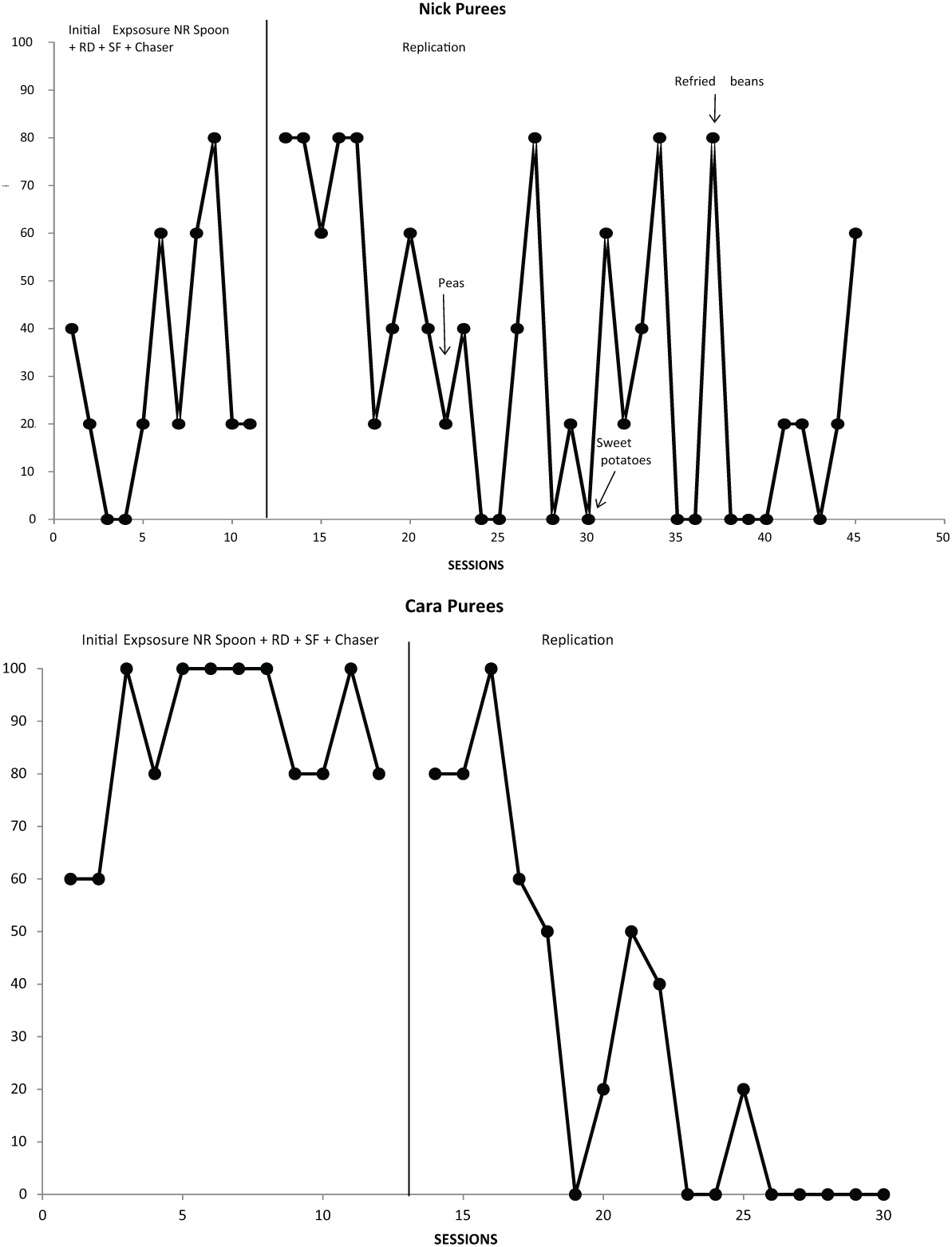
Percentage of food in mouth at 15-s check for Nick with purees (top panel) and Cara (bottom panel).
Nick’s data were difficult to interpret. Percentage of food in the mouth at 15 s was variable throughout the entire assessment with purees. Nick’s packing with purees may have decreased because the chaser reduced the texture of the food and also because he learned to avoid re-distribution and swallow facilitation at the 15-s mouth check but also because re-distribution and swallow facilitation were required to aid swallowing. The data for Cara suggested that packing may have initially decreased as a function of reduced texture and re-distribution and swallow facilitation, which aided swallowing. The within-session analysis of Cara’s data showed that food in mouth at 15 s decreased to between 20% and 0% after 21 sessions. That is, it appeared that over time, re-distribution and swallow facilitation improved her oral–motor skills and she then began to avoid re-distribution and swallow facilitation at the 15-s mouth check. The within-session data were not as readily available for Nick’s analysis with table texture. We could have examined latency to mouth clean data but the data did not map onto the other participants’ data as closely due to differences in the procedure with table food.
A limitation of the current study was that the relationship between the sequence of conditions and packing was unclear. For example, we do not know the effects of implementing the chaser earlier in the sequence for either participant. Although we implemented the chaser first in the table-food analysis with Nick, we also combined this with a flipped spoon presentation and we already exposed his behavior to re-distribution and swallow facilitation in the previous analysis with purees. It is also possible that the chaser was only efficacious because we implemented it last in the sequence and only because of prior exposure to seemingly more invasive procedures (re-distribution and swallow facilitation). Also of interest is the relative size of the chaser. We increased Nick’s chaser from 4 cc to 8 cc to determine whether it would decrease packing. Although we did not observe such benefits, it is quite possible that systematic variations of the chaser under more carefully controlled conditions would prove efficacious.
Differences during re-distribution and swallow facilitation procedures across participants may also limit the current conclusions. Volkert and colleagues (2011) suggested that a flipped spoon distributes pressure to a larger area on the tongue than does a nuk brush, and therefore may be a more effective utensil to use during re-distribution and swallow facilitation (in addition to being a more socially valid utensil) for some children. In our study, we used a nuk brush with Nick (purees) and a flipped spoon with Cara (and Nick table food). As previously mentioned, however, we discontinued the flipped spoon re-presentation with Nick (table food) in favor of an upright spoon representation. Although we did not examine the effects of these different techniques on packing outcomes, placement location of the bolus on the tongue and the relative amount of applied pressure used during re-distribution and swallow facilitation are each potential procedural elements that may influence packing and are thus worthy of further inquiry. We also did not collect treatment integrity data concerning bite placement for re-distribution (mid-tongue) versus swallow facilitation (posterior tongue). Variations in the implementation of re-distribution and swallow facilitation within and across sessions may have accounted for some of the variability in packing. Given the importance of bite placement to these procedures, future research should address this limitation.
It is worthy to note that despite the multi-component treatment package’s efficacy for both children, effects were not as pronounced for Nick during the table-food analysis. Although the reasons are not clear, other procedural variables, such as the increased food texture (i.e., masticated food) or the influences of the chewing-treatment procedures warrant attention. We also used chicken during this analysis, which may have been a more difficult food to swallow overall (e.g., more dry and gritty in addition to the advanced texture) compared with the other purees, especially Cara’s food that we pureed with a Magic Bullet food processor. This specialized processor reduces the texture of purees (more smooth) slightly further than a traditional food processor (e.g., Cuisinart).
Future research should also focus on development of a prescriptive assessment to determine which children will benefit from which treatment component(s). In the current investigation, we evaluated a number of different treatments for packing. Although we ultimately identified an intervention that was effective, treatment could have been more time efficient if we had a method for predicting which treatments would be effective. Said another way, can we identify child behavior that would be indicative of which treatment would be effective for problematic feeding behavior such as packing? For example, would data on where the child packed the bite in his or her mouth (e.g., on the roof of the mouth, between the check and gum, under the tongue) give us an indication of what treatment would work?
In conclusion, our investigation demonstrates the efficacy of a multi-component treatment package that used re-distribution, swallow facilitation, and a chaser to treat packing in two children with ASD and complex feeding problems. Furthermore, the treatment package continued to be effective when we increased the variety and texture of foods. This study adds to the small literature on the treatment of packing specifically with children with ASD and is the second to demonstrate the usefulness of a chaser to reduce packing in children with feeding disorders.
Footnotes
Acknowledgements
Thanks to Rebecca Groff, Jana Frese, and Haley Hall for their assistance with this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.