
Abstract
The purpose of this study was to determine the effect of a motivational interviewing intervention (MII) on regimen adherence and diabetes markers among African Americans with diabetes. Sixty-two participants were assigned to the usual care (UC; n = 36) or MII (n = 26) groups. UC participants received the usual clinic care. MII participants received a maximum of six motivational interviewing (MI) sessions over 3 months. Outcome variables were obtained at baseline and 3-month follow-up. Data were obtained using medical records, self-reports, and glucose monitor and accelerometer print-outs. MII significantly increased the odds of participants adhering to recommended physical activity level (66.7% vs. 38.8%, odds ratio = 2.92, 95% confidence interval = [1.6, 14.3], p = .018) and significantly decreased glucose levels (p = .043) and body mass index (p = .046) over time when compared with UC. Findings support using MI as an intervention for improving health outcomes and regimen adherence rates among the study population.
An estimated 25.8 million persons in the United States have diabetes mellitus (American Diabetes Association [ADA], 2012b) and 90% to 95% of them have type 2 diabetes mellitus (T2DM; National Institute of Diabetes, Digestive, and Kidney Diseases, 2012). T2DM is associated with an insulin deficiency and/or insulin resistance rather than a total deficit of insulin (Chlebowy & Wagner, 2005). T2DM is a significant chronic health problem among African Americans in the United States; approximately 14.7% of African Americans above the age of 20 are living with diagnosed or undiagnosed diabetes (ADA, 2012a). African Americans are disproportionately affected by diabetes and are 1.8 times more likely to develop diabetes than non-Hispanic Whites (ADA, 2012a). They experience higher rates of diabetes-related complications such as kidney disease, blindness, amputations, heart disease, and stroke than other ethnic groups. Moreover, there is growing concern among health care providers about the rising incidence of diabetes and diabetes-related complications among African Americans. Higher rates of diabetes-related complications among African Americans may be due to factors such as financial barriers, limited health care, or heredity (Chlebowy & Garvin, 2006). It is essential to better understand the underlying mechanisms for the existing health disparity and how to reduce it in this vulnerable population.
Motivational Interviewing (MI)
Lifestyle modifications are recommended for individuals with diabetes as part of self-management of the disease (ADA, 2014). It is important for many individuals to modify their self-management behaviors to more effectively manage T2DM. Behavioral strategies differ greatly in their effectiveness, and individuals’ responses vary depending on their readiness to engage in behavior change (World Health Organization, 2012). Adherence to prescribed treatment regimens is important for individuals with T2DM to maintain normal glycemic control and prevent short-term and long-term diabetes-related complications. Although evidence supports the benefits of using behavioral strategies to improve T2DM adherence, few studies have evaluated the effects of MI on adherence to T2DM treatment regimens among African Americans.
MI is a research-supported method that improves patient adherence to change plans and health-related patient outcomes. MI is defined as a directive, person-centered approach that increases intrinsic motivation to change by identifying and piquing the importance of behavioral change and confidence in the ability to change a behavior (Miller & Rollnick, 2004, 2013). It facilitates adherence to prescribed treatment for chronic conditions such as T2DM by helping people resolve ambivalence related to engaging in health- or illness-related behaviors, fostering motivation to change behaviors, and moving ahead with a plan for behavior change (Miller & Rollnick, 2002). It is important to note that since the implementation of this study, Miller and Rollnick (2013) further suggested that MI consists of four higher-level processes: (a) focus on a single behavior for change; (b) fully engage with the client using client-centered methods to achieve a number of strategic objectives moving the client toward commitment to change; (3) evoke client language that favors the importance of change, confidence in changing, commitment to change or change plan ideas; and (4) negotiate and gain commitment to adhere to a plan of change.
Miller and Rollnick’s (2002) work provided the framework for this study. MI involves fidelity to (a) a “spirit” (or style) of interviewing, (b) four counseling principles, and (c) several nuanced counseling techniques that are congruent with its spirit (Miller & Rollnick, 2002). The MI counseling spirit is defined as follows: (a) collaborating with the patient and avoiding direct confrontation; (b) honoring the patient as the expert on themselves, minimizing unsolicited education, and asking permission to educate; and (c) emphasizing patient autonomy and competency while minimizing an authoritative role (Miller & Rollnick, 2002). The MI spirit is comprised of four key principles: (a) expressing empathy, (b) developing discrepancies, (c) rolling with resistance, and (d) supporting self-efficacy (Miller & Rollnick, 2002). Other clinical researchers (Markland, Ryan, Tobin, & Rollnick, 2005; Ryan & Deci, 2008; Vansteenkiste & Sheldon, 2006) have observed that the MI spirit is equivalent to innate psychological needs for autonomy, competency, and relatedness.
Previous researchers have reported that MI interventions (MIIs) are effective in increasing adherence to prescribed treatment among diabetes patients (Chen, Creedy, Lin, & Wollin, 2012; Greaves et al., 2008; Kent, 2007; Ridge, Treasure, Forbes, Thomas, & Ismail, 2012; Welch, Rose, & Ernst, 2006). MIIs significantly improved self-management behaviors, quality of life, and self-efficacy in adults with T2DM (Chen et al., 2012). A one-session MII significantly increased confidence in dietary management among post-menopausal women with pre-diabetes (Kent, 2007). Greaves et al. (2008) found that 24% of participants who received a MII achieved weight loss compared with 7% in the usual care (UC) group; 38% of participants who received a MII reached the target goal for physical activity compared with 28% in the UC group. Thus, MIIs appear to improve self-management behaviors among T2DM patients.
Purpose
The purpose of this study was to determine the effect of a MII on adherence to regimens of primary importance in diabetes self-management (medication use, glucose monitoring, physical activity) and diabetes markers (glycosylated hemoglobin [HbA1C], random serum glucose, body mass index [BMI]) among African American adults with T2DM. The hypotheses were as follows:
Method
Design
A controlled trial was conducted with data collection at baseline and 3-month follow-up. Participants were recruited at the time of their clinic visits and assigned to the UC group (n = 36) or the MII group (n = 26). Initially, participants were randomly assigned to either group; however, some participants (n = 5) were unable to participate in the MII due to lack of transportation for scheduled MII sessions or childcare responsibilities (see Figure 1). A per-protocol analysis was initially performed. In addition, both an intent-to-treat analysis and analysis that did not include n = 5 were performed to examine if conclusions were sensitive to analytical techniques employed. The conclusions were not sensitive and per-protocol results are reported. The research team members informed participants which group they had been assigned at the time of baseline data collection.
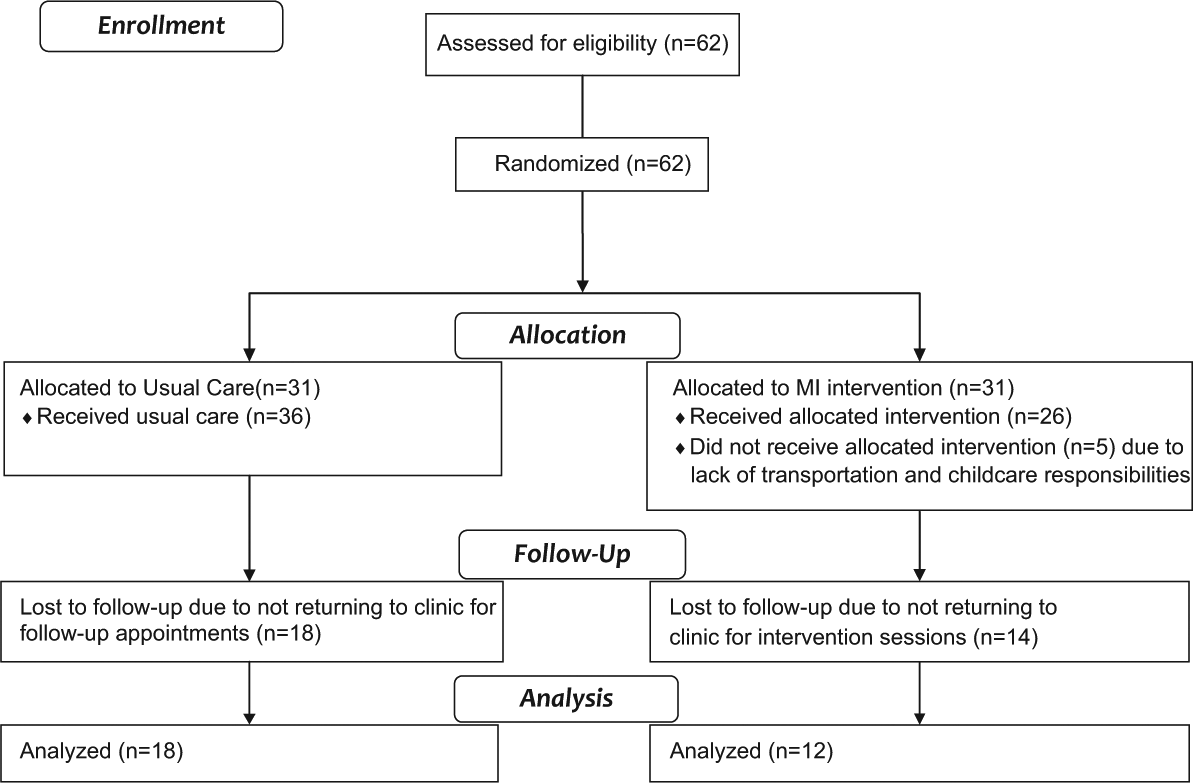
Flow diagram illustrating enrollment and retention of study participants.
Diabetes markers examined included HbA1C, random serum glucose, and BMI. As an 80% cut-off point is traditionally used in similar clinical trials to determine adherence to treatment regimens (McNabb, 1997), adherence to prescribed treatment regimens was defined as follows: (a) taking prescribed diabetes medications at least 80% of the time, (b) following recommended glucose monitoring schedule at least 80% of the time, and (c) participating in the recommended level of physical activity at least 80% of the time. The ADA (2014) recommends 150 min per week of moderate intensity aerobic physical activity over at least 3 days per week for individuals with T2DM.
A total of 62 participants were recruited. Power calculations were based on the total sample size (n = 30) that was available for complete analysis. The study had 81% power to detect a medium-to-small effect size (Cohen’s D = 0.28).
Sample and Setting
The convenience sample consisted of 62 voluntary participants receiving medical care at an outpatient internal medicine clinic in a midsized city in the southeastern United States. Every participant meeting the inclusion and not meeting the exclusion criteria was invited to participate in the study. Inclusion criteria for participation were as follows: (a) 18 years of age or older, (b) African American ethnicity, (c) diagnosis of T2DM which was treated by prescribed oral anti-hyperglycemic agents and/or insulin, and (d) English speaking. Exclusion criteria included the following: (a) inability to understand study purpose and procedures, (b) receiving current treatment from a mental health provider, and (c) inability to engage in moderate physical activity. The sample consisted of 40 women and 22 men with a mean of 53.67 years (SD = 11.2 years) with no significant difference between the genders (p = .623). Demographic and health history information is displayed in Table 1.
Demographic and Health History Characteristics Stratified by Group, at Baseline.
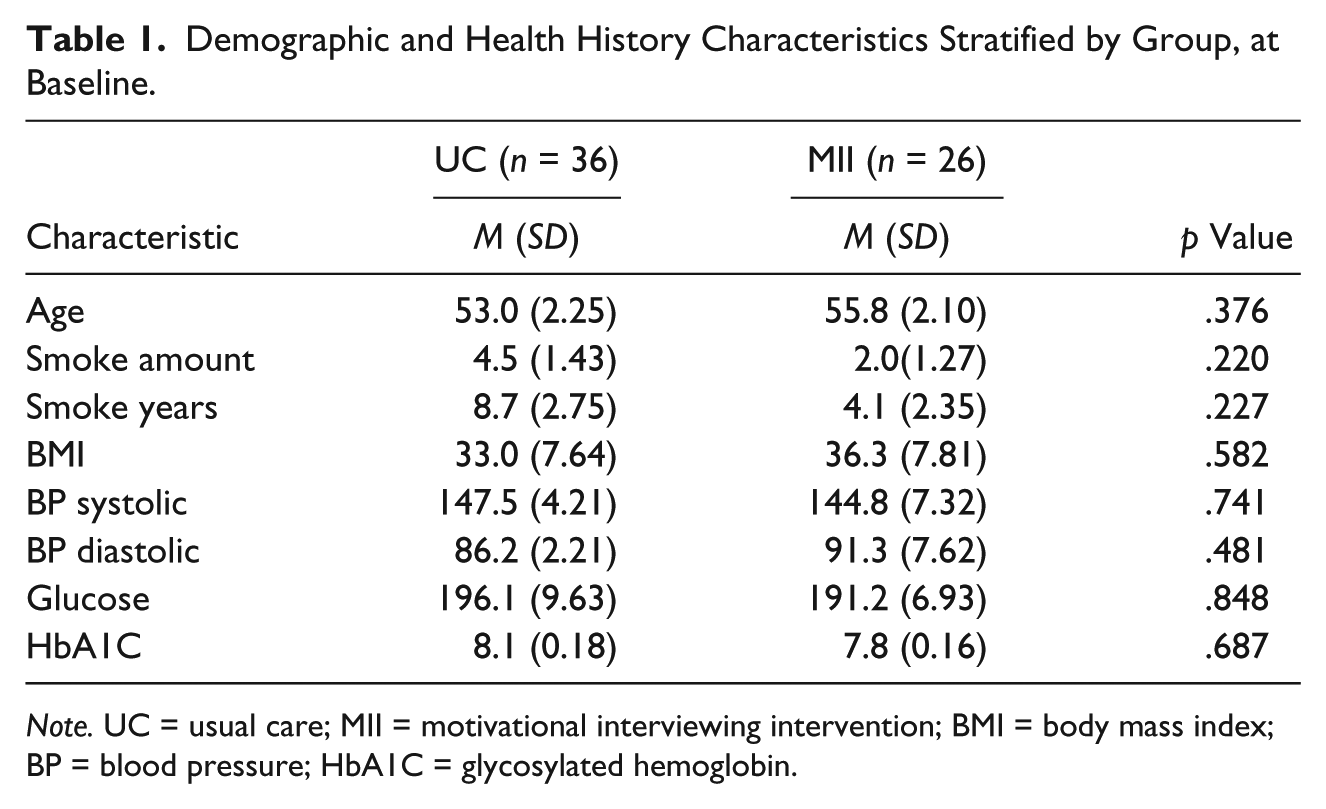
Note. UC = usual care; MII = motivational interviewing intervention; BMI = body mass index; BP = blood pressure; HbA1C = glycosylated hemoglobin.
Measures
Demographic and health history data were collected with a 10-item survey. Demographic data included gender, age, marital status, educational background, monthly income, and type of health insurance. Health history data collected at baseline included smoking amount, years of smoking, and diastolic and systolic blood pressure. Chart reviews were conducted at baseline and at 3-month follow-up to obtain random serum glucose, HbA1C, and BMI. Medication usage data were collected using self-report measures at 3-month follow-up. Data were also obtained from physical activity monitors (MiniMitter®, Respironics; Bend, OR) and blood glucose monitors (Prodigy 800®, Prodigy Diabetes Care, LLC: Charlotte, NC) at 3-month follow-up.
Procedure
After receiving approval from the Institutional Review Board at the sponsoring university, study personnel recruited potential participants at the internal medicine outpatient clinic at an academic medical center. Study personnel explained the procedures, the responsibilities of participants, and the study’s voluntary nature during face-to-face interviews. Informed consent was obtained from all participants. The study personnel read the consent form and demographic survey to study participants if they were unable to read. No health care providers at the clinic were employed as study personnel; all providers were blinded to participants’ group assignments. Participants received a US$10 gift card to a regional retailer at baseline and 3-month follow-up to compensate them for the time they devoted to participation in the study. All participants received a glucose monitor and testing strips for the duration of the study to provide them with the necessary equipment for glucose monitoring. All participants were given an accelerometer to wear for 1 week at baseline and again at 3-month follow-up to measure physical activity.
The intervention was delivered to the experimental group by a baccalaureate prepared registered nurse (RN) with experience caring for adult clients with T2DM. The RN interventionist was not an employee of the clinic where participants were recruited and the intervention took place. The RN interventionist received extensive training from a MI network trained educator prior to delivering the MII (El-Mallakh, Chlebowy, Wall, Myers, & Cloud, 2012). The MIIs addressed medication usage, glucose monitoring, and physical activity. In delivering the MII, the interventionist used the MI spirit by including strategies of building rapport, evaluating current level of adherence to each of the targeted behaviors, exploring costs and benefits of changing the behaviors, assessing the importance that participants assigned to the behavior changes, and assessing confidence in their ability to change the behaviors. Intervention participants received between 4 and 6 one-on-one MI sessions over a 3-month period; not all participants received the study protocol requirement of 6 MI sessions due to attrition. Sessions lasted between 45 min to 1 hr and occurred every 2 weeks during the 3 months. UC participants received the standard care at each clinic visit, which included a review of symptoms of diabetes and hypoglycemia, discussion of medication and glucose monitoring adherence, screening for microvascular complications, and a referral to a diabetes educator, as needed; HbA1C levels, BMI, and random serum glucose levels were obtained every 3 months.
Intervention Fidelity
Assessment of intervention fidelity is essential to determine the degree to which an interventionist adheres to study protocols in intervention delivery. In this study, fidelity assessments were conducted regularly throughout the duration of the study. All intervention sessions were audiotaped, and 25% of these were randomly selected for fidelity assessment. Three members of the research team rated fidelity to the intervention; assessments were guided by the Motivational Interviewing Treatment Integrity Scale (Moyers, Martin, Manuel, Miller, & Ernst, 2007). The fidelity assessments indicated that the intervention was delivered with satisfactory fidelity throughout the study (El-Mallakh et al., 2012). For example, fidelity scores for MI Global Spirit were 4.0 or above in 100% of the assessed interventions, and the interventionist demonstrated 100% MI adherent behaviors in 89% of the assessed interventions. More detailed procedures for conducting fidelity assessments for this study have been described elsewhere (El-Mallakh et al., 2012).
Data Analysis
Differences in demographic and health history data were tested using t tests for continuous data (Wilcoxon methods used when appropriate) and chi-square techniques for categorical data. Repeated-measures ANOVA was used to determine if group affiliation predicted each outcome, while adjusting for traditional risk factors (e.g., age and gender) and any covariates that were significantly different in the univariate analysis. Three repeated-measures ANOVA models were developed for the diabetes markers (HbA1C, random serum glucose, and BMI). Multiple logistic regression was used to evaluate the influence of group affiliation on the odds an individual was adherent to each outcome. Similarly, three logistic regression models were developed for the three adherence measures (medication usage, glucose monitoring, and physical activity).
Results
While 62 African American adults (n = 36, 58.1% in the UC group; n = 26, 41.9% in the MII group) were enrolled at baseline, only 30 participants (n = 18, 60.0% in the UC group; n = 12, 30.0% in the MII group) had data collected at 3-month follow-up (52% attrition). There were no significant differences in demographic and health history data between those who dropped out and those who completed the study. The attrition rate was similar between UC and MII participants (50.0% vs. 53.8%, p = .861). There were no significant differences in education (p = .614), insurance coverage (p = .498), or income (p = .533) between the two groups. As shown in Table 1, no significant differences existed in demographic and health history data between the UC and MII participants, indicating that the randomization scheme was successful.
Table 2 displays the mean for each diabetes marker at the two time points (baseline and 3-month follow-up) stratified by group. MI significantly decreased glucose (a decrease of 34.3 mg/dl for the MII group vs. an increase of 3.1 mg/dl for the UC group) and BMI (a decrease of 2.0 for the MII group vs. an increase of 0.5 for the UC group) over time, when compared with UC (see Table 3). Random serum glucose levels slightly increased for the UC group, but drastically decreased for the MII group (see Figure 1). The response profile for both groups was similar for HbA1C levels, and the BMI increased for the UC group, while decreasing for the MII group.
Diabetes Markers at Baseline and 3-Month Follow-Up Stratified by Group.
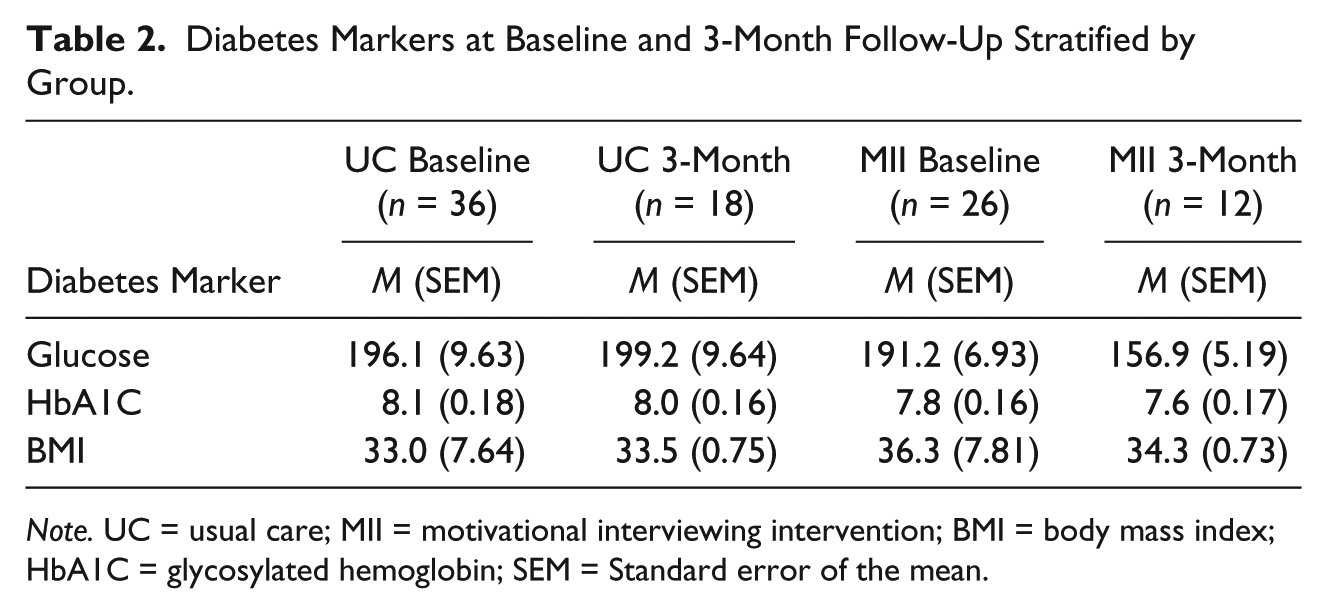
Note. UC = usual care; MII = motivational interviewing intervention; BMI = body mass index; HbA1C = glycosylated hemoglobin; SEM = Standard error of the mean.
Repeated-Measures ANOVA of Diabetes Markers Over Time Stratified by Group; Adjusting for Age and Gender.
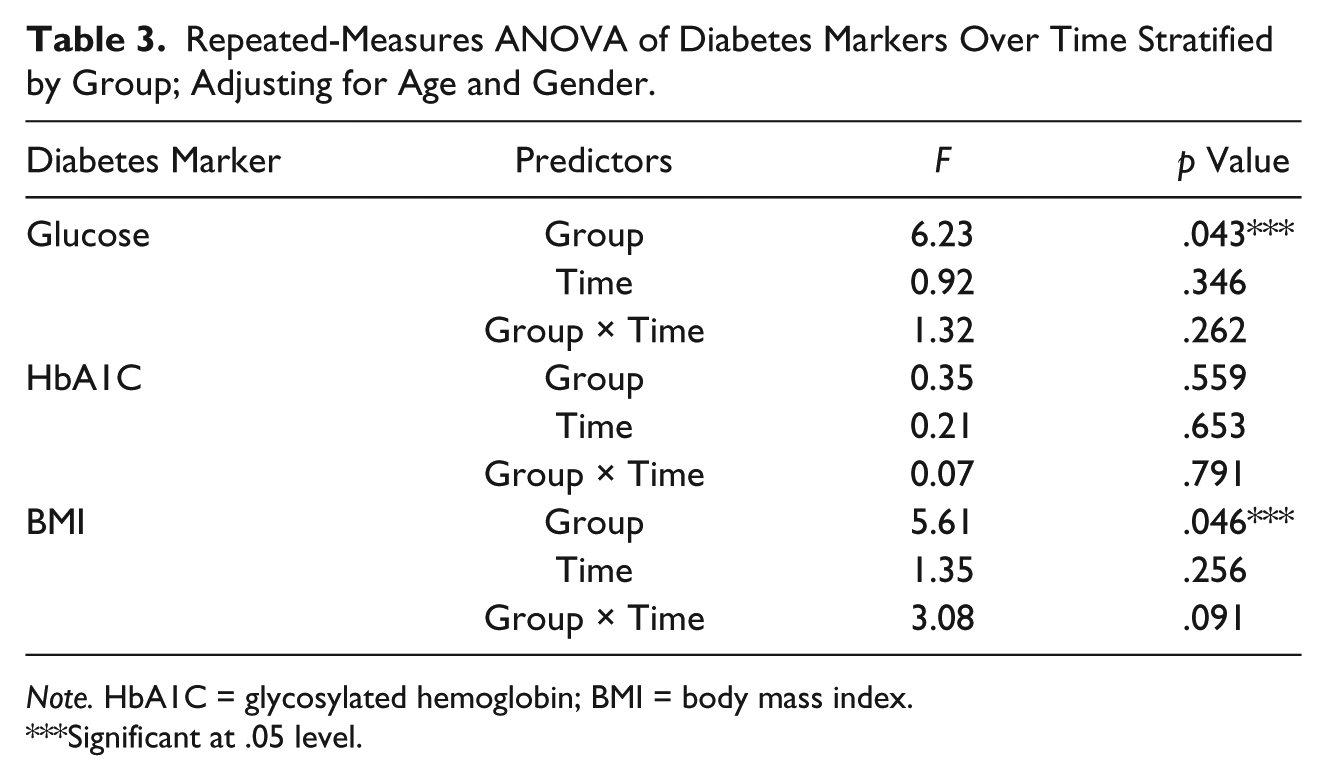
Note. HbA1C = glycosylated hemoglobin; BMI = body mass index.
Significant at .05 level.
Table 4 displays regimen adherence rates (medication usage, glucose monitoring, and physical activity) for the UC and MII participants at the 3-month follow-up along with the odds of adherence stratified by group to evaluate if the changes over time differed by group. As shown in Table 4, MI significantly increased the odds an individual adhered to their recommended physical activity level (66.7% vs. 38.8%, odds ratio [OR] = 2.92, 95% confidence interval [CI] = [1.6, 14.3], p = .018). MI had no effect on adherence to medication recommendations or glucose monitoring.
Regimen Adherence Rates Stratified by Group.
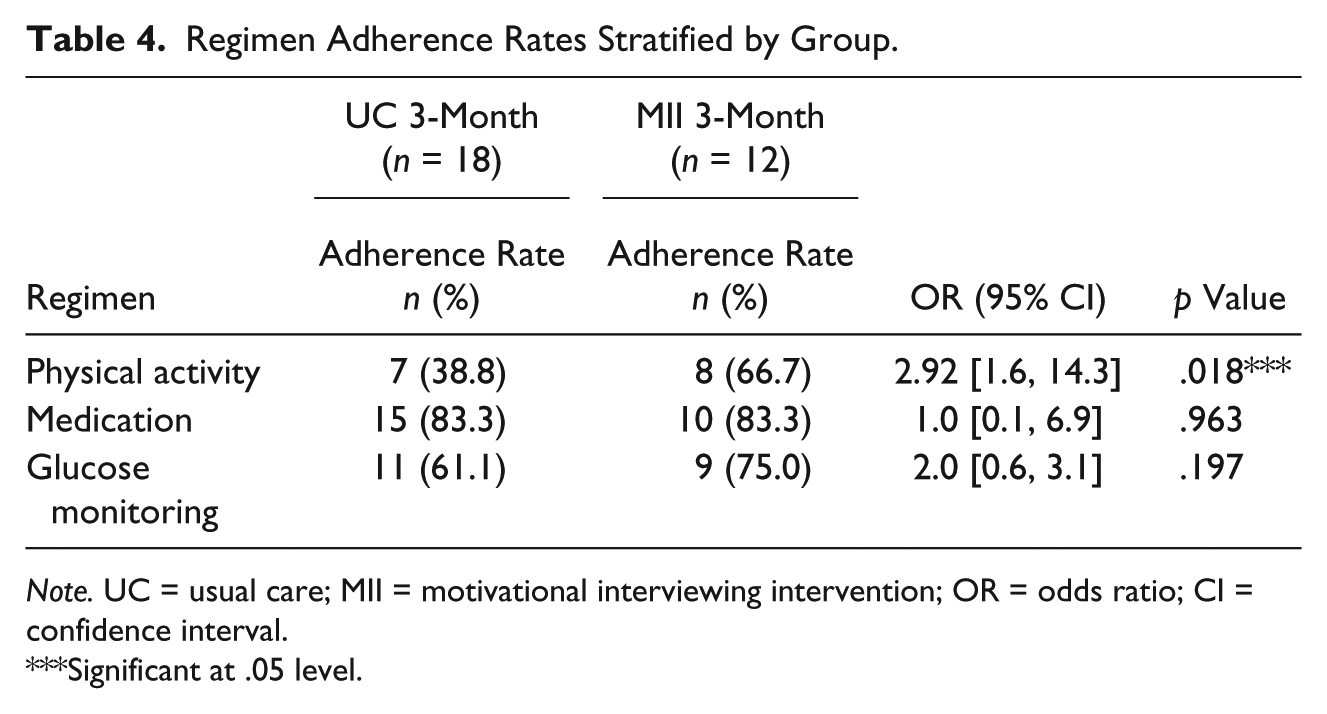
Note. UC = usual care; MII = motivational interviewing intervention; OR = odds ratio; CI = confidence interval.
Significant at .05 level.
Discussion
MII significantly increased the odds that participants improved the frequency in which they engaged in physical activity but not medication-taking and glucose monitoring. It is encouraging that participation in the MII improved frequency of physical activity. Improvement in physical activity may be attributed to the ease with which participants were able to engage in this activity. Physical activity was defined as the amount and frequency that each participant engaged in weekly physical activity. Walking is a relatively simple physical activity that can be completed without an excessive amount of cost, planning, and preparation when built into daily activities. This finding is encouraging, due to the potential benefits of physical activity on maintenance of normal glycemic control, weight loss, and perceptions of self-efficacy and well-being.
The findings that participants demonstrated decreased blood glucose levels and reduced BMI are also encouraging. These findings are consistent with previously reported research on the effectiveness of MI in improving diabetes treatment outcomes (Chen et al., 2012; Lundhall et al., 2013; West, DiLillo, Bursac, Gore, & Green, 2007). Chen and colleagues compared the effectiveness of an MII with UC on HbA1C and adherence to diabetes self-care among individuals diagnosed with T2DM. Findings indicated that participants in the MII group (n = 104) had significantly lower HbA1C levels and significantly improved adherence to diabetes self-care compared with the UC group (n = 111). West and colleagues conducted a randomized controlled trial to examine the effectiveness of a MII on weight loss among 217 women with T2DM. Participants in the MII group (n = 109) lost significantly more weight compared with those in the attention control group (n = 108). Findings indicated that Caucasian women in the MII group had significantly lower weight at 6, 12, and 18 months; however, African American women in the MII group had significantly lower weight at 6 and 12 months, but returned to baseline weight at 18 months. In addition, participants in the MII group had significantly lower HbA1C levels at 6 and 12 months compared with those in the attention control group.
In this study, MII did not increase the likelihood of adherence to glucose monitoring. Glucose monitoring provides feedback about an individual’s glucose levels and is often helpful for the health care provider in guiding some more subtle therapy choices. Participants were provided with a free glucose monitor and testing strips upon enrollment, so the cost of monitoring was not an issue; it was surprising that adherence did not improve. It is possible that participants found glucose monitoring to be a more complex self-care activity compared with physical activity. The finding that participants did not improve medication adherence is concerning as up to half of all patients diagnosed with diabetes are non-adherent with medications (Brennan et al., 2012). Medication adherence is essential to achieve normal glycemic control and avoid long-term consequences of hyperglycemia. Participants had to obtain and pay for their own medications, and cost may have presented a barrier to medication adherence. It is possible that participants found medication adherence to be more complex self-care activity compared with physical activity. Multiple factors can contribute to a patient’s ability to adhere to a medication regimen; non-adherence among those with diabetes has been attributed to health beliefs, lack of confidence that the medication will be effective, and interference with lifestyle (Bailey & Kodack, 2011).
Cost of medications is a significant barrier to medication adherence (Briesacher, Gurwitz, & Soumerai, 2007). Briesacher et al. (2007) found that low income is a strong risk factor for cost-related medication non-adherence, an observation that is particularly relevant in this study. Of the participants in the MII group, one quarter had a monthly income less than US$500, and almost 60% had an income of US$501 to US$1,000 per month (see Table 1). It is possible that rates of medication adherence did not improve among the low-income MII participants due to the inability to purchase their diabetes medications. Further research is needed to determine if MI can improve adherence when factors such as patient income, medication cost, and availability of generic medications are incorporated into a behavioral change plan.
Medication non-adherence may also occur inadvertently due to several practical issues, such as the complexity of medication regimens, changes in daily routines, medication availability when out of the house, and competing demands from work and family responsibilities. In addition, an inability to tolerate the adverse effects of medications, particularly fear of low blood sugar, presents a significant barrier to medication adherence (Chlebowy, Hood, & LaJoie, 2010). Further research is needed to determine how interventionists can effectively and proficiently address the numerous factors that contribute to medication non-adherence during a MI session.
These findings suggest that diabetes clinicians need to use an individualized approach that accommodates contextual features such as socioeconomic status and complexity of the treatment regimen when collaborating with the diabetes patient and other disciplines to develop a behavioral change plan targeted toward medication and glucose monitoring adherence. Planning is a critically important aspect of the MII (Miller & Rollnick, 2002) and a plan for behavioral change needs to be realistic, practical, and manageable for the patient. A key feature of a behavioral change plan is identification of potential barriers to change and potential solutions to overcoming barriers. When collaborating with the patient to develop a change plan, the interventionist and patient need to explicitly address issues specific to the contextual and sociodemographic barriers of medication and glucose monitoring adherence and devise specific strategies to promote success of patient in making changes.
Some study limitations are evident. A convenience sample was selected for participation in the study, which limits generalizability of the study findings to other populations. Attrition for both the MII and UC groups was about 50%, and resulted in a low number of participants included in the final data analysis. As established in previous studies, a high attrition rate can be expected in diabetes research, ranging from 2.3% to 50.0% (Heneghan et al., 2007). As the current study involved a high-risk population, it was anticipated that there would be a high attrition rate. In this study, the attrition rate was similar between the MII and UC groups; therefore, it appears that the intervention did not contribute to the high attrition rate; it was simply an artifact of the population studied. This raises questions about the acceptability of the intervention and the importance of modifying the intervention in future studies. Up to six sessions were used in this study due to the high number of diabetes self-care behaviors that were addressed in the intervention. The intervention was conducted in the clinic in which participants received their diabetes care; traveling to the clinic to receive the intervention was inconvenient for many participants due to their family responsibilities. This underscores the need for interventions that meet the needs of participants, particularly those that are delivered in innovative ways, such as via the telephone. Participants were sometimes inconsistent in wearing the physical activity monitors; therefore, data downloaded from the MiniMitter® physical activity monitors may reflect some inaccuracies. Self-report measures were used to determine medication use, which may possibly contribute to inaccurate reporting. In addition, data collection at other time points such as 6 months and 12 months follow-up would further evaluate the effectiveness of the MII over time.
The study was also conducted among low-income African American participants who were recipients of publically funded medical care. Therefore, findings may not be generalizable to other ethnic groups, those with private insurance or more affluent patients with diabetes. Regardless, the findings lend support to the growing body of evidence that MI is an effective approach to changing illness-related behaviors. The information obtained in this study can be useful in guiding further refinements to MII strategies to promote adherence to self-care of interventions for people with diabetes.
Based on the results of this study, MI appears to be a promising, evidence-based strategy for improving physical activity, but not glucose monitoring and medication adherence, among African Americans with T2DM. Further research is warranted to determine the optimal MI strategies in addressing adherence to a wide variety of self-care activities in this population and the effect of MI using a larger sample size over a longer period of time.
Footnotes
Acknowledgements
Thanks are extended to the study participants and the study personnel.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding provided by the Passport Health Plan’s Improved Health Outcomes Program.