
Abstract
This systematic literature review investigates contraceptive decision-making among Bangladeshi Muslim women while looking at how households discuss reproductive health, especially birth control, and how gender, power, religion, and socio-economic factors can affect these discussions. It also challenges traditional viewpoints on women's empowerment that focus on limits by examining quantitative, qualitative, and mixed-methods research conducted between 1975 and 2025. The findings show that there is a substantial rise in contraceptive prevalence from approximately 17% in 1975 to over 60% by the mid-2010s. Still, women's contraceptive choices always remain subject to debate within patriarchal and religious household environments. Drawing on Mahmood's ideas about piety and agency (2005), Kabeer's ideas about empowerment (1999), and Connell's Gender and Power Theory (1987), the analysis brings together feminist and anthropological perspectives to question liberal ideas that equate agency with individual freedom. Women deal with these boundaries by discussing, reinterpreting religious texts, and choosing birth control methods. Also, education, media exposure, and participation in household decision-making are consistently and positively associated with higher adoption rates. The findings explore the importance of understanding contraceptive behaviour as a socially embedded process, with implications for reproductive health research and programmes that seek to engage women's lived moral and relational realities.
Keywords
Introduction
A complicated mix of gender roles, religious beliefs, and social and economic factors affects how Muslim women in Bangladesh make decisions about birth control. Bangladesh has made significant advances in family planning since 1970, but families are still negotiating, and male dominance and moral expectations about family planning remain important (Hossain, 1998; Rahman et al., 2014). Women in many Muslim families do not make decisions on birth control on their own. Instead, they talk about it with their spouses, in-laws, and religious rules that say how to be a good parent, a good woman, and a good Muslim (Atighetchi, 1994; Mahmood, 2005).
The use of contraceptives is positively correlated with women’s education, employment, media access, and involvement in household decision-making, according to a large body of research. Women who report having joint or autonomous decision-making authority are more likely to use contraception, according to national surveys, especially the Bangladesh Demographic and Health Survey (BDHS). Much qualitative research shows that male dominance in families, particularly in Muslim families, frequently restricts women’s contribution and viewpoint in family decisions. Low-income families frequently associate religion with authority and use it to justify giving boundaries on women’s options (Alam et al., 2018; Chowdhury et al., 2023; Hossain, 1998). For instance, in Saudi Arabia, a lot of women feel like their husbands or in-laws are forcing them not to use birth control. Most of the time, family members use religious or reproductive reasons to back this up (Alomair et al., 2023). Also, in Somalia, despite social pressure to have prominent families as well as religious constraints that contraception use is a “non-Islamic” practice, some women seek contraceptive techniques because they understand the health benefits of spacing out children (Gele et al., 2022). This practice challenges ingrained religious and cultural myths and shows a growing knowledge and assertion of reproductive rights of women, with Bangladesh being no exception. Since the 1970s, Bangladesh’s family planning programs have increased access to contraceptives, but male dominance in decision-making and religious misconceptions continue to limit uptake (Pathfinder, 2022).
Most of the scholars conceptualize the tension through a binary lens where women are either empowered or constrained by patriarchal norms. This idea keeps religious belief as an external barrier to contraceptive use, and not using it is interpreted as a sign of disempowerment (Chowdhury et al., 2023). Such interpretations, however, oversimplify women’s lived experiences in many cases and overlook how reproductive decisions are made within culturally meaningful and morally legitimate forms of action.
Feminist and anthropological scholarship offers alternative ways of understanding agency in constrained contexts. In Kabeer’s (1999) empowerment paradigm, agency is a process that provides women with access to resources and the capacity to act within established boundaries. On the other hand, Connell (1987) focuses on how unequal family relations influence reproductive decisions. Also, Mahmood’s (2005) work further challenges liberal presumptions by defining agency as women’s expression through their behavior, which conforms to religious norms rather than defies them overtly.
Even with these new facts, there is not enough systematic research looking at how religion, home power, and women’s agency all work together to affect Muslim women’s decisions about contraceptives in Bangladesh. The current literature predominantly emphasizes identifiable indicators of empowerment, while insufficiently addressing the role of faith in quotidian household decision-making (Chowdhury et al., 2023).
By combining data from 44 studies published between 1975 and 2025, this systematic review fills these gaps. Drawing on Connell, Kabeer, and Mahmood’s notion of agency, this study explores how Muslim women in Bangladesh make contraceptive decisions in patriarchal, religiously educated environments. The central argument here is that women’s contraceptive behavior should not be understood solely in terms of empowerment or barriers. Rather than that, it should be understood as reflecting forms of situated agency shaped by faith, family dynamics, and structural inequalities.
Materials and Methods
Study Design
This study is a systematic literature review examining contraceptive decision-making among Muslim women in Bangladesh. Additionally, by focusing on context, theory, and intervention assessment, the SQUIRE 2.0 (Standards for Quality Improvement Reporting Excellence) framework further directs transparent reporting (Ogrinc et al., 2015).
Search Strategy
Creating a search strategy is an iterative process that involves ongoing evaluation and improvement, which is seen as a cultivable and practicable art. A thorough search entails conventional procedures, such as creating search strings, browsing through bibliographic databases, searching for grey literature, and hand searching; however, there is no single prescribed method (Aromataris & Riitano, 2014).
Preliminary Literature Search Strategy
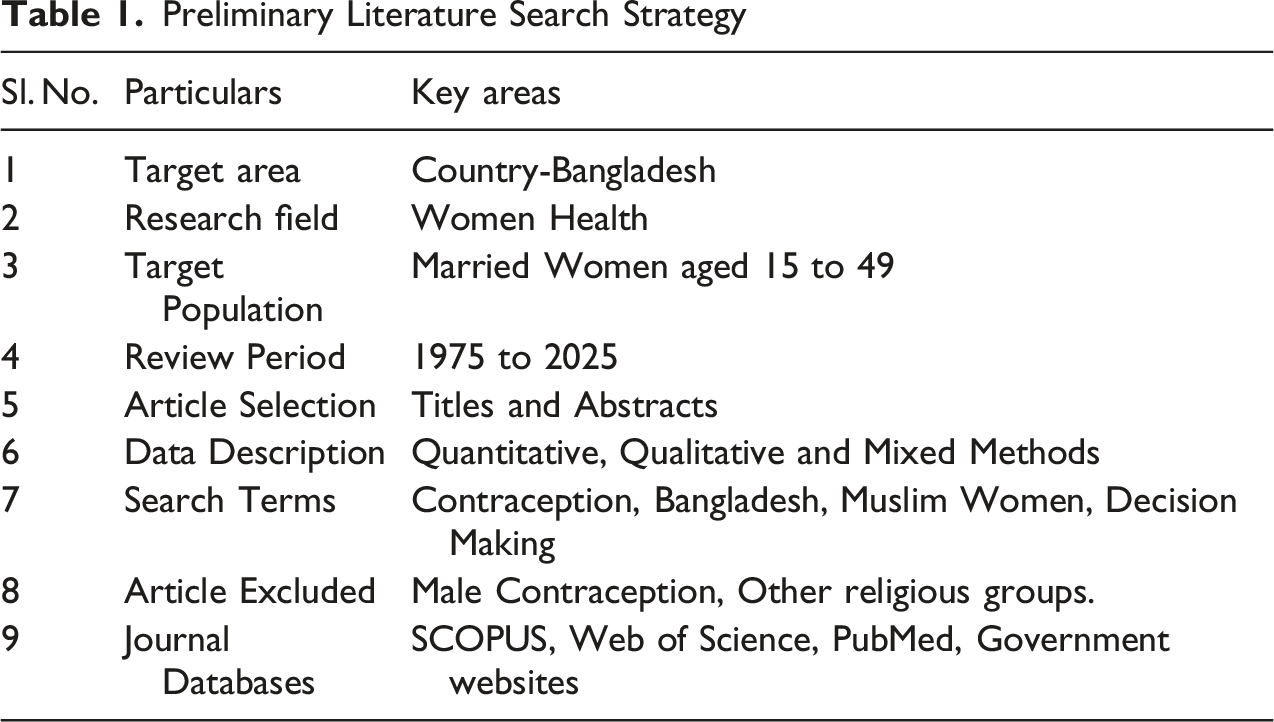
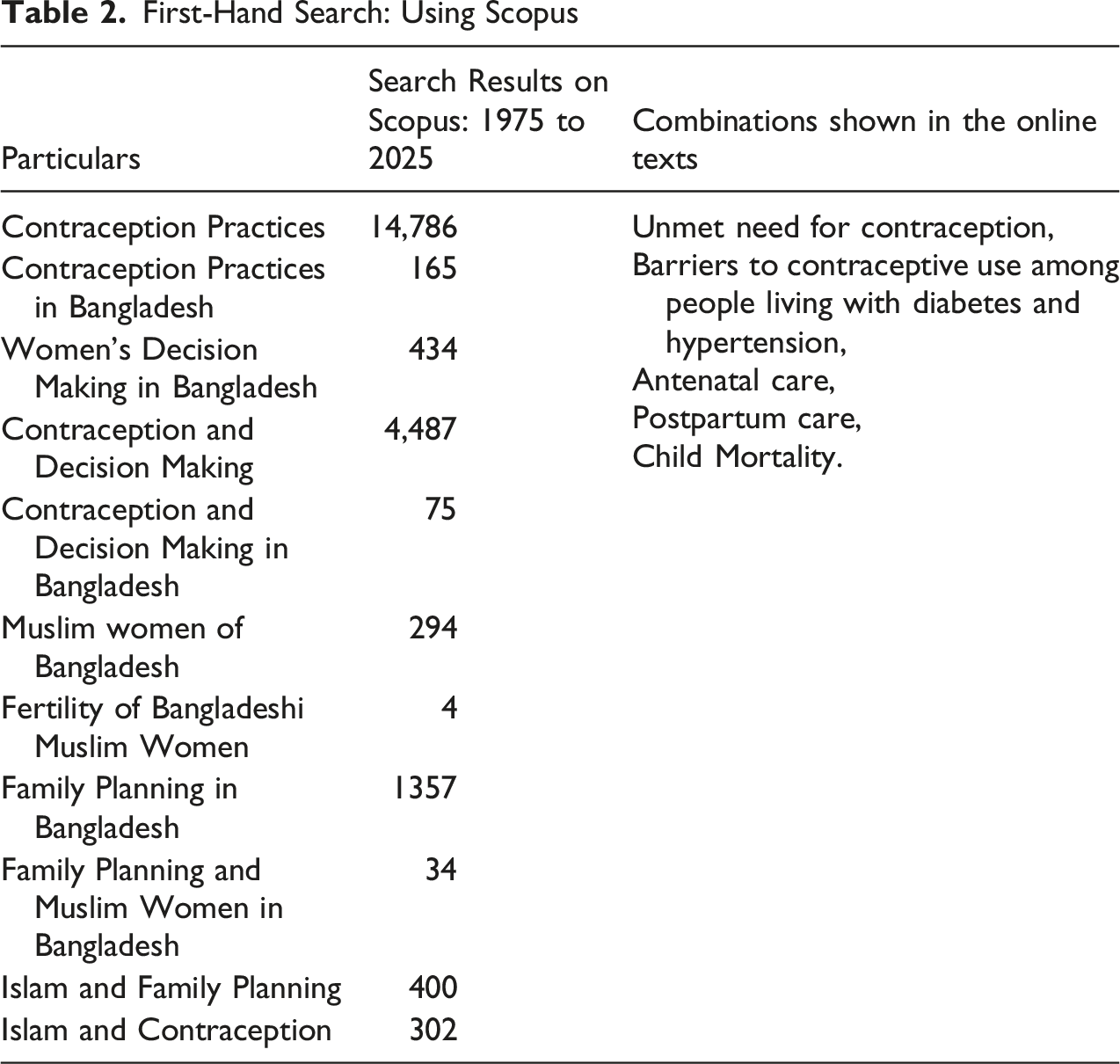
The review followed PRISMA 2020 guidelines to ensure transparency and reproducibility (Page et al., 2021), which enhance clarity, transparency, and quality in health research and support comprehensive systematic analyses of interest to the research community (Sohrabi et al., 2021). A preliminary scoping search was conducted across Scopus, Web of Science, PubMed, and Google Scholar to assess the current literature and optimize the search approach. When we search for “contraception practices,” we got 14,786 results in Scopus, 4,063 in Web of Science, and 19,526 in PubMed. In Scopus, the phrase “contraceptive use and decision making” brought up 4,487 documents. In Web of Science, it brought up 1,673. Using the same keywords, PubMed returned 1,913 results, whereas Google Scholar returned about 61,200.
At this point, it was hard to screen publications solely by title and abstract, since many studies used vague or broad search terms that did not clearly address how people make decisions about contraception. To improve specificity and align the search with the research question, additional keywords related to geographical context and population—including “Bangladesh” and “Muslim women”—were incorporated. This refined search yielded 6 documents in Scopus, 23 in PubMed, 2 in Web of Science, and 17,800 in Google Scholar.
First-Hand Search: Using Scopus
Quality Appraisal of Included Studies
A planned quality assessment was conducted for the included studies in the synthesis to assess the methodological rigor of the literature. The Mixed Methods Appraisal Tool (MMAT, 2018 version) was used to maintain consistency across study types by including qualitative, quantitative, and mixed-methods designs. The MMAT enables systematic evaluation of methodological quality by analyzing essential elements of study design, data collection, analysis, and interpretation.
Each study was independently evaluated according to the MMAT criteria based on its methodological classification (Clark et al., 2025). Based on the lucidity of their research inquiries, the appropriateness of their data sources, the adequacy of their analytical techniques, and the interrelationships among their data, analysis, and conclusions, the study was assessed.
The included studies had good to acceptable methods in both qualitative and quantitative studies. On the one hand, quantitative research, including national surveys, had a robust sample within Bangladesh; on the other hand, qualitative studies revealed inconsistencies in the depth of reflexivity and the honesty of analytical methodologies.
Eligibility Criteria
The eligibility criteria were those studies (1) that concentrated on Bangladesh; (2) studies that looked at the use of contraceptives or reproductive decision-making; (3) studies that included Muslim women as the majority or primary population; and (4) studies that dealt with religion, gender relations, or household dynamics. Studies focusing exclusively on service delivery, male-only perspectives, or non-Muslim populations without disaggregated analysis were excluded.
Study Selection and Data Extraction
To enhance future research, a systematic review is a developed, rational, and thorough assessment of the literature or “existing research” (Thamminaina et al., 2020). Titles and abstracts were assessed for relevance after duplicates were removed, and the full texts were then evaluated. An organized template that included the study design, sample characteristics, methodologies, and key findings on religion, power dynamics, and agency was used to extract the data. The authors repeatedly cross-checked inclusion decisions and documented the reasons for exclusions transparently.
Findings
The main conclusions of the systematic review are presented in this section, which is divided into three subject areas that recurred often in the included studies: gender relations and family decision-making, socioeconomic and demographic impacts, and religion, faith, and moral reasoning. Using data from national surveys and qualitative research, this section summarizes the main conclusions of the systematic study and explains empirical trends in Muslim women’s decision-making regarding contraception in Bangladesh. Themes were refined through iterative comparison across studies to ensure analytic consistency (Iyekekpolor et al., 2026).
Contraceptive Decision-Making Within the Household
According to both qualitative research and national surveys, the majority of Bangladeshi women’s contraceptive and other reproductive health-related decisions are made by families where it is mainly influenced by older members, husbands, and ideas about gender roles that are culturally accepted. Early BDHS statistics showed that there was little marital communication on contraception in the 1990s, and husbands frequently had more control over family planning and women’s decisions (Mitra et al., 1994; NIPORT, 2001). Although more recent data show substantial increases in joint decision-making, reaching nearly 80% by 2022, this shift does not necessarily mean equal power relations (NIPORT et al., 2021; NIPORT & ICF, 2023).
Some studies show that women try to convince their families and husbands by negotiation or use discreet contraceptives to affect reproductive outcomes, especially in situations where overt opposition is socially restricted (Alam et al., 2018; Hossain, 1998).
On the other hand, rural women have to face additional constraints because of low access to information, stronger patriarchal norms, and restricted mobility, which together reduce autonomy in reproductive decision-making (Alam et al., 2018). Also, Gender dynamics continue to play a significant role in households; higher use of contraceptives is mainly linked to interspousal communication and shared involvement in decisions about health care, child-rearing, and household mobility (Islam, 2018; Rahman et al., 2014). Social networks also play an important role, as community- and network-based interventions are more effective than household-level outreach alone (Kincaid, 2000). Boundaries of gender norms including the acceptance of domestic violence count as indicators of structural inequalities that influence reproductive, specifically contraceptive, decisions, even during an increasing number of contraceptive uses (NIPORT, 2008a; Sarwer et al., 2025). Older women and those with higher levels of education, along with greater control over finances and household decisions, indicate a greater influence on reproductive decision-making (Biswas et al., 2017). Different studies highlight intricate power relations within couples, families, as well as an inadequate emphasis on men’s roles in reproductive decision-making (Brandão et al., 2020; Karp et al., 2020).
Socioeconomic and Demographic Influences
Demographic and socioeconomic factors significantly influence women’s ability to make reproductive decisions. The BDHS, UHS, and fertility surveys consistently show that education, wealth, media exposure, employment, and having the final say in household decisions are all positively linked to using birth control (Bhowmik et al., 2024; Hossain, 1998; NIPORT, 2001, 2002, 2005, 2008a, 2013, 2016; NIPORT & ICF, 2020).
Women with more education and those whose husbands are also educated take birth control much more often (NIPORT, 2008b). This is because women have more access to information and more power in their homes (NIPORT, 2001; NIPORT, 2013). Media exposure, especially television, has historically been a major way to spread information about family planning. However, the recent decline in traditional media use raises concerns that not everyone will have access to reproductive health messages (Bhowmik et al., 2024; Hossain, 1998; NIPORT, 2001, 2005, 2008a, 2013, 2016; NIPORT & ICF, 2020).
Employment and financial situation increase women’s capacity to engage in reproductive decision-making; yet, control over earnings does not invariably align with workforce participation (NIPORT, 2013; NIPORT & ICF, 2023).
There are still big differences between rural populations, slum dwellers, and women with low literacy, which shows how poverty and spatial inequality still make it hard for people to use contraceptives even though the country has made progress (Chowdhury et al., 2023; NIPORT, 2008b).
Religion, Faith, and Cultural Norms
Religion constitutes an important dimension of contraceptive decision-making among Muslim women in Bangladesh. Islamic texts do not explicitly prohibit contraception but emphasize marriage, family, and procreation as social ideals (Atighetchi, 1994). Hadith literature offers a variety of interpretations, such as whether coitus interruptus is allowed, which allows for doctrinal flexibility, as shown in various research (Atighetchi, 1994).
Historical survey data indicate that Muslim women have consistently exhibited higher fertility rates and lower contraceptive usage in comparison to non-Muslim women, particularly in earlier decades (NIPORT & International Statistical Institute, 1978). In the 1990s and early 2000s, religion was clearly given as a justification for not using, but by 2014, it was much less common (Mitra et al., 1994; NIPORT, 2001, 2005, 2016). Younger women nevertheless say they feel more religiously constrained, which suggests that faith affects reproductive behavior differently depending on the generation and stage of life.
Regional and qualitative studies indicate that religion frequently functions indirectly by strengthening patriarchal control rather than serving as an independent barrier. Cultural conservatism, especially in areas like Chittagong, makes it harder for spouses to communicate and access information about family planning (Mitra et al., 1994). Research on rural communities and displaced populations, such as Rohingya refugees, indicates that religious misconceptions and patriarchal norms lead to reduced birth spacing through contraceptive use (Alam et al., 2018; Islam & Habib, 2024; Khan & Khanam, 2023). At the same time, studies show that women are using family negotiation and hidden birth control methods more often as awareness and access have grown through government and non-governmental efforts (Kabeer, 1999; Thummalachetty, 2016).
Discussion
This discussion uses feminist and anthropological theories of gender, power, empowerment, and piety to look at how Muslim women in Bangladesh make decisions about contraception. It shows that these decisions are not just signs of empowerment or constraint but also of situated agency.
The literature we looked at shows that deciding on contraception is more of a relational process that is affected by power dynamics in the family than it is an individual choice. In line with Connell’s Gender and Power Theory, men maintain formal authority in several households, influencing reproductive outcomes despite the increasing prevalence of shared decision-making. However, the findings also show that women have power through negotiation, persuasion, timing, and selective disclosure. It goes against the idea that agency is only about making decisions on one’s own.
Kabeer’s empowerment framework helps us understand how access to education, jobs, and media can enable women to negotiate more effectively within existing social systems. Instead of breaking down patriarchal authority, these materials help women manage their own power so that they can have an impact on reproductive outcomes even when they are limited.
Religion makes this process even more difficult. Following Mahmood’s conceptualization of piety and agency, women’s involvement with Islam ought not to be perceived as mere passive submission or resistance, but rather as ethically motivated action. Women find ways to restrict their reproduction that fit with their religious beliefs, such as by changing the meaning of religious teachings and using birth control in secret.
However, from time to time, though there are religious restrictions, women started to negotiate because of their education, social media, and social network expansion, and religious text reinterpretation, despite the ongoing influence of patriarchal norms on reproductive behavior.
Limitations
This review is subject to few limitations. The inclusion of English-language studies only may have excluded relevant Bangla-language research. Furthermore, reliance on published studies limits the ability to capture the full contextual depth of women’s lived experiences, particularly in underrepresented regions (Oladimeji et al., 2026).
Conclusion
Taken together, the findings demonstrate that Muslim women’s contraceptive decision-making in Bangladesh reflects negotiated, morally grounded agency rather than an absence of empowerment. Household power relations, socioeconomic resources, and religious reasoning intersect to shape reproductive choices that are pragmatic, adaptive, and contextually rational. Framing these practices through a deficit lens risks misrecognizing women’s strategies as failure, rather than as forms of agency exercised within constrained social realities. Even though a few women say that religious prohibitions are the reason they don’t use birth control, faith still affects how people use birth control in indirect and socially ingrained ways. Religious norms, combined with expectations, power, and surveillance, determine how and when women can pursue their reproductive goals. These findings highlight the need to distinguish between declining doctrinal opposition and the enduring moral influence of religion in everyday decision-making.
Considering all the themes collectively, it highlights that several factors influence contraceptive behavior in Bangladesh. Instead, it depicts a complex of interconnected socioeconomic circumstances, religious convictions, gendered power dynamics, and women’s adaptive agency. Despite structural barriers, women employ strategies of resistance and negotiation. Mahmood’s (2005) notion of non-Western piety explains how women reinterpret Hadiths or deploy covert contraceptive practices to reconcile religious devotion with reproductive control. Women are constrained, but their reliance on peer networks to share information (even if mixed with myths) shows informal strategies such as relying on social networks for information, haring and circulating experiences, etc. to navigate reproductive health (Islam & Habib, 2024; Kamal & Islam, 2011). Women’s quiet negotiations with husbands, discreet use of methods, and reliance on social networks illustrate agency within constraint. This aligns with Kabeer’s (1999) theory of agency as embedded in resources and relationships, not simply individual choice. The persistence of non-use among one-third of “fully empowered” women (NIPORT, 2016) suggests that male vetoes and cultural norms continue to limit outcomes, even when women possess knowledge and autonomy.
The sources that support women’s autonomy, including wealth and basic education, are still being overruled by patriarchal dominance and religious conservatism in every sector. Women demonstrate resilience by navigating and reinterpreting these contradictions, but they also reveal structural constraints.
These findings suggest that family planning initiatives should incorporate equity-focused, gender-transformative, and faith-sensitive strategies alongside services. Initiatives should add men, people from different religious backgrounds (possibly hujurs, pandits, etc.) and reduce regional inequities, especially in slum and refugee contexts. Although “religious prohibition” as a cause for non-use has been reported to wane, its prevalence among younger women and disadvantaged groups indicates that cultural engagement and empowerment must go hand in hand.
Future studies should examine how reproductive decisions are made over time within homes and moral communities, rather than focusing solely on individual-level indicators of empowerment. Qualitative longitudinal research would be beneficial for showing how women’s methods change across different life stages. Family planning interventions informed by these insights are more likely to be effective if they engage religious discourse and household dynamics rather than treating faith as a residual barrier.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available in Google Scholar, Scopus, and Web of Science for this article.