
Abstract
Population aging presents urgent challenges for global urban health, especially in China. This study examines how three types of neighborhood social infrastructures – public green spaces, gated green spaces, and neighborhood centers – affect health among older adults through physical and social activities and community engagement. Using survey data from Hangzhou, we estimated multilevel regression models. Results show that physical activity in public green spaces and social activities in both public green spaces and neighborhood centers were significantly associated with better health, while gated green spaces showed no independent effects. Higher community engagement was positively associated with health but did not moderate most activity–health relationships, except in neighborhood centers where diminishing returns were observed. Findings highlight that meaningful engagement, rather than access alone, underpins the health benefits of neighborhood environments and provide insights for developing age-friendly communities in rapidly urbanizing contexts.
Introduction
Population aging has emerged as one of the most pressing global public health challenges. In China, this demographic transition is especially pronounced: more than 204 million people were aged 65 or older in 2024, and the number is projected to reach 390 million by 2050 (United Nations, 2024). The rapid growth of the older population is reshaping the demographic composition of Chinese cities, where the majority of older adults now reside (Chen et al., 2022). Central to current policy and scholarly debates is the concept of aging in place, which emphasizes the ability to remain in one’s residence and community safely, independently, and comfortably, regardless of age, income, or functional capacity (Greenfield, 2012). Against this backdrop, our study asks how different forms of neighborhood social infrastructures, defined as the public and semi-public settings that facilitate everyday interaction and collective life (Latham & Layton, 2019), generate or constrain mental health among older adults in China’s urban neighborhoods. Drawing from previous studies on various types of neighborhood spaces (Fu, 2018; Jian et al., 2024; Yan & Zhao, 2024; Zhou, 2021; Zhu & Fu, 2017), we specifically focus on three key forms of neighborhood social infrastructures: public open spaces that are outside residential compounds (e.g., parks and squares), and gated green spaces and shequ zhongxin (neighborhood centers) that are communal spaces within residential compounds.
In China, aging in place is reinforced by cultural traditions of collectivism and Confucian filial piety, which position family members as primary caregivers (Cheng et al., 2011; Silverstein et al., 2006). At the same time, most older adults express a preference for aging in familiar environments (Mo et al., 2025; Yu & Rosenberg, 2017). This is further compounded by the trend of migrant older adults from rural areas into urban areas (Fan et al., 2026). These trends have compelled the Chinese state to reconsider how elder care is organized, promoting integrated approaches that combine home-, community-, and institution-based services (State Council of China, 2022). At the neighborhood level, the development of “age-friendly” environments has been elevated as a national priority (Zhou et al., 2023), with the Healthy China 2030 Agenda explicitly calling for urban spaces that enable physical activity and social participation (State Council of China, 2016).
Within this evolving discourse, urban residential neighborhoods have become central to how older adults experience aging in place. This is situated within a broader urban planning turn toward remaking neighborhoods for aging societies by reducing environmental constraints through design and neighborhood form (Warner et al., 2025). In China, such neighborhoods are typically large-scale developments with multiple high-rise blocks and integrated communal facilities (Lau, 2023), offering both the physical setting and the social infrastructure for daily life (Mo et al., 2025). Their role, however, has transformed significantly across historical periods. Under the planned economy, urban neighborhoods were organized through the danwei (work-unit) system, in which the state and state-owned enterprises served simultaneously as property owners and providers of community services for employees and their families (Bray, 1997; Wang, 2014). Beginning in the 1980s, market-oriented reforms, followed by housing reform in the late 1980s, triggered a dramatic retreat of the state from direct neighborhood governance (Wu, 2002). The dissolution of the danwei system gave rise to gated commodity-housing estates, where community services are now delivered through private and semi-private arrangements (Nie et al., 2024a; Yan & Zhao, 2024; Zhu & Fu, 2017).
Social infrastructure refers to the facilities and settings, which are often manifested as public or semi-public spaces, that enable cities to function as social spaces, where people can interact, form connections, and participate in collective life (Latham & Layton, 2019). Public open spaces such as city parks and squares in China have been traditionally viewed as important social infrastructures (Zhu & Fu, 2017), and older adults often use public spaces as gathering points for community engagement and entertainment (Yung et al., 2016). With the rapid growth of the aging population, older adults have become a sizable group of users, engaging in walking, running, tai chi, karaoke, and other recreational pursuits in urban open spaces (Zhou, 2021). These spaces host a wide range of leisure activities and social encounters, including guangchangwu (square dancing), choral singing, calligraphy, card playing, and various parent–child activities (Flock & Breitung, 2016; Zhou, 2021). These public open spaces are typically municipal facilities located outside gated residential compounds and are generally open-access, meaning older adults often travel beyond their immediate residential compound and encounter a more heterogeneous mix of users, including strangers.
By contrast, neighborhood-scale social infrastructures are commonly embedded within gated residential compounds and their service boundaries, such as communal (gated) green areas and neighborhood centers, where access depends on residence, trips are shorter, and encounters tend to involve neighbors or acquaintances. Chinese residents often perceive communal spaces within neighborhood compounds as extensions of the home that provide settings for outdoor activities while also maintaining a sense of privacy within neighborhood boundaries (Fu & Lin, 2014). These amenities range from traditional features such as community squares and public parks to more contemporary facilities embedded in high-rise complexes and co-living spaces (e.g., shops, libraries, and local services). They function as informal meeting places, which foster opportunities for everyday interactions that promote the development of social capital (Finlay et al., 2019; Kuo et al., 1998). Such spaces also serve as focal points for community participation and network building (Cattell et al., 2008; Fu & Lin, 2014; Tomba, 2005). All of them eventually facilitate the building of cohesion, collaboration, and mutual trust among residents (Kim & Kaplan, 2004; Zhou et al., 2023; Zhu & Fu, 2017).
Shequ zhongxin (neighborhood center) has received relatively less scholarly attention as a type of neighborhood social infrastructure in China. Introduced in the 2000s, drawing inspiration from Singapore’s experience, neighborhood centers quickly proliferated across Chinese cities and have since become a key physical structure for delivering community services (Xu et al., 2005). These centers generally integrate multiple neighborhood-level services within a single building complex, providing essential public spaces and offering a wide range of activities, programs, and support networks that enhance community well-being and development (Yan & Zhao, 2024). By consolidating diverse services under one roof, neighborhood centers address the service gaps often found in gated residential compounds, where developers typically provide only limited “club goods” (Chiu-Shee et al., 2023). More recently, they have expanded their scope to include eldercare functions, effectively serving as neighborhood-based eldercare hubs that resemble localized nursing homes and provide daily care for older adults (Yu, 2022).
Social infrastructures in and around residential neighborhoods have long been recognized as critical for health promotion (Corburn, 2009). Within human geography, the concept of therapeutic landscapes has been widely used to capture the ways in which physical and social qualities of such spaces shape individuals’ sense of health and well-being (Finlay et al., 2015; Völker & Kistemann, 2013). From a physical perspective, these social infrastructures are “enabling places” that encourages physical activity and foster psychological restoration (Duff, 2012; Francis et al., 2012). This relationship can be understood behaviorally, as natural environments provide opportunities for exercise and recreation, while also aligning with biophilia theory, which posits that humans have an innate affinity for nature (Kellert, 1993; Ulrich, 1983). Empirical studies support these claims, showing that urban green spaces promote physical activity (Lachowycz et al., 2012), evoke aesthetic pleasure, and generate psychological attachment (Foster et al., 2010; Parr, 2000). Even passive forms of exposure, such as viewing images of nature, have been found to reduce stress and produce positive emotional and physiological responses (Brown et al., 2013; Ulrich et al., 1991).
From a social perspective, these social infrastructures allow transactions between individuals and their broader socio-environmental contexts, which have been widely recognized as a key determinant of healthy aging (Duff, 2012; Holt-Lunstad, 2024; Monteiro et al., 2025). Lawton’s (1985) classic work demonstrated that older adults are more likely to be physically active, socially engaged, and psychologically positive when they can derive satisfying socio-spatial experiences from their living environments. Building on this, a growing body of research has shown that maintaining social relationships helps buffer stress, foster emotional resilience, and enhance life satisfaction (Chen & Feeley, 2014; Fu, 2018; Kawachi, 2001; Lang & Carstensen, 1994; Toyama & Fuller, 2020). Public spaces have been identified as important nodes for fostering interaction, civic engagement, and social capital (Finlay et al., 2019; Nie et al., 2024b), while strong neighborhood ties have consistently been shown to protect health in urban contexts compared to socially isolated residents (Kawachi, 2001; Moore et al., 2011). In addition, in-person community engagement with family, friends, and community members is central to psychological well-being in later life (Macdonald et al., 2021; Teo et al., 2015).
Despite substantial evidence linking social infrastructures to health, important gaps remain. First, it is unclear how health-related quality of life is shaped by the interplay of physical environments and older adults’ activities. For instance, Wang et al. (2024) showed that participation in activities inside versus outside residential neighborhoods can yield different well-being outcomes, yet the mechanisms behind these differences remain underexplored. Recent evidence further suggests that the health benefits of neighborhood environments are not determined by their presence alone, but by whether they provide accessible, high-quality, and socially vibrant settings that support sustained physical and social engagement (Liu et al., 2023a, 2023b; Wang et al., 2026). Second, while urban open spaces are widely recognized as important venues for health promotion (Zhou, 2021; Zhou et al., 2023), less is known about how communal spaces, such as neighborhood centers and gated green areas within residential neighborhood compounds, function as everyday health-promoting environments for older adults. Third, following the inquiry by Fu (2018) on the indirect effects of social interactions on the use of neighborhood communal spaces and health, and recognizing that the benefits of social interaction may exhibit diminishing returns once social and participatory needs are largely met (Liu et al., 2023b; Luo et al., 2022), the moderating role of older residents’ community engagement within residential neighborhoods remains insufficiently examined.
Taken together, these gaps underscore the need to investigate whether and how different forms of social infrastructure in Chinese urban neighborhoods generate or constrain health-related quality of life among older adults. A further inquiry is to examine the role of community engagement in moderating these relationships. Addressing these questions is particularly important in rapidly transforming urban contexts such as China, where neighborhood infrastructures and social relations are evolving simultaneously. In this study, we focus on three types of neighborhood social infrastructures – public green spaces, gated green spaces, and neighborhood centers – and analyze how older adults’ community engagement within them shapes health outcomes. By integrating physical settings with social processes, the study advances understanding of how neighborhood social infrastructures shape health in later life and contributes new evidence from the rapidly transforming urban contexts of China.
Methodology
Study Setting, Sampling, and Data Collection
This study is based on a cross-sectional survey conducted from May to June 2024 among older adults aged 60 and above living in urban communities in Hangzhou, China. Hangzhou is the capital of Zhejiang Province in the Yangtze River Delta and is a large and rapidly developing city with substantial investment in urban greening and community governance, including community upgrading for age-friendliness (e.g., Zhejiang’s Future Community Initiative) (Tang et al., 2025). The sample was selected in two stages: first, residents’ committees (juweihui) were selected, and then older adults within each selected community. To ensure representation across different residential communities, we employed systematic sampling within four central districts of Hangzhou (Shangcheng, Xihu, Gongshu, and Binjiang). Outlying districts were excluded, as the study focused on urban older adults. We first compiled a complete list of residential communities in the four districts, organized by district and then by subdistrict (jiedao). From this list, we randomly selected one-quarter of the residential communities using systematic sampling with a sampling interval of four. This resulted in 42 residential communities. Within each selected community, older adults were recruited with the assistance of residents’ committee members rather than through random household sampling procedure followed by eligibility screening. This approach was adopted to facilitate access to older residents and to improve recruitment efficiency. To ensure demographic diversity among older adults, district-level quotas were applied for gender (50% male, 50% female) and age (60–64: 30%; 65–69: 30%; 70–74: 20%; 75 and older: 20%).
Data was collected through a standardized questionnaire, which was first piloted to assess clarity and appropriateness among a small group of older adults. Based on pilot feedback, minor revisions were made to improve item comprehension and reliability. The finalized questionnaire was administered face-to-face by trained interviewers from a professional survey company. To differentiate between public and gated green spaces, Figure 1 shows that public green spaces denote open green spaces accessible to older adults outside their immediate neighborhoods. Gated green spaces, on the contrary, are the communal green spaces within the gated communities. Examples of the three types of social infrastructure spaces from surveyed neighborhoods
Measures
Dependent Variable
Participants’ health-related quality of life is the primary outcome of interest, measured using the EQ-5D-5L instrument. This instrument captures five health dimensions: mobility, self-care, usual activities, pain/discomfort, and anxiety/depression. Each dimension is rated on a five-level scale ranging from no problems (level 1) to extreme problems (level 5). A single index score was calculated for each participant using the Chinese EQ-5D-5L value set developed by Luo et al. (2017), which incorporates societal preference weights derived from time trade-off (TTO) and discrete choice experiments. The resulting EQ-5D index score ranges from 1 (full health) to values below 0 (states considered worse than death) and was used as a continuous dependent variable in all regression models.
Independent Variables
The key independent variables included six binary indicators capturing whether the respondent reported having social and/or physical activity in each of the following types of social infrastructure spaces: (1) neighborhood centers, (2) gated green spaces, and (3) public green spaces. Each indicator was coded as 1 if the respondent reported participating in the corresponding type of activity within the specified space, and 0 otherwise. For respondents who reported no participation in any social infrastructure spaces, all six indicators were coded as 0.
Moderator
To assess participants’ level of social engagement in the neighborhood, which could influence their interactions with and behaviors in neighborhood social infrastructure spaces, we constructed a community engagement index (CEI) using three questionnaire items: frequency of communicating with other residents, frequency of helping other residents, and frequency of volunteering in the community. An exploratory factor analysis (EFA) using principal axis factoring supported a one-factor solution (factor loadings: 0.30 for the frequency of volunteering, 0.50 for the frequency of communication, and 0.61 for the frequency of helping neighbors), accounting for 22.4% of the total variance. Given the interpretability and theoretical coherence of this factor, we adopted this CEI construct and used it as a continuous moderator in subsequent regression models. Although factor scores are mean-centered by construction, they are not standardized to unit variance. For ease of interpretation and comparability across models, the index was standardized (mean = 0, SD = 1) prior to regression analyses.
Control Variables
Control variables included age (continuous), gender (female = 1, male = 0), and living arrangement (living with a partner = 1, otherwise = 0). Highest educational attainment was categorized as: (1) junior high school or below; (2) high school or vocational secondary education; and (3) post-secondary education, including associate, bachelor’s, master’s, or doctoral degrees. Annual personal income was grouped into three categories: (1) less than ¥50,000 CNY; (2) ¥50,000–100,000 CNY; and (3) more than ¥100,000 CNY. Hukou registration status was coded as 1 for individuals holding a Hangzhou hukou and 0 for those without. Employment status was defined as 1 for retired or not currently working and 0 for those still working full- or part-time.
Statistical Analysis
We conducted a series of multilevel linear regression models estimated via ordinary least squares (OLS) to examine the association between social infrastructure space use, activity types, and health-related quality of life among older adults. Given the clustered sampling design, with respondents nested within residential communities, all models were estimated using mixed effects modeling with random intercepts at the community level to account for within-community correlation in health outcomes. The outcome variable was the EQ-5D-5L index score, a continuous measure of health utility derived from responses to five health dimensions and calculated using the Chinese value set. All models controlled for the same set of sociodemographic variables, including age, gender, educational attainment, annual income, living arrangement, hukou status, and employment status.
Our analysis proceeded in two stages. In the first stage, we estimated two sequential models using the full sample. Model 1-1 included only control variables to establish a baseline. Model 1-2 included binary variables capturing engagement in physical and social activities within three space types (i.e., neighborhood centers, gated green spaces, and public green spaces), to assess the independent association between space-specific activity and health.
In the second stage, we examined whether community engagement moderated the relationship between activity engagement and health outcome, as shown in the conceptual framework (Figure 2). These interaction models were estimated using a subsample of respondents who reported using at least one type of social infrastructure space. We included interaction terms between activity engagement variables and the standardized CEI to assess whether the relationship between physical or social activity and health varied by the level of social connectedness. Conceptual Framework.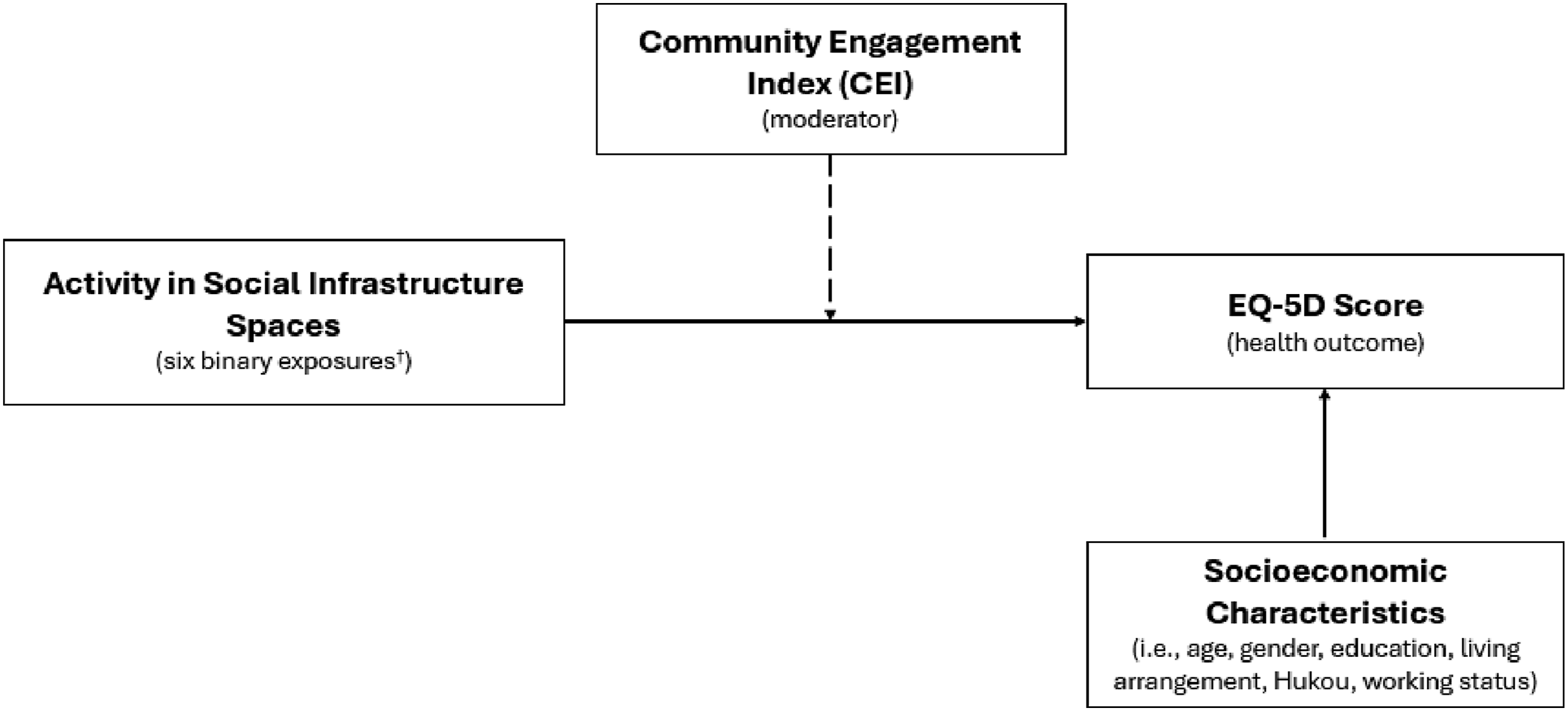
All models were estimated using maximum likelihood estimation. Model fit was assessed using standard information criteria, and intraclass correlation coefficients (ICCs) were examined to quantify the proportion of variance attributable to between-community differences. ICCs ranged from 0.03 to 0.06 across models, indicating modest but non-negligible clustering at the community level and supporting the use of multilevel modeling. Variance inflation factors indicated no problematic multicollinearity among the fixed effect baseline models (all VIFs <2). In interaction model (2-2), higher VIFs were observed for terms involving community engagement and their interactions, reflecting expected collinearity inherent to interaction specifications rather than model instability. Formal tests suggested non-constant residual variance; however, given the large sample size, bounded outcome measure, and use of random effects, this pattern was not unexpected and does not invalidate inference. All analyses were conducted using R (version 4.4.3).
Robustness Checks
To assess the robustness of our main findings, we conducted two sets of additional analyses. First, to evaluate the sensitivity of results to model specification and the treatment of clustering, we re-estimated all main models using single-level ordinary least squares (OLS) regression with cluster-adjusted robust standard errors at the community level. This approach accounts for within-community correlation in outcomes while maintaining a fixed-effects framework. The estimated coefficients and their statistical significance were highly consistent with those obtained from the multilevel models, indicating that the substantive conclusions are not driven by the choice between fixed-effects models with clustered standard errors and random-intercept multilevel specifications.
Second, to examine whether the findings were sensitive to the specific health outcome measure used, we replaced the EQ-5D index with an alternative outcome: overall self-reported health, measured on a five-point scale ranging from very unhealthy to very healthy. This measure captures respondents’ global assessment of their health status and is less directly tied to specific physical functioning dimensions embedded in the EQ-5D. Re-estimating the full set of models using this alternative outcome yielded substantively similar patterns for both the main effects and interaction terms, including the moderating role of CEI. This suggests that our results are not solely driven by the construction of the EQ-5D index and reflect a more general relationship between social engagement, physical activity, and health.
Results
Descriptive Characteristics of the Study Sample by Social Infrastructure Space Use Status (Mean (SD) or N (%))
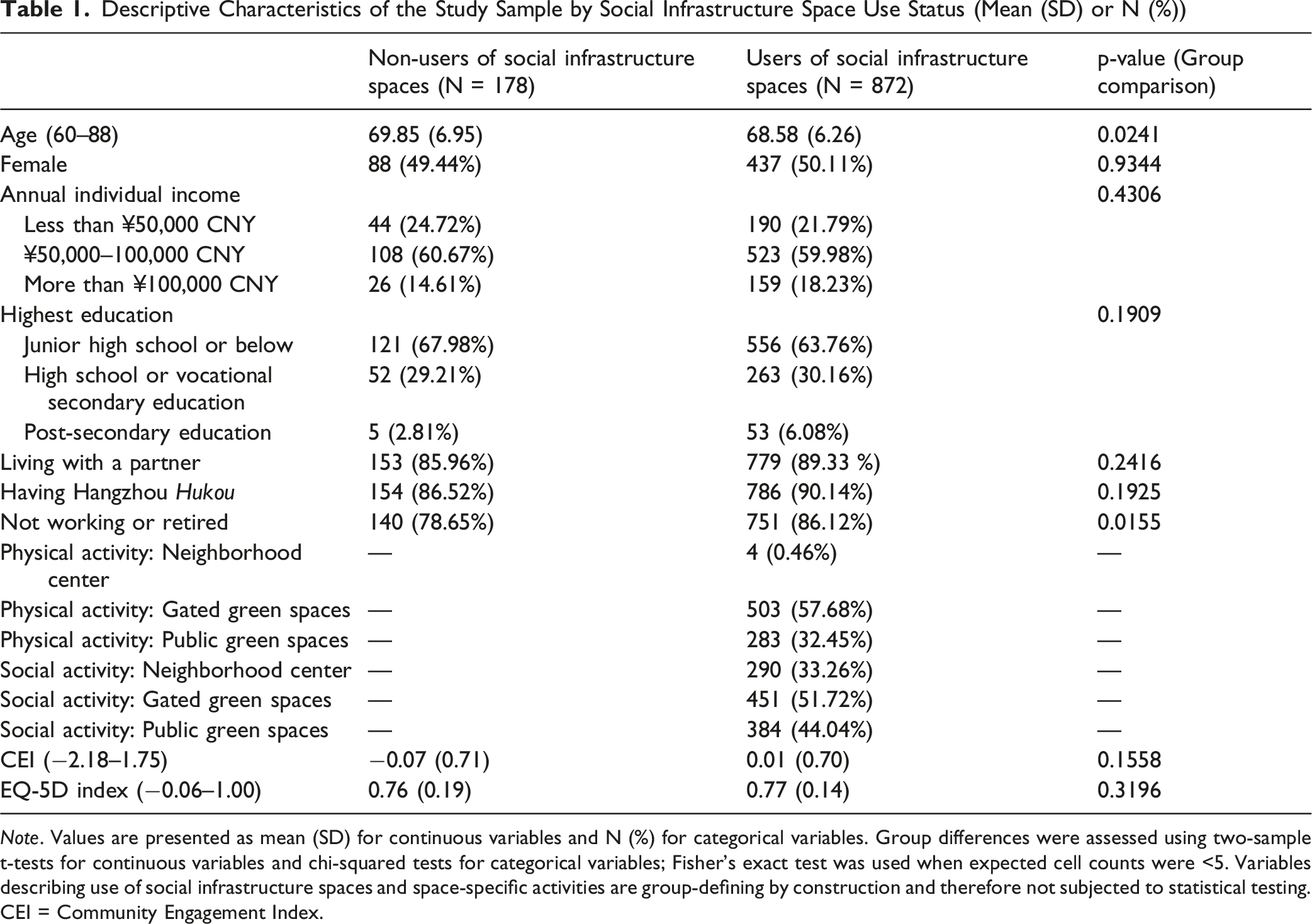
Note. Values are presented as mean (SD) for continuous variables and N (%) for categorical variables. Group differences were assessed using two-sample t-tests for continuous variables and chi-squared tests for categorical variables; Fisher’s exact test was used when expected cell counts were <5. Variables describing use of social infrastructure spaces and space-specific activities are group-defining by construction and therefore not subjected to statistical testing. CEI = Community Engagement Index.
Among users of social infrastructure spaces, physical activity was most frequently reported in gated green spaces, with 57.68% of users engaging in such activity. This was followed by public green spaces (32.45%), while only a small proportion (0.46%, N = 4) reported engaging in physical activity within neighborhood centers. In terms of social activity, gated green spaces were again the most common setting, with 51.72% of users participating in social activities in these areas. This was followed by public green spaces (44.04%) and neighborhood centers (33.26%).
Associations Between Social Infrastructure Space Use, Activity Types, and EQ-5D Health Index (N = 1050)
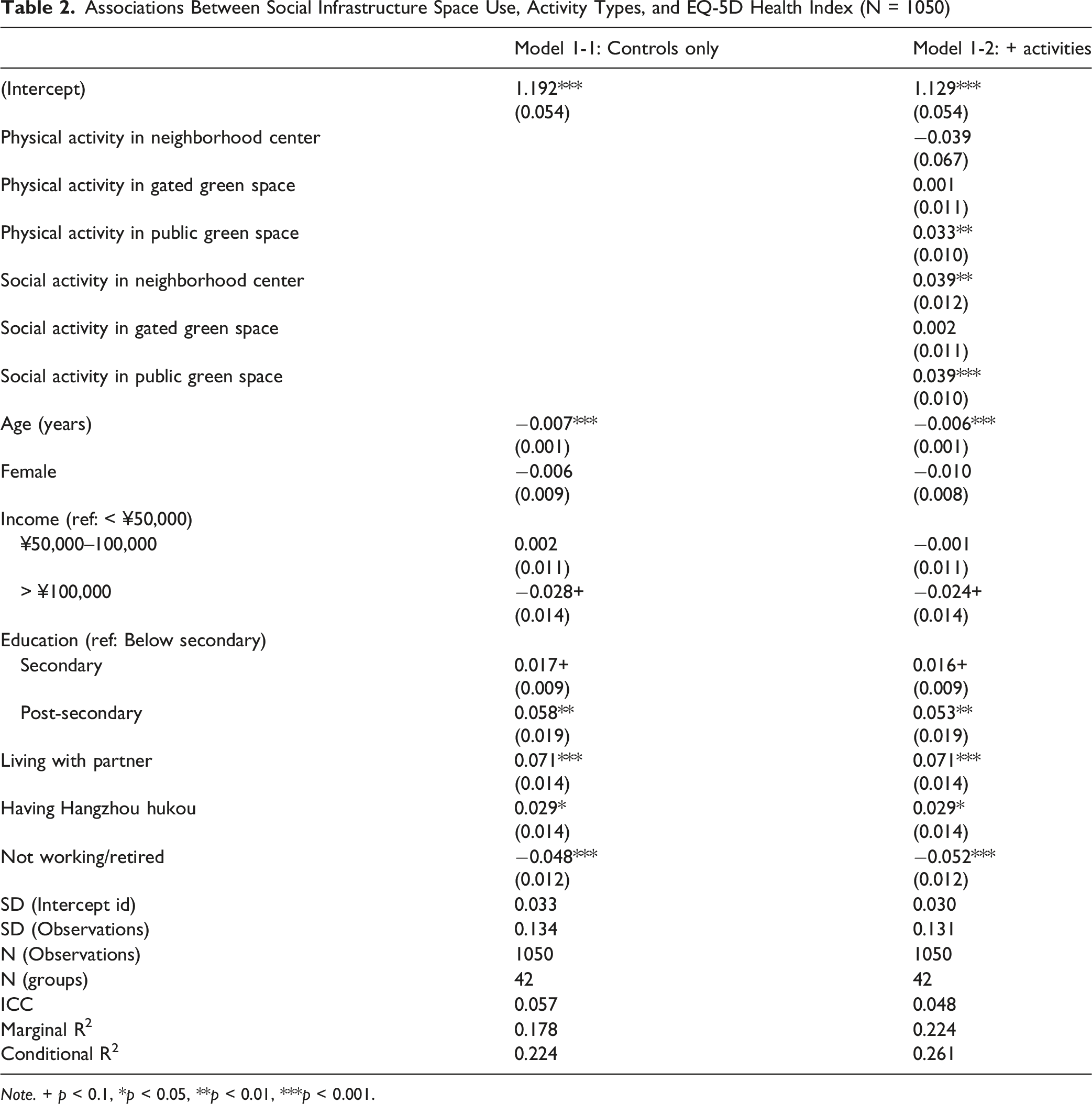
Note. + p < 0.1, *p < 0.05, **p < 0.01, ***p < 0.001.
Moderating Effect of Community Engagement on the Association Between Activity Types and Health Among Social Infrastructure Space Users (N = 872)
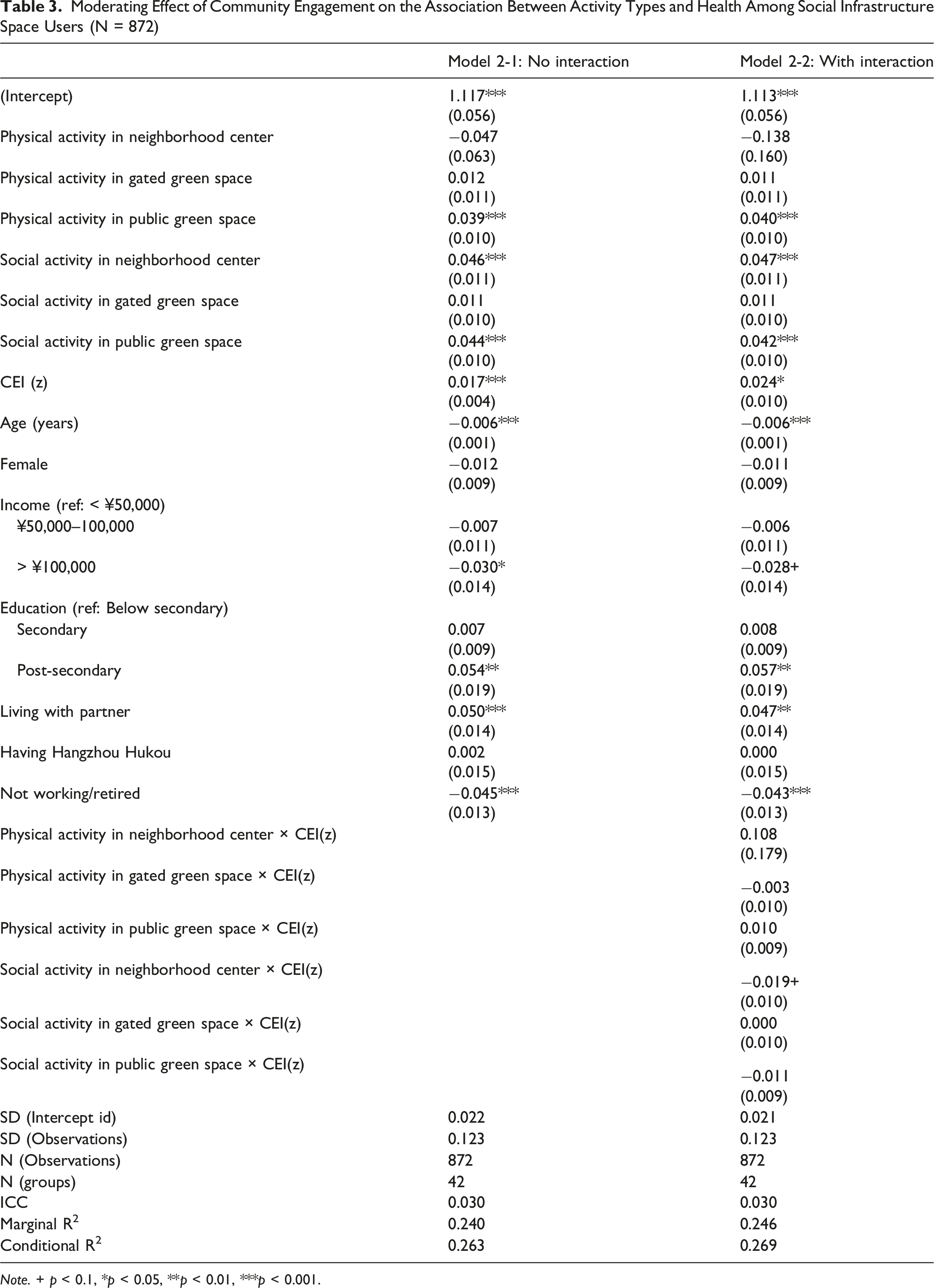
Note. + p < 0.1, *p < 0.05, **p < 0.01, ***p < 0.001.
The inclusion of the interaction terms between the CEI and each type of activity in Model 2-2 did not substantially increase the explained variance compared to Model 2-1 (conditional R2 = 0.263 vs. 0.269). Most interaction effects were statistically non-significant, suggesting that the relationship between activity engagement and health did not vary meaningfully by an individual’s overall level of community engagement. An exception was the interaction between CEI and social activity in neighborhood centers, which was negative and marginally significant (β = −0.019, p < 0.1). This finding indicates the association between this type of activity and health was weaker among individuals with higher levels of CEI.
Discussion
Physical/Social Activities in Different Neighborhood Social Infrastructures
Table 2 reveals mixed patterns of health benefits when considering both the type of social infrastructure spaces (i.e., neighborhood centers, gated green spaces, and public green spaces) and the activities performed within them, underscoring that not all environments contribute to health in the same way. Both physical and social activities in public green spaces contribute positively to health. This finding aligns with earlier studies showing that environments that facilitate physical activity promote psychological restoration (Duff, 2012; Lachowycz et al., 2012). Specifically in China, where the aging population is rapidly expanding, older adults have become a sizable group of users of public green spaces, participating in various forms of physical activities (Zhou, 2021). In line with these expectations, public green spaces in our study supported health, likely because they combine exposure to natural features with opportunities for collective physical activities. While Wang et al. (2024) highlighted the importance of socializing, leisure, and recreation activities outside the immediate neighborhood, our results suggest that physical activities in public green spaces yield stronger health benefits than the same activities in other settings.
At the same time, our results underscore the social dimension of health benefits, which has long been recognized as a key determinant of healthy aging (Holt-Lunstad, 2024; Monteiro et al., 2025). Public spaces such as parks and squares outside of residential neighborhoods in Chinese cities are traditionally viewed as key social infrastructures, providing gathering points for leisure and entertainment among older adults (Yung et al., 2016; Zhu & Fu, 2017). In these contexts, physical and social activities are often intertwined, as group-based practices like guangchangwu and parent–child activities foster both movement and interaction (Flock & Breitung, 2016; Zhou, 2021). This also resonates with the broader literature on therapeutic landscapes, which emphasizes the health-promoting qualities of natural settings through both physical engagement and social interaction (Finlay et al., 2015; Völker & Kistemann, 2013).
However, gated green spaces, commonly incorporated into residential compounds in urban China, did not demonstrate significant health benefits in our analyses. This finding challenges assumptions in the place-and-health literature that natural environments are inherently health promoting (Brown et al., 2013; Foster et al., 2010; Kellert, 1993; Parr, 2000; Ulrich, 1983; Ulrich et al., 1991). It specifically complicates the finding by Wang et al. (2024) that well-being in Chinese neighborhoods is best achieved through passive relaxation and resting activities within residential compounds. As the current study presents, types of social infrastructure and the actual practices in these spaces warrant attention, since green-space effects among older adults are often context-specific and mixed across outcomes (Wang et al., 2026). The health implications of green space are not determined by their presence alone, but also by the intensity and diversity of activities it enables, and the social interactions it supports (Liu et al., 2023a, 2023b). Specifically as Liu et al., 2023a argue, environmental features affect older people’s mental health only when they support meaningful physical and social activities and match older adults’ functional capacities. From this perspective, gated green spaces may have functioned mainly as convenient settings for brief or low-intensity activities and routine interactions with familiar neighbors, which may offer limited additional benefits for self-rated health. Further investigation is needed to clarify these patterns.
Interestingly, neighborhood centers, usually architectural and service-oriented rather than natural, also produced positive health associations. This suggests that built social infrastructures can play roles comparable to green environments when they provide structured opportunities for meaningful social engagements (Xu et al., 2005; Yan & Zhao, 2024). Here, meaningful engagement refers to participation that provides purposeful, socially connective interactions and access to supportive resources, such as interaction whose benefits depend on the quality and context of social exchange and access to resources, not simply how often activities occur. Viewed as a form of communal space within neighborhoods, neighborhood centers align with Fu and Lin’s (2014) observation that Chinese residents often perceive such communal settings as extensions of the home, much like other contemporary neighborhood communal facilities such as shops, libraries, and local services. The can potentially serve as what Jian et al. (2025) identify as flexible places for services, activities, and community support networks.
In addition, our descriptive results in Table 1 suggest that only a small proportion of respondents engaged in physical activity within neighborhood centers, highlighting their predominant role as social rather than physical spaces. They serve as focal points for community participation and network building (Cattell et al., 2008; Fu & Lin, 2014; Tomba, 2005), provide opportunities for everyday interactions that generate social capital (Corburn, 2009; Finlay et al., 2015, 2019; Kuo et al., 1998; Völker & Kistemann, 2013), and facilitate cohesion, collaboration, and mutual trust among residents (Kim & Kaplan, 2004; Zhou et al., 2023; Zhu & Fu, 2017). Such everyday encounters are known to buffer stress, foster resilience, and enhance life satisfaction (Chen & Feeley, 2014; Fu, 2018; Kawachi, 2001; Lang & Carstensen, 1994; Nie et al., 2024b; Toyama & Fuller, 2020). The health benefits of social infrastructure spaces arise not from access alone but from the quality of engagement they support. However, because physical activity in neighborhood centers was reported by very few respondents (0.46% of social infrastructure users), the negative coefficient should be interpreted cautiously. The low prevalence of participation limits the stability and interpretability of the estimate, and the negative association should not be read as robust evidence of an adverse health effect. Instead, it may reflect sparse data or possible selection into low-intensity, home-proximate activity among older adults with greater functional limitations.
The Moderating Effect of Community Engagement
The analysis of community engagement in Table 3 adds further readings of the relationship between activity participation and health. Consistent with earlier work, higher levels of community engagement were directly associated with better health outcomes, reinforcing evidence that social participation and connectedness serve as protective factors for older adults’ well-being (Fu, 2018; Kawachi, 2001; Lang & Carstensen, 1994). This finding also extends Lawton’s (1985) classic insight that older adults are more likely to remain active, socially engaged, and psychologically positive when they derive satisfying socio-spatial experiences from their everyday environments. When residents feel connected and socially integrated, neighborhood social infrastructure spaces are more likely to translate into health benefits. Prior studies have shown that strong neighborhood ties protect health in urban contexts (Kawachi, 2001; Moore et al., 2011) and that in-person socialization with family, friends, and neighbors is central to psychological well-being in later life (Fan et al., 2026; Macdonald et al., 2021; Teo et al., 2015). At the same time, our results indicate that community engagement did not significantly moderate most activity–health relationships, suggesting that the health benefits of physical and social activities accrue relatively consistently across individuals regardless of their baseline level of engagement.
The one exception was social activity in neighborhood centers, where the positive health effect was weaker among individuals with higher community engagement. This pattern suggests a possible saturation or diminishing returns effect, whereby additional participation yields smaller incremental benefits once older adults’ needs for social connection and meaningful participation are largely fulfilled (Luo et al., 2022). Meanwhile, some neighborhood resources may be linked to worse outcomes when they foster excessive engagement (Liu et al., 2023b; Luo et al., 2022). In this context, older adults who are already socially active gain fewer additional benefits from activities in neighborhood centers compared to those with fewer opportunities for engagement. This interpretation is consistent with prior work showing nonlinear or threshold relationships between social participation and well-being in later life, where benefits can plateau at higher levels of engagement (Luo et al., 2022; Windsor et al., 2008). It also aligns with a resource substitution logic in which additional structured opportunities yield larger marginal benefits for individuals with fewer baseline resources or opportunities for engagement (Ross & Mirowsky, 2006). Although Chen et al. (2023) suggest that meeting opportunities are more influential on aging-in-place for non-frail older adults, our findings point to the otherwise – neighborhood center activities appear to yield the greatest marginal benefits for those with lower levels of community connectedness. This divergence highlights that not all social interactions are equally beneficial, as the health impact depends not only on frequency but also on the quality and context of engagement. Neighborhood centers, therefore, remain valuable infrastructures for promoting participation, but their benefits may be most pronounced for individuals who otherwise have limited avenues for social involvement. Future qualitative research could further examine how older adults with different levels of community engagement benefit from neighborhood center activities, including whether such activities provide meaningful support, create social obligations, or meet different engagement needs.
Conclusion
This study contributes to current knowledge on aging in place, particularly in the context of China’s urban neighborhoods, by examining the varied health benefits of three different types of social infrastructure spaces. First, building on Wang et al. (2024), who found that participation in activities inside versus outside residential neighborhoods yields different well-being outcomes, our results show that engaging in meaningful activities in social infrastructure spaces is critical for health. The distinction between green spaces outside and inside the neighborhood lies more in the types of activities they support. Second, we identified neighborhood centers as critical neighborhood infrastructures that complement public green spaces, which have long been recognized as important venues for health promotion (Zhou, 2021; Zhou et al., 2023). Neighborhood centers function primarily as social facilities, with health benefits that are especially pronounced for older adults who are less socially active. Third, while earlier research suggests that the relationship between communal space use and health can be mediated by social engagement (Fu, 2018), our findings indicate that community engagement did not significantly moderate most activity–health relationships. Instead, the health benefits of physical and social activities accrued relatively consistently across individuals regardless of their baseline level of engagement, except for neighborhood centers, while higher community engagement overall was positively linked to better health.
These findings bring important insights into the practice of aging in place in China, where most older adults prefer to remain in their residential neighborhoods (Mo et al., 2025; Yu & Rosenberg, 2017), and where aging in place is reinforced by collective living arrangements and close ties with family, friends, and neighbors (Cheng et al., 2011; Silverstein et al., 2006). While the state, market, and civil society actors have actively sought paradigms to support aging in place, the notion of “age-friendly” neighborhoods cannot be reduced to the provision of physical infrastructures that are ostensibly “easy to use.” Social environments, particularly opportunities for meaningful social activities, play equally, or perhaps even more important roles. This complexity is heightened by the plurality of neighborhood social infrastructures in China’s urban neighborhoods that are typically large in scale, high in density, and diverse in activities within. Addressing aging in place, therefore, requires careful attention to the intersections of multiple physical and social elements of neighborhoods, in this study, public versus gated green spaces and neighborhood centers.
In particular, neighborhood centers are increasingly taking on responsibilities for eldercare provision (Yu, 2022), underscoring the need for further research into how these infrastructures can support older adults who choose to remain in their neighborhoods. These findings also speak to Healthy China 2030, which emphasizes community-scale health promotion (State Council of China, 2016). While the Outline articulates broad goals for healthy aging and community-based support, it offers less guidance on which neighborhood-scale social infrastructures most effectively generate everyday mental-health benefits. Our results suggest that neighborhood centers can serve as practical implementation platforms for these goals, particularly when they foster meaningful participation among older adults who otherwise have limited avenues for engagement.
This has important equity implications that socially isolated or mobility-constrained older adults may benefit most from nearby, low-barrier, non–physically intensive programs delivered through neighborhood centers. Because these facilities are already widely embedded in urban neighborhoods, strengthening programming and outreach within them may represent a cost-effective strategy for advancing community-based healthy aging. Realizing these benefits will require cross-sector collaborations that move age-friendly practice beyond physical accessibility toward inclusive participation, social connection, and mental-health promotion in everyday neighborhood life (Warner et al., 2025). Urban planners and architects can design low-barrier gathering spaces, public health professionals can identify locally salient mental-health risks and develop evidence-informed activity menus, and social service providers and community organizations can translate these capacities into sustained engagement through outreach to socially isolated residents and volunteer coordination.
This study has limitations that should be acknowledged. First, because of the cross-sectional design, our analyses are correlational rather than causal, and the associations observed between social infrastructure spaces, activities, and health should therefore be interpreted with caution. Longitudinal studies are needed to disentangle the temporal dynamic relationships. In addition, key measures of social participation and physical activity were self-reported, which may introduce recall or social desirability bias. Future study would benefit from incorporating more objective or mixed-methods approaches, such as GPS-based mobility tracking, direct qualitative observation, or activity diaries, to improve the validity of measures of space use and activity participation. Second, the study was conducted in Hangzhou, and the extent to which these findings can be generalized across China remains uncertain given the country’s geographic, cultural, and institutional diversity. At the same time, this limitation highlights the value of a place-focused approach – aging-in-place practices in China may need to be tailored to local conditions rather than treated as uniform across contexts. Third, the participants are relatively healthy older adults, which may partially reflect the demographic characteristics of Hangzhou and the practical requirements of participation in an interviewer-administered questionnaire of moderate length. Future studies may benefit from including more diverse populations with varying levels of health, mobility, and support needs to better capture the spectrum of aging experiences.
Footnotes
Ethical Considerations
The study protocol, including participant recruitment, data collection, and informed consent procedures, was reviewed and approved by the Ethics Committee for Scientific Research of the corresponding author’s university.
CRediT Authorship Contribution Statement
Xuanyi Nie: Supervision, Conceptualization, Data curation, Investigation, Writing – original draft, Writing – review and editing. Zili Huang: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Software, Visualization, Writing – original draft, Writing – review and editing. Longfeng Wu: Data curation, Writing – review and editing. Chan Zhang: Data curation, Funding acquisition, Writing – review and editing.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is supported by the Zhejiang University Global Partnership Fund.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data not available due to identification risks.