
Abstract
This study provides one of the first population-based investigations of the longitudinal association between social isolation and sleep difficulty among older adults in China. We analyzed three waves of longitudinal data from the China Longitudinal Aging Social Survey (2014–2018), in which 8456 respondents contributed 16,156 person-year observations. Results from multilevel logistic regression models showed that social isolation was related to a higher risk of sleep difficulty. We also found that socially isolated older adults were more likely to report higher levels of depressive symptoms, a greater prevalence of loneliness and pain, and more chronic diseases compared to their socially integrated counterparts, which in turn increased their risks of sleep difficulty. Moreover, socially isolated older adults with chronic diseases were particularly vulnerable to the risk of sleep difficulty. These findings provide helpful guidance for policymakers and practitioners to design effective intervention strategies to help older adults with sleep problems.
Introduction
Sleep is one of the most important restorative behaviors for individuals’ daily functioning, health, and well-being (Buysse, 2014; Miner & Kryger, 2020). Sleep patterns change with age, and older adults are more vulnerable to various sleep problems than their younger counterparts (Crowley, 2011). It has been estimated that nearly half of older adults complain about difficulty initiating or maintaining sleep around the world (Crowley, 2011; Neikrug & Ancoli-Israel, 2010). Studies using a variety of data have consistently shown many psychological and physiological determinants of sleep, such as depression, anxiety, loneliness, chronic diseases, and bodily pain (Benson et al., 2021; Cacioppo et al., 2002; Cho et al., 2019; Foley et al., 2004; Karayannis et al., 2019; McHugh et al., 2011; Smagula et al., 2016).
Recently, there is emerging literature studying the role of social relationships in influencing sleep, with the main focus on the importance of family ties, such as spousal and intergenerational relationships (Chen et al., 2015; Wang et al., 2020, 2021). Beyond family members, older adults’ well-being is further conditioned on larger social networks surrounding them, including extended family members and friendship ties. Isolation from social relationships has been found to be detrimental for a range of physical and mental health outcomes, including cardiovascular disease, depression, anxiety, and mortality (Holt-Lunstad et al., 2015; Leigh-Hunt et al., 2017; National Academies of Sciences, Engineering, and Medicine, 2020). Despite the importance of social relationships in later life, how the isolation from family and/or friendship ties may influence the sleep difficulty of older adults is less studied, and even less has been done to explore potential mechanisms linking social isolation and sleep difficulty in non-Western social contexts like China.
Using data from the China Longitudinal Aging Social Survey (CLASS, 2014–2018), we provide one of the first population-based longitudinal studies investigating the association between social isolation and sleep difficulty among older adults in China. We address three major research questions: (1) does the risk of sleep difficulty in later life vary by older adults’ social isolation status experienced in daily life? (2) to what extent are the associations between social isolation and sleep difficulty mediated by the psychological and physical well-being of older adults? and (3) do existing psychological and physical problems exacerbate the association between social isolation and sleep difficulty? We extend the existing literature on associations between relationships with particular family members and sleep difficulty by incorporating older adults’ social relationships with broader social networks. Our findings of pathways linking social isolation and sleep difficulty will help health policymakers and practitioners identify intervention opportunities to enhance the welfare of socially isolated older adults with sleep problems.
Social isolation and sleep in later life
Previous studies have provided both theoretical perspectives and empirical evidence on the associations between social isolation and various health outcomes (for reviews, see Holt-Lunstad et al., 2015; Leigh-Hunt et al., 2017). A recent advance in this line of research has been devoted to the link between social isolation and sleep in old age (Benson et al., 2021; Cho et al., 2019; Miner & Kryger, 2020). Theoretically, from the stress process perspective (Pearlin & Bierman, 2013), isolation from various supportive relationships represents a primary source of stress for older adults, which may lead to more sleep problems. Meanwhile, the biological perspective posits that social isolation can reduce immune system functioning and increase the neuroendocrine dysregulation system, both of which can negatively affect sleep (Cacioppo & Hawkley, 2003; Leigh-Hunt et al., 2017).
According to the social convoy model (Antonucci et al., 2014), individuals go through the life course surrounded by different dimensions of social relationships (i.e., spouse, children, relatives, and friends), all of these social relationships combine to influence individuals’ health and well-being. Among limited prior research on social determinants of sleep in later life, studies focused primarily on how relationships with particular family members are associated with sleep. For example, a study in China revealed that older parents were less likely to report sleep difficulty when receiving financial support from their children and maintained emotionally close intergenerational relationships (Wang et al., 2020). Another study of older couples in the U.S. demonstrated that their sleep was closely associated with their relationships with spouses, with the prevalence of reporting troubled sleep being much higher among poor-quality marriages (Chen et al., 2015).
In comparison, less attention has been paid to the link between isolation from a broad range of social relationships (e.g., friends and extended kin) and sleep difficulty in later life. Relationships with friends or other nonkin social connections, for example, are based on shared interests or values, mutual trust, and advantages in satisfying companionship and social integration (Huxhold et al., 2014). Studies in both developed and developing countries have consistently provided evidence of the association between diverse social networks and favorable physical and mental health outcomes (Burr et al., 2020; Huxhold et al., 2014; Tang et al., 2020). However, only a few studies from Western societies have directly investigated the associations between isolation from social relationships beyond family and sleep health, suggesting that strain with friends or other nonkin relationships is related to higher odds of sleep difficulty (Chung, 2017; Kent et al., 2015). Drawing on previous literature and theoretical considerations, we suggest that older adults who are isolated from their social relationships (family/friendship ties) are more likely to suffer from sleep difficulty.
The Roles of Psychological and Physical Well-Being
Many studies have shown that isolated older adults suffer from a series of adverse health conditions and an increased risk of mortality (Holt-Lunstad et al., 2015; Leigh-Hunt et al., 2017). Another line of research has demonstrated that older adults’ health deficits are closely associated with undesirable sleep outcomes, including lower levels of sleep quality (McHugh et al., 2011), more insomnia symptoms (Benson et al., 2021), and poorer sleep efficiency (Cacioppo et al., 2002; Smagula et al., 2016). Adding to the existing literature on social relationships, health, and sleep, in this study, we explore the roles of psychological and physical well-being in connecting social isolation to sleep difficulty. Unlike previous studies which focus on the link between social relationships and individual well-being, and that between well-being and sleep separately, we argue that we need to examine how social isolation/integration and various health indicators may jointly influence sleep in later life.
The stress process model points out both psychological and physiological pathways through which social detachment undermines individuals’ well-being (Pearlin & Bierman, 2013). Social isolation from family members or friends may serve as a stressor that produces mental health problems, which in turn, leading to sleep difficulty (Cacioppo & Hawkley, 2003). The stress from social isolation can also lead to sleep difficulty by generating physiological dysfunction, such as sympathetic nervous system activation, increased cortisol secretion, and metabolic activation (Kahn et al., 2013).
Indeed, prior research has provided solid evidence on the negative consequences of social isolation for older adults’ psychological and physical well-being (Holt-Lunstad et al., 2015; Leigh-Hunt et al., 2017), including depressive symptoms (Cho et al., 2019), higher levels of loneliness (Cacioppo et al., 2002), chronic pain (Eisenberger et al., 2006), and cardiometabolic conditions (Foley et al., 2004). However, with just a few exceptions, previous studies rarely investigated whether and how various health indicators might explain or moderate the associations between social relationships and older adults’ sleep. For example, a recent study among U.S. older adults reported that depression significantly mediated the relationship between intergenerational relationships and insomnia symptoms, while the mediating effect of loneliness was not significant (Wang et al., 2021). To our best knowledge, no published research conducted such investigations in the context of China with longitudinal survey data.
It is also possible that poor psychological and physical well-being may exacerbate the identified linkage between social isolation and sleep outcomes. It is reasonable to assume that the more stressors people experience, the higher likelihood they would suffer from poor health and well-being. From the stress buffer perspective (Pearlin & Bierman, 2013), support from social networks may buffer the harmful impacts of stress from other domains, such as mental and physical illness. As such, older adults with problems in psychological or physical well-being may be especially vulnerable to the detrimental effects of social isolation on sleep outcomes. While bivariate associations between social isolation, psychological/physical well-being, and sleep have been well reported in previous research, few studies have attempted to address joint links among these three constructs, which we try to understand in this study.
The Context of China
This study focuses on China, which represents the largest aging population as well as one of the fastest-growing aging countries in the world (United Nations, 2019). According to the 2020 census, there were 190.6 million Chinese aged 65 years and older, or 13.5% of the entire population (National Bureau of Statistics of China, 2021). The number of older people aged 65 years or over is projected to reach 365.6 million by 2050, which represents 26.1% of the total population (United Nations, 2019). While the proportion of older adults who have sleep difficulty remains unclear, the available evidence suggests that, in general, a substantial proportion of older Chinese report sleep difficulty, ranging from 14 to 50% (Gu et al., 2010; Li et al., 2013). The high prevalence of sleep difficulty and the dramatic population aging urgently call for research to identify risk factors that may lead to sleep difficulty among Chinese older adults.
Compared to the burgeoning literature examining social determinants of general health in later life, relatively less attention has been paid by social scientists to understand Chinese older adults’ sleep problems and their social correlates. For example, social networks, including both family and friendship ties, are widely recognized as important predictors of physical and mental health among older adults (Burr et al., 2020; Tang et al., 2020). Similarly, the lack of such social connections, or social isolation, was closely associated with a higher risk of stroke incidence and cognitive decline among older Chinese (Yang et al., 2020; Zhou et al., 2019). Nevertheless, only a small number of studies have demonstrated the social correlates of sleep health, such as marital status and living arrangements (Gu et al., 2010; Li et al., 2013), and intergenerational relationships (Wang et al., 2020). No study to our knowledge has examined the relationship between isolation from social networks and sleep difficulty of older Chinese, as well as the complex interplay of psychological and physical well-being under the perceived association.
Research Hypotheses
Based on the theoretical implications and empirical findings outlined above, the current study develops and tests the following hypotheses in the context of China:
Socially isolated older adults have a higher risk of sleep difficulty than those who are not socially isolated.
The association between social isolation and sleep difficulty is partially accounted for by older adults’ psychological and physical well-being.
Existing psychological and physical problems further exacerbate the association between social isolation and sleep difficulty.
Research Design
This study used data from the CLASS conducted by the Renmin University of China (for details, see http://class.ruc.edu.cn/). The baseline survey was conducted in 2014 and follow-up surveys were conducted in 2016 and 2018. As a nationally representative data, the CLASS used a multistage stratified sampling strategy, with counties as primary sampling units and rural villages or urban communities in each county were randomly drawn as secondary sampling units. Households in each village or community unit were randomly selected using a mapping sampling method, and one older adult was selected from each household for a face-to-face interview.
The current study used all three waves of CLASS data with noninstitutionalized adults aged 60 years and older from 28 provinces, autonomous regions, and municipalities in mainland China. In order to strengthen the validity of self-reported measurements, CLASS asked each of the respondents five cognition-related questions which were drawn from the Mini-Mental State Examination (MMSE, see Folstein et al., 1975). The five cognitive questions were: “What is the date today?” “What is the name of the community (village)?” “What day is the national holiday?” “Who is the president of China?” and “What is the lunar year in this year?” Respondents who answered correctly on at least three proceeded to the self-reported questions, such as sleep difficulty, depressive symptoms, and loneliness. It is a widely used practice in clinical and epidemiological studies to decide whether respondents are cognitively suited to answering these questions (Tang et al., 2020; Wang et al., 2020; Wang et al., 2014). Approximately 20–26% of the sample across waves were excluded in this study as a result. These cognitively impaired older adults were more likely to be women, live in rural areas, and have lower socioeconomic status. As such, our results may not be generalized to cognitively impaired older people. Missing data, with the most missing cases for the household income (9.4%), were handled using the Multiple Imputation via Chained Equations with 10 generated multiply imputed data sets (White et al., 2011). The final analytic sample included 8456 community-dwelling respondents (contributing 16,156 person-periods) aged 60–98 in 2014 and had no signs of cognitive impairment at the time of interview.
Measures
Sleep difficulty
China Longitudinal Aging Social Survey measured sleep difficulty using a single item “Did you find it hard to sleep well during the last week?” The original responses were “no,” “sometimes,” or “always.” In line with previous research (e.g., Bassett & Moore, 2014; Kutner et al., 2001; Wang et al., 2020), sleep difficulty was coded as a dichotomous variable by combining “no” and “sometimes” to indicate no sleep difficulty as opposed to “always,” indicating sleep difficulty. Additional analyses using the original measure of sleep difficulty (considered as either continuous or ordinal variables) showed identical findings to those presented in our current paper.
Social isolation status
We used the Lubben Social Network Scale (LSNS-6; Lubben et al., 2006) to measure social isolation status. The LSNS-6 scale includes six items to assess the number of family members/friends the respondents see or hear at least once a month, feel at ease talking about private matters, and could call on for help. Each item ranged from 0 (none) to 5 (nine or more). The summed scores range from 0 to 30, with higher scores representing larger social networks (Cronbach’s alpha = .78). As recommended by previous research (Lubben et al., 2006), those with scores less than 12 were categorized as social isolation. Our measure of social isolation represents the functional dimension of social contacts and is one of the two most widely used indicators of social isolation along with the structural dimension of isolation (e.g., living arrangements, contact frequency, and social participation) (Huisman, 2021).
Psychological well-being
We included two variables to assess the psychological well-being of older adults: depressive symptoms and loneliness. Depressive symptoms were measured by a short form of the Center for Epidemiologic Studies Depression (CES-D) scale (Radloff, 1977). The scale included the feelings of happiness, enjoying life, pleasure, lonely, upset, useless, having nothing to do, poor appetite, and trouble sleeping. Respondents were asked how often they experienced these symptoms in the past week, ranging from 0 (none of the time) to 2 (most of the time). Following prior research (Wang et al., 2021), the sleep and loneliness items were dropped from the original scale to avoid overlapping. The final 7-item CES-D scale was summed (positive items were reverse coded), with a higher score indicating greater depressive symptoms (Cronbach’s alpha = .71; range: 0–14). Loneliness was assessed with a question: “How often do you feel lonely?” (1 = seldom/never, 2 = sometimes, and 3 = often/always). In line with previous research (Luo & Waite, 2014), we formed a dummy variable by grouping the categories “sometimes” and “often/always” indicating lonely as opposed to “seldom/never” indicating not lonely. This self-reported measure of loneliness has demonstrated solid validity and has been widely used in studies of Chinese older adults as well as other populations (Fokkema et al., 2012; Luo & Waite, 2014; Yang & Victor, 2008). It is also found to be highly correlated with another two widely used loneliness assessment tools, the De Jong Gierveld Loneliness Scale (De Jong Gierveld & Van Tilburg, 1999) and the UCLA Loneliness Scale (Russell, 1982).
Physical well-being
We analyzed two indicators of physical well-being: self-rated pain and chronic diseases. Self-rated pain was a dummy variable measured by whether the respondents felt any bodily pain during the last month (1 = yes, 0 = no). The variable of chronic diseases was created by summing up self-reported diagnoses of chronic illnesses, such as high blood pressure, diabetes, lung disease, and stroke (range: 0–16).
Covariates
Throughout the analyses, we controlled for a set of covariates previously shown to influence older Chinese’s sleep difficulty (Gu et al., 2010; Li et al., 2013; Wang et al., 2020). These variables included age (in years), gender 1 (1 = female, 0 = male), marital status (1 = married, 0 = not married), education (1 = secondary education or above, 0 = otherwise), annual personal income (logged), household registration status (hukou status) (1 = urban/non-agricultural hukou, 0 = rural/agricultural hukou), living arrangements (1 = living alone, 0 = living with others), number of children (range: 0–12), and household size (range: 1–17).
Analytic Strategy
We first calculated descriptive statistics of the study variables for the whole sample and by sleep difficulty status at baseline. Then, we used data from 2014, 2016, and 2018 waves of the CLASS and multilevel logistic regression models to estimate the longitudinal link between social isolation and sleep difficulty. A hierarchical strategy was used, where repeated observations (Level 1) were nested within respondents (Level 2). Odds ratios (ORs) and corresponding 95% confidence intervals (CI) were used to assess the direction and magnitude of relationships. We first examined the association between social isolation and sleep difficulty in Model 1. Then we added psychological and physical well-being separately (Models 2 and 3) to examine how the coefficient of social isolation changed after we held specific health variables constant, followed by the full model with all health indicators included (Model 4). In addition, to understand how social isolation and health conditions jointly shape sleep in later life, we added interactions terms between social isolation and four health indicators in Model 5. We conducted a variance inflation factor (VIF) test, and no multicollinearity was detected (no value greater than 2 in the full model). We also estimated a series of multilevel regression models to assess four health indicators as outcomes to study the associations between social isolation and psychological and physical well-being. We used multilevel linear regression models for the continuous outcomes (depressive symptoms and chronic diseases) and multilevel logistic regression models for the binary indicators (loneliness and pain).
It should be noted that in nested multilevel logit models, the change in the coefficient of key predictor (i.e., social isolation) cannot be straightforwardly attributed to the inclusion of confounding variables (i.e., health indicators) (Karlson et al., 2012). As noted by Winship and Mare (1984), coefficients in logit models are not directly comparable across nested models because the function fixes the error variance at an arbitrary constant, which may mask or underestimate the contribution of confounding factors. To address this problem, in this study, we adopted the Karlson–Holm–Breen (KHB) decomposition method (Karlson et al., 2012) to elaborate the specific contribution of each health indicator in explaining the relationship between social isolation and sleep difficulty. Karlson–Holm–Breen is a widely used decomposition method unaffected by potential biases resulting from model comparisons of nonlinear models (Karlson et al., 2012). It decomposes the total effect of a variable into direct and indirect effects. This method also allows for the calculation of the percentage of the main association between social isolation and sleep difficulty that can be explained by either psychological or physical well-being indicators.
Results
Descriptive Statistics of All Analytic Variables at Baseline, China Longitudinal Aging Social Survey 2014.
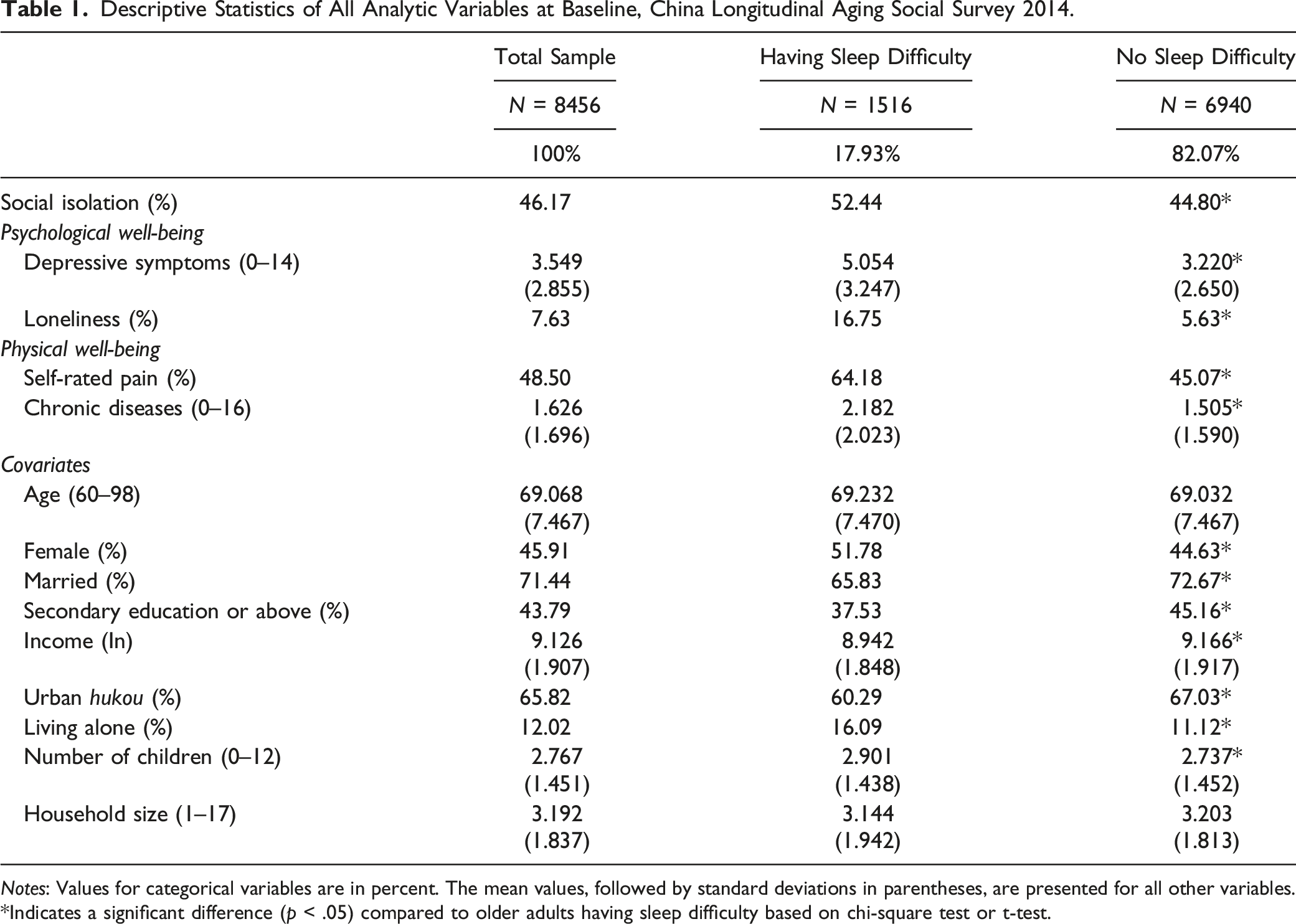
Notes: Values for categorical variables are in percent. The mean values, followed by standard deviations in parentheses, are presented for all other variables.
*Indicates a significant difference (p < .05) compared to older adults having sleep difficulty based on chi-square test or t-test.
Estimated Odds Ratios of Sleep Difficulty by Social Isolation and Health Status of Older Adults, China Longitudinal Aging Social Survey 2014–2018.
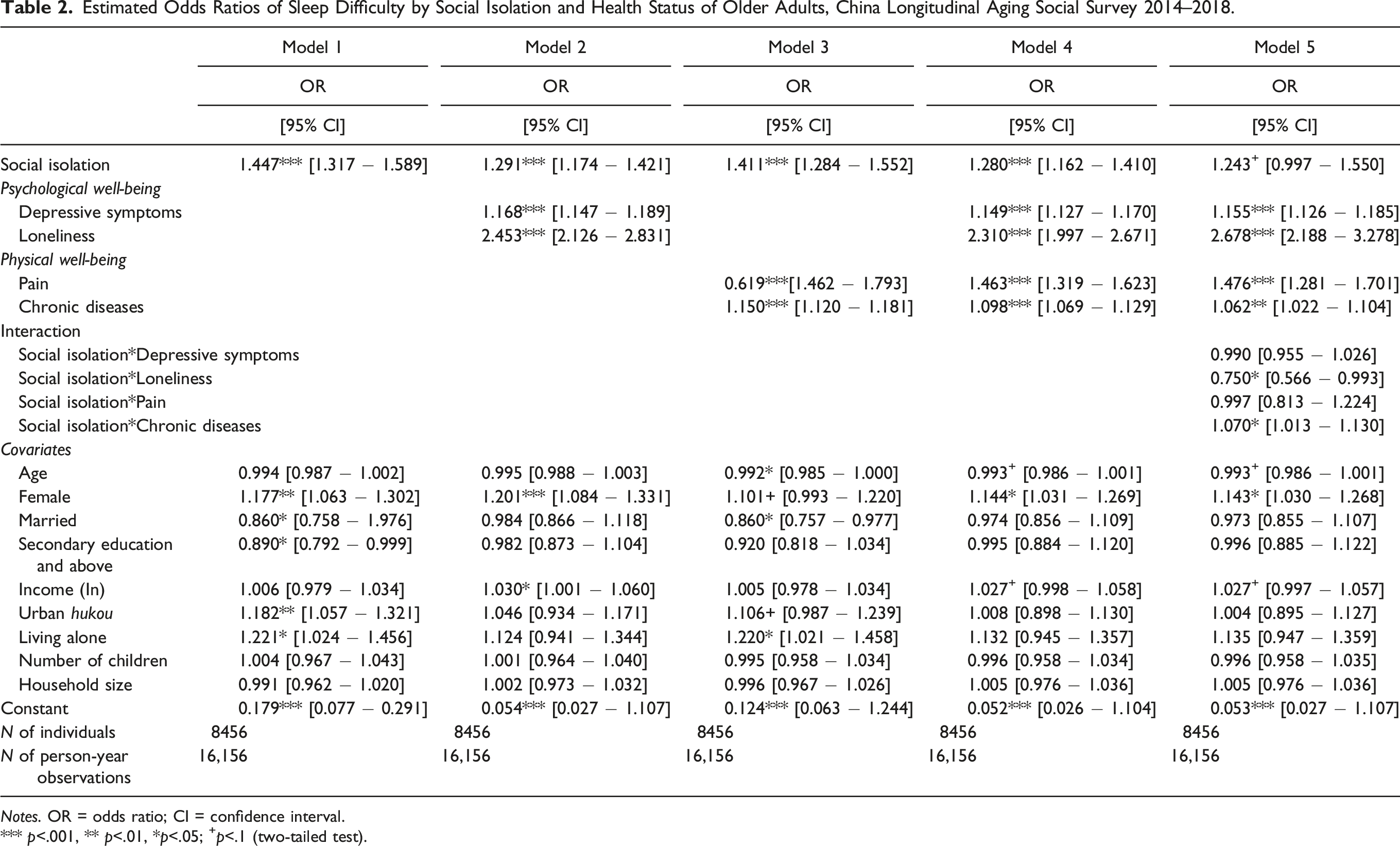
Notes. OR = odds ratio; CI = confidence interval.
*** p<.001, ** p<.01, *p<.05; +p<.1 (two-tailed test).
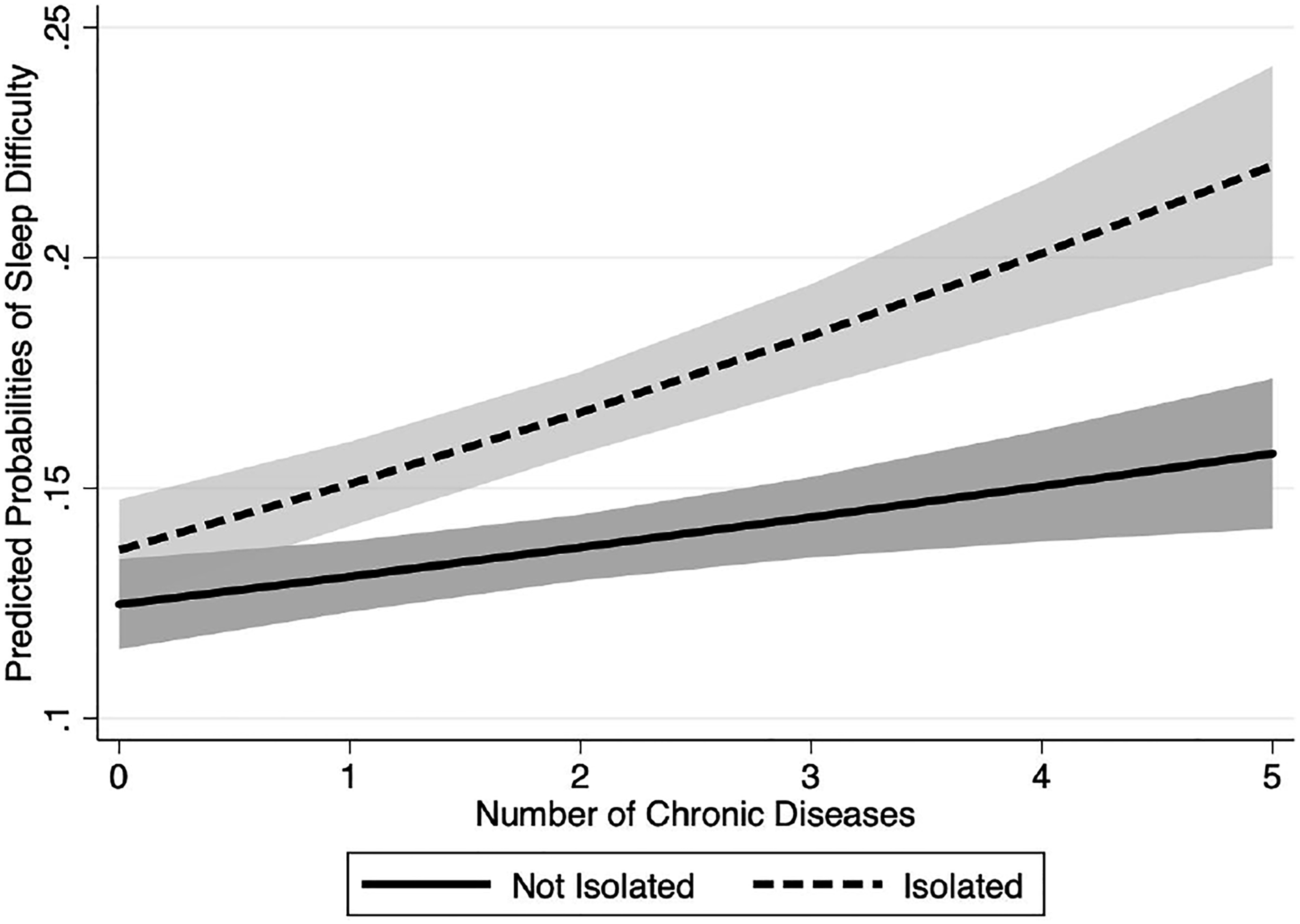
To aid interpretation, we presented predicted probabilities of sleep difficulty by isolation and loneliness status in Figure 1, and by isolation and chronic diseases in Figure 2, holding all other variables at their means (for continuous variables) and modes (for dummy variables). Figure 1 shows that older adults who felt lonely were exposed to a high risk of sleep difficulty, regardless of their social isolation status. Among those who did not feel lonely, socially isolated older adults had modest but significantly higher risks for sleep difficulty compared to those who were not isolated from their social relationships. Figure 2 shows increasing disadvantages for socially isolated older adults with multiple chronic diseases. We found that for older adults without any chronic diseases (about 30% of the sample), social isolation was not significantly associated with the risk of sleep difficulty (overlapping confidence intervals). However, as older adults suffered from more chronic diseases, those who were socially isolated experienced a sharp increase in their risks of sleep difficulty, while socially integrated older adults had relatively low risks of sleep difficulty, even for those with multiple chronic diseases. Predicted Probabilities of Sleep Difficulty (with 95% confidence intervals) by Social Isolation and Loneliness. Predicted Probabilities of Sleep Difficulty (with 95% confidence intervals) by Social Isolation and Chronic Diseases.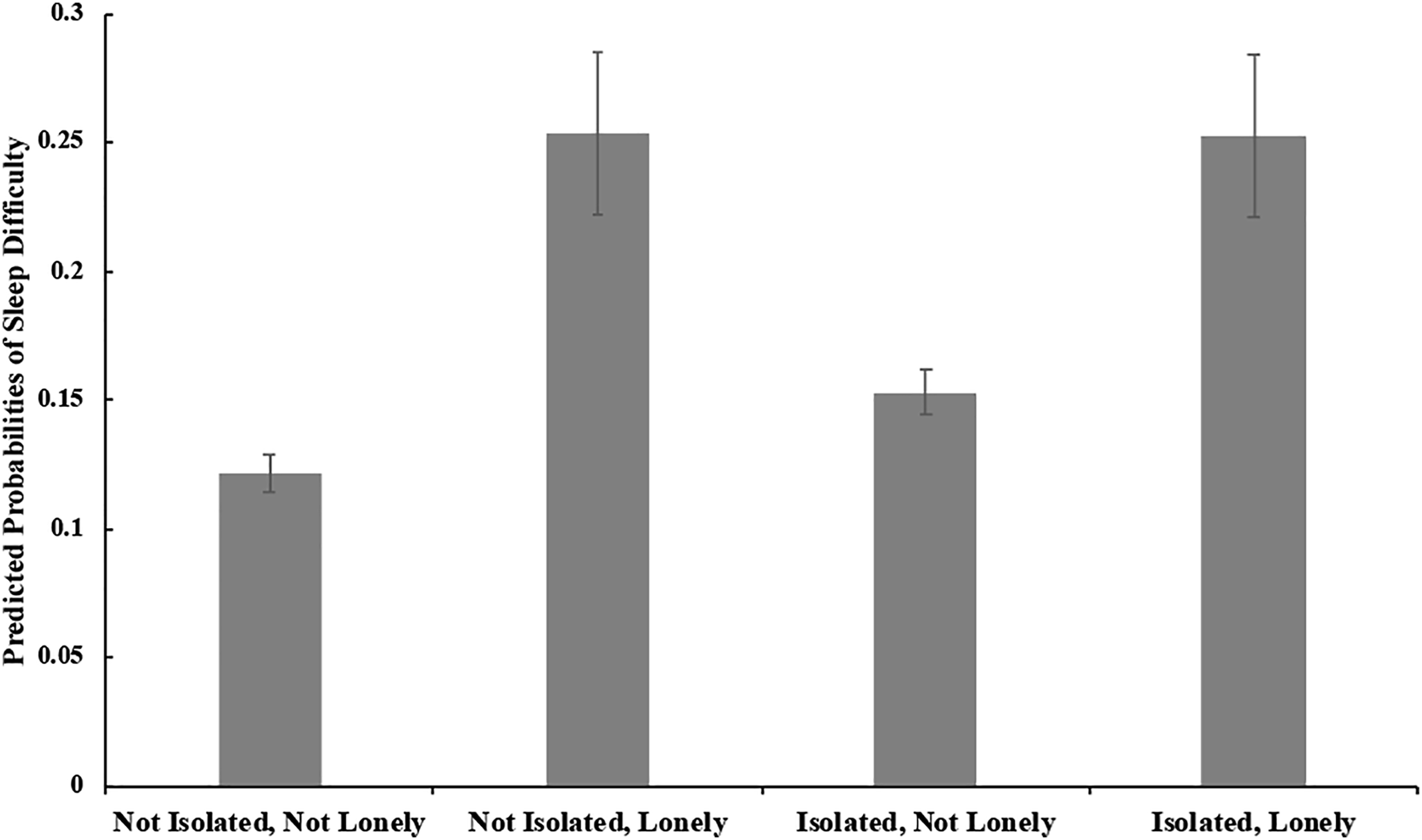
Multilevel Regression Models Predicting Psychological and Physical Well-Being of Older Adults, China Longitudinal Aging Social Survey 2014–2018.
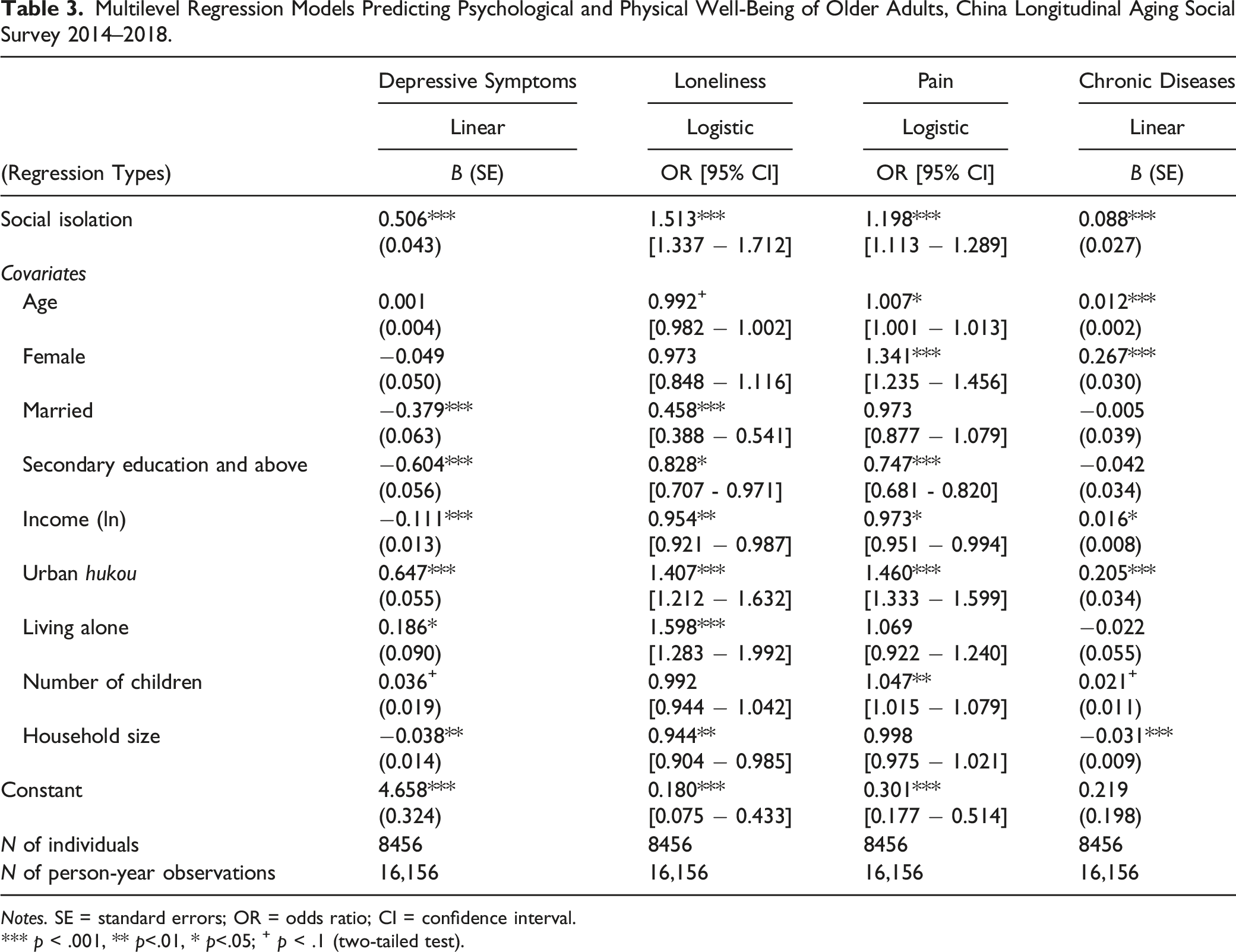
Notes. SE = standard errors; OR = odds ratio; CI = confidence interval.
*** p < .001, ** p<.01, * p<.05; + p < .1 (two-tailed test).
KHB Mediation Analysis Results of Psychological and Physical Well-Being, China Longitudinal Aging Social Survey 2014–2018.
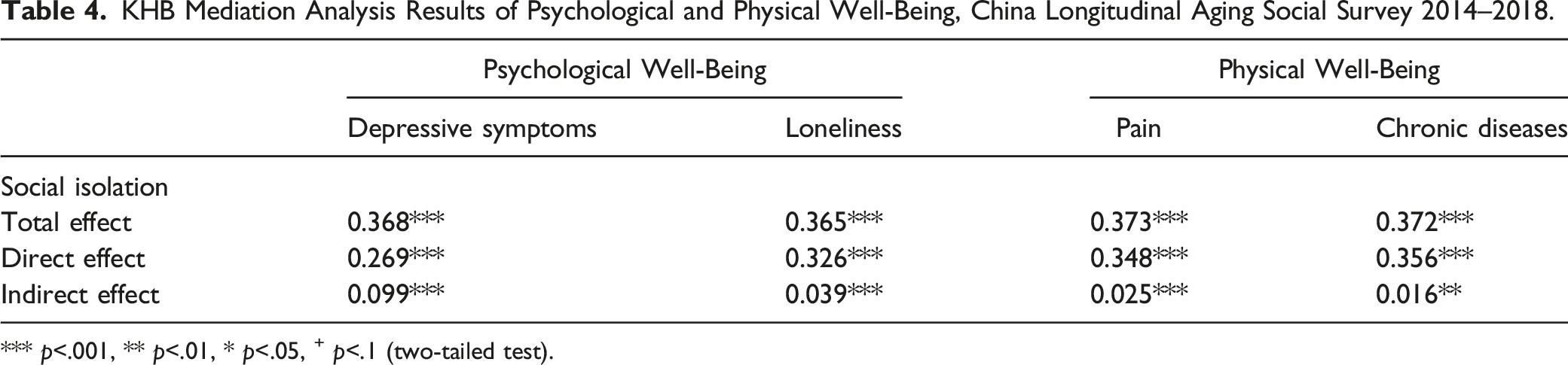
*** p<.001, ** p<.01, * p<.05, + p<.1 (two-tailed test).
Discussion
This study is among the first attempts to use nationally longitudinal data to examine the associations between social isolation and sleep difficulty, an essential but understudied behavioral health, in the context of the largest aging population in the world. Furthermore, we explore potential psychological and physiological pathways through which social isolation may be linked to the sleep outcome. The main findings and implications are discussed below.
First, we find clear evidence that isolation from social relationships (family/friendship ties) is an independent risk factor for sleep difficulty. These findings are consistent with Hypothesis 1 and are in line with the limited but developing literature on the topic of social relationships and sleep health in later life (Chen et al., 2015; Wang et al., 2020, 2021). By focusing on sleep health, this finding also joins and extends a growing body of literature showing the protective role of social networks on general health outcomes among Chinese older adults (Burr et al., 2020; Tang et al., 2020). According to the social convoy model (Antonucci et al., 2014), individuals go through life embedded in different circles of personal networks. Relationships with members of the inner circle (e.g., spouse and children) are more intense and have higher degrees of closeness than outer circles (i.e., extended kin and friends). In this regard, differential levels of density and duration experienced within social networks may be associated with sleep outcomes in different ways. Future research with more detailed information on multiple social relationships and sleep outcomes should continue to explore how older adults’ isolation from different types of relationships may have adverse impacts on their sleep health.
This paper also contributes to the literature by elucidating psychological and physical pathways responsible for the links between social isolation and sleep difficulty in later life. Our results indicate that socially isolated older adults were more likely to report higher levels of depressive symptoms, a greater prevalence of loneliness and pain, and more chronic diseases compared to their socially integrated counterparts, and all of these psychological and physical well-being indicators were found to be closely associated with the risk of sleep difficulty. Our formal mediation tests using the KHB method also confirm that depressive symptoms and loneliness, to a lesser degree, pain and chronic diseases, accounted for significant proportions of the link between social isolation and sleep difficulty, findings that support Hypothesis 2. These findings, therefore, highlight the importance of considering both psychological and physical well-being when trying to understand social determinants of sleep health in later life.
It should be noted that compared to psychological well-being, physical indicators played a less important role in explaining the social isolation and sleep difficulty associations. For example, as a sensitive barometer of population health and well-being (Zajacova et al., 2021), we have found that pain is closely associated with both social isolation and poor sleep outcomes. However, it only explains 6% of the association between social isolation and sleep difficulty. Similarly, we also expect that chronic diseases may be another important physical pathway for the connection between social isolation and sleep difficulty since prior studies have separately indicated the direct effect of social isolation on increased chronic diseases as well as the close associations between multiple chronic conditions and sleep outcomes (Foley et al., 2004; Leigh-Hunt et al., 2017). Contrary to our expectations, chronic diseases only explained 4% of the link between social isolation and sleep difficulty. In contrast, psychological well-being, especially depressive symptoms, have accounted for 27% of the isolation-sleep linkage. Given that sleep is especially sensitive to psychological stressors (Kahn et al., 2013), it is not surprising that psychological factors play more important roles than physical well-being in linking social isolation to sleep difficulty. These findings were also in line with recent studies highlighting psychological pathways linking family relationships to sleep outcomes (Chen et al., 2015; Wang et al., 2021).
In addition, our results suggest that the risk of sleep difficulty was especially pronounced for older adults who were both socially isolated and suffered from multiple chronic diseases (partly supporting Hypothesis 3). On the one hand, isolation from supportive social ties has reduced older adults’ sense of mattering, self-esteem, and belongings, which in turn increase their physiological arousal (Thoits, 2011). On the other hand, suffering from multiple chronic illnesses, such as heart disease, arthritis, diabetes, and stroke, may lead to such sleep-related problems as difficulty falling asleep, staying asleep all night, breathing pauses while sleeping, and daytime sleepiness (Crowley, 2011; Foley et al., 2004; Miner & Kryger, 2020; Smagula et al., 2016). And this situation might get worse if they were isolated from supportive networks. We suggest that these vulnerable subgroups of older adults should be a priority to target for interventions.
This study has several limitations worth noting. First, although our use of three waves of longitudinal data and multilevel mixed-effects models can effectively account for individual-specific heterogeneities, it does not directly establish a causal relationship between social isolation and sleep difficulty. It is plausible that those who have sleep difficulty are more likely to experience social isolation, and those who have poor psychological and physical health conditions are also prone to be socially isolated from family and/or friends. However, from a theoretical perspective, we suggest that it is imperative to explore the potential pathways that may intervene in the process by which social isolation translates into subsequent sleep difficulty. Our findings offered preliminary evidence for the underlying health mechanisms through which social isolation may be linked to sleep. Second, our measure of sleep difficulty was based on one self-reported item. This self-reported measure has been validated and is extensively used in studies among older Chinese and other populations (e.g., Bassett & Moore, 2014; Kutner et al., 2001; Wang et al., 2020). Still, future research would benefit from considering objective measurement approaches by using actigraphy or polysomnography to evaluate the robustness of the focal findings (Buysse, 2014). Likewise, the single-item measure of pain in this study was also relatively crude. Future research could continue to expand this study by adopting more detailed clinical pain examinations. Third, due to the data limitation, we could not examine a full range of potential health pathways linking social isolation to sleep difficulty. Future studies should continue to explore other psychological (e.g., sadness, regret, shame, and anger) and behavioral (e.g., drinking, smoking, physical inactivity, obesity, and poor nutrition) mediators when studying the sleep outcome (Buysse, 2014; Kahn et al., 2013). Finally, data limitation also prohibits us from including confounders such as environmental factors and sleep medication usage, which previous studies have found to be associated with sleep in later life (Chen et al., 2015; Miner & Kryger, 2020).
Conclusion
Despite these limitations, this study contributes to cross-cultural knowledge in the field of social relationships and health literature by examining how social isolation is associated with sleep difficulty among older adults in China. Our results demonstrate that social isolation from family and/or friendship ties are independent risk factors for older adults’ sleep. Our findings have important implications for both scientific understandings and effective prevention of sleep problems among older adults in China, which is experiencing unprecedented rates of population aging. Researchers need to step away from a narrow family network when examining social relationships and their associations with sleep health. Policy interventions that integrate social connections from the broader social networks, such as friends and neighbors, would be critical. Policymakers should commit resources to provide older Chinese adults with more opportunities to participate in various social activities in the community and activate social interactions among those with limited social networks. In light of the ongoing COVID-19 pandemic whereby the social distancing is heightened, it is crucial to help older adults to learn how to use digital technology, which may play an important role in connecting older adults with their social network members, keeping them socially engaged, and decreasing the risk of social isolation. In addition, our analyses show that the associations between social isolation and sleep difficulty can be attributed to and also conditioned upon older adults’ mental and physical health. These results suggest that programs and interventions that strive to improve older Chinese adults’ psychological and physical health may have additional benefits on sleep in their later years.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Natural Science Foundation of China (Grant number 72074177), China Scholarship Council (CSC, 202006280098), National Social Science Foundation of China (Grant Number 21ARK005), and the U.S. Eunice Kennedy Shriver National Institute of Child Health and Human Development (Grant number P2CHD042849, P30AG066614).