
Abstract
Purpose
To examine accessibility, availability, and quality of diabetes self-management education (DSME) for uninsured adults or those utilizing Medicaid in a community with a high poverty rate.
Methods
A descriptive needs assessment was conducted in 8 health care agencies serving the uninsured. Face-to-face audiotaped interviews were conducted with 22 health care providers, educators, and administrators to capture descriptive characteristics about clinical care, DSME, continuity of care, and organizational function.
Results
Twenty-nine percent of adults with diabetes were reported to be uninsured or utilizing Medicaid in these settings. Only 4% of adults received the American Diabetes Association’s DSME standards of care. At 5 agencies, there was no direct access to DSME. Uninsured individuals had access to 2 programs; individuals utilizing Medicaid had access to 1 program. Certified diabetes educators were available at only 3 agencies. There were DSME programs that adhered to recommended guidelines but limited availability for these adults. The majority of education (86%) was limited to clinical encounters with providers, which were infrequent and variable in duration. Time spent on education ranged from 2 to 120 minutes depending on agency type. Education topics addressed by providers varied by agency.
Conclusions
Findings of this study suggest that adults who are utilizing Medicaid or are uninsured do not get the amount, type, or quality of DSME needed to sustain successful self-management. Limited availability and inadequate access to quality DSME place vulnerable adults at increased risk for devastating and costly complications despite the known benefits.
Diabetes self-management education (DSME) is the foundation of diabetes care and is essential for improving the knowledge and skills necessary to perform self-management. 1 DSME’s importance is evidenced by its inclusion in the American Diabetes Association’s (ADA’s) Standards of Medical Care in Diabetes and Clinical Practice Recommendations. 2 Maintaining glycemic control and preventing devastating and costly complications requires a comprehensive approach utilizing appropriate clinical care in addition to optimal self-management practices.2-4 DSME improves clinical outcomes and quality of life especially in the immediate follow-up period of 6 months or less,3-5 and ongoing follow-up and support have been shown to increase the positive effects of DSME and sustain successful long-term self-management. 4
Diabetes education can reduce health care costs and hospitalization rates.6,7 In particular, DSME has been shown to reduce health care costs in high-risk populations.8,9 Low-income and minority populations are examples of high-risk groups that have higher rates of diabetes complications and health care utilization, as well as poor disease management.10-15
Uninsured adults constitute another high-risk group. Their growing number presents an enormous challenge for health care professionals and policy makers. Uninsured adults with diabetes have poorer health care than those with insurance, including those with Medicare and veterans benefits, and are disproportionate from low-income or minority populations. 13 Approximately 15.5% of Americans were uninsured in 2007-2008, a substantial increase from 12.5% in 2003. 16 According to findings from the 2003 National Health Interview Study, 15% of nonelderly adults who report having diabetes are uninsured. 17 Chronically ill uninsured adults, including those with diabetes, are less likely to have seen a physician in the past 12 months, less likely to have a source for regular care, and are likely to use hospital emergency departments for routine care.17,18 They are also less likely to receive preventive measures and engage in blood glucose monitoring, both of which can detect and prevent costly and devastating complications.13,17 The uninsured may have inadequate self-management practices and poor adherence to a treatment plan due to a multitude of factors, including poor health literacy, 8 poor access to primary care providers, 17 the high costs of medications and blood glucose testing supplies, and poor access to diabetes self-management education.7,9
Despite recognition that DSME is critical for improving self-management skills and patient outcomes, only 56% of US adults with diabetes have ever participated in DSME. 19 This public health challenge is complicated by the disproportionately high rate of diabetes among persons in low-income groups. Only 42% of uninsured adults reported ever attending a diabetes education class. 13 Furthermore, in many states, Medicaid does not reimburse for DSME for individuals at the poverty level. The Medicaid reimbursement policy for DSME is determined at the state level, and with many state budgets in crisis, more will likely drop this benefit. This lack of coverage may pose a significant threat to the health of persons with diabetes who are low income, blind, or disabled. Additionally, limited physician referral, poor insurance reimbursement, and lack of funding for DSME programs demonstrate that policy changes are needed to ensure DSME accessibility for all individuals. 20 Despite the passage of the Patient Protection and Affordable Care Act of 2010, care for individuals with diabetes is still unclear. Specific approaches are needed to address issues faced by high-risk populations such as the uninsured that prohibit their obtaining the needed education to manage a chronic progressive disease such as diabetes.
As the rate of uninsured persons with diabetes continues to grow, it is important to examine barriers to obtaining DSME for this population. While research has shown the impact of DSME in the socially disadvantaged, racial, and ethnic minorities and Medicaid recipients, little is known about DSME and the uninsured.7-9 As part of a larger study examining DSME and clinical care for vulnerable populations, this study examined the accessibility, availability, and quality of DSME for adults who were uninsured or utilizing Medicaid in a community with a high poverty rate.
Methods
A descriptive needs assessment was conducted in health care settings serving uninsured adults in a midsized town in the Southeastern United States with a 19% poverty rate. Approval was obtained from the Human Assurance Committee of the Medical College of Georgia.
Participants
Eight health care agencies agreed to participate in the study: 2 emergency departments (ED), 2 hospital-based (HB) diabetes education departments, 2 free primary care clinics (PC), and 2 sliding-scale fee-for-service PCs. Although DSME may not typically occur in EDs or PCs, this study was part of a larger study assessing DSME and clinical care to uninsured and underinsured adults. The investigator chose to interview providers in these settings to determine what was actually in place since many of these vulnerable adults may use these agencies as their “one-stop shop” for health care.
A letter was sent to each agency asking for voluntary participants who provided clinical care or education to adults with diabetes mellitus. Participants consisted of health care providers, educators, and administrators working at these agencies (n = 22). The number of participants varied by agency and included: 11 registered nurses of whom 4 were administrators; 6 physicians; 2 registered dieticians; 1 medical social worker; 1 executive director; and 1 health educator/community outreach coordinator. Four certified diabetes educators (CDEs) participated: 2 registered nurses and 2 registered dieticians. Those providing care exclusively to adults with gestational diabetes or children were excluded. No patients were included.
Instruments
A 28-item interview guide was developed using themes from a literature review, the Standards of Medical Care in Diabetes, 2 the National Standards for DSME, 3 and the assessment of Primary Care Resources and Supports for Chronic Disease Self Management (PCRS). 21 The interview guide captured quantitative and descriptive data about clinical care, self-management education, continuity of care, and organizational function and attributes. A 10-item demographic questionnaire was designed to obtain information about patients with diabetes, providers, funding sources, and hours of operation at each agency.
The PCRS was designed to assess self-management support integration in primary care settings. 21 Based on the Chronic Care Model and the Resources for Self-Management and Support, the PCRS assesses the level of care between the patient and the care providers (patient support) and the level of support at the clinic or health care systems level (organizational support).21,22,24 The PCRS consists of 16 items, rated on 10-point Likert scales yielding 4 levels of performance: nonexistent or inadequate support (score = 1, or level D), inconsistent sporadic interactions and support (2-4, level C), coordinated and consistent supports (5-7, level B), and consistently systematic integrated approaches (8-10, level A). A range of numbers are used within levels A-C to rate the degree to which an element is being met. The PCRS was designed to be used as a self-assessment tool for teams in primary care settings. In this study, ratings were completed by the investigator after listening to audiotaped interviews of each participant and entering data on an interview coding form.
Reliability for the PCRS has been high, with Cronbach α = 0.94 for individual support and 0.90 for organizational support. 22 Internal consistency of the PCRS in this project also was high: overall, α = 0.93; patient support, α = 0.91; and organizational support, α = 0.81.
Audiotaped, face-to-face interviews were conducted with each participant. Two investigators separately completed interview coding forms while listening to recordings of each interview. Interrater reliability for the interview coding form was acceptable (κ = .77). The PCRS ratings were completed by 1 investigator using data from the interview coding form. A demographic questionnaire was given to each agency to complete and return by mail. Agencies were contacted to verify and obtain missing information on the demographic form if needed.
Results
Data for the demographic questionnaire, the interview guide, and the PCRS ratings were entered into an Excel spreadsheet. Data were analyzed using SAS 9.1.3 and SPSS.
Agency Demographics
The total number of individuals with a diagnosis of diabetes mellitus who received reported care over a 1-year period was 8338: free PCs, n = 457; fee-for-service PCs, n = 511; EDs, n = 6474; and HB DSME programs, n = 896. Figure 1 illustrates the percentage of uninsured adults and those utilizing Medicaid with diabetes mellitus reported by agency type. Overall, 20.6% were uninsured (n = 1725) and 8.4% utilized Medicaid (n = 692), for a total of 29% for all agencies (n = 2417). Reported care was provided to 64% of uninsured patients with diabetes in EDs (n = 1104) and to 33.5% in PCs (n = 577); only 2.5% attended HB DSME (n = 44). For Medicaid recipients, 81.6% were seen in EDs (n = 565), 10% were seen in PCs (n = 69), and 8% attended HB DSME programs (n = 58).
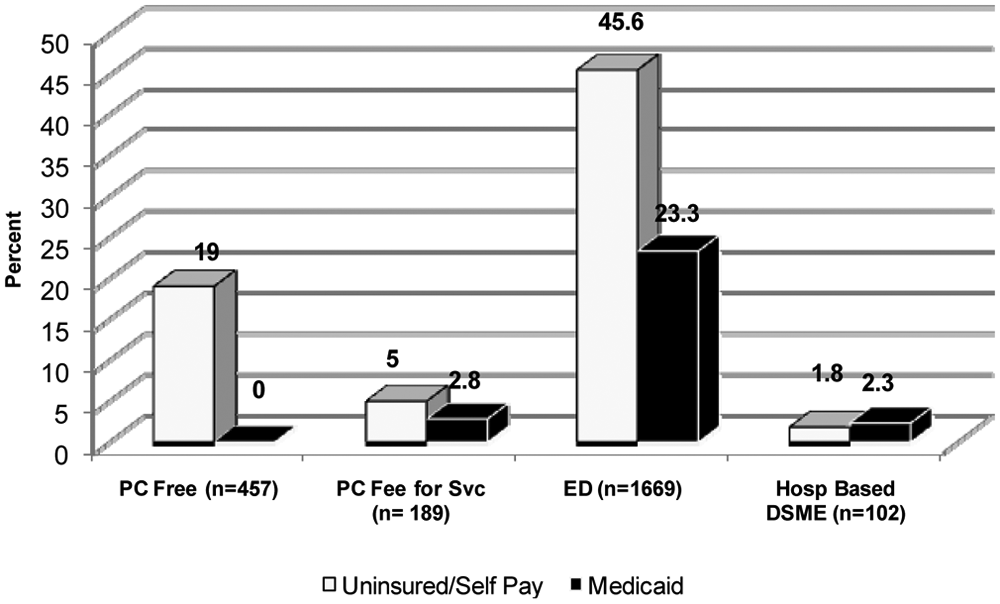
Percentage of self-pay, uninsured, and Medicaid covered adults with diabetes mellitus seen in free and fee-for-service primary care, emergency departments, and hospital-based diabetes self-management education programs (n = 2417).
At several agencies, uninsured patients were identified as self-pay status. The 2 free clinics did not accept Medicaid or payment for services. One agency reported no patients who were self-pay, uninsured, or covered by Medicaid.
Accessibility
Access to DSME was measured by determining whether education was offered, what type of education was offered, whether CDEs were on site, and whether a process was in place for uninsured persons or those using Medicaid to obtain education. Two HB diabetes education programs were ADA recognized and provided comprehensive DSME. One HB program reported having no mechanism in place for those who are uninsured and having no uninsured or Medicaid clients. The other HB program had a mechanism in place for self-pay or uninsured persons to receive DSME, but only 4% of the uninsured or Medicaid patients received care there (n = 102). A third agency provided free DSME but was not an ADA-recognized program (free PC).
Of the 3 agencies providing DSME, 2 required qualifying income documentation to receive free services (HB DSME, free PC). A fourth agency provided diabetes classes sponsored by a pharmaceutical representative on an infrequent basis (fee-for-service PC). CDEs and diabetes educators were employed full-time at 2 of the 8 agencies. The remaining 6 agencies had limited or no CDEs on site.
Availability
DSME availability was assessed by hours of operation and location of programs. The 2 HB programs offered day and evening classes several times a month and were open weekdays, 8
All agencies were located on city bus lines and were easy to reach by bus, car, or foot. The 2 HB programs had parking fees ranging from $1.00 to $1.50 per hour. Additionally, one PC agency provided DSME in Spanish, and all agencies had Spanish translators or bilingual staff available.
Quality of DSME
Reported use of recommended guidelines and PCRS ratings were used to measure quality of DSME. Two DSME programs had ADA recognition, indicating adherence to the ADA’s National Standards for DSME. A third agency offered comprehensive DSME but was not an ADA-recognized program and did not meet all criteria.
Mean PCRS ratings of all participants were 3.50 for patient support and 3.09 for organizational support. Individual item scores ranged from 1 (inadequate or nonexistent) to 9 (systematic integrated support). PCRS ratings were also analyzed and compared by agency type (Figure 2). Agency mean ratings for patient support ranged from 2.63 to 6.90; mean ratings for organizational support ranged from 2.28 to 5.59. The ADA-recognized DSME programs received the highest overall ratings. CDEs were rated highest regardless of agency (patient support, mean = 6.06; organizational support, mean = 5.03).
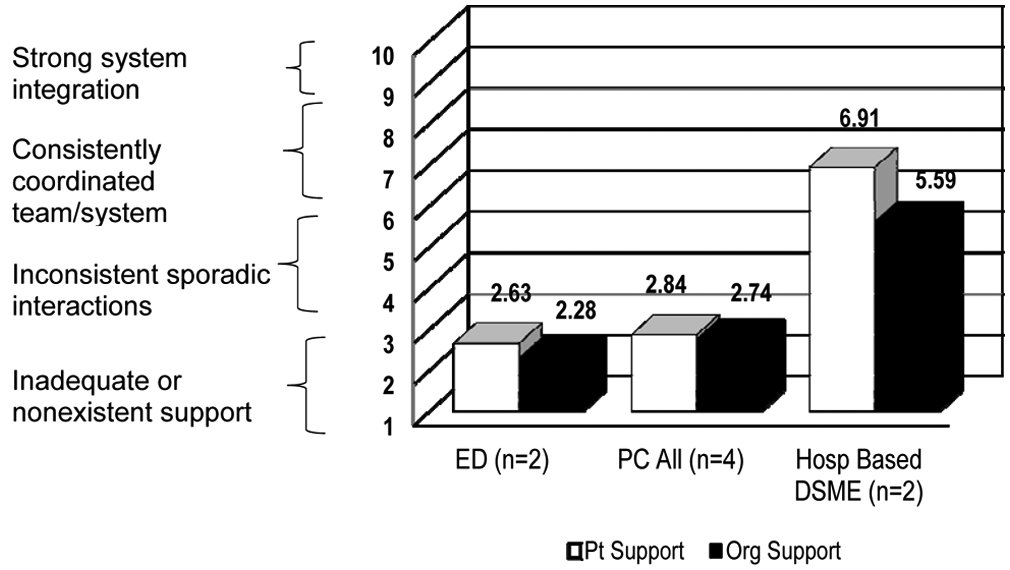
Mean assessment of Primary Care Resources and Supports for Chronic Disease Self Management ratings by agency type.
The data showed that 86% of education was provided by care providers during clinical encounters, with visit times ranging from 15 minutes to 5 hours, depending on the agency. PC visit times ranged from 15 to 75 minutes, with frequency of PC visits ranging from every 3 to 6 months. Education time ranged from 2 to 120 minutes across settings, with a mean education time of 8 minutes for EDs (range, 5-15 minutes), 34 minutes for PCs (range, 2-120 minutes), and 120 minutes for HB DSME programs (Figure 3).
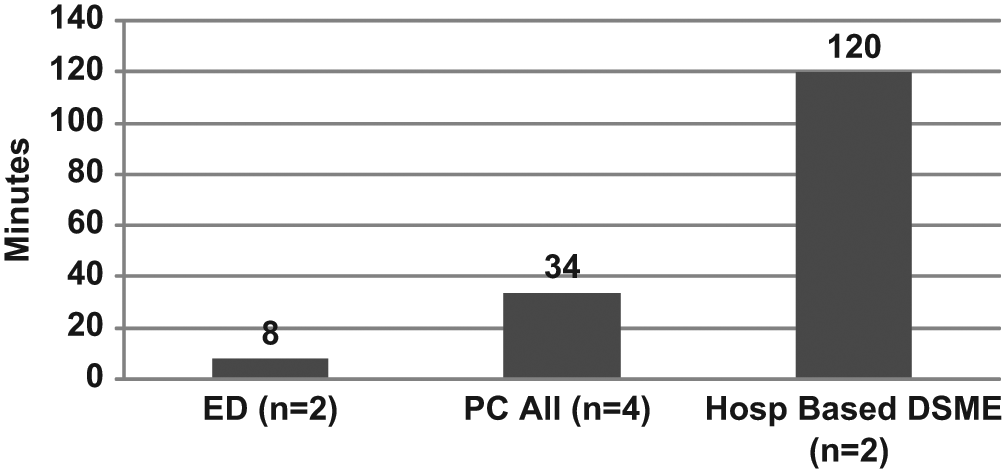
Mean education time reported by agency type.
Participants were asked to report which education topics were covered during encounters, using the American Association of Diabetes Educators 7 self-management behaviors: diet, exercise, monitoring, medications, stress management and coping, problem solving, and preventing complications. 23 Figure 4 displays reported frequency of education topics addressed by agency type. The HB DSME programs reported covering all topics 100% of the time, while the PCs reported covering diet, exercise, and preventing complications 80% to 90% of the time and problem solving and stress management only 50% to 60% of the time. EDs reported addressing all topics much less frequently. Exercise and stress management were addressed the least, only 13% of the time.
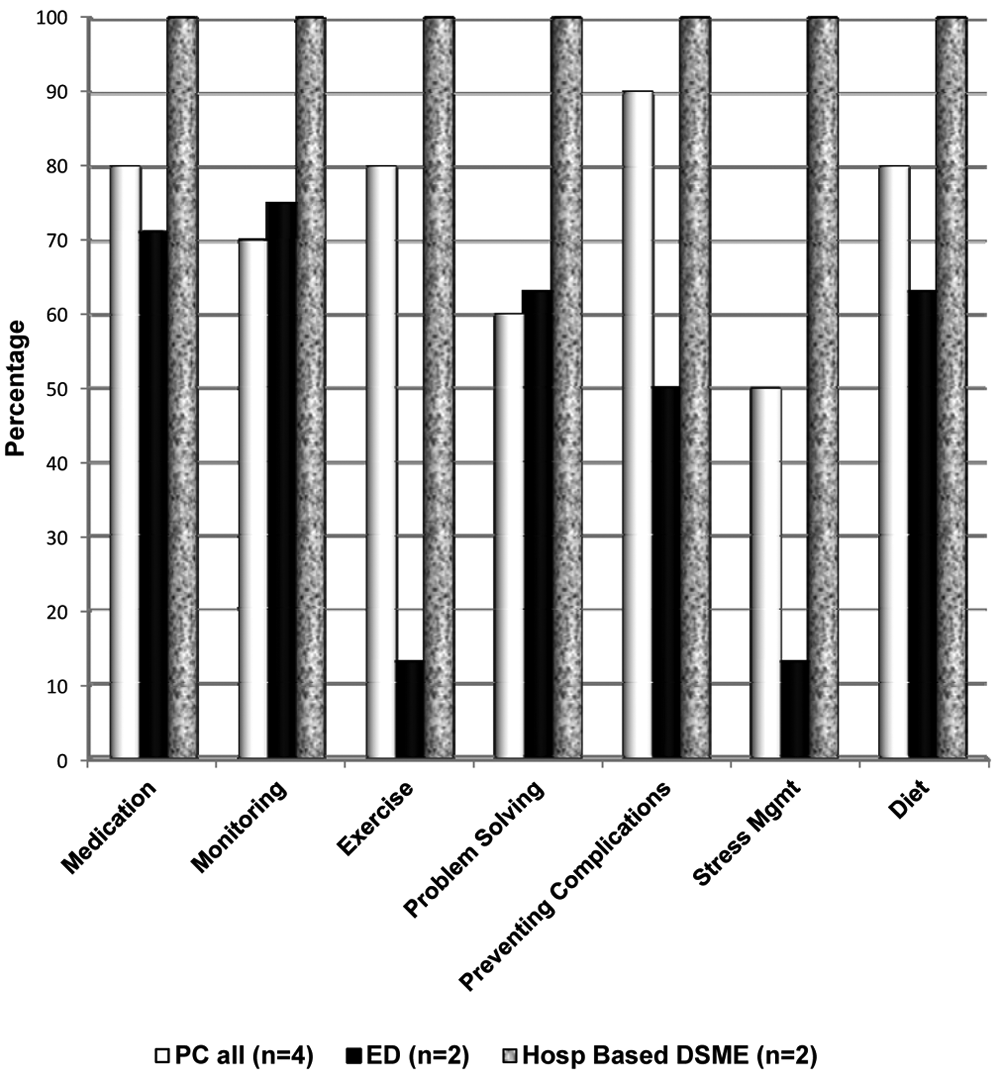
Education topic reported by agency type.
Additional Findings
The data showed that referrals for DSME and other community resources consisted of giving written information with little or no follow-up or coordination of referrals. There also was a general lack of information about services provided by other agencies. A Community Health Worker Program was in place at 1 free PC. An unexpected finding was that, across all agencies, 68% of the participants reported that depression screening was not being done as part of the care provided.
Discussion
This comprehensive needs assessment was the first systematic evaluation of accessibility, availability, and quality of diabetes care for uninsured adults in this community. The overall percentage of uninsured adults with diabetes seen in the 8 participating agencies was similar to the estimated percentage of uninsured in the community studied (20%). By far, the hospital EDs provided care for the largest number of uninsured patients with diabetes. However, it was not just the uninsured who sought treatment in EDs: Even in a community with a high poverty rate, 74% of ED patients with diabetes were insured.
We concluded that accessibility to quality DSME programs was inadequate and availability severely limited for adults with diabetes who are uninsured or utilizing Medicaid in this community. The adults with diabetes in these settings rarely received the standard of care for DSME. Quality programs and adherence to ADA guidelines were limited to 2 ADA-recognized programs, with only 1 serving a small fraction of the uninsured and Medicaid clients with diabetes (4%). For almost 90% of the patients seen, diabetes education was limited to infrequent clinical encounters that were variable in duration and did not cover all topics essential for diabetes self-management. The lack of referral follow-up by providers also suggests that these individuals may not be referred to DSME, so these brief clinical encounters may be the totality of education received. These findings suggest neither Medicaid recipients nor the uninsured get the amount, type, or quality of DSME needed to sustain successful self-management to prevent costly and devastating complications.
The generally low range of PCRS scores demonstrates limited and inconsistent support for self-management in PCs and EDs. Only HB DSME programs demonstrated consistent and comprehensive patient and organizational support for self-management. CDEs had the highest PCRS ratings of all participants, which suggests that using recognized, approved guidelines supports successful patient self-management and improved organizational integration.
Additional findings are disturbing—namely, the substantial majority of participants who consistently failed to screen for depression and the low frequency of education on stress management. Both findings demonstrate the critical need to educate health care professionals about the importance of addressing mental health needs of patients with diabetes. Administering a simple depression screening tool and facilitating stress management techniques are critical elements of comprehensive diabetes care that can result in improved patient outcomes in the management of a chronic illness.2,23-25
There were several limitations to this study. The interview guide and the demographic questionnaire were designed to obtain information in a brief and comprehensive manner during face-to-face interviews. However, some items did not translate well across all settings, nor did the interview guide capture aspects of care needed to score every item on the PCRS accurately. Because the PCRS was designed to be used as a self-report tool in PC settings, ratings based on interviews may not have accurately reflected the care provided in different settings.
Implications for Practice
The growing number of uninsured persons with diabetes requires prompt community action to address inadequate access and limited availability to quality DSME programs. Despite passage of the Patient Protection and Affordable Care Act of 2010, adults with diabetes who are uninsured or utilizing Medicaid may continue to have an uncertain future when it comes to obtaining the necessary DSME to successfully manage their disease.
Utilization of evidence-based practice models can improve accessibility and availability of quality DSME. One strategy that has been useful in comparable populations is creating a community diabetes collaborative network that can serve as an effective mechanism for fostering partnerships and exploring problems and solutions related to diabetes care.23-25 A collaborative can also improve continuity of care, communication among providers, and knowledge of community resources and serve as a forum to explore evidence-based practice models that have been effective in populations with similar challenges.
Improving access to DSME requires developing and implementing a process for DSME for uninsured and underinsured individuals regardless of setting or agency type. In a community with limited CDEs and DSME programs, forming community partnerships is essential to providing DSME for all who need it. Effective strategies for meeting the needs of high-risk populations include partnering DSME programs with primary care visits, offering DSME in the same location as primary care visits, and expanding community health worker programs that focus exclusively on diabetes care.23-25
Awareness of the existing barriers and gaps to obtaining DSME is the first step in improving accessibility and availability to quality DSME programs. The knowledge generated by this study can be utilized to identify and reduce these barriers, coordinate existing services, foster community partnerships, and develop new methods of care delivery for these vulnerable adults with diabetes.
Footnotes
Acknowledgements
We thank Thomas Joshua, MS, Medical College of Georgia, for statistical support, and Autumn Schumacher, PhD, RN, Medical College of Georgia, for review of a previous draft of the manuscript.