
Abstract
Using data drawn from biennial waves of the Health and Retirement Study (HRS) collected between 2008 and 2018, this study examines how early-life health adversities relate to aging trajectories, influencing self-rated health, aging perceptions, and late-life resilience. The baseline sample comprised 19,931 individuals aged 50 and older (mean = 66.30 ± 11.14 years; 58.0% females), of who 3.9% reported chronic functional disability in childhood. Employing a General Linear Model (GLM) repeated-measures analysis, we compared outcome variables both between groups (childhood disability vs. no childhood disability) and within groups across three measurement points. Results indicated that the subgroup with childhood functional disability reported significantly lower levels of resilience and positive aging perceptions at baseline compared to those without such experiences. However, no significant group differences were observed at either follow-up. Over the 8-year period, resilience, positive aging perceptions, and perceived health changed within and between the groups, but in varied ways.
Introduction
A life course approach to healthy aging emphasizes how multiple risk factors, often beginning early in life, exert enduring influences on aging trajectories (Bengtson et al., 2012; Elder & Johnson, 2018; Kuh et al., 2013). This perspective finds strong empirical support in research grounded in Adverse Childhood Experiences (ACEs) and life course epidemiology, which consistently demonstrate how early life stressors—often categorized into the domains of threat (e.g., abuse or violence) and deprivation (e.g., neglect or poverty)—persist and reverberate across the lifespan (e.g., Cheval et al., 2019; Kemp et al., 2022; McLaughlin & Sheridan, 2016). While the impacts of socio-familial adversities are well-documented, the specific role of childhood health-related adversities remains relatively underexplored in gerontological research. One possible reason is that, historically, for older cohorts, long-term childhood health problems often led to early mortality due to limited medical interventions, preventing many from reaching old age (McEniry, 2013). As a result, aging research may lack sufficient data on survivors who experienced severe health threats in childhood. In recent decades, however, improved pediatric care and chronic disease management have enabled individuals with childhood health adversities or life-long disabilities to reach older adulthood in greater numbers (Coppus, 2013; Lee et al., 2020). In such cases, the long-term impact of childhood health shocks may appear less detrimental in old age, prompting researchers and practitioners to downplay their significance in promoting health and well-being of older adults. Nonetheless, from a life course perspective, the experience of managing chronic health problems, and the resulting disruption to daily functioning during critical developmental periods may have subtle yet far-reaching consequences, potentially affecting personality development, social relationships, emotional regulation, and resilience—factors with enduring implications for health and well-being in later life. This study addresses the limited understanding of childhood health problems as a distinct life-course disruption and examines whether those with early-life health challenges follow different aging trajectories from those who did not face such health shocks in childhood.
Childhood Adversity and its Divergent Impact in Old Age
Significant longitudinal associations between early-life adversities and late-life health are well-evidenced, particularly concerning its profound impact on mental health disparities among older adults (e.g., Amemiya et al., 2018; Lin et al., 2023; Mian et al., 2022). Together, these findings highlight a pattern of compounded disadvantage, where the impact of early adversity intensifies over time and increases vulnerability to comorbid physical and mental health risks. Furthermore, later-life interventions and available resources may not fully compensate for the negative impact of childhood adversities. For instance, Cheval et al. (2019) found that childhood adversities tended to increase the risk of low muscle strength (LMS) in older women, and that several positive developments in adulthood (educational attainment, job, and satisfaction with household financial situation) could not fully offset the long-term effects. Similarly, Cosco et al. (2019) showed that psychosocial adversities in childhood were significantly related to greater levels of anxiety and depression symptoms, regardless of protective resources and behavioral interventions such as physical activity, occupational status, education, social support, and neighborhood cohesion. These findings reinforce the enduring and deeply embedded impact of childhood adversities.
Paradoxically, however, some studies suggest that childhood adversities do not always necessarily follow detrimental pathways. In facing adversities, people also tend to build coping strategies and resilience (Fridman et al., 2011; Leung et al., 2022; Woods-Jaeger et al., 2018). For instance, Schafer et al. (2011) investigated how experiences of childhood adversity contribute to cumulative inequality over the life course, influencing individuals’ perceptions of their own life trajectories. The study found that while early adversity led to greater perceived disadvantage over time, study participants rarely lowered their expectations and hopes for the future. Fridman et al. (2011) examined older female Holocaust survivors in Israel, and found that these survivors appeared to be highly resilient and adaptive in coping with declines in mental and physical health and cognitive functioning in old age. This suggests that while experiencing adversities during childhood might lead to lifelong hardship and embedded chronic stress, individuals are capable of finding and developing resources to compensate for the negative effects and constructing positive transitions during or after stressful life events.
In the same vein, chronic health problems in childhood may act as a critical developmental juncture, unfolding into divergent pathways that range from cumulative biological vulnerability to the cultivation of adaptive resilience. Unlike the interpersonal adversities typically assessed in traditional inventories (e.g., abuse or neglect), the onset of disability or chronic illness during childhood can impose unique functional constraints. Health constraints, for example, restrict children’s involvement in daily activities, school participations, and peer interactions, all of which are crucial for healthy development. Prolonged exclusion from these activities may delay social-functioning development and identity formation compared to that of their unaffected peers. Beyond individual development, these limitations can place significant strain on the family unit, including caregivers and siblings, potentially producing interpersonal tensions and conflicts that further complicate the child’s adaptive coping (Emerson & Llewellyn, 2021; Peer & Hillman, 2014). Furthermore, individuals with early-life disabilities often encounter multiple, overlapping risks rooted in structural barriers, such as limited access to inclusive education, inadequate community resources, and stigmatizing social attitudes. These systemic inequities rarely occur in isolation; rather, their effects compound to undermine health, well-being, and long-term developmental trajectories. That is, childhood disability is not merely a matter of individual pathology, but a dynamic interaction between health conditions and the socio-familial environments that either facilitate or hinder the coping process and developmental outcomes.
More recent studies have revealed associations between childhood health adversities and mental health in later life (Bergmans & Smith, 2022; Smith & Larkina, 2021; Wang et al., 2023; West & Kamis, 2022). For example, West and Kamis (2022) found a consistent pattern of depression development with age among older adults (a mild U-shaped curve, decreasing between ages 50 and 65–70, followed by a gradual increase). However, their study highlighted significantly higher levels of depressive symptoms among older adults with a history of childhood health constraints compared to those without. According to Smith and Larkina (2021), older adults who experienced chronic illness and poor childhood health before age 16 were more prone to developing a negative perception of aging. Similarly, Xie et al. (2023) showed that older Chinese adults who reported childhood malnutrition and limited healthcare access were more likely to perceive themselves as older in both felt age and appearance, with this association being stronger among rural residents. This suggests that early exposure to health threats, regardless of its termination or continuity in old age, can remain a hidden yet chronic, lifelong stressor, limiting positive development over time. As a result, older adults who experienced health adversities during childhood may face more psychological challenges, feel less confident in the aging process, and experience heightened sensitivity to health declines.
On the other hand, older adults who experienced early-life health adversities may have developed greater resilience, tolerance, and perseverance. For those who have survived into old age, it can be assumed that their childhood health problems appear to be, to some extent, coped with and/or adapted to over the life course, either through full recovery or long-term management of a chronic condition. Through the process of overcoming these stressors, they may cultivate coping strategies, both attitudinal and behavioral, that strengthen their capacity to manage health difficulties and broader life challenges. In addition, such individuals may be more inclined to adopt health-promoting behaviors, such as balanced nutrition, regular exercise, and proactive health monitoring, as a compensatory mechanism for early health threats. Disability research often highlights that people with disabilities demonstrate diverse abilities and potential for growth and resilience when facing challenges related to their disabilities (e.g., King et al., 2003; Martz & Livneh, 2016; Scheffers et al., 2020). In this sense, early-life health adversities may not only pose long-term risks but also foster resilience and essential coping strategies that serve as a foundation for navigating the aging process.
The Present Study
Our primary research question focuses on whether severe, chronic early-life health adversities—defined here as six or more months of functional disability—exerts a long-term effect on aging trajectories. Of particular interest are several interrelated domains, including psychological resilience, perceived health, and interpretations of the aging process, all of which serve as important predictors of healthy aging (Jylhä, 2009; Kotter-Grühn et al., 2009; Sargent-Cox et al., 2012; Taylor & Carr, 2021). Psychological resilience is a key coping resource that reflects self-efficacy, a sense of control, and an optimistic view, helping individuals adapt more effectively to life’s challenges (Lee, 2023a; Manning et al., 2016). Because resilience can be cultivated and strengthened through overcoming limitations and adversities, childhood challenges may provide a foundational steeling effect across the life course, thereby manifesting as a psychological asset in later life. These early experiences can also foster a ‘survivor identity,’ characterized by a more positive view of aging, the perception of longevity as an achievement rather than a burden, and a more resilient appraisal of current health in light of difficulties previously overcome.
At the same time, a critical developmental paradox remains. While some individuals develop resilience, others may find that early health adversities engender lasting physiological sensitivities and lower tolerance, leading to more negative health appraisals in later life. This duality underscores that self-rated health is not merely a reflection of physical status (such as symptoms or functional capacity), but rather a dynamic cognitive process influenced by social comparisons and individual resilience (Lazarevič & Brandt, 2020). In this sense, early-life health history acts as a prism, shaping whether aging is viewed through a lens of mastery or a lens of vulnerability. For those who did not experience early-life health constraints, the absence of such experiences may leave them less equipped to manage the psychological burden of age-related functional and physical decline. For these individuals, the onset of disease or significant functional decline in later life may therefore lead to more depression and a diminished sense of perceived health, compared with peers who have already navigated substantial health challenges earlier in the life course.
Acknowledging that the developmental pathways shaped by childhood adversity can unfold in diverse ways, establishing the direct effect through group comparison is a necessary and rigorous first step in identifying the unique legacy of childhood health adversities. To achieve this, we employ a systematic comparison between two groups, allowing us to isolate the impact of early-life disability from subsequent life-course factors. We hypothesize that significant differences in psychological resilience, perceptions of aging, and perceived health will exist between older adults who report childhood disability and those who did not, and that these patterns will persist over time. It is important to clarify that our study does not assume a deterministic, unidirectional pathway of lifelong disadvantage. While embedded within a life-course framework that reinforces the long-term implications of early-life adversities, our analysis moves beyond the traditional cumulative inequality model, which often focuses on how early-life adversities lead to a cascade of socioeconomic deficits (e.g., lower education or income). Instead, we aim to estimate the internal, psychological impact that persists even after accounting for subsequent social or economic attainment. In addition, given the scarcity of longitudinal data that follow individuals who experienced childhood health adversities into older adulthood, our study utilizes retrospective data from a sample of older adults. In doing so, the present study avoids conceptualizing childhood disability as a static label or fixed, lifelong medical condition. Instead, we operationalize it as an adverse developmental experience marking significant disruptions during a sensitive developmental period, whether temporary or enduring. The findings can inform the development of intervention strategies to better support children and adolescents who are navigating the aging process with a history of early-life or lifelong disability.
Methods
Study Design and Sampling
The study used multiple datasets drawn from biennial waves of the Health and Retirement Study (HRS) between 2008 and 2018, yielding a total of 38,654 observations. The HRS is a nationally representative longitudinal survey of adults over the age of 50 in the United States, collecting extensive data on a wide range of topics, including health status (i.e., biomarker data, cognitive assessments, and psychosocial measures), family trajectories, and retirement (https://hrsonline.isr.umich.edu/). The HRS study was approved by the University of Michigan Institutional Review Board. All respondents were asked to read the confidentiality statement and informed sheet, and informed consent was obtained from all study participants. A detailed description of the HRS methodology can be found elsewhere (Faul & Smith, 2017; Servais, 2010). As this study involved secondary data analysis, which is publicly available HRS survey data, the ethics committees of the author's institution waived the requirement for additional ethical approval.
For the current study, two data sources were integrated; the Aggregated HRS Childhood Family and Health dataset, which provides information about respondents’ childhood family environments and health conditions (e.g., childhood disability), and the HRS core survey data including the self-administered Leave-Behind Questionnaire (LBQ) survey. The LBQ focuses on psychosocial and lifestyle factors that allow researchers to construct late-life resilience indexes and subjective aging experiences of the respondents (Smith et al., 2017). Since the childhood disability question was first implemented in HRS 2008 (through HRS 2016), and HRS psychosocial and lifestyle questionnaire is surveyed to same subsample every four years, the current study set HRS 2008 and 2010 as a baseline (Time 1). The baseline sample included respondents who (1) completed the psychosocial and lifestyle questionnaire in either the 2008 or 2010 wave, (2) provided valid information on childhood disability status (yes/no), and (3) were aged 50 or older at baseline. The baseline sample was followed up using data collected in 2012 and 2014 (first follow-up, Time 2) and in 2016 and 2018 (second follow-up, Time 3), retrospectively (see Figure 1 in the Supplemental Material). More recent HRS data (i.e., HRS 2020 and 2022) were not considered to avoid additional bias, as the responses were greatly affected by the pandemic situations.
Measurements
Childhood disability—defined here as chronic functional limitations—was measured using a self-reported yes/no question. Respondents were asked to indicate if they were ever disabled for six months or more because of a health problem before they were 16 years old that prevented them from participating in the usual activities of classmates or other children of the same age. Accordingly, childhood disability was coded as a binary variable (0 = no experience of chronic functional disability during childhood; 1 = experienced disability).
Descriptive Statistics of the Baseline Sample: Mean, Standard Deviations, Range, and %
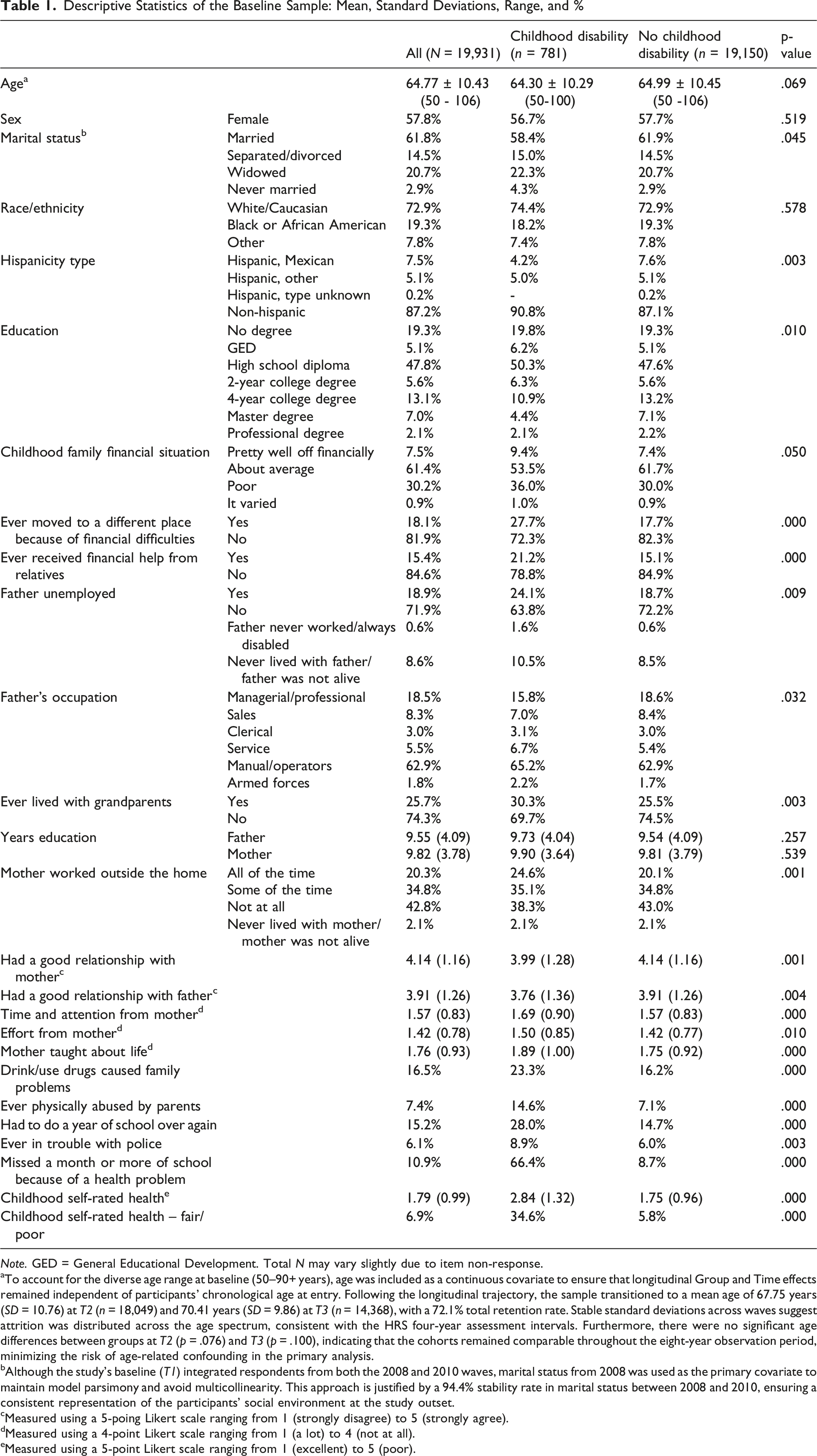
Note. GED = General Educational Development. Total N may vary slightly due to item non-response.
aTo account for the diverse age range at baseline (50–90+ years), age was included as a continuous covariate to ensure that longitudinal Group and Time effects remained independent of participants’ chronological age at entry. Following the longitudinal trajectory, the sample transitioned to a mean age of 67.75 years (SD = 10.76) at T2 (n = 18,049) and 70.41 years (SD = 9.86) at T3 (n = 14,368), with a 72.1% total retention rate. Stable standard deviations across waves suggest attrition was distributed across the age spectrum, consistent with the HRS four-year assessment intervals. Furthermore, there were no significant age differences between groups at T2 (p = .076) and T3 (p = .100), indicating that the cohorts remained comparable throughout the eight-year observation period, minimizing the risk of age-related confounding in the primary analysis.
bAlthough the study’s baseline (T1) integrated respondents from both the 2008 and 2010 waves, marital status from 2008 was used as the primary covariate to maintain model parsimony and avoid multicollinearity. This approach is justified by a 94.4% stability rate in marital status between 2008 and 2010, ensuring a consistent representation of the participants’ social environment at the study outset.
cMeasured using a 5-poing Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree).
dMeasured using a 4-point Likert scale ranging from 1 (a lot) to 4 (not at all).
eMeasured using a 5-point Likert scale ranging from 1 (excellent) to 5 (poor).
Subjective aging perceptions—participants’ positive evaluation of the experiences of their own aging—was measured using a 6-point Likert-scale. Respondents were asked to indicate how much they agree or disagree with each statement describing the way people feel about their age and about the things that happen as they get older. Responses ranged between 1 “strongly disagree” and 6 “strongly agree.” In total, four questionnaire items were used: 1) I have as much pep as I did last year, 2) I am as happy now as I was when I was younger, 3) As I get older, things are better than I thought they would be, and 4) So far, I am satisfied with the way that I am aging. These items were adapted from two sources: the Attitudes Toward Own Aging subscale of the Philadelphia Geriatric Center Morale Scale (Lawton, 1975; Liang & Bollen, 1983) and the Berlin Aging Study (Kotter-Grühn et al., 2009). Higher scores indicate more positive aging perceptions.
Self-rated health was measured using a 5-point Likert-scale questionnaire item. Respondents were asked to indicate how they would rate their health as excellent, very good, good, fair, or poor (Ware & Sherbourne, 1992). The resulting score indicates a higher value as a poor or more negative health evaluation.
Data Analysis
Descriptive statistics were performed using non-weighted sample data to characterize the initial sample structure. Correlation analyses between the key independent variable (childhood functional disability) and late-life outcomes, as well as with covariates, were conducted to examine associations between the measured variables (see Supplemental Tables 3-1 and 3-2, respectively).
To examine longitudinal trajectories in the dependent variables while comparing individuals with and without a history of childhood functional disability, we employed a General Linear Model (GLM) framework, specifically using two-way repeated measures ANOVA. This approach allowed for the simultaneous examination of: 1) between-person differences (main effect of group) to determine if childhood functional disability is associated with stable, overall differences in psychological resilience, aging perception, and self-rated health; 2) within-person changes (main effect of time) to observe general developmental trends as participants aged across the three measurement waves; and 3) the group × time interaction to determine if the rate of change (slope) in the outcomes differed significantly based on the experience of chronic functional disability during childhood. To ensure the robustness of the within-person estimates, we assessed the assumption of sphericity using Mauchly’s test, with Greenhouse-Geisser corrections applied where the assumption was violated. Post-hoc analyses were conducted using Bonferroni corrections to identify specific time-point differences. In addition to null-hypothesis significance testing, we estimated effect sizes using partial eta-squared (
To ensure population-representative estimates and account for the complex survey design of the HRS, analyses were adjusted using respondent-level sampling weights. Specifically, the primary psychosocial variables (i.e., resilience and aging perceptions) were derived from the Leave-Behind Questionnaire (LBQ), which is administered to a rotating 50% subsample; the study’s baseline (T1) integrated respondents from both the 2008 and 2010 waves. Accordingly, a baseline weight was assigned to each participant based on their respective entry wave: for those entering the sample in 2008, the 2008 LBQ respondent weight was applied, while the 2010 LBQ weight was applied to those entering in 2010. This approach ensured that each participant received the appropriate sampling weight from their initial psychosocial assessment, thereby adjusting for non-response and maintaining the integrity of the nationally representative baseline sample.
Missing value analysis was conducted with specific consideration for the HRS split-sample design. For self-rated health, assessed as part of the core survey, missingness was negligible across waves (T1: 0.04%, T2: 0.11%, T3: 0.12%). For psychosocial variables from the LBQ, missingness calculations were based on the wave-specific eligible samples to exclude design-based non-eligibility resulting from the rotating subsample structure. Among the eligible subsample at baseline (T1), total analytical missingness was 25.82% for resilience and 20.80% for positive aging perceptions (see Supplemental Table 2). Over subsequent waves, total variable-specific missingness was 31.88% at T2 and 40.84% at T3 for resilience, and 26.04% at T2 and 36.45% at T3 for aging perceptions; these reflect ongoing non-response and longitudinal attrition among eligible participants. Following HRS conventions, composite indices were treated as missing only if more than half of the component items were incomplete. Although cases with missing values were excluded via listwise deletion, the final analytical sample remains highly powered to detect the specified interaction effects, and the use of LBQ weights ensures the data are representative of the broader population. Data processing and analysis were performed using IBM SPSS Statistics 25.0.
Covariates
Our analytical goal is to isolate the direct impact of childhood health adversities on aging trajectories. To do so, this study adjusted for a comprehensive suite of life-course confounders. We controlled for early-life structural conditions and household functioning. These included childhood socioeconomic circumstances (e.g., father’s occupation, family finances) and family environments (e.g., family structure, parent–child relationships).
In addition to the primary measure of childhood functional disability, we adjusted for subjective childhood health perceptions; the Pearson correlation between these two measures was r = .212 (p < .01), indicating that the two variables share less than 5% of their variance (see Supplemental Table 3-2). This empirical evidence supports our theoretical position that overall health perceptions and functional disability represent distinct dimensions of early-life health status. The inclusion of this covariate ensures that the observed effects are specific to the functional constraints arising from health problems, rather than a general history of poor childhood health.
The analyses also accounted for stable socio-demographic variables as fundamental stratifiers that shape life-course trajectories. These included sex, age, and race/ethnicity (categorized as White/Caucasian, Black/African American, and Others: Native American or Asian), with ethnicity assessed separately (Hispanic or non-Hispanic). Furthermore, the models were adjusted for key adult stratification factors that serve as social determinants of late-life health. These factors included educational attainment (ranging from no degree or GED to professional degrees) and marital status (categorized as married, separated/divorced, widowed, and never married). The inclusion of these variables is supported by a robust body of research linking socio-demographic and adult stratifiers to late-life health, resilience, and well-being (e.g., Grigoraş et al., 2025; Josefsson et al., 2016; Martínez-Moreno et al., 2020; Tang et al., 2025). Detailed measurement information for covariates are provided in Table 1.
Results
Descriptive Statistics
Table 1 presents the descriptive characteristics of the baseline sample stratified by childhood disability status. The baseline sample comprised 19,931 individuals aged 50 and older (Mean = 64.77 ± 10.43 years; range 50–106 years). Of the total sample, 3.9% reported having experienced more than six months of functional disability during childhood (N = 781; N = 539 from HRS 2008 and N = 242 from HRS 2010). Females comprised 57.8% of the sample. In terms of racial and ethnic composition, White/Caucasians accounted for 72.9%, 19.3% were Black or African Americans, and 7.8% identified as other races (i.e., Native American, Asian); 12.8% of the sample considered themselves Hispanic. Of respondents, 47.8% reported they attained a high school diploma, 18.7% maintained a two- or four-year college degree, 9.1% maintained master’s or professional degrees, 19.3% had no degree, and 5.1% completed the General Educational Development (GED). In the overall sample, the majority of respondents were married (61.8%), followed by widowed (20.7%), separated or divorced (14.5%), and never married (2.9%). Because the baseline sample pooled respondents from two study waves (HRS 2008 and 2010), we examined whether marital status varied significantly between these two measurement points. A comparison of the 2008 and 2010 assessments indicated a high degree of stability (94.4%). Therefore, marital status was derived from the 2008 wave, supporting its use as a stable baseline covariate.
As shown in Table 1, stratifying the sample by childhood functional disability revealed systematic differences in sociodemographic profiles, baseline health, and early-life conditions. Most notably, substantial disparities were observed across the majority of childhood family environment measures. This included significantly higher rates of residential instability due to financial difficulties (27.7% vs. 17.7%, p = .000) and a greater dependence on financial help from relatives (21.2% vs. 15.1%, p = .000). Furthermore, compared to those who did not experience health adversities, these individuals reported lower levels of parental support; they were less likely to receive adequate time and attention (p < .001) and effort (p = .010) from their mothers, pointing to reduced emotional and relational resources during childhood. Educational disruption was salient among this cohort: those with childhood disability were twice as likely to repeat a school year (28.0% vs. 14.7%, p = .000) and over two-thirds of these respondents reported missing a month or more of school due to health problems, compared to fewer than one in ten among their peers without childhood disability (66.4% vs. 8.7%, p = .000). Correspondingly, childhood self-rated health was significantly worse in this group, with 34.6% reporting fair or poor health in childhood, compared to only 5.8% of the comparison group (p = .000).
Main Effects of Time and Childhood Disability
Summary of General Linear Model – Tests of Within-Subjects Effects and Between-Subjects Effects
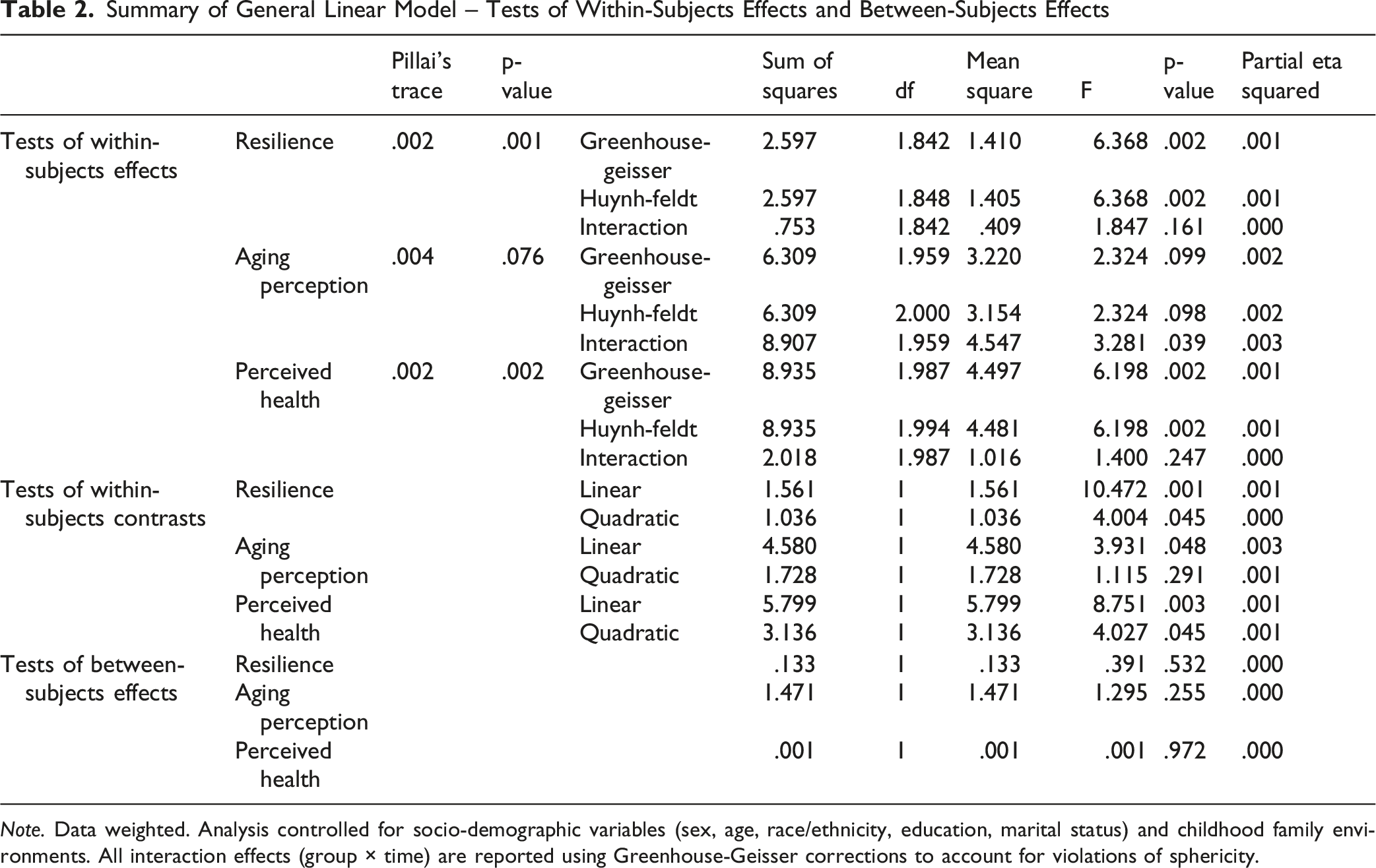
Note. Data weighted. Analysis controlled for socio-demographic variables (sex, age, race/ethnicity, education, marital status) and childhood family environments. All interaction effects (group × time) are reported using Greenhouse-Geisser corrections to account for violations of sphericity.
Within-subjects contrasts indicated a highly significant linear trend for resilience (p = .001), with a smaller but significant quadratic pattern (p = .045). Self-rated health scores also exhibited both a significant linear trend (p = .003) and a quadratic pattern (p = .045), suggesting overall change with curvature across waves. Additionally, although aging perceptions lacked a significant omnibus time effect, its linear contrast was modestly significant (p = .048). Supplemental Figure 2 displays the estimated marginal means for each outcome at all three measurement points by groups.
Tests of between-subjects effects indicated no significant main effect of childhood functional disability on the outcomes when averaged across the three measurement waves (see Table 2). This suggests that there were no stable, overall mean differences in psychological resilience, positive aging perceptions, or self-rated health between the groups over the entire study period. Notably, the partial eta-squared for all three outcomes was negligible (
Mean Score (SD) and Parameter Estimates at Baseline (T1), T2, and T3
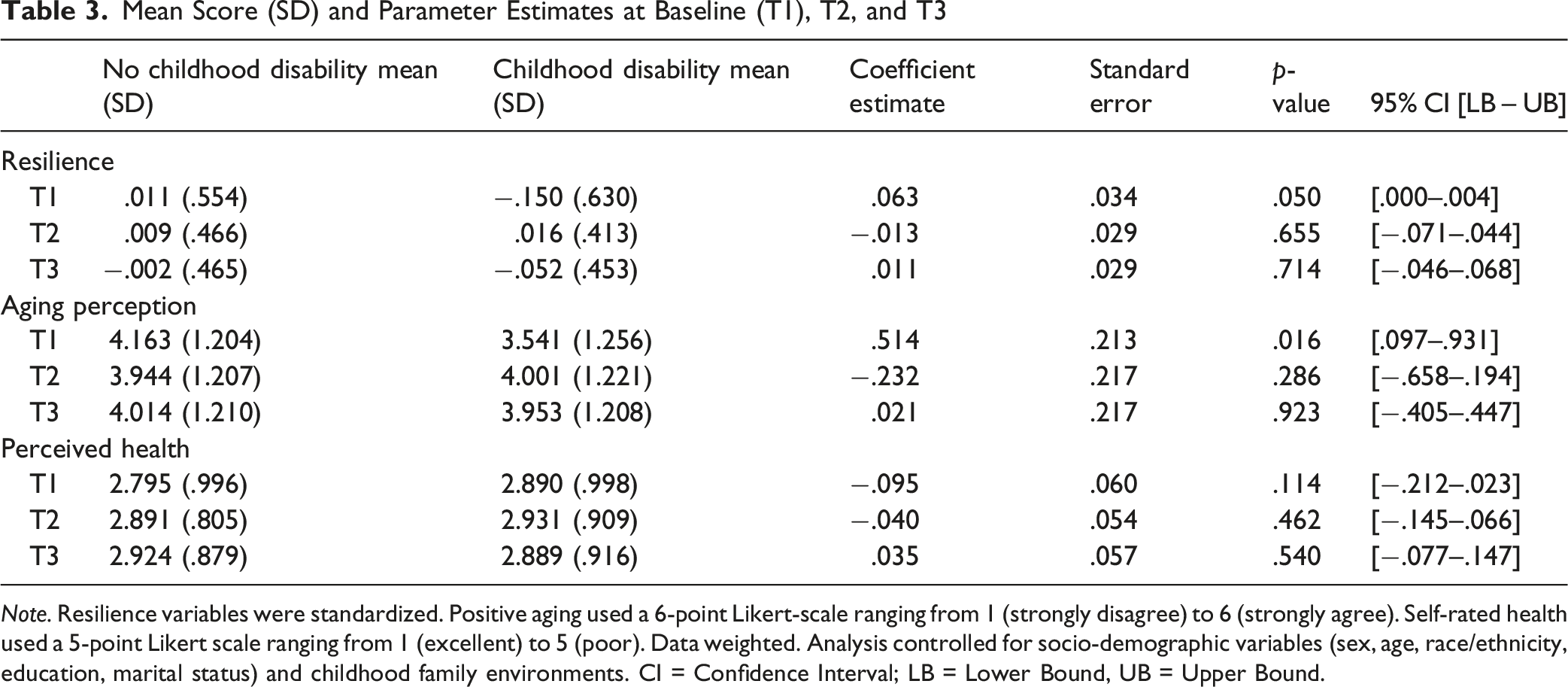
Note. Resilience variables were standardized. Positive aging used a 6-point Likert-scale ranging from 1 (strongly disagree) to 6 (strongly agree). Self-rated health used a 5-point Likert scale ranging from 1 (excellent) to 5 (poor). Data weighted. Analysis controlled for socio-demographic variables (sex, age, race/ethnicity, education, marital status) and childhood family environments. CI = Confidence Interval; LB = Lower Bound, UB = Upper Bound.
Taken together, these results suggest that while childhood disability is associated with a specific deficit in psychological resources at the beginning of the observation period, this disparity did not persist as a statistically reliable main effect when averaged over the full longitudinal course. Detailed parameter estimates for all primary longitudinal models—including unstandardized coefficients (B), standard errors, and significance levels for all covariates—are provided in Supplemental Table 5-1, 2, and 3.
Longitudinal Trajectories and Interaction Effects
To determine if childhood functional disability influences the rate of change in late-life outcomes, we examined the time × childhood disability interaction (see Table 2). While the omnibus test for time indicated a significant overall change in resilience across the three measurement waves, the interaction between time and childhood disability was not statistically significant, F (1.84, 15218.48) = 1.85, p = .161,
For positive aging perceptions, the omnibus main effect of time did not reach statistical significance. However, a significant time × childhood disability interaction was observed, F (1.96, 2417.34) = 3.28, p = .039,
For self-rated health, the omnibus test of time indicated that health perceptions changed significantly across the waves for the total sample. However, the time × childhood disability interaction was not statistically significant, F (1.99, 15571.49) = 1.40, p = .247,
Discussion
The current study examined if early-life experience of disability contributed to psychological resilience, attitudes toward aging, and perceived health in old age. Given that previous studies have provided strong evidence for a long-term, negative association between childhood health adversities and psychological and mental health in older adults (e.g., Smith & Larkina, 2021; West & Kamis, 2022), we might have expected consistently lower levels of resilience, less positive aging perceptions, and poorer self-rated health among those who reported experiencing health threats in childhood. While our results demonstrate significant wave-to-wave variation in these outcomes, childhood disability does not appear to significantly influence these trajectories. Specifically, once covariates were controlled, there were no statistically significant long-term differences in these outcomes between older adults who experienced disability in childhood and those who did not. A significant difference was observed only at baseline, where older adults with childhood disability showed lower levels of resilience and less positive aging perceptions compared to their peers; however, these differences were minuscule. These results indicate that the role of childhood disability in later life is rarely deterministic, extending beyond a simple deficit or disadvantage. Given the advanced age of the study sample, the lack of evidence for a direct association may suggest that the influence of early-life health adversities either attenuates across the life course or operates through mechanisms not captured in the present analyses.
Despite the limited impact of childhood functional limitations on later-life outcomes, our analysis showed inconsistent changes in resilience, aging perceptions, and perceived health over the 8-year follow up period. Consistent with existing literature suggesting that resilience remains relatively stable compared to other resources in later life (Fuller & Huseth-Zosel, 2021; Taylor & Carr, 2021), resilience scores in the subsample without childhood disability remained largely stable, exhibiting only a slight decline. In contrast, the subsample with a history of childhood health threats showed a marginal improvement in resilience at the first follow-up, followed by a slight decline at the second. For these individuals, resilience may be less robust and more affected by other factors, compared to their unaffected peers. Fridman et al. (2011) noted that while survivors of childhood adversities develop resilience and adaptability, they may remain vulnerable to the specific challenges that come with aging. While aging perceptions showed no significant omnibus change across time, it did exhibit a modest linear trend that was consistent with the changes observed in resilience. Descriptively, older adults without childhood disability experienced a decrease in positive aging perceptions at the first follow-up, with a slight rebound at the second; conversely, those who experienced chronic functional limitations during childhood demonstrated a greater improvement between baseline and the first follow-up, followed by a decline. These diverging, nonlinear patterns highlight the complex and dynamic nature of resilience and aging perceptions among older adults, particularly, for those with early-life health threats, as they might navigate the unique stressors of later life through a combination of hard-won adaptability and heightened sensitivity to age-related challenges.
Repeated measures of perceived health indicated the most notable change over time. For those with chronic functional disability during childhood, their self-rated health did not differ significantly from peers without such experiences. Rather, perceived health of this group remained relatively stable over the eight-year period, whereas their comparing group exhibited a more pronounced decline, leading to a convergence of trajectories by the final measurement point. These findings contrast with the observed resilience patterns, where resilience remained stable among those without such a history, but showed more irregular patterns among those with a history of childhood disability. As older adults generally encounter age-related health declines (Diehr et al., 2013; McCurry et al., 2002), the linear, negative development of self-rated health observed in those without childhood health adversities aligns with existing literature. What is particularly intriguing is that older adults with such a history did not follow this normative decline. This non-normative trajectory suggests that individuals with early health adversities may have already adapted or recalibrated their health expectations and self-assessments over the life course. In contrast, older adults without such a history may consider new health threats as major challenges, resulting in a sharper negative shift in self-assessment. This interpretation is consistent with the greater decline in positive aging perceptions observed in the unaffected group. Given that self-rated health is a multifaceted, subjective assessment based on diverse factors, including physical functioning, disease status, pain, and mental health (Lazarevič & Brandt, 2020), replicating these analyses while incorporating additional health indicators would yield a more comprehensive understanding of how early-life health constraints shape health trajectories in older adulthood.
In addition, it is worth noting that there were significant differences between the two groups regarding childhood family and health conditions. Overall, the subgroup with childhood functional disability reported being financially less affluent and having more limited parental support compared to their peers without such experiences, suggesting that childhood health adversities often cluster with other forms of socio-environmental disadvantage. Children coping with health adversities require extra support within the household and from medical to social services. However, while coping with health limitations in their childhood, many older adults—if not most—likely also struggled with limited household resources and multifaceted constraints, a reality particularly pronounced for older cohorts with fewer social safety nets. According to West and Kamis (2022), older adults who experienced childhood disabilities are significantly more likely to report childhood depression and lower socioeconomic status. That is, while some individuals with childhood health adversities may develop resilience and adaptive capacities over the life course, these pathways are deeply influenced by the broader contexts of social support and resource availability.
Study Limitations and Directions for Future Research
A primary limitation of this study concerns the use of secondary data based on retrospective self-reports. Measures of childhood functional disability and socio-familial factors may be subject to recall bias, wherein participants’ current psychological or health status influences their reconstruction of early-life events. While retrospective measures are a staple of in life-course research, they lack the objective verification provided by prospective medical records or administrative data. For instance, our sample included a few cases with longitudinal inconsistencies in their reports of childhood health across the three measurement points. Vuolo et al. (2014) explicitly highlighted such inconsistent responses within HRS data and their potential impact on life-course analysis. Furthermore, Greenfield (2021) noted that responding to questions on childhood adversities should be carefully addressed and designed with cultural sensitivity, particularly for minority groups, considering the societal and cultural system back then, which could determine how adversities were embedded and evolved across different racial and ethnic groups. Therefore, the recollection of childhood health in old age should be approached with cultural and contextual specificity.
Relatedly, the observed impact of childhood health adversity may depend on how the construct is operationalized. Previous studies using HRS data have employed various measures to capture childhood health. For instance, Smith and Larkina (2021) used both the number of childhood chronic illnesses and self-rated childhood health to predict self-perceptions of aging (SPA) in later life, and found that the number of chronic illnesses was significantly associated with SPA, whereas self-rated childhood health was not. Using early HRS survey data, Blackwell et al. (2001) showed that infectious and non-infectious diseases in childhood are associated with increased morbidity (i.e., cancer, lung disease, cardiovascular conditions, and arthritis/rheumatism), though these associations varied by diagnosis. Coyle and Putnam (2017) noted that while various childhood health indicators (e.g., chronic conditions and functional limitations) are mutually correlated, childhood disability status may be a less potent predictor of later-life health status compared to adult-onset measures. This suggests that self-reported, retrospective measures of childhood disability may not consistently show a direct association with health outcomes in later life. Since the current study conceptualizes childhood disability as exposure to a significant adverse experience during a critical developmental period—rather than a clinical diagnosis or a lifelong status—the use of a functional disability measure is sufficient to capture this scope. However, the use of a stand-alone, binary nature of this measure without incorporating additional indicators, such as chronic conditions with typical childhood onset, may restrict our ability to capture fully the complexity of early-life health experiences. Furthermore, this simple classification may include both individuals whose impairments were temporary and resolved, as well as those with enduring conditions, potentially introducing heterogeneity within the affected group. Thus, this study possesses inherent limitations in its ability to differentiate between the impacts of chronic, lifelong disability and those of shorter-term functional disruptions.
Additionally, study findings might be subject to mortality selection and survival bias. Specifically, the childhood disability group represents a unique cohort of individuals who successfully navigated the increased mortality risks associated with early-life health problems. This healthy survivor’ effect suggest that individuals with the most severe health problems, or those with lower physiological and psychological resilience, may have died prior to reaching the age of eligibility for the HRS. The descriptive observation of a compressed age distribution within the disability group partly supports this potential mortality selection at advanced ages; while mean ages were comparable, the childhood disability cohort exhibited a narrower age range at the oldest extreme. Consequently, our results should be interpreted as reflecting the resilience trajectories of older adult survivors rather than a universal representation of all individuals exposed to early-life disability.
Finally, our analysis found insufficient evidence to account for unexpected longitudinal shifts, specifically the quadratic trends observed in resilience and self-rated health, between the two follow-up points. It remains unclear whether these patterns represent stochastic fluctuations or are driven by unmeasured variables. Consequently, we interpret these findings cautiously as short-term longitudinal trajectories rather than universal, age-based developmental patterns, particularly given the sample’s wide age range (50–90+ years), which encompasses distinct and heterogenous phases of the aging process. Future research should employ a more extensive observation period to fully characterize how these variables evolve and diverge in relation to early-life adversity. It is also important to note that this limitation stems, in part, from the study’s focus on group-level disparities rather than specific intermediary pathways. Our models excluded potential mediators that may function as mid- or late-life compensatory resources such as lifestyle factors, social support, and broader environmental influences. Building on these delimitations, and noting that several covariates demonstrated significant associations with the outcomes, future research should explore the roles of both included stratifiers and omitted mediators to identify the underlying mechanisms of change. To this end, a companion study is currently examining the potential moderation and mediation effects of the covariates laid out in the current analysis and other life course factors. This approach directly addresses the lack of a conceptual linkage between childhood health adversities and late-life outcomes, which is crucial for bridging the several decades that separate these life stages.
Supplemental Material
Supplemental Material - Can Childhood Health Adversities Determine Trajectories of Aging? Findings From the Health and Retirement Study
Supplemental Material for Can Childhood Health Adversities Determine Trajectories of Aging? Findings From the Health and Retirement Study by Sunwoo Lee in Research on Aging
Footnotes
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
Author Biography
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.