
Abstract
Aim:
The aim was to investigate factors influencing obesity among stroke survivors based on demographics and lifestyle behaviors.
Background:
Stroke survivors are more likely to experience stroke recurrence within a few years. As obesity is a traditional risk factor for stroke, obesity should be managed in stroke survivors to prevent stroke recurrence.
Methods:
A cross-sectional secondary data analysis analyzed data from the 2017 United States Behavioral Risk Factor Surveillance System (BRFSS) survey. Demographics, frequency of vegetable and fruit intake, smoking, alcohol use, physical activity, and sleep were examined.
Results:
Among 1032 stroke survivors, 57.8% were obese. Advanced age, female sex, veteran status, at least once-daily fruit intake, current smoking, and lack of physical activity were associated with obesity.
Conclusion:
Stroke survivors should be encouraged to pursue healthy behaviors to manage obesity. Appropriate transitional care, including diet education and tailored exercise, can be an effective strategy.
Stroke refers to acute and focal neurological deficits resulting from vascular injuries, such as blockage or rupture. 1 Advanced medical care contributes to decreased stroke mortality, but stroke remains a major cause of death worldwide. According to 2022 stroke statistics, 6.5 million people die globally every year due to stroke. Approximately 63% of strokes occur among individuals younger than 70 years, and 101 million people are currently living with stroke worldwide. 2 Once stroke occurs, stroke survivors inevitably suffer from complications, including functional impairments, sensory deficits, hormone dysregulation, and depression; even worse, stroke survivors may become bed-ridden.3-5 Because of these complications, stroke survivors are more likely to experience drug-induced drowsiness, decreased physical activity, fatigue, and a sedentary lifestyle.5,6
After an initial stroke, stroke survivors can have a stroke again. Recurrent strokes occur in 22.5% of stroke survivors within 5 years of the first stroke. 7 According to a study that examined rates of recurrent stroke from 1995 to 2015 in the United Kingdom, the rate of stroke recurrence at 5 years decreased over time from 18% to 12%; since 2005, the rate of stroke recurrence has remained at 12%. 8 These findings demonstrated that stroke recurrence is still a critical issue among stroke survivors, and risk factors should be more actively managed to prevent secondary stroke. The American Heart Association and American Stroke Association (AHA/ASA) recently announced updated guidelines to prevent secondary stroke. 9 The guidelines emphasize the importance of healthy behaviors, recommending healthy eating behavior, sufficient exercise, quality sleep, avoiding binge drinking, and smoking cessation. 9
Among various stroke risk factors, obesity can be prevented by pursuing healthy behaviors such as healthy diet, sufficient physical activity, and high-quality sleep. 4 Stroke survivors are likely to be obese because of restricted physical function, antiepileptic drug and antidepressant use, and altered sleep patterns.10,11 According to previous studies, there were numerous conceptual frameworks that explained obesity mechanisms and risk factors.12,13 The mechanisms of obesity may vary depending on population characteristics. However, there were several risk factors that were similarly mentioned in many previous studies: demographic factors (eg, genetic and socioeconomic factors), social factors (eg, family influences, peer influences), lifestyle behaviors (eg, food consumption, physical activity, sleep), and environmental factors (eg, community characteristics, state policies). In this study, variables were selected based on a literature review including the conceptual frameworks of previous studies.
Among the potential risk factors, obesity, sleep (lifestyle behaviors), and veteran status (demographic factor) can be significant for stroke survivors. After a stroke, 30% to 64% of stroke survivors experience hypersomnia, excessive daytime sleepiness, insomnia, and sleep-disordered breathing; these issues increase the risk of obesity by affecting metabolic functions.6,14 Regarding veteran status, it has been known that veterans have a high incidence of stroke as well as obesity. According to a large cohort study analyzing data from 57 000 Scottish veterans and 173 000 Scottish non-veterans, veterans had a 1.21 times higher rate of stroke than non-veterans. 15 The literature also shows that the risk of obesity was significantly higher in veterans than non-veterans. 16 Trauma and extremely short mealtimes during military service have been reported as obesity risk factors among veterans.17,18
According to our search, the effects of obesity on stroke occurrence are well documented in various fields. However, risk factors for obesity among stroke survivors have not been fully investigated. To prevent stroke recurrence, obesity and its risk factors should be managed. Given the reviewed literature, we explored the relationship between demographic characteristics, lifestyle behaviors, and obesity in stroke survivors.
Aims
The aim of this study was to explore factors influencing obesity among stroke survivors. Specifically, we explored whether demographics, diet, smoking, alcohol consumption, physical activity, and sleep were associated with the risk of obesity.
Methods
Design
This study was a secondary analysis of data from the 2017 Behavioral Risk Factor Surveillance System (BRFSS) survey. The BRFSS is a yearly state surveillance system that collects health-related data, including health risk behaviors, chronic diseases conditions, and availability of health care services. 19 The survey items included in the BRFSS differ from state to state and by year of investigation. Although the 2021 BRFSS data were available, we used the 2017 data to include variables of interest. Sleep was one of our variables of interest, and it was investigated only in 2017.
Study Population
Participants were eligible to participate in the BRFSS survey if they were (a) non-institutionalized adults (≥18 years old); (b) currently living in the United States, including the District of Columbia, Guam, and Puerto Rico; and (c) living in private or college housing with access to a telephone. In the 2017 BRFSS survey, the initial number of participants was 450 016.
Of the 450 016 participants, we only included participants who were aged ≥40 years, had experienced their first stroke, and had their sleep data measured (sleep data were measured only in 7 states). As the incidence of stroke increases in middle age, we applied the ≥40 years age criterion. 4 A total of 1853 participants met the criteria. After removing extreme outliers, we classified participants according to their body mass index (BMI). As we wanted to compare healthy weight (BMI 18.5-<25 kg/m2) and obese participants (BMI ≥30 kg/m2), participants who were underweight and overweight were excluded. Therefore, a total of 1032 participants were included in this analysis (see Figure 1).
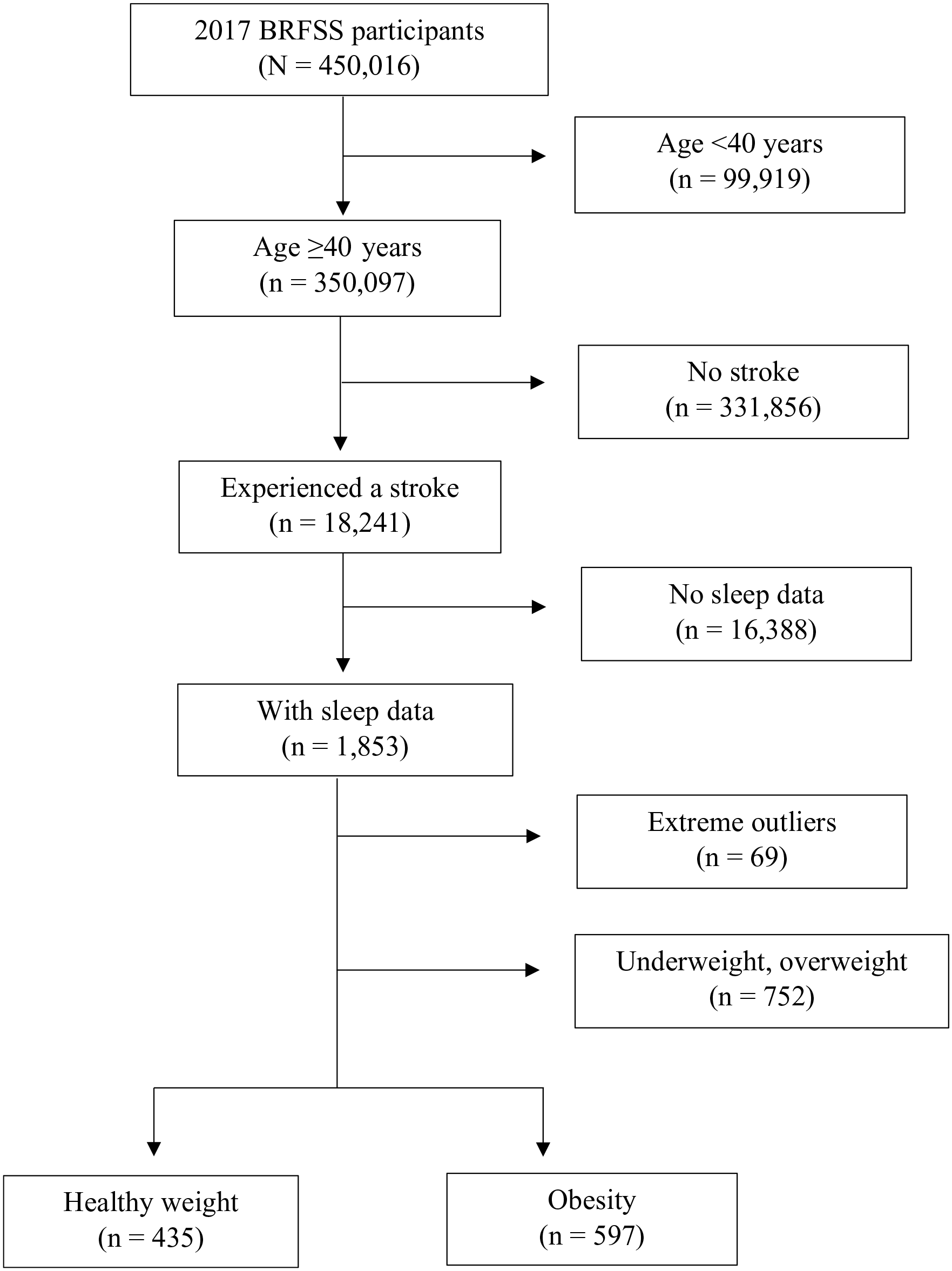
Flow diagram of the study participant selection process.
Data Collection
The BRFSS used a random-digit dialing telephone survey to collect data from potential participants. 19 During the interview, a standardized questionnaire was used. The questionnaire consisted of the core component (questions about current health and behaviors), optional modules (questions on specific topics), and state-added questions (questions developed by individual states). The core component questions were used for all states; the use of the optional modules and state-added questions were determined according to the state’s needs. The phone survey usually lasted 18 minutes, with 5 to 10 minutes of variance. 19
Measures
Demographic characteristics
Data on demographic characteristics (age, sex, race, marital status, income, and veteran status) were retrieved from the BRFSS data set. The number of comorbidities (hypertension, hyperlipidemia, asthma, depressive disorders, kidney diseases, and diabetes mellitus) was measured by the following items: (a) Are you currently taking antihypertensives? (b) Are you currently taking cholesterol medications? (c) Do you have asthma now? (d) Have you ever been diagnosed with depressive disorders? (e) Have you ever been diagnosed with kidney diseases? (f) Have you ever been diagnosed with diabetes mellitus? To the questions, participants responded yes, no, or do not know. The presence of a comorbidity was not separately measured because the number of respondents was too small.
Lifestyle behaviors
Eating behaviors were evaluated by asking about the daily consumption of vegetables and fruits. 19 Based on the participants’ responses, daily consumption was divided into less than once daily and at least once daily. Smoking status was evaluated by asking whether participants were current smokers; the possible responses were yes, no, or do not know. The use of alcohol was evaluated by asking whether participants were heavy drinkers. If male and female participants consumed >14 and >7 drinks per week, respectively, they were classified as heavy drinkers. Physical activity was measured by asking participants how much they exercised. If participants performed aerobic exercise ≥150 minutes per week, they were considered to meet aerobic exercise guidelines. If participants performed strength exercises twice per week, we considered them to meet the strength exercise guidelines. To evaluate sleep characteristics, we used sleep duration and the number of difficult sleep days. Sleep duration was measured by the total sleep hours that participants had in a 24-hour period. The number of difficult sleep days was measured by recalling the previous 2 weeks.
Obesity
The degree of obesity was classified by BMI, which is a simple index for estimating body fat mass. Body mass index is calculated as weight (kg) divided by the square of height (m2). According to the World Health Organization, 20 BMI is classified into 4 categories: (a) a BMI <18.5 indicates underweight, (b) a BMI 18.5 to <25 indicates a healthy weight, (c) a BMI 25 to <30 indicates overweight, and (d) a BMI ≥30 indicates obesity.
Ethical Considerations
The BRFSS survey data are publicly available. Therefore, this study was exempt from a review by the Institutional Review Board.
Data Analysis
Data analyses were conducted using IBM SPSS version 28 (IBM Corp, Armonk, New York), and statistical significance was set at p < .05. As we planned to conduct a logistic regression, the assumptions for logistic regression were checked. We eliminated extreme outliers, and the ratio of missing values was checked. The sample size was large enough to conduct a logistic regression, and multicollinearity among variables was not observed. 21
In this study, descriptive statistics were used to analyze the variables’ means, standard deviations, frequencies, and percentages. Independent t-tests were used to compare whether groups of continuous variables significantly differed. To explore the univariate relationship between lifestyle behaviors and obesity, univariate logistic regression analysis was conducted; the number of comorbidities was not included in the analysis due to a missing value rate of 94%. To predict how multiple variables affected obesity, we performed multiple logistic regression analysis with selected variables. The selected variables included those found to be significant in the univariate analysis and in the literature.
Results
General Characteristics of Stroke Survivors
Table 1 presents the general characteristics of stroke survivors (n = 1032). Among them, 42.2% had a healthy weight (BMI 18.5-<25 kg/m2), and the rest were obese (BMI ≥30 kg/m2). Compared to the obese group, the healthy weight group had a higher mean age (71.25 vs 65.89, p < .001) and more frequent vegetable (1.92 vs 1.72, p = .005) and fruit intake (1.50 vs 1.24, p = .001). The average number of comorbidities and number of difficult sleep days were significantly higher in the obese group (comorbidities 3.94 vs 3.30, p = .015; difficult sleep days 4.59 vs 3.70, p = .011) than in the healthy weight group. There was no significant difference in mean (standard deviation [SD]) sleep hours between the healthy weight (7.25 [1.60]) and obese groups (7.13 [1.70], p = .248).
Comparison of Characteristics Between Healthy Weight and Obese Stroke Patients (N = 1032).
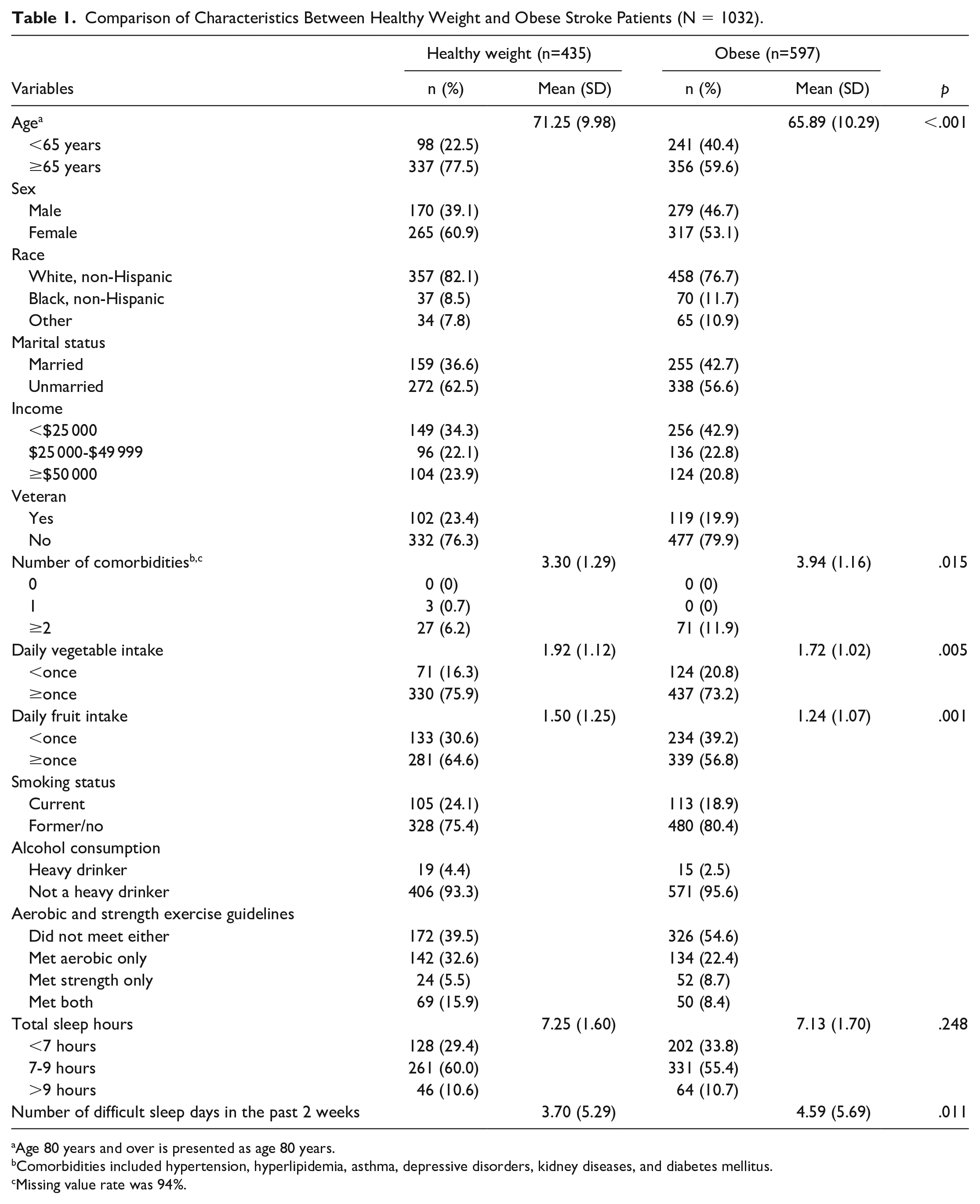
Age 80 years and over is presented as age 80 years.
Comorbidities included hypertension, hyperlipidemia, asthma, depressive disorders, kidney diseases, and diabetes mellitus.
Missing value rate was 94%.
In the healthy weight group, most stroke survivors were aged ≥65 years, female, white (non-Hispanic), and unmarried. Approximately 34.3% had a low income of less than $25 000, and 23.4% were veterans. Most stroke survivors seemed to have healthy behaviors; most of them consumed vegetables and fruits at least once a day, were not current smokers, and did not drink heavily. Approximately 60.5% performed at least aerobic or strength exercises, and 60% had an adequate amount of sleep (7-9 hours). The demographics of the obese group were similar to those of the healthy weight group. However, the proportions of people with low incomes, those who did not exercise, and those with sleep deprivation (<7 hours) were slightly higher in the obese group than in the healthy weight group.
The Association Between Lifestyle Behaviors and Obesity
Table 2 presents the results of the logistic regression analysis. In the univariate analysis, age ≥65 years (odds ratio [OR] = 2.328, 95% confidence interval [CI] = 1.763-3.074, p < .001), female sex (male OR = 0.729, 95% CI = 0.567-0.937, p = .014), unmarried status (married OR = 0.775, 95% CI = 0.601-0.999, p = .049), and low income (OR = 1.441, 95% CI = 1.036-2.004, p = .030) were significantly associated with obesity. Regarding lifestyle behaviors, fruit consumption ≥once a day (OR = 1.458, 95% CI = 1.119-1.901, p = .005), current smoking (OR = 1.360, 95% CI = 1.007-1.836, p = .045), insufficient exercise (strength exercise only OR = 2.990, 95% CI = 1.632-5.477, p < .001; neither type of exercise OR = 2.616, 95% CI = 1.739-3.934, p < .001), and difficulty sleeping (OR = 1.030, 95% CI = 1.007-1.054, p = .012) were significantly related to obesity.
Univariate and Multivariate Associations of General Characteristics and Lifestyle Behaviors With Obesity (N = 1032).
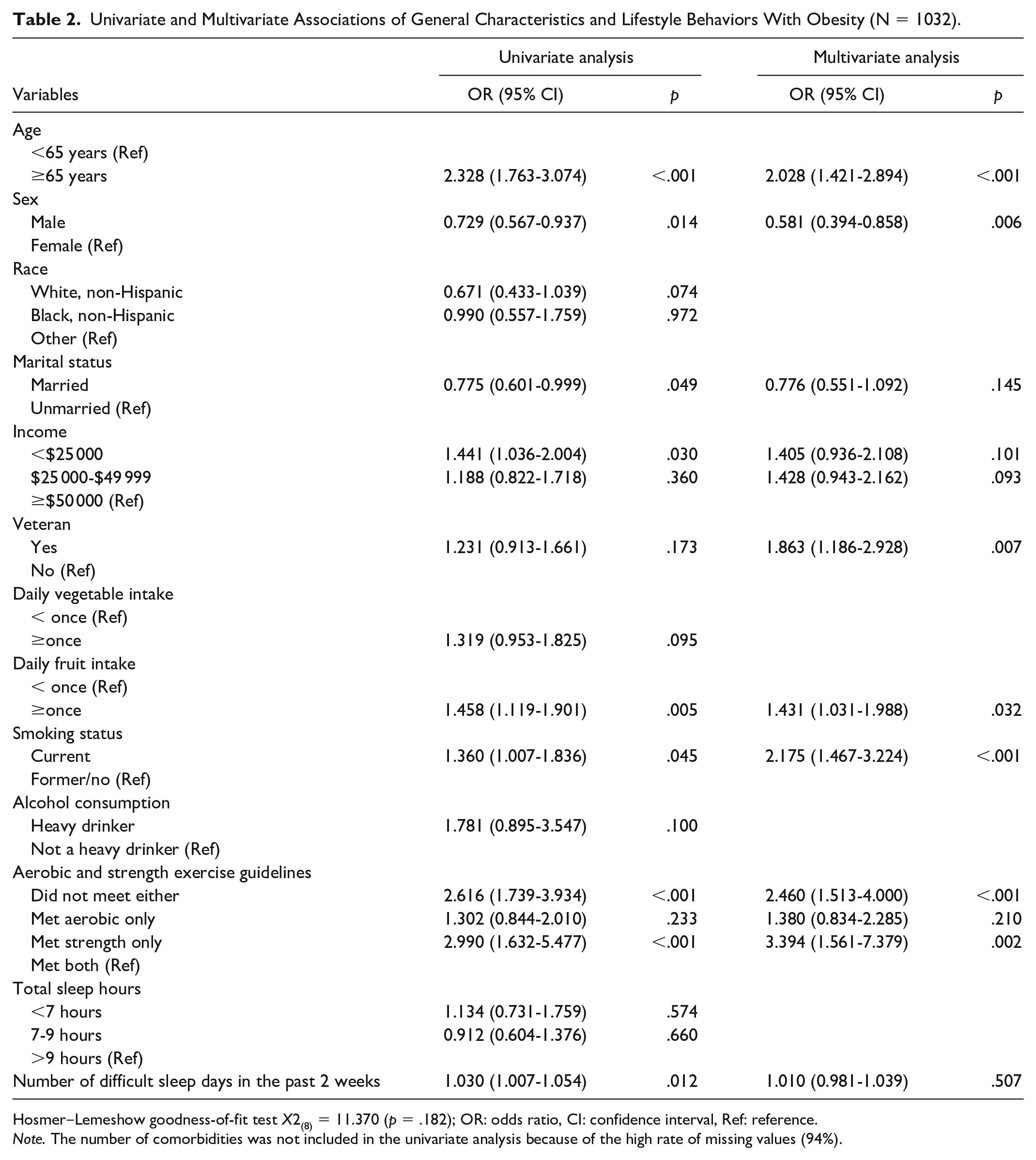
Hosmer‒Lemeshow goodness-of-fit test X2(8) = 11.370 (p = .182); OR: odds ratio, CI: confidence interval, Ref: reference.
Note. The number of comorbidities was not included in the univariate analysis because of the high rate of missing values (94%).
The results of the multivariate analysis are also presented in Table 2 and Figure 2. In the multivariate analysis, variables that were significant in the univariate analysis were included. Veteran status was not a significant variable in the univariate analysis, but it was considered in the multivariate analysis based on a literature review. Overall, the proposed model performed better than the intercept model. The result of the Hosmer‒Lemeshow test showed that the proposed model fit the data well (X2(8) = 11.370, p = .182). When multiple variables were considered, the risk of obesity increased if stroke survivors were aged ≥65 years (OR = 2.028, 95% CI = 1.421-2.894, p < .001), female (male OR = 0.581, 95% CI = 0.394-0.858, p = .006), and veterans (OR = 1.863, 95% CI = 1.186-2.928, p = .007). The risk of obesity was positively associated with a ≥once-daily fruit intake (OR = 1.431, 95% CI = 1.031-1.988, p = .032), current smoking (OR = 2.175, 95% CI = 1.467-3.224, p < .001), and a lack of exercise (strength exercise only OR = 3.394, 95% CI = 1.561-7.379, p = .002; neither type of exercise OR = 2.460, 95% CI = 1.513-4.000, p < .001). None of the sleep variables were associated with obesity.
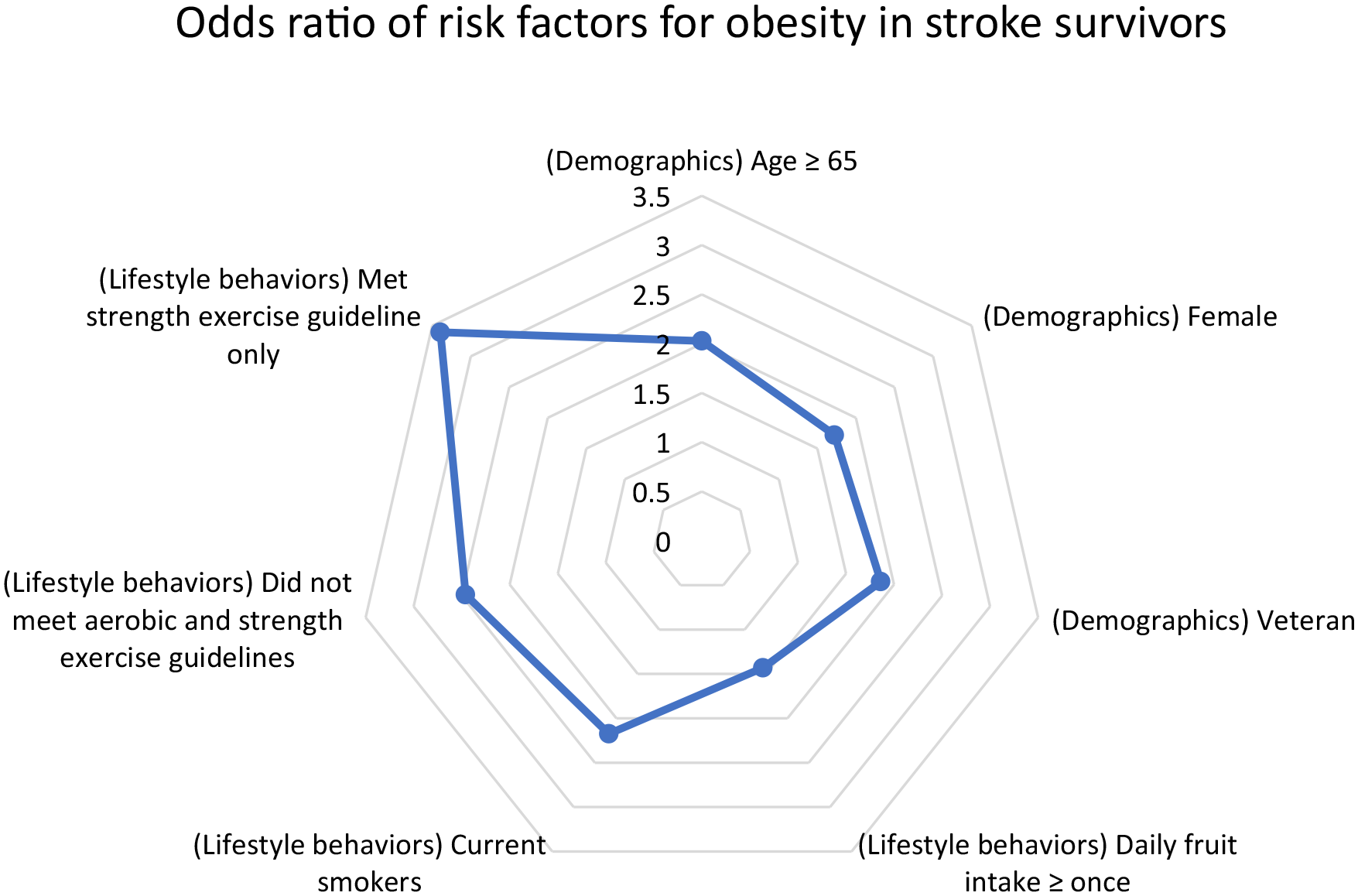
Risk factors for obesity among stroke survivors.
Discussion
The aim of this study was to explore which characteristics (demographics, diet, smoking, alcohol, physical activity, and sleep) affected obesity among stroke survivors. In the multivariate analysis, age ≥65 years, female sex, veteran status, ≥once-daily fruit intake, current smoking, and insufficient physical activity were positively associated with the risk of obesity. The relationship between age and obesity has been well documented in previous studies. As people age, they are likely to have reduced physical activity due to disability, arthritis, visual and hearing impairment, and pain; aging can also increase the risk of obesity by altering energy expenditure and hormone levels. 4 Compared to healthy older adults, older adults who have experienced a stroke might have more difficulty performing physical activities due to various complications, which may lead them to be obese.
In this study, female sex was a significant risk factor for obesity among stroke survivors. This finding was consistent with those of previous studies. Many researchers have reported that women are vulnerable to obesity because of hormone changes after menopause.22,23 Through the menopausal transition, women suffer from estrogen deficiency as well as excessive androgen; these hormonal imbalances increase food intake and body fat accumulation. 23 Stroke survivors who were veterans had a higher risk of obesity than stroke survivors who were not veterans. It is assumed that exposure to trauma, a unique meal culture during military service, and decreased physical activity may affect weight gain in veterans.17,18 In 1 study, 17% of veterans responded that they had retired from the military but still had eating disorders; respondents said they still ate very fast and thought of food all the time. 18
The stroke survivors in this study seemed to have healthy behaviors. More than half of them consumed fruit at least once a day and were non-smokers and non-heavy drinkers. The findings showed that stroke survivors who consumed fruit ≥once a day and those who currently smoked had a 1.4 times and 2.2 times higher risk of obesity than those who did not, respectively. Whether fruit intake increases or decreases the risk of obesity is still controversial across studies. According to researchers who advocate for the antiobesity effects of fruit, fruit is a great source of satiety, micronutrients, and fiber.24,25 However, other researchers have refuted these claims because fruit contains high amounts of simple sugars.25,26 The relationship between fruit and obesity may vary depending on the type of fruit and the amount of sugar in the fruit. As our data set did not contain any information on the type of fruit, it was not possible to further evaluate their relationship.
In this study, smoking was also found to be a significant risk factor for obesity among stroke survivors. This finding was inconsistent with well-known evidence that smoking decreases appetite and metabolic activities. 27 According to a large randomized trial conducted in 10 hospitals in the United States, a 1-year follow-up after smoking cessation showed a weight gain of 10 to 11 pounds, and the weight gain effect continued until the 5-year follow-up. 28 However, we could not find this relationship in our study. One possible explanation is that there might be other mediating factors between smoking and obesity in stroke survivors. For example, disease characteristics, including types of medications and the presence of depression, can mediate the effect of smoking on obesity.
Compared to participants who met both aerobic and strength exercise guidelines, participants who did not meet either or who only met strength exercise guidelines showed a higher risk of obesity. The Physical Activity Guidelines Advisory Committee recommends that older American adults engage in at least 150 minutes of aerobic activity and 2 strength exercise activities every week. 29 Our findings demonstrated that insufficient physical activity was associated with obesity among stroke survivors, and the association was greater in the group that met only the strength exercise guidelines. Performing sufficient physical activity can be difficult for stroke survivors because of their limited physical function, cognitive impairment, and lack of financial and social support.10,11,30 To encourage sufficient physical activity, tailored exercise and factors that interfere with exercise should be considered.
Marital status, income, and sleep difficulty were not significantly related to obesity among stroke survivors in the multivariate analysis. In previous studies, marital status has been reported as a significant risk factor for obesity. According to a large cohort study conducted in Korea, married people had a significantly higher prevalence of obesity in the middle-aged population than unmarried, divorced, and widowed people. 31 Considering that marital status was a significant factor in the univariate analysis, the effect of marital status on obesity might have been attenuated in the multivariate analysis. Low income is another conventional risk factor for obesity because of food insecurity and a poor living environment. Living in a food desert and lack of transportation can limit people’s access to fresh foods, and insufficient safe places for physical activity lead people to have a sedentary lifestyle. 32 Similar to marital status, income was a significant factor in the univariate analysis but not in the multivariate analysis. It is assumed that the effect of income on obesity was not large enough to be detected when covariates were considered. In several prospective studies, researchers reported that persistent and frequent sleep difficulty increased obesity. 33 However, a relationship between sleep difficulty and obesity was not found in this study. Possible explanations are that participants may have had mild symptoms or had recently developed symptoms. In the BRFSS survey, sleep difficulty was evaluated by asking about sleep in the past 2 weeks. Therefore, recent sleep difficulty reported at the time of the survey may not have been related to obesity.
Limitations
This study had some limitations. First, it was difficult to use the most recent BRFSS survey data set, although the 2021 BRFSS data set has been released. The BRFSS survey does not use a consistent questionnaire each year, and the 2017 BRFSS survey data set was the most recent data set that included sleep variables. As sleep variables were variables of interest, we used the 2017 data set. Second, the data set had limited information for further analysis. For example, the frequency of daily food intake was measured, but not the exact amount. Therefore, it was difficult to understand how much participants consumed of a particular food. Third, the relatively small sample size can affect generalizability and statistical power. Therefore, the findings of this study should be interpreted with caution.
Conclusion
The findings of this study showed that older age, female sex, a history of military service, frequent intake of fruit, smoking, and insufficient physical activity were associated with obesity among stroke survivors. Whereas previous obesity studies predominantly targeted the general population, especially children, this study targeted stroke survivors. Considering that obesity is a common risk factor for stroke recurrence as well as other chronic diseases, unhealthy behaviors should be modified for stroke survivors’ health. To promote healthy behaviors, health care providers need to formulate tailored diet education and exercise plans. In addition, appropriate transitional care should be provided to stroke survivors to prevent obesity and other chronic diseases after discharge.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (No. 2020 R1A6A1A03041989). This research was supported by the Brain Korea 21 FOUR Project funded by National Research Foundation (NRF) of Korea, Yonsei University College of Nursing.