
Abstract
Culturally tailored interventions have been applied to provide benefits to ethnic minorities’ care; however, the effectiveness of these interventions for chronic conditions is mixed. This systematic review of systematic reviews critically evaluates recent evidence of the effects that culturally tailored interventions have on health care outcomes among ethnic minorities with chronic conditions. It synthesizes results of eight English-language systematic reviews published between 2010 and 2018 and identifies four health care outcomes common to the reviews: disease knowledge, objective clinical outcomes, satisfaction, and access. Our findings suggest that culturally tailored interventions can contribute to the improvement of ethnic minorities’ health care outcomes and especially improve patients’ satisfaction with care. However, results overall are mixed. Further studies to better understand the value of culturally tailored interventions for ethnic minorities’ care are needed.
Keywords
In Europe, the United States, and Australia, the number of ethnic minorities—that is, immigrant or racial groups “regarded by those claiming to speak for the cultural majority as distinct and unassimilated” (Collins Dictionary, 2019)—is increasing rapidly (Coleman & Angosta, 2017). In 2018 in the United States, Asians, African Americans, and Hispanics represented about 37.6% of the total population (United States Census Bureau, 2018). Meanwhile, ethnic minorities’ share of the total population was 19.5% in the 2018 census of the United Kingdom (Government United Kingdom, 2018).
Ethnic minority groups living in these developed countries often experience health disparities and inequities (Darlington-Pollock & Norman, 2017; Joo, 2014). Diminished access to the health care system due to costs and language barriers expose ethnic minorities to high risk for chronic conditions (Joo, 2014). In fact, ethnic minorities have higher prevalence of chronic conditions such as diabetes and prediabetes than the majority population (Hawthorne et al., 2010; Joo, 2014). These populations therefore present new challenges to Western counties’ health care systems and health care practitioners (Joo & Liu, 2019).
To reduce health disparities and provide more equitable care, efforts have been made to provide culturally tailored care for ethnic minorities with chronic conditions (Coleman & Angosta, 2017). Cultural tailoring is synonymous with “cultural targeting” and “cultural competency,” but most researchers call it “cultural tailoring,” and it means “employing the native language, integrating cultural dietary preferences, encouraging family participation and support, and holding open discussions of cultural beliefs and treatment practices” (Choi & Rush, 2012, p. 379). Other researchers have defined it as tailoring a health message that “recognizes and reinforces a group’s cultural values, beliefs, and behaviors and built upon those to provide context and meaning to the message about a given health problem or behavior” (van der Veen et al., 2010, p. 3).
Several empirical studies have applied culturally tailored interventions in the treatment of ethnic minorities’ chronic conditions and have shown the impact of the interventions on disease knowledge and clinical outcomes. For example, Choi and Rush (2012) and Islam et al. (2013) researched culturally tailored interventions with immigrants with diabetes and found the interventions to be effective at inspiring behavioral changes. Similarly, culturally tailored interventions have been found to be effective when screening for cancer and when teaching awareness to ethnic minorities with cancer (Briant et al., 2018; Maxwell et al., 2008; Chee et al., 2017). But other studies found no significant changes on breast and cervical cancer screening outcomes with mammography use or Pap tests (Kim & Menon, 2009; Moskowitz et al., 2007). These conflicting results suggest the effectiveness of culturally tailoring interventions to ethnic minorities with chronic conditions is still largely unknown.
To establish an evidence base of the effectiveness of culturally tailored interventions with ethnic minorities on disease knowledge and access outcomes, several systematic reviews and meta-analyses have been conducted. However, these results are also mixed. For example, Fisher and colleagues (2007) found that culturally tailored interventions were effective at changing racial minorities’ health-condition disparities, such as knowledge of self-care and accessibility of health care systems. Meanwhile, Heo and Braun (2014) found that culturally tailored interventions are insufficient to entirely control chronic conditions.
This systematic review of systematic reviews is therefore needed to obtain clear evidence of intervention effectiveness (Smith et al., 2011). Specifically, it synthesizes recent research into culturally tailored interventions to obtain clear evidence of the interventions’ effectiveness on health care outcomes among ethnic minorities with chronic conditions.
Purpose
The purpose of this systematic review of reviews was to critically synthesize the findings from systematic reviews that evaluated the impacts of culturally tailored interventions used in the management of care for ethnic minorities with chronic conditions. The review question was “How effectively do culturally tailored interventions promote and impact health care outcomes for ethnic minorities with chronic conditions?”
Methods
Design
A systematic review of systematic reviews is a new review method for advanced health care research to report integrated evidence. To conduct it, we used a methodology devised by Smith et al. (2011). This methodology makes it possible to discuss current evidence-based research by summarizing, synthesizing, and comparing evidence reported by systematic reviews (Smith et al., 2011).
Reporting methods in this review adhere to the Participants, Interventions, Comparison, Outcomes (PICO) framework for systematic reviews (Robinson et al., 2011) and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement (Moher et al., 2009).
Search Strategy
To find relevant systematic reviews, five electronic bibliographic databases—CINAHL, PubMed, PsycINFO, Web of Science, and the Cochrane Database of Systematic Reviews—were used. The search strategies included Medical Subject Headings (MeSH) terms and the following keywords: (“culturally tailored” or “culturally appropriate intervention,” or “cultural competence” or “culturally targeting”) and (“systematic review” or “meta-analysis”) and (“chronic illness,” chronic disease,” or “chronic condition”) and (“ethnic minority” or “vulnerable population”). Six additional search terms were also used: “intervention,” “program,” “education,” “immigrant,” “health promotion,” or “health education.” To include only the most recent 10 years of evidence, reviews were limited to publication dates between 2010 and 2019. Searches were initially conducted in September 2019 and updated in November 2019.
Inclusion and Exclusion Criteria
The PICO (Patients, Intervention, Context, Outcome) criteria guided our inclusion criteria (Robinson et al., 2011). In this study, “Participants” refer to ethnic minorities with chronic conditions, “Interventions” refer to culturally tailored interventions targeted to the care of ethnic minorities with chronic conditions, “Comparison” refers to care as usual, which means comparison groups received interventions that were not culturally tailored, and “Outcomes” mean any health care outcomes that resulted from receiving culturally tailored interventions.
Identified systematic reviews synthesized empirical studies having the following inclusion criteria: First, reviews must have reported a systematic review or meta-analysis of empirical studies with experimental studies. This also means reviews should have been guided by the PRISMA statement criteria. Second, reviews must have evaluated the effectiveness of culturally tailored interventions on the health care outcomes of ethnic minorities with chronic or high-risk chronic conditions. This review defined ethnic minorities as individuals who are in a nondominant position and who have linguistic, religious, or ethnic characteristics distinct from the dominant populations—the same criteria established by the United Nations (2010). This study did not limit participants, by age but it did limit chronic conditions to diseases lasting one year or more and that cause death or disability, limit daily living, and require medical attention (Centers for Disease Control and Prevention, 2019). Third, reviews must have been published in English.
Reviews were excluded if they included indigenous populations as participants or if results were not relevant to health care outcomes as an impact of culturally tailored interventions.
Search Outcome
Seventy-eight publications were identified in the initial search. EndNote X9 was used to import the search results, and 33 duplicate publications were removed. Another 33 publications were excluded on the basis of a title and abstract review. Full-text review of the remaining 12 publications resulted in the further exclusion of four reviews. Either their target participants (n = 2), interventions (n = 1), or outcomes (n = 1) did not meet the inclusion criteria of this review. The eight remaining systematic reviews were selected for quality appraisal. Figure 1 presents a PRISMA flow chart of the selection process.
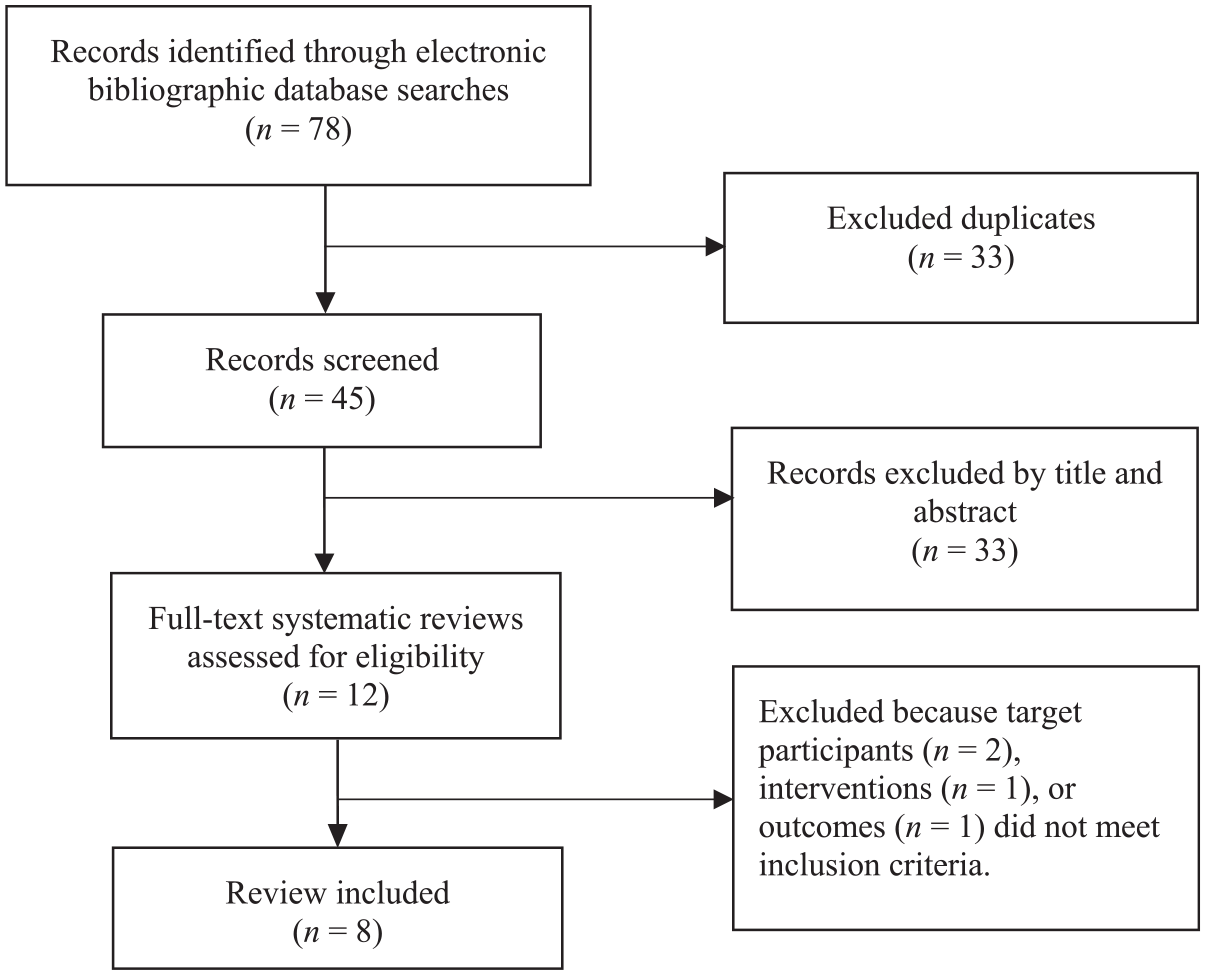
PRISMA flow diagram of the selection process.
Quality Appraisal
A Measurement Tool to Assess Systematic Reviews (AMSTAR) was used to assess the quality and risk of bias of the extracted systematic reviews (Smith et al., 2011; Shea et al., 2007). Higher AMSTAR scores means high quality of review (scores 8–11 = high-quality review; 4–7 = medium-quality review; 3–0 = low-quality review) (Smith et al., 2011; Shea et al., 2007). Each systematic review was assessed with AMSTAR by each author of this study independently; the authors then met to reach consensus on their scores.
Data Extraction
A data sheet was developed to extract relevant data from the reviews. Each author independently extracted and recorded the following data: review design, aim, methods, search strategy, study participant, types of culturally tailored interventions, country of publication, and original individual studies’ publication year. This data-extraction process was guided by the guidelines for systematic reviews of systematic reviews (Smith et al., 2011). The authors then cross-checked the data-extraction sheet.
Data Synthesis
The synthesis of data from the eight systematic reviews followed the methodology of systematic review of systematic reviews (Smith et al., 2011). Due to the heterogeneity of outcome measures from the individual reviews, statistical pooling outcomes was impossible. Instead, a narrative synthesis of the results from reviews was undertaken to identify conclusions.
Results
Description of Included Reviews
Table 1 summarizes the eight systematic reviews that met the inclusion criteria for this review (Goris et al., 2013; Hawthorne et al., 2010; Heo & Braun, 2014; Huang & Garcia, 2018; Joo, 2014; McCurley et al., 2017; Renzaho et al., 2010; Zeh et al., 2012). The reviews were conducted in Australia (n = 2), the United Kingdom (n = 2), and the United States (n = 4) and were published between 2010 and 2018. All the reviews systematically examined the effectiveness of culturally tailored interventions to control or prevent the worsening of ethnic minorities’ chronic conditions, synthesizing the effectiveness of these interventions across 150 empirical studies published between 1993 and 2015. Ninety-nine of the studies were randomized controlled trails (RCTs); the rest were experimental studies. Two of the reviews conducted a meta-analysis (Goris et al., 2013; Hawthorne et al., 2010). Four studies were included in half of the systematic reviews. Seven studies’ systematic review processes were guided by the Cochrane process or PRISMA statement; the last did not report a methodological guideline (Renzaho et al., 2010).
Characteristics of the Included Reviews.
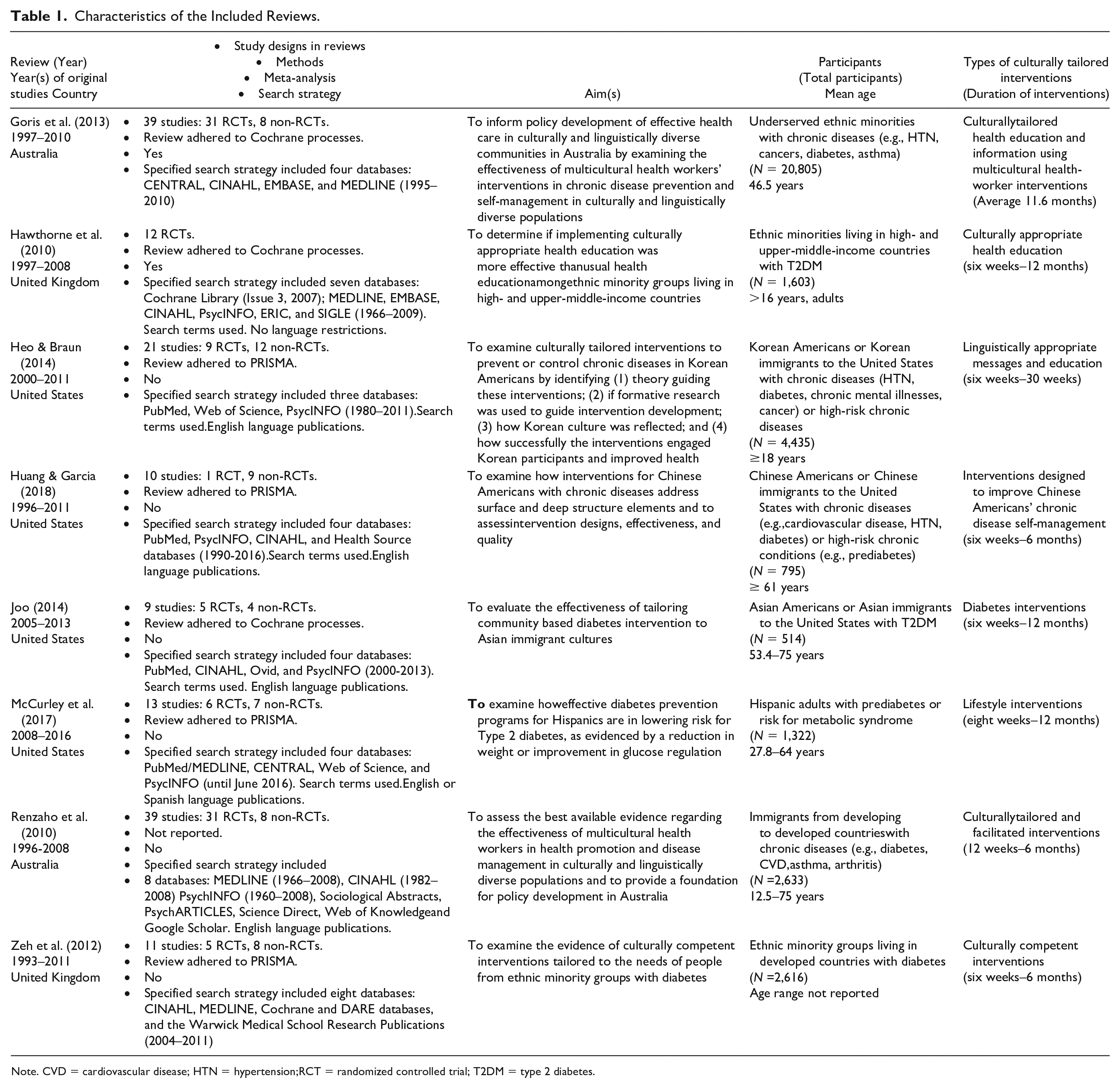
Note. CVD = cardiovascular disease; HTN = hypertension;RCT = randomized controlled trial; T2DM = type 2 diabetes.
This review of reviews did not limit the specific age groups of participants, so the ethnic minority participants ranged from 12.5 years to 75 years old. However, most participants included adults over 18 years old and elders over 65 years. Reviews included samples as small as 514 and as large as 20,805. Participants were diagnosed with at least one chronic disease (e.g., diabetes, hypertension [HTN], congestive heart failure [CHF], cancers, asthma, and arthritis) or high-risk chronic condition (e.g., prediabetes). Ethnic minorities included immigrants from developed countries and were identified as Hispanic, African American, Asians in the United States or the United Kingdom, and first- or second-generation immigrants in the Netherlands and Australia.
Methodological Quality of Included Reviews
Table 2 shows the AMSTAR scores used to assess the methodological quality of each systematic review. Seven of the reviews received scores of 8 or 9, indicating they were rated as high quality; one received a score of 7, a medium-quality rating (Renzaho et al., 2010). Five reviews were assessed to have publication bias, meaning they indicated positive results and did not guarantee the absence of negative results (Hawthorne et al., 2010; Heo & Braun, 2014; Huang & Garcia, 2018; Joo, 2014; McCurley et al., 2017).
AMSTAR Quality Appraisal of Included Systematic Reviews.
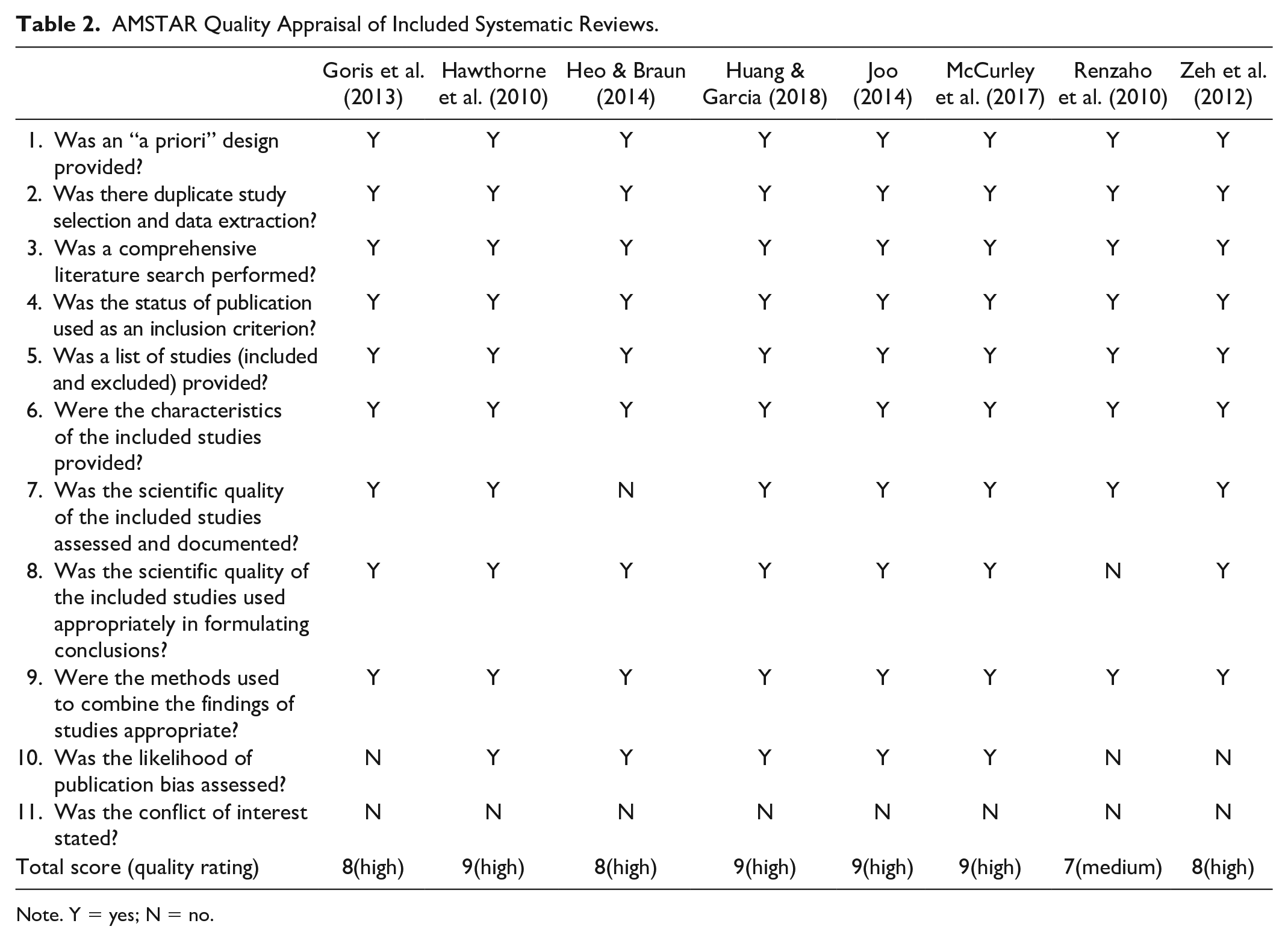
Note. Y = yes; N = no.
Methodological Quality of Included Studies
Seven reviews assessed the methodological quality with appropriate appraisal tools. These tools included the Consolidated Standards of Reporting Trials (CONSORT) statement (Goris et al., 2013), the Jadad scale, and the Cochrane Handbook criteria (Hawthorne et al., 2010); assessments of study designs, treatment allocation blinding, power analysis of sample size, dropouts, and retention rate (Huang et al., 2018); the Amsterdam Maastricht Consensus List for Quality Assessment (Joo, 2014); the Effective Public Health Practice Project Quality Assessment Tool (McCurley et al., 2017); assessments of design, adequate sample size, control group (CG) comparability, clear outcome measures, and analyses (Renzaho et al., 2010); and assessments of randomization, blinding, dropouts, follow-up rate, and recruitment sample description (Zeh et al., 2012). Heo and Braun (2014) did not appraise the methodological quality of their included studies.
Culturally Tailored Interventions
All eight reviews described how their original studies applied culturally tailored interventions to ethnic minorities to coordinate care for their chronic conditions. The studies also synthesized the interventions’ effectiveness on patients’ outcomes. Most of the culturally tailored interventions were conducted in community based settings with experienced bilingual nurses, bilingual community health care providers, or trained multicultural community health workers (Goris et al., 2013). One review reported that interventions were delivered by hired interpreters to aid communication between health care providers and ethnic minority participants (Huang & Garcia, 2018). The aims of interventions were congruent to enhance ethnic minorities’ improvement of care. The types of interventions varied, but common among them were education and counseling about disease, culturally competent health care and cultural myths, exercise and dietary advice based on culture-specific nutrition, and referrals to health services. The duration of interventions was 6 weeks to 12 months. Some reviews analyzed structure and mode of interventions from the original studies (Heo & Braun, 2014; Huang & Garcia, 2018; Zeh et al., 2012). All reviews’ CG participants received care as usual.
Health Care Outcomes
Table 3 summarizes primary health care outcomes of interest to this systematic review of reviews: disease knowledge, objective clinical outcomes, satisfaction, and access outcomes. This section synthesizes the findings from the reviews.
Summary of Common Outcomes of Included Reviews.
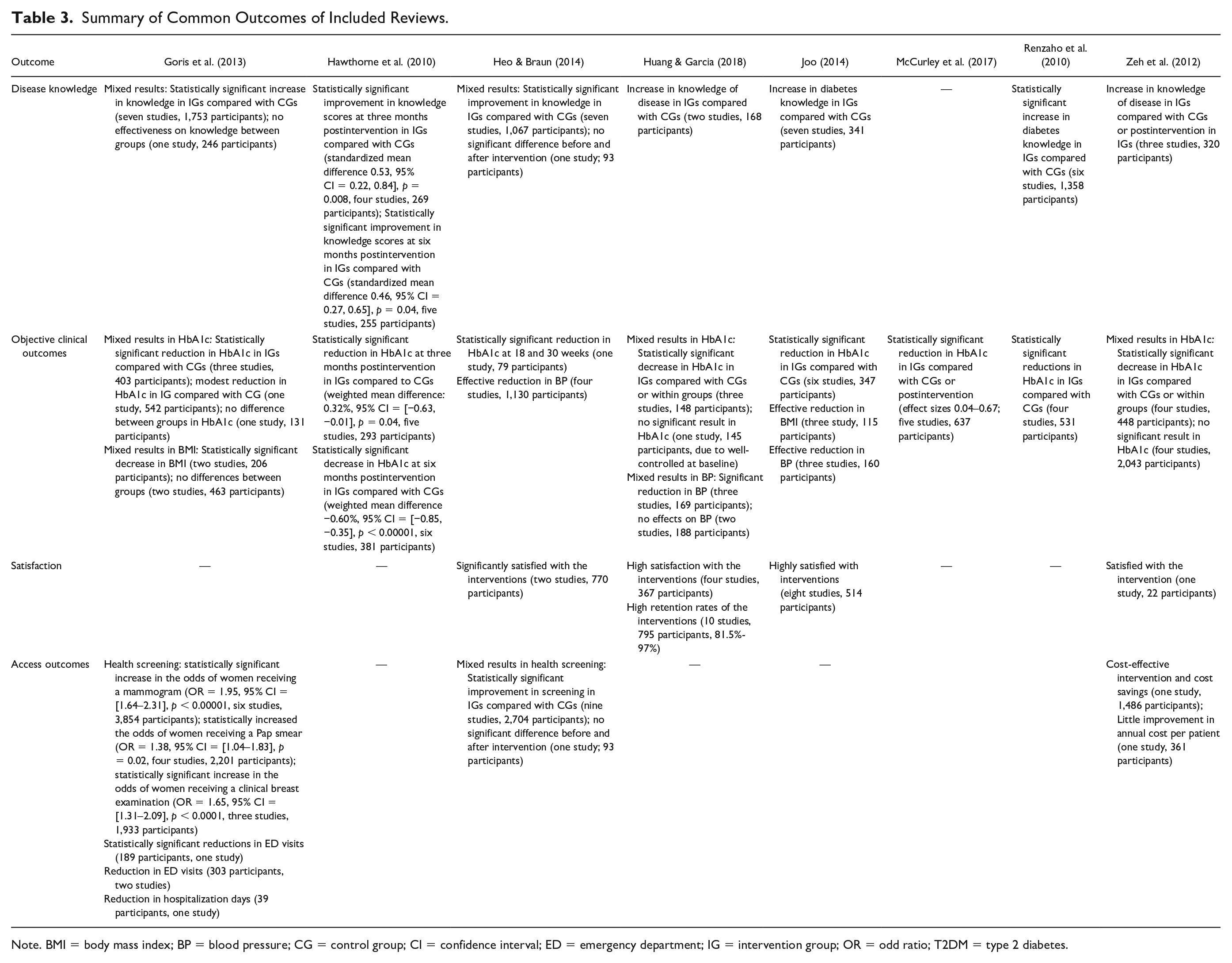
Note. BMI = body mass index; BP = blood pressure; CG = control group; CI = confidence interval; ED = emergency department; IG = intervention group; OR = odd ratio; T2DM = type 2 diabetes.
Disease knowledge
Seven reviews reported on disease knowledge as a primary outcome of culturally tailored interventions with ethnic minority participants (Goris et al., 2013; Hawthorne et al., 2010; Heo & Braun, 2014; Huang & Garcia, 2018; Joo, 2014; Renzaho et al., 2010; Zeh et al., 2012). This outcome was measured for cancers, HTN, diabetes, or prediabetes. Five of these reviews reported postintervention improvement of knowledge of disease scores in the intervention groups (IGs) compared to the CGs (Hawthorne et al., 2010; Huang and Garcia, 2018; Joo, 2014; Renzaho et al., 2010; Zeh et al., 2012). Hawthorne et al. (2010), pooling results from five RCTs (among 12 total studies), demonstrated statistically significant improvement in knowledge of disease scores when compared with CGs at six months postintervention (standardized mean difference (SMD) 0.46, 95% CI = [0.27, 0.65], p = 0.04, five studies, 255 participants). Renzaho et al. (2010) reported a significant difference in favor of diabetes knowledge (p < 0.05, six studies, 1,358 participants). Joo (2014) reported benefits for IGs in diabetes knowledge (seven studies, 341 participants). And Huang and Garcia (2018) reported increased knowledge of disease in IGs compared to CGs (two studies, 168 participants).
Two reviews reported mixed results regarding knowledge of disease (Goris et al., 2013; Heo & Braun, 2014). In Goris et al. (2013), seven studies demonstrated significant effectiveness of culturally tailored interventions on disease knowledge (1,753 participants); however, there were no differences between IGs and CGs (one study, 246 participants). Heo and Braun (2014) reported similarly mixed findings with culturally tailored interventions on knowledge of disease. Seven of the studies reported statistically significant improvement in knowledge in the IGs compared with the CGs (1,067 participants), but one study found no significant difference between pre- and postintervention knowledge (93 participants).
Objective clinical outcomes
The reviews investigated objective clinical outcomes such as HbA1c, blood pressure (BP), and body mass index (BMI). All eight systematic reviews used HbA1c as an objective clinical outcome in type 2 diabetes or prediabetes care among ethnic minorities when comparing IGs and CGs. Five reviews demonstrated culturally tailored interventions were effective in reducing HbA1c levels (Hawthorne et al., 2010; Heo & Braun, 2014; Joo, 2014; McCurley et al., 2017; Renzaho et al., 2010). Hawthorne et al. (2010), pooling results from six studies, demonstrated that HbA1c was significantly decreased at six months of intervention for ethnic minorities with diabetes and prediabetes (weighted mean difference −0.60%, 95% CI = [−0.85, −0.35], p < 0.00001, 381 participants). McCurley et al. (2017) found a statistically significant reduction in HbA1c with pooled results from five studies (standardized effect sizes 0.04–0.6; 637 participants).
However, three studies reported mixed results with respect to interventions’ effects on HbA1c levels (Goris et al., 2013; Huang & Garcia, 2018; Zeh et al., 2102). Goris et al. (2013) demonstrated statistically significant reductions in HbA1c with IGs over CGs (three studies, 403 participants), modest but not significant reductions (one study, 542 participants), and no differences between groups at all (one study, 131 participants). In Zeh et al. (2012), four studies reported that culturally tailored interventions effectively reduced HbA1c (448 participants), but four studies reported no differences (2,043 participants). Finally, Huang and Garcia (2018) reported no significant differences between groups (one study, 145 participants); however, the reason for this result was due to the fact HbA1c was well controlled at baseline.
Three reviews reported the impact of culturally tailored interventions on BP (Heo & Braun, 2014; Huang & Garcia, 2018; Joo, 2014). In Heo and Braun (2014), four studies evaluated systolic and diastolic BP changes before and after intervention with ethnic minority participants diagnosed with HTN, and all reported a reduction in BP between groups (1,130 participants). In Joo (2014), BP was reduced after intervention, but not all study results were statistically significant at p < 0.05 (three studies, 160 participants). Finally, there was no conclusion regarding BP in Huang and Garcia (2018), where BP was reduced in the IGs (three studies, 169 participants), but no effect was reported in two studies (188 participants).
BMI outcomes were measured in Goris et al. (2013) and Joo (2014). Goris et al. (2013) reported mixed results: BMI was statistically decreased in the IGs (two studies, 206 participants); however, no difference was reported in two studies (463 participants). In Joo (2014), three studies reported culturally tailored interventions were effective at lowering BMI (115 participants), but only one study showed a statistically significant difference (41 participants).
Satisfaction
In the reviews, satisfaction was a measure of the feasibility of culturally tailored interventions. Four reviews identified satisfaction with care as a result of culturally tailored interventions (Heo & Braun, 2014; Huang & Garcia, 2018; Joo, 2014; Zeh et al., 2012). All four reviews reported that ethnic minority patients with chronic conditions who were subject to the interventions were satisfied. In Heo and Braun (2014), IGs were significantly satisfied with the interventions (two studies, 770 participants). Joo (2014) reported that IGs were highly satisfied with the interventions (eight studies, 514 participants). Similarly, Zeh et al. (2012) reported satisfaction with an intervention (one study, 22 participants). And Huang and Garcia (2018), pooling results of four studies, demonstrated high satisfaction with interventions (367 participants) and reported that the IGs showed high retention rates of 81.5%–97% across 10 studies (795 participants).
Access outcomes
Three reviews reported access outcomes (Goris et al., 2013; Heo & Braun, 2014; Zeh et al., 2012). In the reviews, access outcomes were measures of health screening, hospital utilizations, or health care costs.
Two reviews reported on health screening and health examination (Goris et al., 2013; Heo & Braun, 2014). Goris et al. (2013), pooling results from six studies, reported statistically increased odds of women receiving a mammogram (odds ratio [OR] = 1.95, 95% CI = [1.64–2.31], p < 0.00001, 3,854 participants). Goris et al. also demonstrated that culturally tailored interventions showed statistically significant increased odds of women receiving a clinical breast examination (OR = 1.65, 95% CI = [1.31–2.09], p < 0.0001, three studies, 1,933 participants). However, Heo and Braun (2014) reported mixed results in health screening. Six studies showed statistically significant improvement in cancer screening such as breast, cervical, or colorectal (1,433 participants), but studies showed no successful health screening results (1,564 participants).
Otherwise, access outcomes were measured by hospital utilization and health care costs (Goris et al., 2013; Zeh et al., 2012). Goris et al. (2013) reported a large reduction in emergency department (ED) visits in culturally tailored intervention IGs compared with CGs (four studies, 492 participants). One study even showed statistically significant reduction in ED visits (one study, 189 participants), and another demonstrated the interventions were effective at reducing days in hospital (one study, 39 participants). Zeh et al. (2012) found that culturally tailored interventions were cost-effective (one study, 1,486 participants), meaning that the intervention reduced health care costs. However, the review also revealed that there was little improvement in annual cost per participant (one study, 361 participants).
Discussion
This study is the first systematic review of systematic reviews to synthesize the effectiveness of culturally tailored interventions for ethnic minorities with chronic conditions. A narrative synthesis of eight systematic reviews encompassing 150 empirical studies, this review found that the use of culturally tailored interventions was associated with increased disease knowledge (Hawthorne et al., 2010; Huang & Garcia, 2018; Joo, 2014; Renzaho et al., 2010; Zeh et al., 2012), improved objective clinical outcomes (Hawthorne et al., 2010; Heo & Braun, 2014; Joo, 2014; McCurlet et al., 2017; Renzaho et al., 2010), increased satisfaction (Heo & Braun, 2014; Huang & Garcia, 2018; Joo, 2014; Zeh et al., 2012), and improved access outcomes (Goris et al., 2013).
In the included studies, dosage and duration of culturally tailored interventions ranged widely. Common types of interventions included health education, linguistically appropriate messaging, counseling about cultural myths, exercise and dietary advice, provision of social supports, and referral services to other health care services. However, the eight reviews lacked standardized reporting methods. Moreover, the descriptions of how interventions were delivered was often vague. Among eight reviews, two tried to evaluate culturally tailored interventions’ structures to analyze which intervention elements affected participants (Heo & Braun, 2014; Huang & Garcia, 2018). However, the evidence of how interventions actually affected patients’ health care outcomes was limited. In addition, all of the studies lacked descriptions of how usual care was applied to CGs. Usual care could have elements that promote health care outcomes that could confound the outcome measures of culturally tailored interventions. For evidence-based culturally tailored intervention research and practices, further systematic reviews and empirical studies need to identify dosage of culturally tailored interventions and to connect that dosage to health care outcomes. Moreover, what constitutes usual care needs to be fully described in future empirical intervention studies and reviews (Egan & Mainous, 2012).
Due to heterogeneity of outcomes and of disorders, only two reviews conducted a meta-analysis. In Joo (2014), the included individual studies investigated knowledge of diabetes; however, because outcome measures were heterogeneous, results could not be pooled. Similar results were obtained in satisfaction with care. For evidence-based research of culturally tailored interventions, it is imperative to develop a valid and reliable instrument that can measure the true effectiveness of the intervention (Burns & Grove, 2012).
Seven of the included systematic reviews had high quality-of-appraisal scores. One review was rated as medium quality because it did not report the review methodology (Renzaho et al., 2010). No reviews reported a review protocol. To reduce opportunity of potential bias, it is recommended that future systematic reviews submit International Prospective Register of Systematic Reviews (PROSPERO) registration information, including registration numbers (Centre for Reviews and Dissemination, 2019).
To strengthen culturally tailored interventions as an effective health care management for ethnic minorities’ chronic care, it is essential to analyze cost effectiveness so health care researchers, providers, or policymakers can make informed decisions. Only three of the included reviews reported access outcomes. Among these, two reported hospital utilization outcomes (e.g., number of hospitalizations or ED visits) with cost-effectiveness analysis from individual studies (Goris et al., 2013; Zeh et al., 2012). Future systematic reviews and individual intervention studies should identify more details about health care utilization outcomes and health care cost analysis. Such analyses may help health care providers and policymakers better accept culturally tailored interventions as primary care interventions for ethnic minorities.
This systematic review of systematic reviews has some limitations. First, the majority of the included reviews were conducted in only a few developed countries. In addition, participants were weighted toward Hispanics or Asian Americans with diabetes. Both of these limitations could result in unintentional reporting bias, so this review’s results may be hard to generalize to all ethnic minorities. Second, this review of reviews only included studies published in English between 2010 and 2018. Third, culturally tailored interventions could have more beneficial outcomes, such as retention rates, self-efficacy, or quality of life, than the four this review found. Last, this systematic review of systematic reviews may tend to report positive aspects from retrieved reviews to the exclusion of negative aspects.
This systematic review of systematic reviews synthesized the effectiveness of culturally tailored interventions in the care of ethnic minorities’ chronic conditions, finding that cultural tailoring has the potential to reduce worsening chronic conditions and to increase satisfaction of care. However, further rigorously designed empirical studies and systematic reviews are required to facilitate how culturally tailored interventions improve health care outcomes and to identify the essential elements of interventions. Health policymakers, researchers, and health care providers need to understand the complex nature of health care practices that benefit ethnic minorities with chronic conditions and should pay attention to culturally tailored strategies to promote ethnic minorities’ care coordination.
Footnotes
Acknowledgements
The authors wish to thank to Gachon University for supporting this research.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.