
Abstract
Older Black and Hispanic adults report more religious involvement, and religious involvement has been linked to better cognition. This study examined which aspects of religious involvement are associated with better longitudinal episodic memory and whether religious involvement offsets racial and ethnic inequalities in episodic memory. Using Health and Retirement Study data (N = 16,069), latent growth curves estimated independent indirect pathways between race and ethnicity and 6-year memory trajectories through religious attendance, private prayer, and religious belief, controlling for nonreligious social participation, depressive symptoms, chronic health diseases, age, education, and wealth. Negative direct effects of Black race and Hispanic ethnicity on memory were partially offset by positive indirect pathways through more private prayer and religious attendance. While results were significant for memory intercept and not subsequent memory change, religious attendance and private prayer were independently associated with better cognitive health among diverse older adults. Findings may inform culturally relevant intervention development to promote successful aging and reduce older adults’ cognitive morbidity.
Substantial theoretical and empirical research has delineated the potential health consequences of social inequalities experienced by racial and ethnic minorities (Anderson, 1989; Clark, Anderson, Clark, & Williams, 1999; King, 1996). For example, older Black and Hispanic adults have a higher risk of dementia compared with non-Hispanic White counterparts (Mayeda, Glymour, Quesenberry, & Whitmer, 2016; Tang et al., 2001). Underlying mechanisms are multifactorial, extending beyond racial and ethnic disparities in education, literacy, and cardiovascular diseases (Tang et al., 2001). Research has recently implicated psychosocial experiences such as discrimination in racial and ethnic inequalities in episodic memory, a primary determinant of dementia risk (Barnes et al., 2012; Zahodne, Sol, & Kraal, 2019). While research in health disparities typically focuses on risk factors using a deficit model, accumulating research suggests the utility and importance of moving toward a more holistic model that incorporates a strengths-based approach in order to ultimately achieve health equity (Saleeby, 2012). Relative to risk factors, empirical evidence rooted in a strengths-based approach examining the role of protective pathways in minority cognitive aging is underdeveloped. Enhanced understanding of protective pathways could reveal new targets for intervention development in cognitive aging. Religious involvement, in particular, may be a salient and culturally relevant protective pathway for reducing racial and ethnic inequalities in cognitive aging.
Literature Review
Religious involvement and cognition
Religious involvement is multidimensional and encompasses several related but distinct dimensions: organizational (e.g., frequency of religious attendance), nonorganizational (e.g., frequency of private prayer), and personal beliefs (e.g., religious belief; Levin, Chatters, & Taylor, 1995; Levin, Taylor, & Chatters, 1995). Religious involvement may provide protective pathways in cognitive aging, as it has been associated with better mental (Ayele, Mulligan, Gheorghiu, & Reyes-Ortiz, 1999; Koenig, Ford, George, Blazer, & Meador, 1993; Koenig, George, Titus, & Ãk, 2004) and physical (Koenig et al., 1998, 2004; Taylor, Chatters, & Levin, 2004) health, lower mortality (Mccullough, Hoyt, Larson, Koenig, & Thoresen, 2000), and more recently, better cognitive health (Hosseini, Chaurasia, & Oremus, 2017). Empirical evidence linking religious involvement to better health is grounded primarily within two theoretical frameworks. First, religious involvement has been included as a fourth, conceptually distinct factor (Crowther, Parker, Achenbaum, Larimore, & Koenig, 2002) in Rowe and Kahn’s (1998) three-factor model of successful aging, which can be targeted to facilitate better physical and cognitive health outcomes.
While associations between the multiple dimensions of religious involvement and physical health outcomes are well documented, prior research linking religious involvement to cognitive outcomes has primarily focused on religious attendance. The second framework used to guide research in this area is grounded in the theory of social engagement that argues that social activities and relationships provide a cognitively demanding environment, which limits age-related decrements in cognitive performance (Bassuk, Glass, & Berkman, 1999). Bassuk, Glass, and Berkman (1999) posit that religious attendance represents a unique component of social engagement that provides opportunities for social interaction. Thus, positive associations between religious attendance and cognition may be due to the social nature of religious attendance (Reyes-Ortiz et al., 2008; Van Ness & Kasl, 2003; Yeager et al., 2006) as social participation may be protective in cognitive aging (Bassuk et al., 1999; Fratiglioni, Paillard-Borg, & Winblad, 2004). Altogether, these findings support the possibility that religious attendance may be associated with better cognitive health via the social aspects inherent in attending religious services.
Importantly, however, associations between religious attendance and cognitive outcomes may be confounded by an individual’s general or trait-like nonreligious social participation. A greater tendency toward social participation more broadly (i.e., across multiple social engagement domains) may increase the extent to which one also engages in social participation more specifically (e.g., attending religious services). Because greater social participation in nonreligious activities has also been linked to better cognitive functioning (Fratiglioni et al., 2004), general or trait-like social participation may confound associations between religious attendance and cognitive outcomes. Indeed, previous research has shown that positive associations between religious attendance and cognition persist after controlling for social support (Corsentino, Collins, Sachs-Ericsson, & Blazer, 2009) and nonreligious social participation (Hill, Burdette, Angel, & Angel, 2006; Van Ness & Kasl, 2003). Notably, however, few studies quantify the association between religious attendance and cognition independent of general, nonreligious social attendance (for a review, see Hosseini et al., 2017). Indeed, this recent systematic review of the literature recommended that future studies control for social participation in order to isolate the associations between dimensions of religious involvement and health.
Compared with religious attendance, less is known regarding other dimensions of religious involvement, including private prayer and religious belief. Crowther et al. (2002) posit that religious involvement facilitates successful aging as it encourages behaviors such as meditation and prayer that have been associated with better physical health (for a review, see Seeman, Dubin, & Seeman, 2003). Specifically, praying privately may benefit physiological health (Seeman et al., 2003; Townsend, Kladder, Ayele, & Mulligan, 2002), which has been associated with better memory functioning in older adults (Beeri, Ravona-Springer, Silverman, & Haroutunian, 2009). Therefore, it is plausible that the benefits of private prayer on physical health and physiological functioning could be extended to cognitive health in older adults. Indeed, private prayer has been positively associated with cognition in midlife (Inzelberg et al., 2013), but its association with cognition among older adults is inconsistent (Yeager et al., 2006). Finally, strength of religious belief has been positively associated with physical health (Ellison & Levin, 1998) yet inversely associated with cognitive health (Ritchie, Gow, & Deary, 2014; Zuckerman, Silberman, & Hall, 2013). The negative association between religious belief and cognition may reflect reverse causation, as individuals with fewer cognitive resources may utilize religious beliefs to obtain self-control, which may be obtained through alternative means by individuals with more cognitive resources (Zuckerman et al., 2013). Previous research has also suggested that greater religious belief may reflect higher utilization of intuitive processes relative to analytical cognitive processes (Gervais & Norenzayan, 2012). Given positive associations between religious belief and physical health, additional research investigating the association between religious belief and cognitive health is warranted. In this regard, quantifying multiple independent religious involvement pathways to cognition within a single model may clarify patterns of association.
Religious involvement and minority cognitive aging
Research on religious involvement is highly relevant to racial and ethnic inequalities in cognitive aging because Black and Hispanic older adults report more religious involvement than non-Hispanic Whites (Maldonado, 1995; Taylor et al., 2004). While within-group research using longitudinal designs has demonstrated the salutary health effects of religious involvement in older Hispanic (Hill et al., 2006) and Black (Levin, Chatters, & Taylor, 2011) adults, the extent to which this greater religious involvement may reduce the magnitude of measured cognitive inequalities remains unknown. Furthermore, most studies include only one or two racial or ethnic groups and do not quantify the extent to which positive indirect pathways through greater religious involvement could offset negative associations between Black race or Hispanic ethnicity and cognitive outcomes. Thus, because religious involvement represents a culturally relevant resource, investigating the role of religious involvement in associations between race and ethnicity and memory decline could clarify the magnitude of racial and ethnic inequalities in cognitive aging and inform intervention development efforts for older adults who report religious practice.
The current study
Using 6 years of Health and Retirement Study (HRS) data, the current study quantified indirect pathways from race and ethnicity to longitudinal memory outcomes through baseline religious attendance, religious belief, and private prayer. Previous research demonstrates that Black and Hispanic older adults obtain lower scores on cognitive tests (Gross et al., 2015; Manly & Mungas, 2015) and report greater religious involvement relative to non-Hispanic White counterparts (Maldonado, 1995; Taylor et al., 2004) and that religious involvement is associated with a variety of positive health outcomes (Bassuk et al., 1999; Crowther et al., 2002). Based on this literature, we hypothesized that (1) the negative associations between Black race and Hispanic ethnicity and memory outcomes would be offset by positive associations through dimensions of religious involvement. Specifically, Black and Hispanic older adults would report more religious involvement than non-Hispanic White older adults, and religious attendance and private prayer, but not religious belief, would be independently associated with better memory outcomes. Previous research has also demonstrated that religious involvement represents a unique aspect of social engagement that may confer cognitive health benefits (Bassuk et al., 1999) independent of general or trait-like sociability (Hosseini et al., 2017). Thus, we also hypothesized that (2) positive indirect pathways from Black race and Hispanic ethnicity to memory through religious involvement would persist after controlling for nonreligious social participation.
Method
Participants
The HRS is a nationally representative sample of Americans over age 51 who are interviewed every 2 years (Sonnega et al., 2014). Details of the HRS are available online (http://hrsonline.isr.umich.edu). Inclusion criteria for the current study were: age 51 years or older at the 2006 wave, available data on the outcome variable (memory; see below), and self-report as non-Hispanic Black, non-Hispanic White, or Hispanic (of any race). The 2006 wave was the baseline occasion because it was the first wave in which all of the religious involvement measures were administered to a large proportion of participants. Participant characteristics (N = 16,069) are provided in Table 1. Participants provided written informed consent. Study procedures were approved by the University of Michigan Institutional Review Board.
Participant Characteristics at Baseline, Expressed as Mean (Standard Deviation) Unless Otherwise Specified.
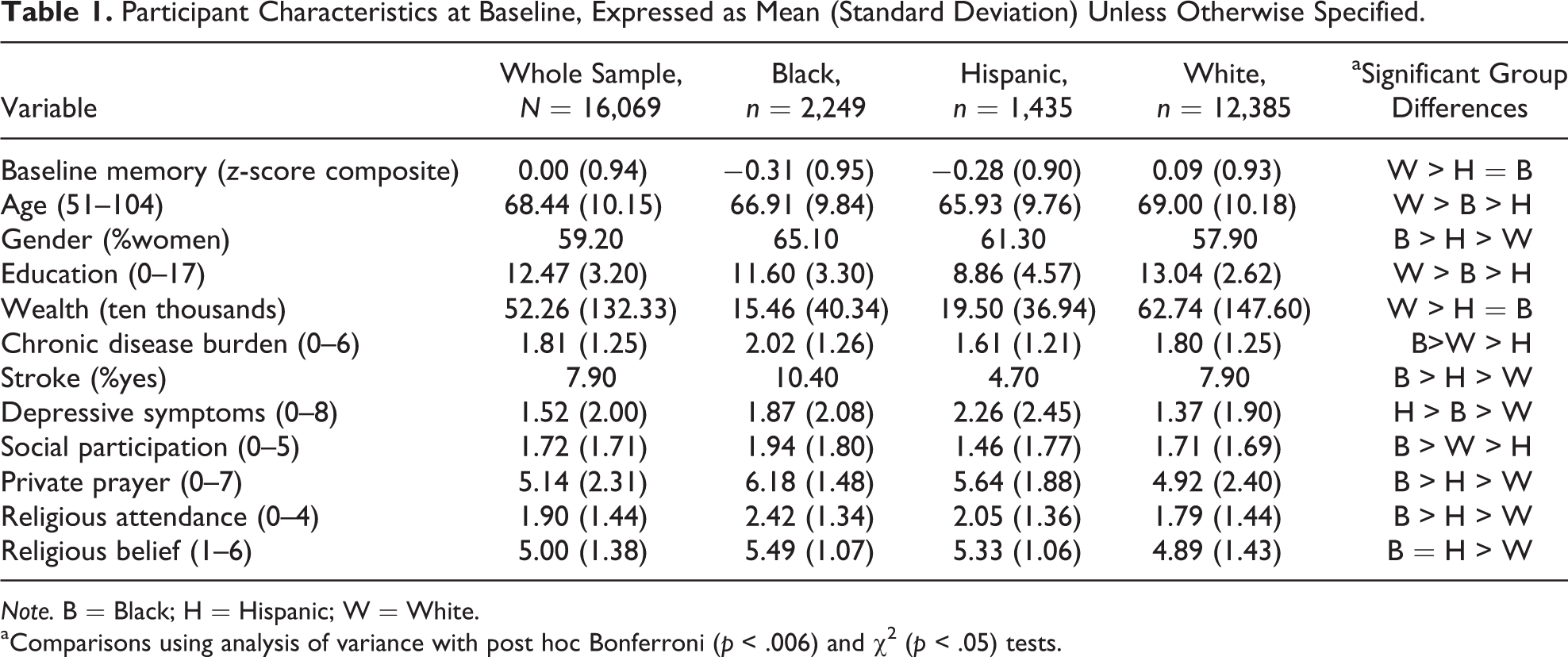
Note. B = Black; H = Hispanic; W = White.
aComparisons using analysis of variance with post hoc Bonferroni (p < .006) and χ2 (p < .05) tests.
Measures
Outcome variables
Memory
Episodic memory was selected as our measure of cognitive performance because it is sensitive to age-related cognitive decline and is a well-documented primary determinant of dementia risk (Backman, Small, & Fratiglioni, 2001). Episodic memory was assessed longitudinally across the four waves (2006–2012) with a list learning task, which is routinely used to assess episodic memory (Lezak, 1995; Rabin, Barr, & Burton, 2005). In the HRS, participants hear a list of 10 words and recall the words immediately and after a 5-min delay. A z-score composite was computed from raw scores on both trials using means and standard deviations from the baseline (2006) wave.
Predictors of interest
Race and ethnicity
Race and ethnicity were assessed via self-report. The three categories of non-Hispanic Black, non-Hispanic White, and Hispanic (of any race) were dummy-coded. Non-Hispanic White was the reference group.
Religious attendance
Frequency of attending religious services over the past year was assessed with the question “About how often have you attended religious services during the past year?” This measure was coded with responses ranging from 0 (not at all) to 4 (more than once a week). The HRS selected this item based on workgroup recommendations for measuring religious involvement in health research (Levin, 2003).
Private prayer
Frequency of private prayer was assessed with the question “How often do you pray privately in places other than at church or synagogue?” This measure was coded with responses ranging from 0 (never) to 7 (more than once a day). The HRS selected this item based on workgroup recommendations for measuring private religious practices in health research (Levin, 2003).
Religious belief
Religious belief in the HRS was assessed with 4 items selected based on workgroup guidelines for measuring religious belief in health research (Fetzer Institute, 2003). Items included “I believe in a God who watches over me” and “The events in my life unfold according to a divine or greater plan.” Responses ranged from 1 (strongly disagree) to 6 (strongly agree). Scores were averaged, and higher values correspond to stronger religious belief. Cronbach’s α in the HRS was .92.
Nonreligious social participation
Frequency of nonreligious social participation was assessed with the question “Not including attendance at religious services, how often do you attend meetings or programs of groups, clubs, or organizations that you belong to?” This measure was coded with responses ranging from 0 (never) to 5 (more than once a week). For simplicity, this variable will be shortened to “social participation” henceforth. This social participation measure was selected because it captures respondents’ general or trait-like social engagement outside of religious involvement, which could reflect a confounder of associations between certain religious involvement variables (e.g., religious attendance) and cognition. Bivariate correlations among the religious involvement and social participation variables demonstrated significant associations (Supplementary Table 1).
Covariates
Sociodemographics
Age was participants’ age at the baseline wave. Sex was dichotomized, with male as the reference category. Education was years of education (0–17). Baseline wealth was the sum of assets (e.g., stocks, bonds) minus debts (e.g., loans, mortgages). These sociodemographic variables were selected as covariates because they are major contributors to cognition and represent life-course determinants of racial and ethnic inequalities in cognitive aging (for a review, see Glymour & Manly, 2008).
Physical health
Chronic disease burden at baseline was the sum of the self-reported presence of diabetes, cancer, lung disease, heart problems, hypertension, and arthritis. Prevalent stroke at baseline was dichotomized, with absence of stroke as the reference category. As previously recommended (Hill, 2008), physical health was included as a covariate to control for possible health-related selection effects.
Depressive symptoms
Depressive symptoms over the past week were assessed at baseline with 8 items from the Center for Epidemiologic Studies Depression Scale (Radloff, 1977) modified into a yes/no format. Higher scores correspond to more depressive symptoms. As previously recommended (Hill, 2008), depressive symptoms were included as a covariate to control for possible mental health–related selection effects.
Analytic Strategy
χ2 tests and analysis of variance with Bonferroni correction compared race and ethnicity groups. Structural equation models (SEM) using latent growth curve analysis with maximum likelihood estimation quantified memory trajectories from 2006 to 2012. Time was parameterized as years from the 2006 assessment wave. Participants had an average of 3.4 time points of data (range: 1–4). Missing data were managed with full information maximum likelihood.
The first hypothesis was tested using a single SEM to estimate the direct and indirect effects between race and ethnicity and memory trajectories through three independent pathways: religious attendance, private prayer, and religious belief. In this SEM framework, “indirect effects” reflect the product of all coefficients within a given pathway from race/ethnicity to memory through religious involvement variables, independent of all covariates. “Direct effects” reflect associations between race/ethnicity and memory, independent of other variables (i.e., predictors and covariates). “Total effects” are the sum of indirect and direct effects. To restate our hypotheses, a positive “indirect effect” through religious involvement would decrease the magnitude of a negative “direct effect” to determine the “total effect” of race or ethnicity on cognition. Two latent variables were estimated: initial memory performance (intercept) and rate of memory change over the 6-year follow-up (linear slope). Memory intercept and slope were each regressed onto the three religious involvement variables, race, and ethnicity, and covariates. The three religious involvement variables were regressed onto race, ethnicity, and covariates (Figure 1).
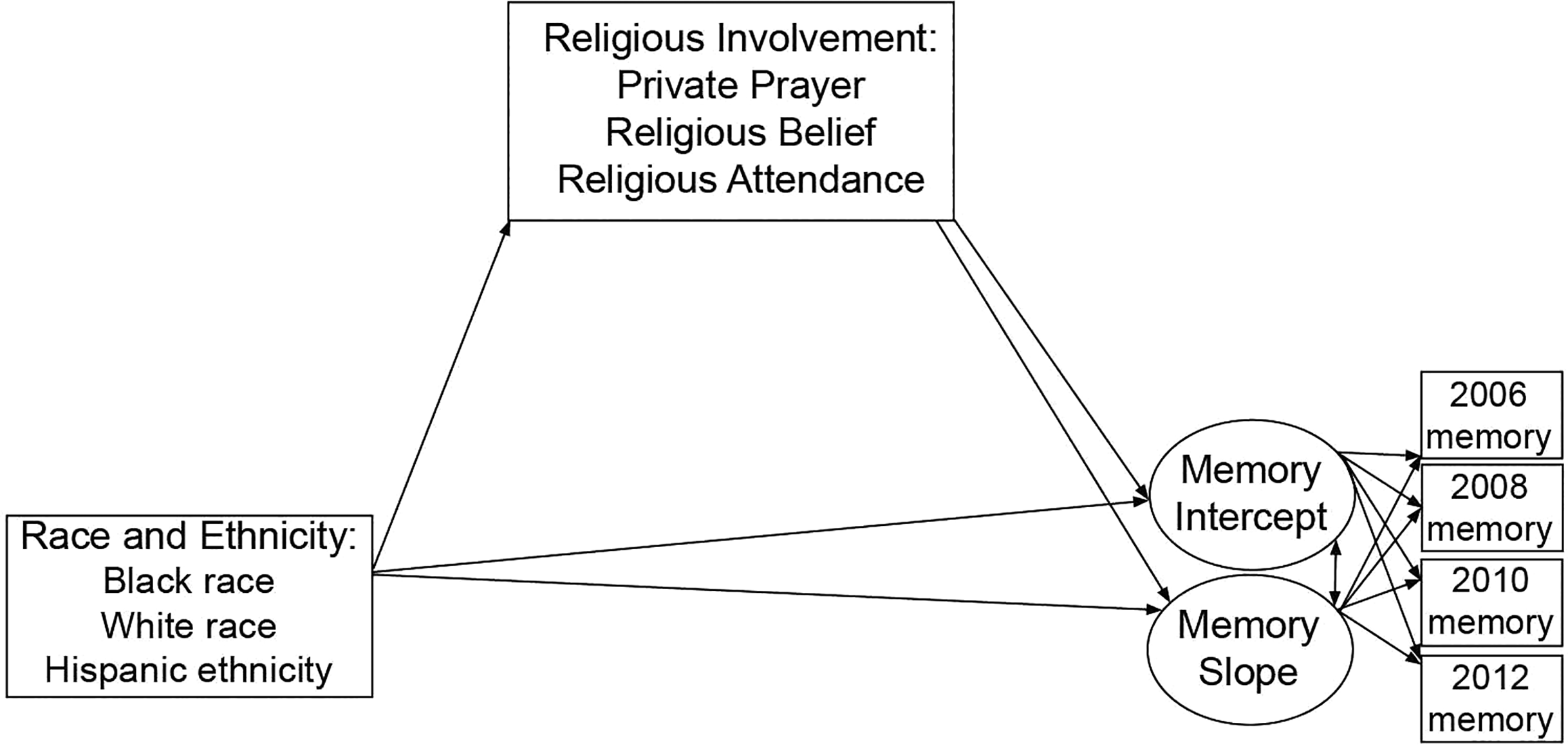
Schematic of direct and indirect paths estimated in the structural equation model. For simplicity, the figure does not depict covariates or independent pathways through each religious involvement variable.
The second hypothesis was tested in a subsequent SEM. Specifically, social participation was included as a separate predictor to determine whether religious involvement was associated with the memory outcomes independent of participants’ general or trait-like sociability.
Next, a series of sensitivity analyses were conducted. First, due to mixed evidence regarding whether associations between religious involvement and health outcomes vary by race or ethnicity, we tested whether findings from our core analyses (i.e., Hypotheses 1 and 2) remained when allowing for the possibility of effect modification by race and ethnicity (Valeri & VanderWeele, 2013). Independent interaction terms for each predictor variable were computed separately for Black race and Hispanic ethnicity. Second, because the HRS was designed to include respondents and their spouse from sampled households, associations may be subject to bias related to nonindependence of observations. Thus, analyses were conducted using only one randomly selected respondent per household. Finally, because immigration status could be related to religious involvement and health, we conducted a third set of sensitivity analyses in a restricted sample of U.S.-born participants only.
Model fit was evaluated using comparative fit index (CFI), root mean square error of approximation (RMSEA), and standardized root mean square residual (SRMR). CFI > .95, RMSEA < .06, and SRMR < .05 determined adequate model fit (Hu & Bentler, 1999). Unstandardized effects are provided below. Standardized effects are provided in supplementary tables (Supplementary Table 2).
Results
Participant Characteristics
There were group differences in participant characteristics (Table 1). Specifically, in comparison to White participants, both Black and Hispanic participants were more likely to be older and female, had fewer years of education and less wealth, were more likely to have experienced a stroke, and reported more depressive symptoms at baseline.
Black participants reported more religious attendance, social participation, and private prayer than Hispanic and White participants. Hispanic participants reported more religious attendance and private prayer, but less social participation, than White participants. Both Black and Hispanic participants reported more religious belief than White participants.
Hypothesis 1: Pathways From Race and Ethnicity to Memory Trajectories via Religious Involvement
The initial SEM fit very well: CFI = .992, RMSEA = .024 (90% CI [.021, .026]), SRMR = .012. There were significant negative direct effects of Black race and Hispanic ethnicity on initial memory performance, relative to non-Hispanic Whites (Table 2; Figure 1). These negative direct effects were attenuated by the positive indirect effects through two religious involvement dimensions: private prayer and religious attendance.
Unstandardized Results From a Single Structural Equation Model (Hypothesis 1).
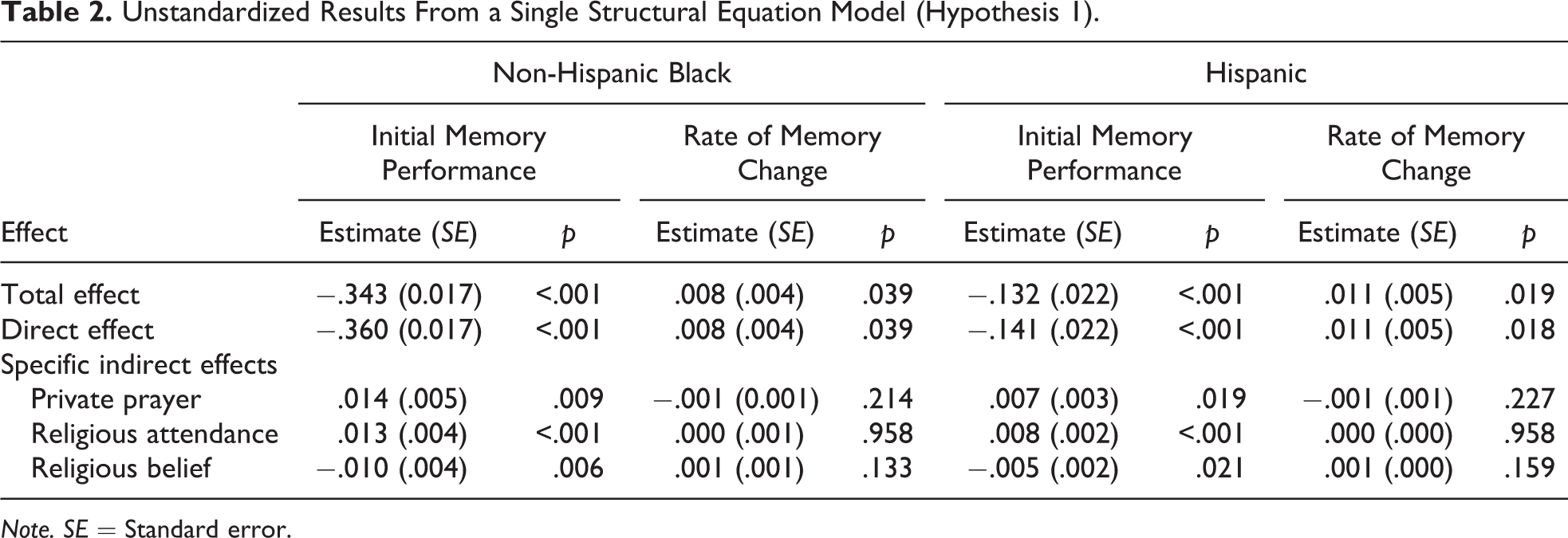
Note. SE = Standard error.
Initial memory performance
Both Black (B = .997; SE = .074; p < .001) and Hispanic (B = .492; SE = .098; p < .001) participants reported more private prayer than non-Hispanic White participants. In turn, more private prayer was associated with better initial memory performance (B = .014; SE = .005; p = .007).
Independent of private prayer, both Black (B = .661; SE = .033; p < .001) and Hispanic (B = .370; SE = .042; p < .001) participants reported more religious attendance than non-Hispanic White participants. More religious attendance, in turn, was associated with better initial memory performance (B = .020; SE = .005; p < .001).
Independent of private prayer and religious attendance, Black (B = .440; SE = .047; p < .001) and Hispanic (B = .222; SE = .062; p < .001) participants reported more religious belief, which was associated with lower initial memory performance (B = −.023; SE = .008; p = .004).
Rate of memory change
There were positive direct effects of Black race and Hispanic ethnicity on memory slope. Black and Hispanic participants exhibited slower memory decline than non-Hispanic Whites (Table 2). There were no indirect effects of Black race or Hispanic ethnicity on memory slope.
Hypothesis 2: Religious Involvement Pathways Independent of Social Participation
In a subsequent SEM, nonreligious social participation was added to the model (Table 3). The model fit well, CFI = .987; RMSEA = .028 (90% CI[.026 to .030]); SRMR = .019. Magnitudes of associations between variables were somewhat attenuated; however, all patterns of association were similar to those in the initial model (Table 3).
Unstandardized Results From a Single Structural Equation Model Controlling for Social Participation (Hypothesis 2).
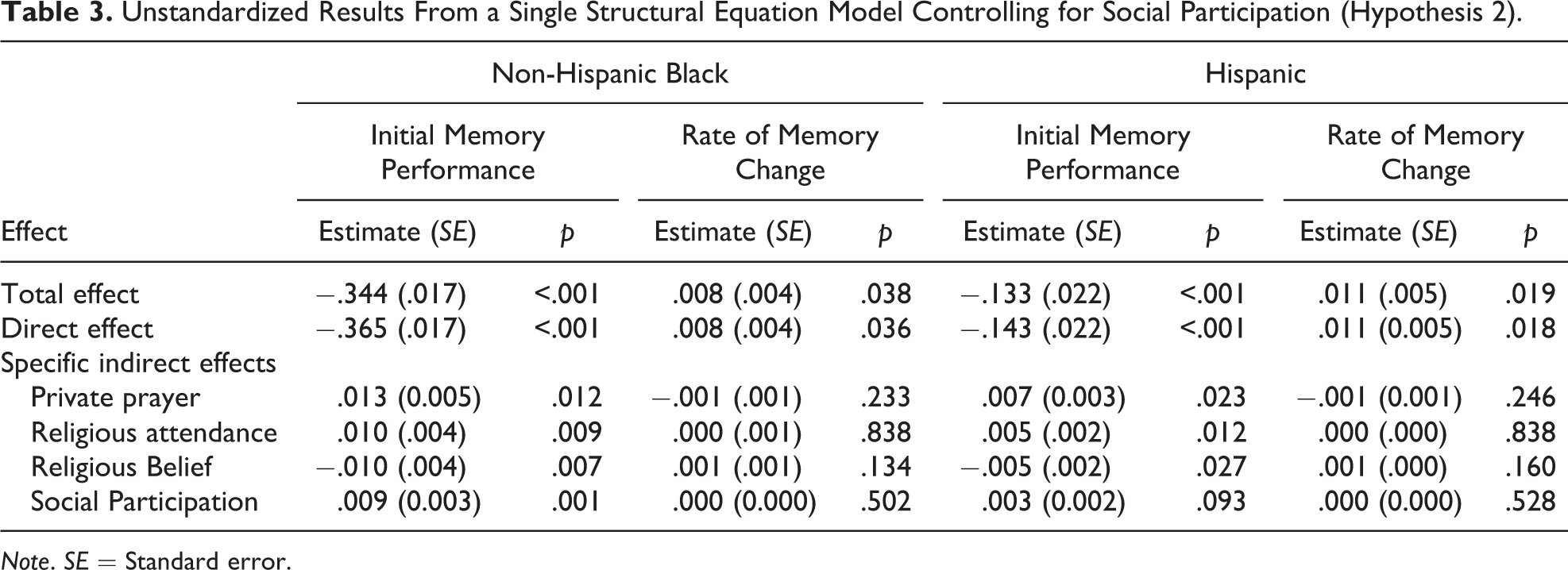
Note. SE = Standard error.
Sensitivity Analyses
Subsequent models tested a series of three sensitivity analyses (Supplementary Table 3). First, models included interaction terms to allow for the possibility that associations between religious involvement and memory vary by race or ethnicity. All models fit well, and the magnitude and pattern of direct and indirect pathways to memory trajectories were largely similar with the exception of the indirect effect of Black race on initial memory through religious attendance. However, the interaction term was not significant, demonstrating that the race did not moderate the association between religious attendance and initial memory. Second, we randomly selected one respondent per household for inclusion in our core analyses (n = 10,633) to address potential concerns about nonindependence of observations due to the HRS household sampling strategy. All models fit well, with similarly sized effects in comparison to the primary models, though the smaller sample in these sensitivity analyses was not adequately powered to detect all effects. Third, we restricted the sample to participants who were born in the United States (n = 14,594). The models fit well, with similarly sized effects and identical patterns of significant associations.
Discussion
Findings of this nationally representative longitudinal study integrated and extended previous research by demonstrating that the magnitude of racial and ethnic inequalities in episodic memory is partially offset by older Black and Hispanic adults’ greater religious involvement. Furthermore, this study documented independent, positive pathways to initial memory performance through two different dimensions of religious involvement, religious attendance and private prayer (Hypothesis 1), that persisted after controlling for general social participation (Hypothesis 2).
In the whole sample, more frequent religious attendance was associated with better initial memory performance, independent of social participation. The current study’s finding on memory performance extends previous research that controlled for social support (Corsentino et al., 2009), social engagement (Van Ness & Kasl, 2003), and social networks (Yeager et al., 2006). The fact that the association between religious involvement and memory was independent of nonreligious social participation helps to rule out the possibility that it was driven entirely by individuals’ inclination or ability to participate in community activities outside the home. However, in line with the theory of social engagement, the mechanism underlying the association between religious involvement and memory may still involve some social resources obtained through religious service attendance (Bassuk et al., 1999). Indeed, recent findings suggest that positive social engagement with religious peers may reduce psychological distress (Nguyen et al., 2018), and psychological distress is known to have negative effects on cognitive functioning (Paterniti, Verdier-Taillefer, Dufouil, & Alpérovitch, 2002). Religious attendance may also be linked to better cognitive health above and beyond its social benefits because it involves additional, uniquely stimulating cognitive activities including discussions of sermons and/or applications of scriptural study (Corsentino et al., 2009; Hill, 2008; Van Ness & Kasl, 2003).
Independent of religious attendance, private prayer was also associated with better initial memory performance. The current study’s finding on memory performance is consistent with previous cross-sectional research demonstrating that prayer in midlife reduces the risk of mild cognitive impairment among older Arabic women (Inzelberg et al., 2013) but contrasts cross-sectional research among older Taiwanese adults demonstrating no association (Yeager et al., 2006). However, the latter study investigated a composite of multiple religious practices beyond prayer frequency, including more passive activities (e.g., watching and listening to religious programs) and context-specific prayer (e.g., before making important decisions). One potential mechanism underlying a positive association between private prayer and memory may involve its meditation/relaxation benefits. Meditation and relaxation reduce physiological stress (Seeman et al., 2003), which in turn can help maintain cognitive function (Crowther et al., 2002). Another potential mechanism may be that the procedural aspects of prayer are cognitively demanding. Specifically, episodic memory may be required to recall prayer content (i.e., words), target (i.e., people to pray for), and purpose (i.e., reasons for prayer). Exercising these cognitive skills may have long-term benefits for cognitive aging (e.g., “use it or lose it”; Hultsch, Hertzog, Small, & Dixon, 1999).
While extant research has documented positive associations between religious belief and physical health (Ellison & Levin, 1998; Levin, Chatters, et al., 1995; Seeman et al., 2003; Taylor et al., 2004) in the current study, religious belief was inversely associated with cognition, consistent with previous cognitive health research (Ritchie et al., 2014; Zuckerman et al., 2013). Individuals with lower cognition may utilize religious belief to obtain self-control and self-enhancement attributes that may be more readily obtained through alternate means by individuals with more cognitive resources (Zuckerman et al., 2013). Additionally, greater religious belief may reflect more use of intuitive processes rather than analytic cognitive processes (Gervais & Norenzayan, 2012). The contrasting directions of associations with memory involving religious attendance and private prayer (i.e., positive) versus religious belief (i.e., negative) may reflect differences in the cognitive demands of these different dimensions of religious involvement. Specifically, in contrast to the memory demands of behaviors such as religious attendance (e.g., recalling sermons and interacting with fellow attendees) and private prayer (e.g., recalling specific prayers, who to pray for, and what to pray about), religious beliefs may not actively recruit memory-related processes. Given that religious belief is positively associated with multiple physical health outcomes (Ellison & Levin, 1998; Levin, Chatters, et al., 1995; Seeman et al., 2003; Taylor et al., 2004), research is needed to better understand its inverse association with cognition. Future studies should additionally examine whether regional or other differences in religious belief may influence its association with cognitive health.
Independent of predictors and covariates, Black race and Hispanic ethnicity were associated with lower initial memory, highlighting well-documented inequalities in the level of cognition in these groups (Manly & Mungas, 2015). Importantly, independent positive pathways through two dimensions of religious involvement partially offset or attenuated racial and ethnic differences in initial memory. The current study’s inclusion of a racially and ethnically diverse sample addresses a key gap in research on religion and cognitive aging, as previously described (Hill, 2008), extending previous research that comprised samples of Hispanic-only (e.g., Hill et al., 2006; Reyes-Ortiz et al., 2008) or Black and White (e.g., Corsentino et al., 2009) older adults. Specifically, our findings suggest a target for intervention development to reduce cognitive inequalities among minority older adults who endorse religious practice. Greater religious involvement among Black and Hispanic older adults suggests that interventions targeting religious involvement may be particularly feasible and culturally relevant for Black and Hispanic individuals due to these higher levels of naturally occurring religious involvement. While it is not ethical to prescribe religion in a clinical setting, religious involvement may represent a target in interventions for those who already endorse religious practice.
The current study’s finding that Black race and Hispanic ethnicity were associated with a slower rate of memory decline was unexpected yet parallels the inconsistent associations between race and ethnicity and memory decline. Specifically, while some studies have found that Black and/or Hispanic older adults demonstrate greater memory decline relative to non-Hispanic White counterparts (Gross et al., 2015), our findings are in line with contrasting research that has documented opposite findings (Early et al., 2013; Wilson, Capuano, Sytsma, Bennett, & Barnes, 2015) or no racial or ethnic associations with rates of decline (Carvalho et al., 2015; Weuve et al., 2018). These inconsistencies may be due differences in selection, literacy, region of origin, acculturation, residence in ethnic enclaves, and generational status across samples, highlighting the critical need for additional research to characterize factors contributing to change in minority cognitive aging.
In the current study, dimensions of religious involvement were associated with initial memory level but not rate of memory change. As with all cross-sectional findings, we are unable to rule out concerns regarding reverse causality. However, this study’s finding is similar to previous research showing smaller effects of social variables on cognitive change versus level (Manly & Mungas, 2015) as well as nonsignificant associations between religious involvement and cognitive change (Hosseini et al., 2017; Zuckerman et al., 2013). It is possible that having a longer follow-up would have yielded greater memory decline, as well as greater individual variability in decline, and revealed associations between religious involvement and memory trajectory. Future research should employ time-series modeling using life-course data to clarify the direction of associations and causal processes. It should be noted that associations with initial cognitive level in the absence of association with cognitive change may still have implications for dementia risk. Specifically, individuals who start at a higher cognitive level will take longer to reach a dementia threshold even if they decline at the same rate as individuals who start at a lower cognitive level. Microsimulation studies demonstrate that delaying the onset of dementia by 5 years would almost halve its prevalence (Zissimopoulos, Crimmins, & St Clair, 2015). Thus, identifying modifiable factors related to level of episodic memory performance, a key determinant of dementia risk, may have important implications for cognitive aging.
This study’s limitations include its inability to definitively conclude the direction of the cross-sectional associations, brief cognitive assessments, self-reported physical health, and single-item religious attendance, private prayer, and social participation variables. Additionally, although the social participation measure specifically queries attendance of “nonreligious” activities, it may not fully capture the breadth of respondents’ general social participation. Future studies should replicate results using comprehensive assessments and objective health measures. Future studies could also examine religious affiliation subgroups, which was not feasible in the current study due to low variability in religious affiliations.
Major strengths of the current study include modeling three dimensions of religious involvement within a single model. We also included nonreligious social participation to control for older adults’ tendency or ability to participate in community activities and examined three racial and ethnic groups. That magnitudes and patterns of associations remained largely similar across a thorough set of sensitivity analyses provide empirical support for the robust nature of findings doucmented in the current study. Additionally, this study extends previous findings on context-specific prayer (Yeager et al., 2006) by testing the contribution of typical prayer behavior regardless of context. Other strengths include using longitudinal data in a large, nationally representative sample of older adults and a comprehensive set of covariates.
Conclusion
Altogether, the current longitudinal study supports the positive effects of private prayer and religious attendance on cognitive health and highlights how older Black and Hispanic adults may benefit from their naturally occurring high levels of religious involvement. Results may inform the development of strengths-based, culturally relevant interventions that promote successful aging and reduce inequalities in the level of cognition among racially and ethnically diverse older adults who endorse religious involvement. Findings from the current study also support previous work demonstrating that social engagement and private meditative prayer more broadly may be beneficial for cognitive health outcomes.
Supplemental Material
Supplementary_Table_1_RoA - Dimensions of Religious Involvement Represent Positive Pathways in Cognitive Aging
Supplementary_Table_1_RoA for Dimensions of Religious Involvement Represent Positive Pathways in Cognitive Aging by A. Zarina Kraal, Neika Sharifian, Afsara B. Zaheed, Ketlyne Sol and Laura B. Zahodne in Research on Aging
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes on Aging [Grant Numbers R00AG047963 and R01AG054520]. The HRS (Health and Retirement Study) is sponsored by the National Institute on Aging (grant number NIA U01AG009740) and is conducted by the University of Michigan. The sponsor had no role in the current analyses or the preparation of this paper.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.